
Case Prep: Tethered Cord Release
Case / Approach Snapshot
- Anatomy at risk: the named neural, vascular, bony, CSF, and soft-tissue structures that determine the safe corridor and likely morbidity.
- Operative steps: confirm indication and imaging, position and expose deliberately, complete the core surgical maneuver, verify the result, and close with a complication-prevention plan; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: bleeding, neurologic change, wrong target or level, CSF leak, infection, hardware or reconstruction failure, and a staged or alternate-treatment plan.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] [child/adult] with tethered cord syndrome ([tight filum / lipomyelomeningocele / post-repair retethering / split cord]) presenting with [back/leg pain, motor or sensory decline, bladder dysfunction, scoliosis, foot deformity] planned for [level] laminectomy for microsurgical untethering.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior thoracolumbar approach — midline lumbosacral exposure, laminoplasty/laminectomy, dural opening, and closure principles.
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Tethered cord syndrome — Agarwalla PK. Neurosurgery clinics of North America 2007. PubMed
- Tethered Cord Syndrome After Myelomeningocele Repair: A Literature Update — Ferreira Furtado LM. Cureus 2020. PubMed
- Clinical criteria for filum terminale resection in occult tethered cord syndrome — Klinge PM. Journal of neurosurgery. Spine 2024. PubMed
- Tethered cord syndrome from pediatric and adult perspectives: a comprehensive systematic review of 6135 cases — He K. Neurosurgical focus 2024. PubMed
- Mapping and monitoring of tethered cord and cauda equina surgeries — Galloway G. Handbook of clinical neurology 2022. PubMed
- [Tethered cord syndrome in children: about a case] — Hode L. The Pan African medical journal 2019. PubMed
- Tethered cord syndrome in KBG syndrome — Hills S. American journal of medical genetics. Part A 2023. PubMed
- Tethered Cord Syndrome (TCS) — Weisbrod LJ. 2026. PubMed
- Diagnosis and Management of Tethered Cord Syndrome — Hara T. Advances and technical standards in neurosurgery 2024. PubMed
- Split cord malformation and tethered cord syndrome: case series with long-term follow-up and literature review — Kobets AJ. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2021. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
 Fig. 1. Patient 2 preoperative supine anteroposterior view (90 degrees T11–L3). Abbreviation: AP, anteroposterior. Source: Concurrent Tethered Cord Release and Growing-Rod Implantation—Is It Safe? — Global Spine Journal 2012; open access.
Fig. 1. Patient 2 preoperative supine anteroposterior view (90 degrees T11–L3). Abbreviation: AP, anteroposterior. Source: Concurrent Tethered Cord Release and Growing-Rod Implantation—Is It Safe? — Global Spine Journal 2012; open access.
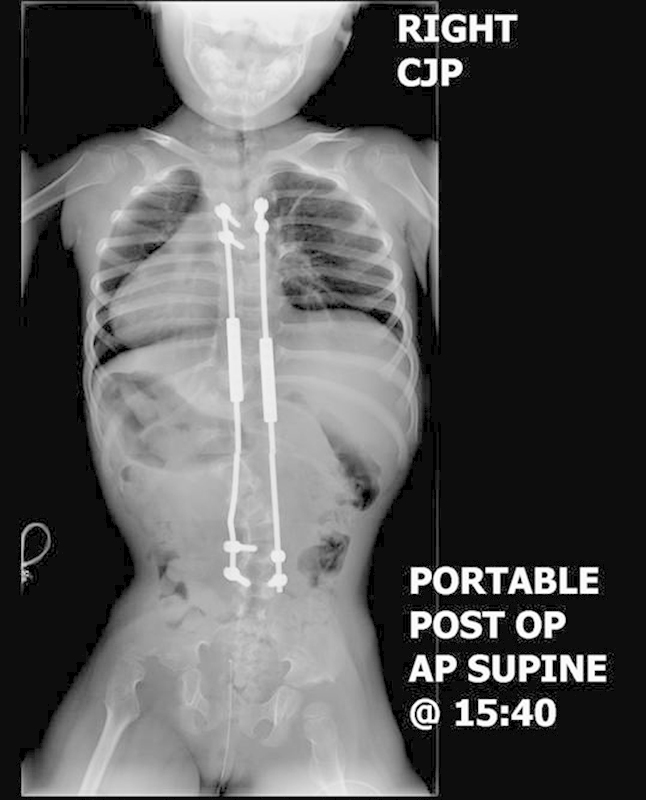 Fig. 2. Patient 2 postoperative supine anteroposterior view (53 degrees T11–L3). Abbreviations: AP, anteroposterior; post op, postoperative. Source: Concurrent Tethered Cord Release and Growing-Rod Implantation—Is It Safe? — Global Spine Journal 2012; open access.
