
Operative Approach: Posterior Thoracolumbar Approach (Midline & Wiltse / Pedicle Screw Fixation)
Case / Approach Snapshot
- Anatomy at risk: thoracolumbar cord/conus/cauda equina, traversing and exiting roots, pedicles and medial walls, segmental vessels, epidural venous plexus, facets/pars/transverse processes, paraspinal muscle innervation, and posterior tension band.
- Operative steps: localize levels, position prone with abdomen free, choose midline/Wiltse/percutaneous corridor, expose bony landmarks, decompress when indicated, place instrumentation with imaging/neuromonitoring checks, decorticate/graft, and close the fascial envelope securely.
- Rescue plans: wrong-level concern, pedicle breach, neuromonitoring change, epidural bleeding, dural tear, poor screw purchase, malreduction, junctional alignment problem, and wound/closure failure.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
CNS Video Library
AO Spine / Surgery Reference — posterior thoracolumbar · Neurosurgical Atlas — Spine · Radiopaedia — pedicle screws · PubMed Central — Wiltse approach
High-Yield Literature
- Microsurgical anatomy and treatment of dural defects in spontaneous spinal cerebrospinal fluid leaks — Matsuhashi A. Journal of neurosurgery. Spine 2021. PubMed
- Clinicopathologic Features of Thoracolumbar Interdural Disc Herniations: A Retrospective Case Series with a Systematic Literature Review — Fiorenza V. World neurosurgery 2020. PubMed
- [Microsurgical treatment of spinal cavernous malformation] — Gu XC. Zhonghua yi xue za zhi 2008. PubMed
- Posterior Thoracolumbar Instrumented Fusion for Burst Fractures: A Meta-analysis — Ituarte F. Clinical spine surgery 2019. PubMed
- Recognition of posterior thoracolumbar instrumentations used in spinal deformity surgery and techniques for implant removal — Kato S. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia 2021. PubMed
- Comparison of Anterior Versus Posterior Approach in the Treatment of Thoracolumbar Fractures: A Systematic Review — Zhu Q. International surgery 2015. PubMed
- Posterior thoracolumbar hemivertebra resection and short-segment fusion in congenital scoliosis: surgical outcomes and complications with more than 5-year follow-up — Bao B. BMC surgery 2021. PubMed
- Postoperative ileus risk after posterior thoracolumbar fusion performed with total intravenous anesthesia versus inhaled anesthesia — Sherrod BA. Journal of neurosurgery. Spine 2023. PubMed
- Biomechanical effects of osteoporosis severity on the occurrence of proximal junctional kyphosis following long-segment posterior thoracolumbar fusion — Zhao G. Clinical biomechanics (Bristol, Avon) 2023. PubMed
- Spinal instrumentation — Spivak JM. Current opinion in rheumatology 1994. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
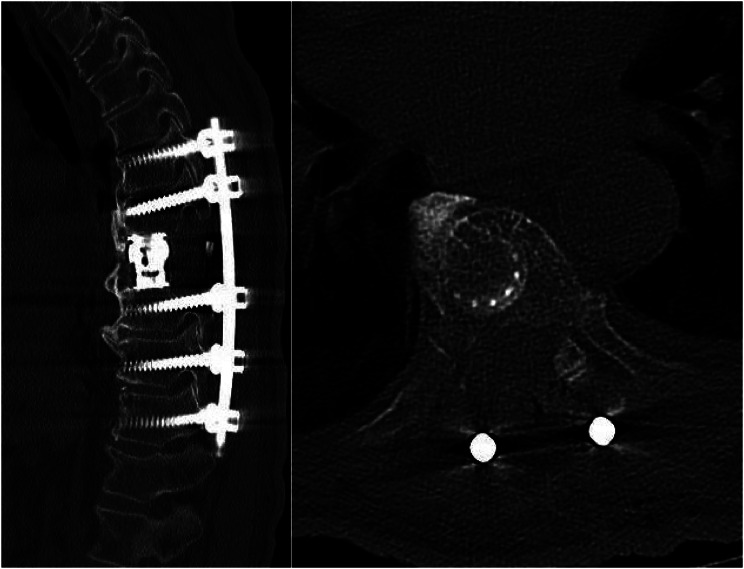 Fig. 4. Sagittal (left) and axial (right) slices from the patient’s post-operative CT scan demonstrating the sagittal anterior column reconstruction and intact costocentral articulation on the… Source: A rib-sparing unilateral transpedicular thoracic corpectomy using the ultrasonic bone scalpel: a novel technique and pictorial guide — BMC Surgery 2024; CC BY-NC-ND.