Fig. 2. Patient 2 postoperative supine anteroposterior view (53 degrees T11–L3). Abbreviations: AP, anteroposterior; post op, postoperative. Source: Concurrent Tethered Cord Release and Growing-Rod Implantation—Is It Safe? — Global Spine Journal 2012; open access.
 Fig. 3. Patient 2 preoperative recumbent lateral view. Note thoracolumbar kyphosis. Source: Concurrent Tethered Cord Release and Growing-Rod Implantation—Is It Safe? — Global Spine Journal 2012; open access.
Fig. 3. Patient 2 preoperative recumbent lateral view. Note thoracolumbar kyphosis. Source: Concurrent Tethered Cord Release and Growing-Rod Implantation—Is It Safe? — Global Spine Journal 2012; open access.
 Fig. 4. Patient 2 postoperative lateral view. Abbreviations: post op, postoperative. Source: Concurrent Tethered Cord Release and Growing-Rod Implantation—Is It Safe? — Global Spine Journal 2012; open access.
Fig. 4. Patient 2 postoperative lateral view. Abbreviations: post op, postoperative. Source: Concurrent Tethered Cord Release and Growing-Rod Implantation—Is It Safe? — Global Spine Journal 2012; open access.
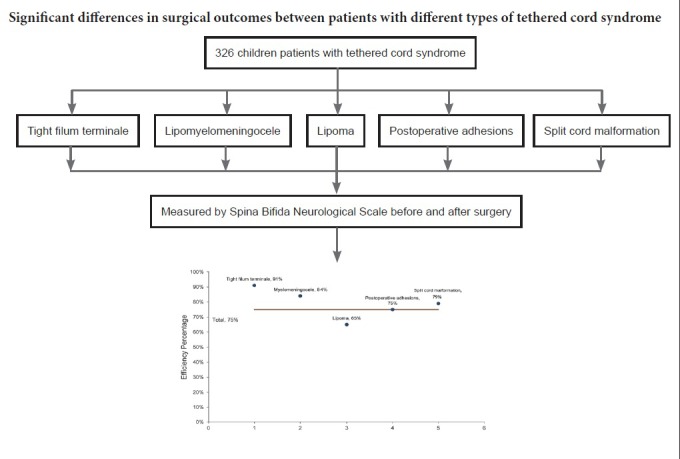 Figure 6. Source: Microsurgical efficacy in 326 children with tethered cord syndrome: a retrospective analysis — Neural Regen Res. 2019 Jan;14(1):149–55. doi: 10.4103/1673-5374.243720; CC BY-NC-SA.
Figure 6. Source: Microsurgical efficacy in 326 children with tethered cord syndrome: a retrospective analysis — Neural Regen Res. 2019 Jan;14(1):149–55. doi: 10.4103/1673-5374.243720; CC BY-NC-SA.
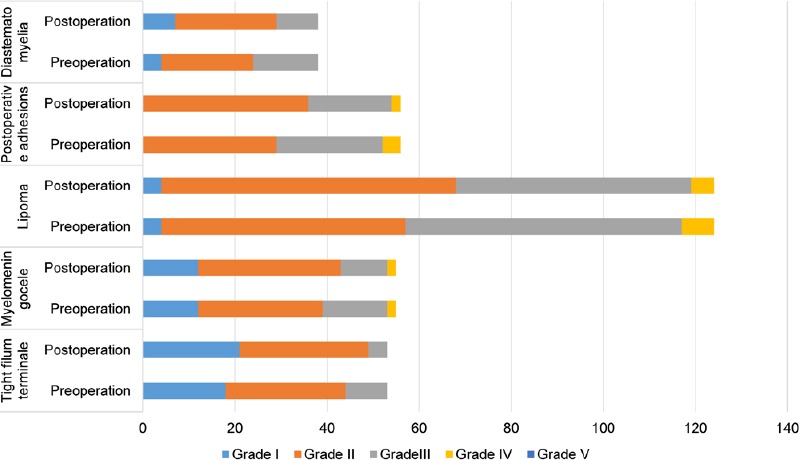 Figure 2. Spina Bifida Neurological Scale (SBNS) functional classification of children with different types of tethered cord syndrome before surgery and 3 months after surgery (n = 326).Horizontal… Source: Microsurgical efficacy in 326 children with tethered cord syndrome: a retrospective analysis — Neural Regeneration Research 2019; CC BY-NC-SA.