Fig. 4. Sagittal (left) and axial (right) slices from the patient’s post-operative CT scan demonstrating the sagittal anterior column reconstruction and intact costocentral articulation on the… Source: A rib-sparing unilateral transpedicular thoracic corpectomy using the ultrasonic bone scalpel: a novel technique and pictorial guide — BMC Surgery 2024; CC BY-NC-ND.
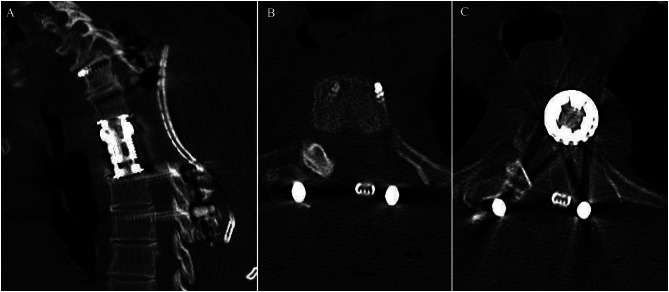 Fig. 6. Sagittal (A), axial T3 level (B), and axial T4 level (C) slices from the patient’s post-operative CT scan demonstrating the two-level sagittal anterior column reconstruction and… Source: A rib-sparing unilateral transpedicular thoracic corpectomy using the ultrasonic bone scalpel: a novel technique and pictorial guide — BMC Surgery 2024; CC BY-NC-ND.
Fig. 6. Sagittal (A), axial T3 level (B), and axial T4 level (C) slices from the patient’s post-operative CT scan demonstrating the two-level sagittal anterior column reconstruction and… Source: A rib-sparing unilateral transpedicular thoracic corpectomy using the ultrasonic bone scalpel: a novel technique and pictorial guide — BMC Surgery 2024; CC BY-NC-ND.
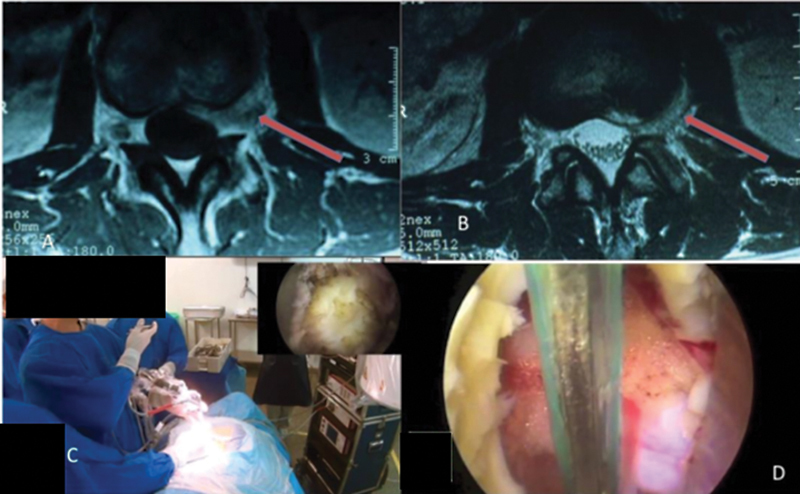 Fig. 2. Transforaminal endoscopic approach. (A) location of the nerve root ganglion, (B) direct access to the disc abscess, (C) positioning of the team, (D) endoscopic view of the neural root. Source: Access to the Lumbosacral Spine: A Current View — Revista Brasileira de Ortopedia 2024; CC BY.
Fig. 2. Transforaminal endoscopic approach. (A) location of the nerve root ganglion, (B) direct access to the disc abscess, (C) positioning of the team, (D) endoscopic view of the neural root. Source: Access to the Lumbosacral Spine: A Current View — Revista Brasileira de Ortopedia 2024; CC BY.
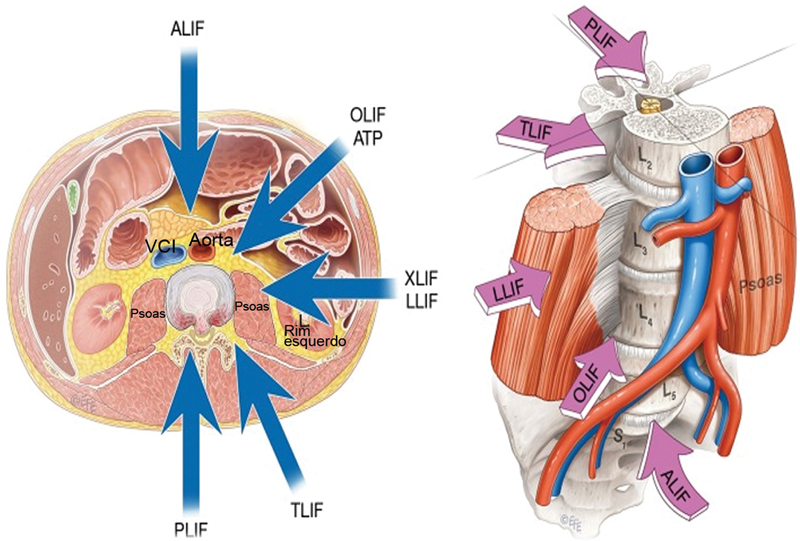 Fig. 1. Possíveis abordagens à fusão intervertebral lombar. ALIF, fusão intersomática lombar anterior; OLIF, fusão intersomática lombar lateral oblíqua; ATP, abordagem anterior ao psoas; XLIF,… Source: Access to the Lumbosacral Spine: A Current View — Revista Brasileira de Ortopedia 2024; CC BY.