Figure 2. Spina Bifida Neurological Scale (SBNS) functional classification of children with different types of tethered cord syndrome before surgery and 3 months after surgery (n = 326).Horizontal… Source: Microsurgical efficacy in 326 children with tethered cord syndrome: a retrospective analysis — Neural Regeneration Research 2019; CC BY-NC-SA.
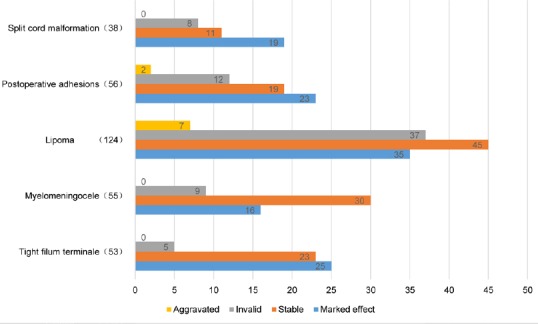 Figure 3. Efficacy analysis of different types of tethered cord syndrome postoperatively.Horizontal axis shows the number of patients (n = 326). Source: Microsurgical efficacy in 326 children with tethered cord syndrome: a retrospective analysis — Neural Regeneration Research 2019; CC BY-NC-SA.
Figure 3. Efficacy analysis of different types of tethered cord syndrome postoperatively.Horizontal axis shows the number of patients (n = 326). Source: Microsurgical efficacy in 326 children with tethered cord syndrome: a retrospective analysis — Neural Regeneration Research 2019; CC BY-NC-SA.
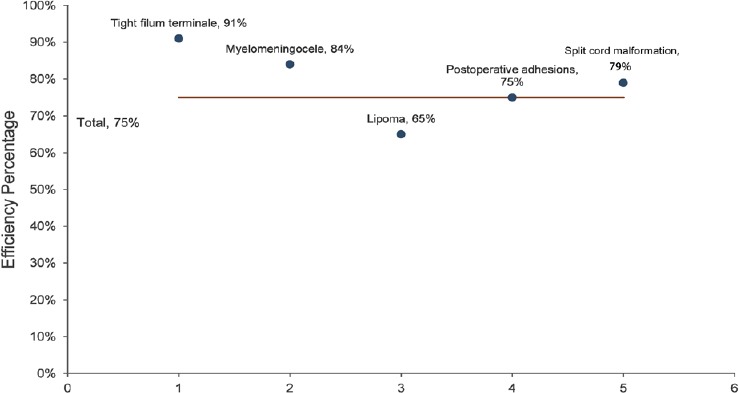 Figure 4. Efficacy percentage of different types of tethered cord syndrome postoperatively.Efficiency = (marked effect + stable)/total number of cases followed up (n = 326). Source: Microsurgical efficacy in 326 children with tethered cord syndrome: a retrospective analysis — Neural Regeneration Research 2019; CC BY-NC-SA.
Figure 4. Efficacy percentage of different types of tethered cord syndrome postoperatively.Efficiency = (marked effect + stable)/total number of cases followed up (n = 326). Source: Microsurgical efficacy in 326 children with tethered cord syndrome: a retrospective analysis — Neural Regeneration Research 2019; CC BY-NC-SA.
 Figure 10. Source: Microsurgical efficacy in 326 children with tethered cord syndrome: a retrospective analysis — Neural Regen Res. 2019 Jan;14(1):149–55. doi: 10.4103/1673-5374.243720; CC BY-NC-SA.