Fig. 1. Possíveis abordagens à fusão intervertebral lombar. ALIF, fusão intersomática lombar anterior; OLIF, fusão intersomática lombar lateral oblíqua; ATP, abordagem anterior ao psoas; XLIF,… Source: Access to the Lumbosacral Spine: A Current View — Revista Brasileira de Ortopedia 2024; CC BY.
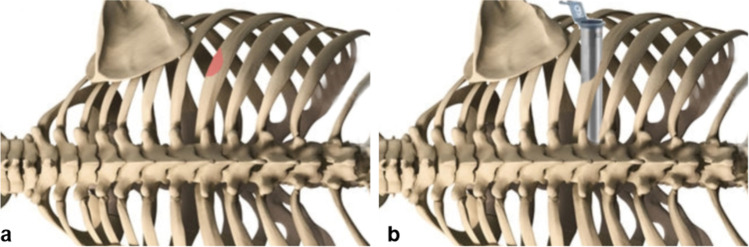 Fig. 1. Schematic illustration of partial resection of the lower rib (a) and positioning of the tubular retractor (b) for the retropleural, retractor-assisted approach to thoracic disc herniations Source: A minimally invasive tubular retractor–assisted retropleural approach for thoracic disc herniations — case series and technical note — Acta Neurochirurgica 2023; CC BY.
Fig. 1. Schematic illustration of partial resection of the lower rib (a) and positioning of the tubular retractor (b) for the retropleural, retractor-assisted approach to thoracic disc herniations Source: A minimally invasive tubular retractor–assisted retropleural approach for thoracic disc herniations — case series and technical note — Acta Neurochirurgica 2023; CC BY.
 Fig. 2. Insertion of the tubular retractor (a) with the aid of intraoperative fluoroscopy at the level Th 10/11 (b) and drilling of the head of the rib and posterior lateral part of the disc (c)… Source: A minimally invasive tubular retractor–assisted retropleural approach for thoracic disc herniations — case series and technical note — Acta Neurochirurgica 2023; CC BY.
Fig. 2. Insertion of the tubular retractor (a) with the aid of intraoperative fluoroscopy at the level Th 10/11 (b) and drilling of the head of the rib and posterior lateral part of the disc (c)… Source: A minimally invasive tubular retractor–assisted retropleural approach for thoracic disc herniations — case series and technical note — Acta Neurochirurgica 2023; CC BY.
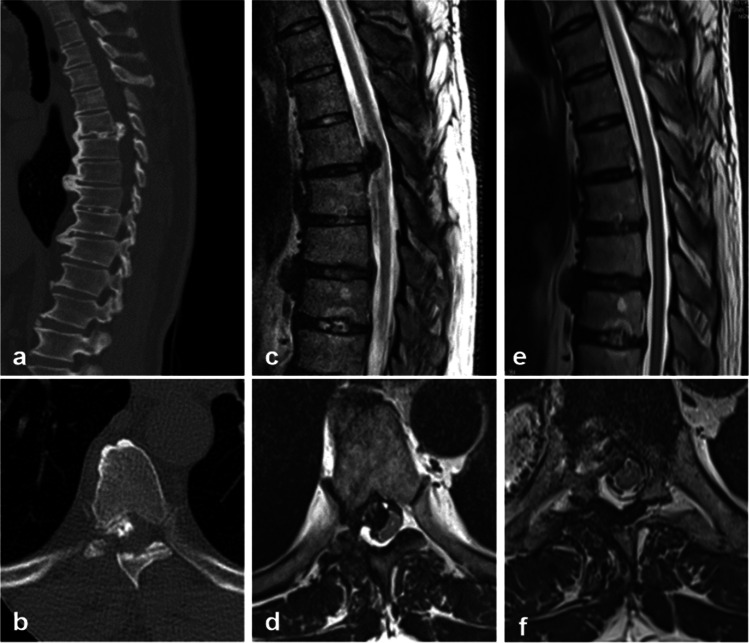 Fig. 3. Preoperative (a–d) and postoperative (e–f) MRI of patient No. 5 with a mediolateral left-sided, partially calcified disc herniation at level Th 7/8 causing relevant spinal cord… Source: A minimally invasive tubular retractor–assisted retropleural approach for thoracic disc herniations — case series and technical note — Acta Neurochirurgica 2023; CC BY.