Figure 10. Source: Microsurgical efficacy in 326 children with tethered cord syndrome: a retrospective analysis — Neural Regen Res. 2019 Jan;14(1):149–55. doi: 10.4103/1673-5374.243720; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Progressive neurological/urological decline, back/leg pain (worse with flexion/activity), bladder dysfunction, lower extremity weakness/sensory change, foot deformity, scoliosis (children)
- Pediatric: cutaneous stigmata (hairy patch, dimple/sinus, lipoma, hemangioma), delayed milestones, gait/urinary change
- Adult: pain-predominant, often after activity/trauma; or retethering after prior myelomeningocele repair
- Prior spinal dysraphism surgery (retethering)
Past Medical History
- Prior dysraphism repair (myelomeningocele, lipoma), prior untethering (retethering)
- Associated anomalies (Chiari II, syrinx, anorectal/GU anomalies — VACTERL), latex allergy
- Standard PMH
Imaging Review
MRI Lumbosacral Spine (T1, T2)
- Low-lying conus (below L2), thickened/fatty filum terminale (> 2 mm), filar lipoma
- Lipomyelomeningocele, intradural lipoma, dermal sinus tract, split cord malformation (diastematomyelia — bony/fibrous septum), syrinx
- Level of tethering, neural placode (post-repair), arachnoid adhesions
MRI Brain (if symptoms)
- Chiari II, hydrocephalus (dysraphism)
Urodynamics
- Baseline bladder function (pre- and post-op comparison)
Labs
- CBC, BMP, Coags, type and screen; latex precautions (dysraphism)
Neurological Examination
- Lower extremity motor/sensory/reflexes, sphincter tone, perianal sensation, gait, foot deformity, back/spine (stigmata, scoliosis), urological baseline
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: radiolucent spine-capable table selected for approach, imaging, instrumentation, patient size, and alignment goals; keep abdomen free for prone cases.
- OR setup: microscope, neuromonitoring, prone positioning pads, ultrasound/navigation if needed, dural repair materials, and CSF-leak management supplies.
- Special needs: Foley for detethering/bladder baseline, urology plan when neurogenic bladder is relevant, MAP/normothermia for cord perfusion, no long paralytic with MEPs, and meticulous skin-pressure protection.
- Immediate postop orders: motor/sensory/bladder checks, flat or activity restrictions per dural closure, wound/CSF-leak watch, pain/spasm regimen, MRI follow-up when indicated, and PT/urology follow-up.
Diagnosis & Indication
- Indication: Symptomatic tethered cord (progressive neuro/urologic decline, pain), or prophylactic in selected lipomas/asymptomatic (controversial — individualized)
- Goals: Release the tethering element, preserve neural function; for complex lipomas, debulk and reconstruct to reduce retethering
Position
- OR table/bed: radiolucent spine-capable table selected for approach, imaging, instrumentation, patient size, and alignment goals; keep abdomen free for prone cases.
- Prone, chest rolls, abdomen free, foam/horseshoe (peds — avoid pins in young), latex-free, IONM baseline (incl. EMG, BCR/sphincter); per level
Key Surgical Steps
- Level localization, midline incision (over prior scar if retethering), laminectomy/laminoplasty over the tethering level
- Midline durotomy under microscope, tack-up; careful — adhesions/placode immediately deep (retethering)
- Tight filum: identify the filum terminale (distinct from nerve roots — midline, often fatty, may have a vessel; confirm with stimulation — filum does not produce EMG/movement, nerve roots do); coagulate and divide the filum, confirm cut ends retract
- Lipoma/lipomyelomeningocele: debulk lipoma (CUSA/laser), dissect the lipoma-cord interface, untether the placode, reconstruct (pial closure) to reduce retethering; intraoperative neuromonitoring/mapping to distinguish functional neural tissue
- Split cord (diastematomyelia): resect the bony/fibrous median septum, untether
- Dermal sinus: excise the entire tract to its termination (intradural inclusion — dermoid risk)
- Continuous EMG/stimulation to protect functional roots; confirm release
- Watertight dural closure, sealant; multilayer closure
Critical Anatomy & Structures at Risk
- Functional nerve roots / conus / placode — distinguish from filum (stimulation mapping); injury → motor/sensory/sphincter deficit