Fig. 3. Preoperative (a–d) and postoperative (e–f) MRI of patient No. 5 with a mediolateral left-sided, partially calcified disc herniation at level Th 7/8 causing relevant spinal cord… Source: A minimally invasive tubular retractor–assisted retropleural approach for thoracic disc herniations — case series and technical note — Acta Neurochirurgica 2023; CC BY.
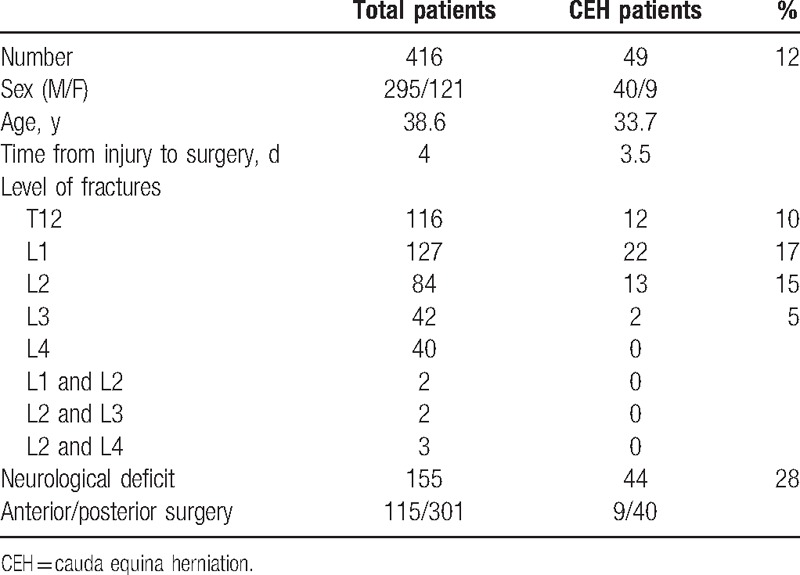 Figure 8. Source: Clinical case-series report of traumatic cauda equina herniation: A pathological phenomena occurring with thoracolumbar and lumbar burst fractures — Medicine (Baltimore). 2017 Apr 7;96(14):e6446. doi: 10.1097/MD.0000000000006446; CC BY.
Figure 8. Source: Clinical case-series report of traumatic cauda equina herniation: A pathological phenomena occurring with thoracolumbar and lumbar burst fractures — Medicine (Baltimore). 2017 Apr 7;96(14):e6446. doi: 10.1097/MD.0000000000006446; CC BY.
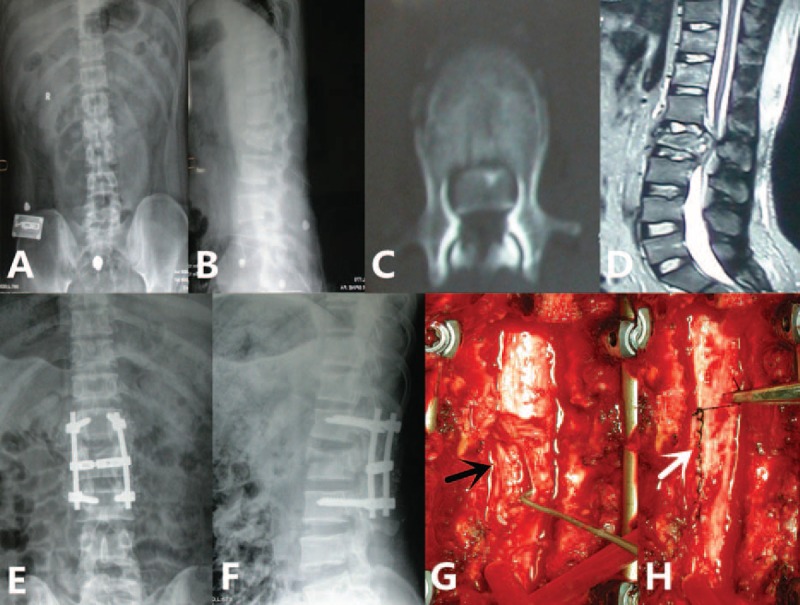 Figure 2. A 32-year-old male patient with L2 burst fracture, with ASIA C neurological impairment. (A and B) preoperative anteroposterior and lateral radiographs showed a L2 burst fracture; (C and… Source: Clinical case-series report of traumatic cauda equina herniation — Medicine 2017; CC BY.