- Sphincter/bladder innervation (S2-4) — urodynamic decline
- Dura — watertight closure (CSF leak/pseudomeningocele common)
- Retethering (reconstruction technique), inclusion dermoid (incomplete sinus excision)
Equipment
- Microscope, nerve stimulator / EMG mapping, CUSA (lipoma), micro-instruments, fine bipolar
- Ultrasound (localization), dural substitute, sealant, latex-free supplies
- Laser (selected, lipoma)
Monitoring
- EMG (lower extremity + anal sphincter), SSEPs, MEPs, bulbocavernosus reflex — essential to protect sacral function
Anesthesia
- No paralytic (IONM), prone precautions, latex-free, pediatric thermoregulation/fluids
Potential Complications
- Neurological/urological decline (root/conus/sphincter injury)
- CSF leak / pseudomeningocele (closure)
- Retethering (esp. lipomas — lifelong risk), inclusion dermoid
- Wound issues, infection, hydrocephalus (dysraphism)
Operative Note Template
Preoperative Diagnosis: Tethered cord syndrome ([tight filum / lipomyelomeningocele / retethering / split cord]) at [level]
Postoperative Diagnosis: Same
Procedure: [Level] laminectomy/laminoplasty for microsurgical tethered cord release [filum sectioning / lipoma debulking and untethering / septum resection]
Surgeon / Assistant: Anesthesia: General endotracheal, no paralytic, latex-free EBL / Fluids: Adjuncts: Microscope, ultrasound, nerve stimulator/EMG (lower extremity + anal sphincter), bulbocavernosus reflex, CUSA (lipoma) Implants: Dural substitute, sealant Complications: None
Indications: [Age]yo [M/F] [child/adult] with symptomatic tethered cord (progressive [neuro/urologic] decline, [back/leg pain]) from [etiology]. Risks (neuro/sphincter decline, CSF leak, retethering) discussed; latex precautions observed.
Description of Procedure: After consent and time-out, general anesthesia was induced (no paralytic, latex-free) and neuromonitoring with sphincter EMG/BCR established. The patient was positioned prone; the level was localized and a laminectomy/laminoplasty performed [over prior scar if retethering]. A midline durotomy was made under the microscope, with care given to adhesions immediately deep to the dura.
[Tight filum: the filum was identified (midline, fatty), confirmed non-functional by stimulation (no EMG), and coagulated and divided, with the cut ends retracting.] [Lipoma: the lipoma was debulked (CUSA), the lipoma-cord interface dissected, the placode untethered, and a pial reconstruction performed to reduce retethering.] [Split cord: the median septum was resected.] Continuous EMG/stimulation protected functional roots and sacral function. A watertight dural closure was performed with sealant.
Multilayer closure was completed. The patient was kept flat per protocol and transferred with neuro/sphincter monitoring.
Postoperative Plan
- Flat bed rest 24-72h (CSF leak prevention, esp. complex closures), prone/side positioning
- Neuro checks (motor/sensory/sphincter), wound/CSF leak monitoring
- MRI postop (release, residual lipoma), postop urodynamics (compare baseline)
- Latex-free, bowel/bladder management, urology follow-up
- DVT prophylaxis (mechanical; adults), rehab
- Counsel: goal is to halt progression (may not reverse established deficits); lifelong retethering surveillance
Chief-Level Case Review
Use these as the senior-level mental model for Tethered Cord Release:
- Decision point: Trajectory and hardware choice should follow the failure mode: obstruction, infection, overdrainage, loculation, slit ventricle, distal failure, or wrong pressure setting.
- Technical lever: Document the system: entry point, catheter target/depth, valve type and setting, distal site, antibiotic-impregnated hardware, and what imaging confirms placement.
- Bailout: Rescue plan is practical: poor CSF return, bloody CSF, malposition, distal access failure, abdominal/pleural complication, or inability to safely pass the catheter.
- Postop watch: Postop orders must be unambiguous: drain height/rate/max output, valve setting, clamp parameters, imaging, antibiotics, ICP/neuro checks, and overdrainage precautions.
Common Pimp Questions
Use these to pressure-test preparation for Tethered Cord Release:
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]