Figure 2. A 32-year-old male patient with L2 burst fracture, with ASIA C neurological impairment. (A and B) preoperative anteroposterior and lateral radiographs showed a L2 burst fracture; (C and… Source: Clinical case-series report of traumatic cauda equina herniation — Medicine 2017; CC BY.
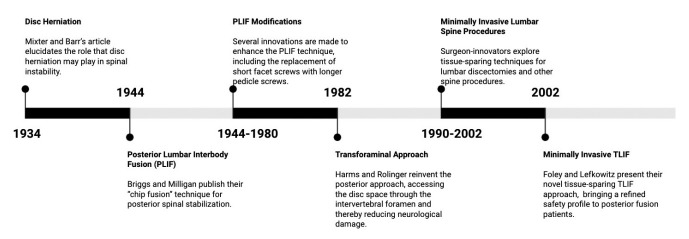 Fig. 3.. The evolution of posterior-approach lumbar fusion, from 1934–2002. Source: History and Evolution of the Minimally Invasive Transforaminal Lumbar Interbody Fusion — Neurospine 2022; CC BY-NC.
Fig. 3.. The evolution of posterior-approach lumbar fusion, from 1934–2002. Source: History and Evolution of the Minimally Invasive Transforaminal Lumbar Interbody Fusion — Neurospine 2022; CC BY-NC.
The posterior thoracolumbar approach is the universal posterior corridor to the thoracic and lumbar spine — the basis for laminectomy, TLIF/PLIF, pedicle-screw fixation, deformity correction, and tumor/trauma stabilization. It is performed midline (subperiosteal exposure of the posterior elements) or via the muscle-splitting Wiltse paramedian plane for lateral/percutaneous screw placement with less muscle stripping.
General Considerations
- What it accesses: the posterior elements (spinous processes, laminae, facets, pars, transverse processes) and, through them, the pedicles (for screws), the canal/thecal sac and roots (decompression), and the disc space (TLIF/PLIF).
- Midline vs Wiltse:
- Midline subperiosteal: the standard for open decompression + fusion; full exposure of laminae/facets but more paraspinal muscle stripping/denervation.
- Wiltse paramedian (muscle-splitting): a plane between multifidus and longissimus that goes directly onto the facet/transverse process — ideal for far-lateral discs, percutaneous/MIS pedicle screws, and reducing muscle morbidity.
- Abdomen free (Jackson/Wilson frame) is the single most important set-up detail — it lowers epidural venous pressure and blood loss and helps restore lordosis.
Approach Choice: Midline vs Wiltse vs Percutaneous
| Need | Midline subperiosteal | Wiltse paramedian | Percutaneous / MIS |
|---|---|---|---|
| Central decompression | Best exposure | Limited unless tubular decompression planned | Limited |
| TLIF / facetectomy | Standard, flexible | Excellent for unilateral TLIF/far-lateral access | Possible with tubular systems |
| Trauma fixation | Fast and extensile | Useful for short-segment fixation without decompression | Useful when no open decompression needed |
| Deformity/osteotomy | Required for wide releases/osteotomies | Adjunct only | Adjunct only |
| Muscle preservation | More stripping | Muscle-splitting | Most preserving but imaging-dependent |
| Revision anatomy | Direct scar control | May avoid midline scar | Challenging if landmarks distorted |
The practical rule: choose the smallest corridor that still allows safe decompression, reduction, fixation, grafting, and hemostasis. A percutaneous construct is not a virtue if the patient needs direct canal decompression, durotomy repair, tumor separation, or osteotomy work.
Indications
- Degenerative: stenosis/spondylolisthesis → lumbar laminectomy, TLIF; far-lateral disc (Wiltse)
- Trauma: thoracolumbar burst fracture, flexion-distraction (Chance)
- Deformity: adult deformity / osteotomy
- Tumor (posterolateral decompression / vertebral corpectomy), infection
Relevant Surgical Anatomy
- Midline: supraspinous/interspinous ligaments and the avascular raphe; paraspinal muscles — multifidus (medial) and longissimus/iliocostalis (lateral); the Wiltse plane is the natural cleft between multifidus and longissimus.
- Pedicle entry points: lumbar — at the junction of the transverse process, superior articular facet, and pars (Roy-Camille / Magerl); thoracic — just below the facet/transverse-process junction with a steeper medial/caudal angle. Trajectory must respect the medial pedicle wall (canal/cord/root) and inferior wall (exiting root).
- Neural elements: thecal sac, traversing and exiting nerve roots (TLIF works through Kambin’s triangle / facetectomy window), conus (upper lumbar), thoracic cord (low tolerance — thoracic medial breach is catastrophic).
Preoperative Evaluation
- CT/MRI for levels, pedicle diameter and trajectory, deformity/alignment; navigation/robotics dataset; bone quality (osteoporosis → augmentation). Level localization plan (counting is error-prone in the thoracic spine).
Level Localization Strategy
- Count from fixed landmarks on pre-op imaging: sacrum upward for lumbar, C2 downward and ribs for thoracic, and correlate with transitional anatomy.
- Mark the intended levels with AP/lateral fluoroscopy before incision and again before irreversible bone work.
- In thoracic cases, rib counting and poor shoulder visualization can mislead; use full-spine scout imaging or navigation when numbering is ambiguous.
- For deformity, define the upper/lower instrumented vertebrae, neutral/stable vertebrae, and planned osteotomy levels before positioning.
- For tumor/infection, confirm the pathologic level against MRI, CT, and intraoperative localization; wrong-level exposure is easy when multiple compression fractures exist.
Logistics, OR Setup & Orders
- OR table/bed: radiolucent spine-capable table selected for approach, imaging, instrumentation, patient size, and alignment goals; keep abdomen free for prone cases.
- OR setup: Jackson/radiolucent spine table or approach-specific lateral/anterior setup, C-arm/O-arm/navigation availability, microscope/loupes, neuromonitoring leads before positioning, and implant trays opened only after final level/plan confirmation.
- Special needs: arterial line and Foley for long instrumented cases, type/screen or crossmatch for deformity/corpectomy/trauma, antibiotic redosing plan, MAP support for SCI/myelopathy, and no long paralytic when MEPs are needed.
- Immediate postop orders: neuro checks focused on myotomes/sensory level, postop CT/X-rays per construct, brace/activity orders, drain output thresholds, DVT prophylaxis timing, dysphagia/airway monitoring for anterior cervical cases, and rehab mobilization plan.
Anesthesia & Neuromonitoring
- GA, prone; SSEP/MEP and free-run/triggered EMG (pedicle screw stimulation), especially for thoracic/deformity; no long-acting paralytic with MEPs; antifibrinolytics for deformity; blood available.
Positioning
- OR table/bed: radiolucent spine-capable table selected for approach, imaging, instrumentation, patient size, and alignment goals; keep abdomen free for prone cases.
- Prone on a Jackson or Wilson frame with the abdomen hanging free (reduces venous bleeding; Jackson preserves lordosis, Wilson flexes for stenosis exposure). Pad eyes/face (prone ION), chest, knees, ulnar nerves; arms ≤90°. Reverse Trendelenburg slightly; confirm orthogonal fluoroscopy.
Incision & Exposure
- Midline: incise to the fascia, split the avascular raphe, and subperiosteally elevate the paraspinals off the spinous processes/laminae out to the transverse-process tips for fusion levels (preserve facet capsules at non-fused segments).
- Wiltse: paramedian fascial incisions ~1.5–2 finger-breadths off midline; finger-develop the multifidus–longissimus plane directly to the facet/TP (the corridor for percutaneous/MIS screws).
- Localize the level fluoroscopically before bone work.
Pedicle Screw Fixation & Decompression

Avila MJ, Baaj AA. *Cureus 2016;8(3):e501 — CC BY.*
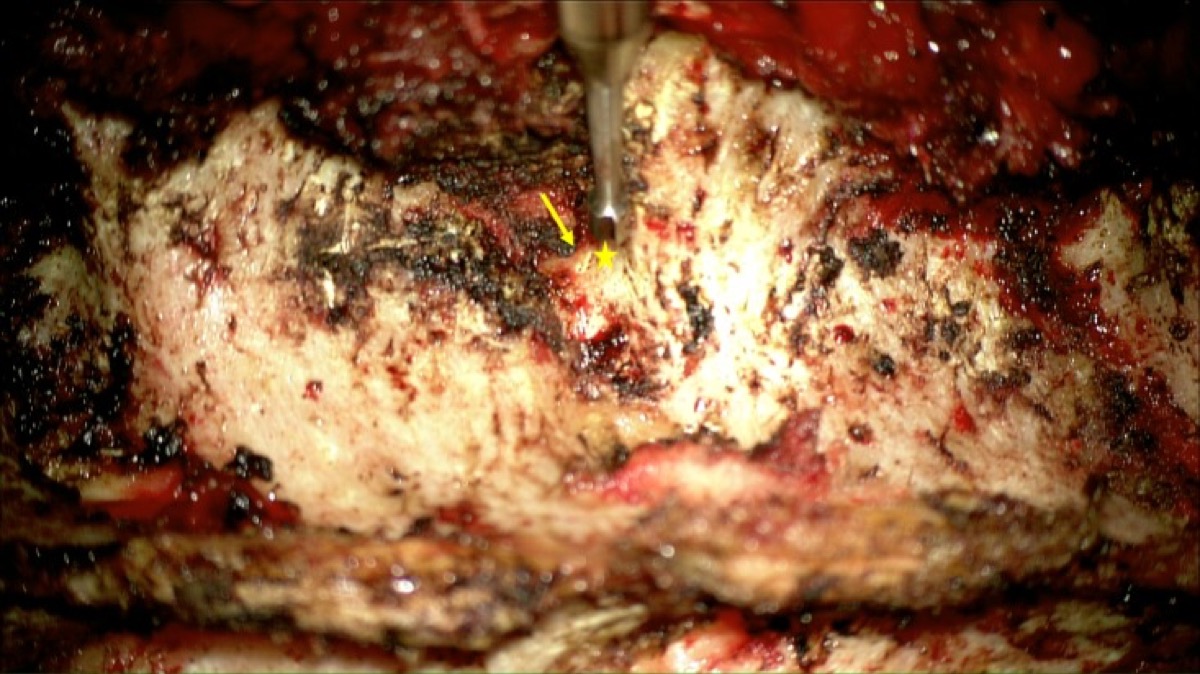
Avila MJ, Baaj AA. *Cureus 2016;8(3):e501 — CC BY.*
- Cannulate the pedicles at the level-specific entry/trajectory (freehand, fluoro, navigation, or robotic); confirm with triggered EMG and imaging — respect the medial and inferior pedicle walls. Decorticate and graft the posterolateral gutter; place rods after decompression/interbody.
- Decompression (laminectomy/facetectomy) and interbody fusion (TLIF/PLIF) proceed per the procedure guide → TLIF.
Freehand Pedicle Screw Sequence
- Expose the transverse process, pars, facet complex, and mammillary/superior articular landmarks without violating adjacent-level facets.
- Start with a burr at the level-specific entry point; create a cancellous pilot channel rather than skiving on cortical bone.
- Use a pedicle probe with tactile feedback: cancellous corridor, no sudden loss of resistance medially/inferiorly, and a trajectory matching pre-op CT.
- Ball-tip palpate all walls: medial, lateral, superior, inferior, and floor. Any soft breach should trigger redirection or imaging confirmation.
- Tap, repalpate, place screw, check triggered EMG when used, and confirm with fluoroscopy/navigation before rod reduction.
Decompression Sequence
- Remove bone in an outside-in, ligament-preserving fashion until the safe plane is clear; in stenosis, keep Kerrisons pointed away from dura and avoid levering against the thecal sac.
- For thoracic cord compression, favor drill/ultrasonic bone removal and thin-shell removal over aggressive rongeur bites; the thoracic cord does not tolerate manipulation.
- In tumor or infection, obtain cultures/pathology early, protect uninvolved dura, and plan reconstruction/fixation before destabilizing posterior elements.
- In trauma, decide whether decompression is direct (laminectomy/transpedicular) or indirect via reduction/ligamentotaxis; laminectomy alone can worsen instability if not paired with fixation.
Intraoperative Rescue
- Medial breach or triggered EMG concern: leave the tract, redirect laterally/superiorly, confirm with imaging, and do not accept a questionable thoracic medial wall.
- Dural tear: expose enough normal dura to repair without tension; primary suture when possible, patch/sealant adjunct, Valsalva test, and drain strategy tailored to repair quality.
- Epidural venous bleeding: confirm abdomen is free, lower venous pressure, pack with hemostatic matrix/patties, and avoid blind bipolar deep in the foramen.
- Loss of MEP/SSEP: stop correction/distraction, raise MAP, check anesthetic/paralytic/temperature, remove offending hardware or reverse correction, and inspect for hematoma/compression.
- Poor bone purchase: upsize/redirect, cement augmentation, cortical trajectory, hooks/bands, longer construct, or pelvic fixation depending on pathology.
Closure
- Hemostasis, layered closure of fascia/muscle, then fascia, subcutaneous, skin; subfascial drain common. Meticulous posterior closure limits infection/dehiscence.
Bony anatomy (vertebra / pedicle detail)
Nuances & Pitfalls (surgeon-level)
- Abdomen free = less bleeding and better lordosis — never skip it.
- Pedicle breach: medial → dura/root/cord (thoracic medial breach = cord injury); lateral → poor purchase/vascular; use triggered EMG/navigation and check walls.
- Wrong-level surgery — fluoroscopic localization, count from fixed landmarks (sacrum/ribs), mark.
- Muscle morbidity: prefer Wiltse/MIS when extensive midline stripping isn’t needed (less denervation/atrophy and pain).
- Maintain sagittal alignment (lordosis) — flat-back/junctional failure follows poor restoration.
- Dural tear (revision/ossified ligamentum) — repair/augment; infection/dehiscence risk is higher posteriorly.
Complications
Pedicle-screw malposition (neuro/vascular), dural tear/CSF leak, wound infection/dehiscence, blood loss/epidural hematoma, junctional kyphosis/flat-back, pseudarthrosis, positioning injuries (ION, pressure, brachial plexus), wrong-level surgery.
Cross-links
- Procedures: lumbar laminectomy · TLIF · thoracolumbar burst fracture · adult deformity osteotomy · vertebral corpectomy
- Related corridors: transpsoas-approach.md · transthoracic-approach.md · posterior-cervical-approach.md
Figure Use & Attribution
About the figures. Copyrighted operative figures/videos are linked (Neurosurgical Atlas, AO Spine / Surgery Reference); embedded images are public-domain (Gray’s Anatomy), credited beneath each image. See media-sources.md and figures/CREDITS.md.
Technique references: AO Spine / Surgery Reference — Thoracolumbar · Neurosurgical Atlas — Spine · Radiopaedia — thoracolumbar
Chief-Level Corridor Review
Use these as the senior-level mental model for Posterior Thoracolumbar Approach (Midline & Wiltse / Pedicle Screw Fixation):
- Decision point: Define the exposure goal before incision: target, working angles, proximal/distal control, and the structure that cannot tolerate retraction.
- Technical lever: Know the first irreversible step: bone removal, dural opening, vascular control, or muscle/fascial division that commits the corridor.
- Bailout: Verbalize the bailout: extend exposure, change trajectory, add CSF drainage, obtain proximal control, convert to a larger corridor, or stop for imaging.
- Postop watch: Protect closure from the start: vascularized tissue, watertight dural/reconstruction plan, dead-space control, and drain strategy should be chosen before the final intradural step.
Common Pimp Questions
Use these to pressure-test preparation for Posterior Thoracolumbar Approach (Midline & Wiltse / Pedicle Screw Fixation):
- What patient position and head rotation make gravity work for this corridor?
- What named nerve, vessel, sinus, or muscle/fascial plane is most commonly injured?
- What bone work or soft-tissue step creates the exposure rather than simply using more retraction?
- What is the bailout if exposure is inadequate, bleeding occurs, or the brain is tight?
- What closure maneuver prevents the signature complication of this approach?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Exact head rotation/flexion/extension and pin placement: [attending-specific]
- Skin incision length, flap type, and muscle/fascial preservation technique: [attending-specific]
- Drill, rongeur, endoscope, microscope, retractor, and navigation preferences: [attending-specific]
- Drain use, closure materials, watertightness threshold, and postop imaging routine: [attending-specific]
Case Guides Using This Approach
- Adult Spinal Deformity Correction (with Osteotomy — SPO / PSO / VCR)
- Flexion-Distraction (Chance) Injury Fixation
- Intradural Extramedullary Spinal Tumor Resection (Meningioma / Schwannoma)
- Intramedullary Spinal Cord Tumor Resection (Ependymoma / Astrocytoma / Hemangioblastoma)
- Intrathecal Baclofen (ITB) Pump Implantation
- Lumbar Laminectomy for Spinal Stenosis
- Lumbar Microdiscectomy
- Penetrating Spine Injury (Gunshot / Stab) Management
- Sacral Fracture / Spinopelvic (Lumbopelvic) Fixation
- Spinal Arteriovenous Malformation (Intramedullary / Perimedullary)
- Spinal Cord Cavernous Malformation Resection
- Spinal Cord Stimulator (SCS) Placement
- Spinal Dural Arteriovenous Fistula (dAVF) — Surgical Ligation
- Spinal Epidural Abscess — Decompression & Drainage
- Syringomyelia — Management / Syringosubarachnoid Shunt
- Tethered Cord Release
- Thoracolumbar Burst Fracture Fixation
- Transforaminal Lumbar Interbody Fusion (TLIF)
- Vertebral Osteomyelitis / Discitis — Surgical Management
References
- Wiltse LL, Bateman JG, Hutchinson RH, Nelson WE. The paraspinal sacrospinalis-splitting approach to the lumbar spine. J Bone Joint Surg Am. 1968;50(5):919–926.
- Roy-Camille R, Saillant G, Mazel C. Internal fixation of the lumbar spine with pedicle screw plating. Clin Orthop. 1986.
- Magerl F. External skeletal fixation of the lower thoracic and lumbar spine. 1984.
- AO Foundation. Posterior approach, thoracolumbar spine; pedicle screw fixation. AO Spine / Surgery Reference. link