
Operative Approach: Posterior Cervical Approach (Laminectomy / Laminoplasty / Foraminotomy / Lateral Mass Fixation)
Case / Approach Snapshot
- Anatomy at risk: myelopathic cord, exiting roots, dorsal dura, epidural venous plexus, C2 semispinalis attachment, C7/T1 transition, lateral masses, vertebral artery in the transverse foramina, C2 pars/pedicle anatomy, and posterior tension-band musculature.
- Operative steps: position the myelopathic neck safely, localize levels, split the nuchal raphe in the midline, expose only the necessary lateral mass/facet anatomy, choose laminectomy/laminoplasty/foraminotomy/fusion strategy, place fixation with VA/root-aware trajectories, decompress without cord manipulation, and close the posterior fascial envelope securely.
- Rescue plans: wrong-level exposure, neuromonitoring change, C5 palsy risk, lateral mass or pedicle breach, vertebral artery injury, epidural bleeding, dural tear, post-laminectomy kyphosis, wound dehiscence/infection, and inadequate decompression in kyphotic alignment.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
CNS Video Library
AO Spine / Surgery Reference — posterior cervical · Neurosurgical Atlas — Spine · Radiopaedia — cervical stenosis · PubMed Central — lateral mass fixation
High-Yield Literature
- Microsurgical Neurovascular Anatomy of the Brain: The Posterior Circulation (Part II) — Giotta Lucifero A. Acta bio-medica : Atenei Parmensis 2021. PubMed
- Why the Craniovertebral Junction? — Visocchi M. Acta neurochirurgica. Supplement 2019. PubMed
- High anterior cervical approach to the clivus and foramen magnum: a microsurgical anatomy study — Russo VM. Neurosurgery 2011. PubMed
- Microsurgical cervical nerve root decompression by anterolateral approach — Bruneau M. Neurosurgery 2006. PubMed
- The Anterolateral Approach, Revisited for Benign Jugular Foramen Tumors With Predominant Extracranial Extension: Microsurgical Anatomy and Case Series (SevEN-012) — Park HH. Operative neurosurgery (Hagerstown, Md.) 2023. PubMed
- Anterior Microsurgical Approach to Ventral Lower Cervical Spine Meningiomas: Indications, Surgical Technique and Long Term Outcome — Fraioli MF. Technology in cancer research & treatment 2015. PubMed
- Applied anatomy of a minimally invasive muscle-splitting approach to posterior C1-C2 fusion: an anatomical feasibility study — Bodon G. Surgical and radiologic anatomy : SRA 2014. PubMed
- Cochlear implantation using posterior suprameatal approach — Répássy G. Ear, nose, & throat journal 2018. PubMed
- Microsurgical and endoscopic anatomy of the extended retrosigmoid inframeatal infratemporal approach — Colasanti R. Neurosurgery 2015. PubMed
- The posterior cervical transdural approach for retro-odontoid mass pseudotumor resection: report of three cases and discussion of the current literature — Schomacher M. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 2020. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
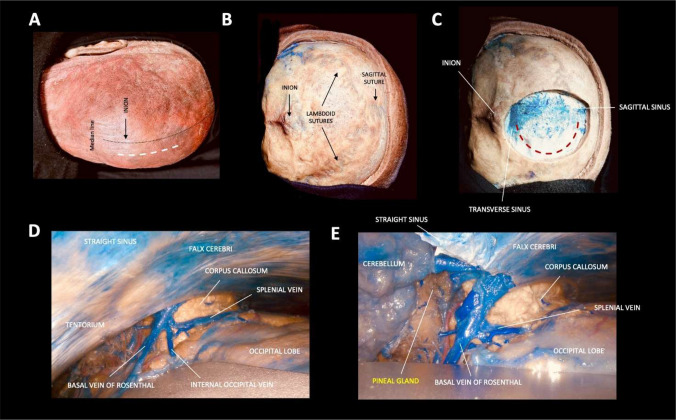 Fig. 2. A–E. Step-by-step dissection illustrating the occipital interhemispheric transtentorial (OITA) approach Source: What is the best surgical approach for Pineal Region Tumors? A systematic literature review and anatomical comparative study — Child’s Nervous System 2026; CC BY.
Fig. 2. A–E. Step-by-step dissection illustrating the occipital interhemispheric transtentorial (OITA) approach Source: What is the best surgical approach for Pineal Region Tumors? A systematic literature review and anatomical comparative study — Child’s Nervous System 2026; CC BY.
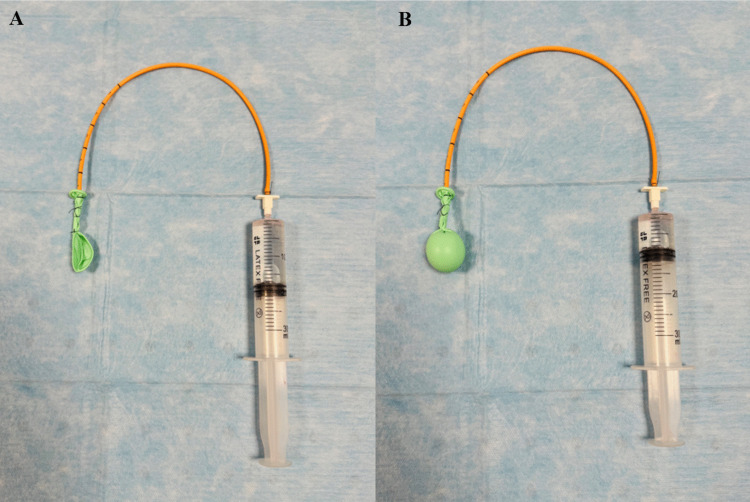 Fig. 3. Illustration of the water-balloon technique simulating a pineal-region tumor. The latex balloon attached to a ventricular catheter is shown deflated (A) and inflated with water and… Source: What is the best surgical approach for Pineal Region Tumors? A systematic literature review and anatomical comparative study — Child’s Nervous System 2026; CC BY.
Fig. 3. Illustration of the water-balloon technique simulating a pineal-region tumor. The latex balloon attached to a ventricular catheter is shown deflated (A) and inflated with water and… Source: What is the best surgical approach for Pineal Region Tumors? A systematic literature review and anatomical comparative study — Child’s Nervous System 2026; CC BY.
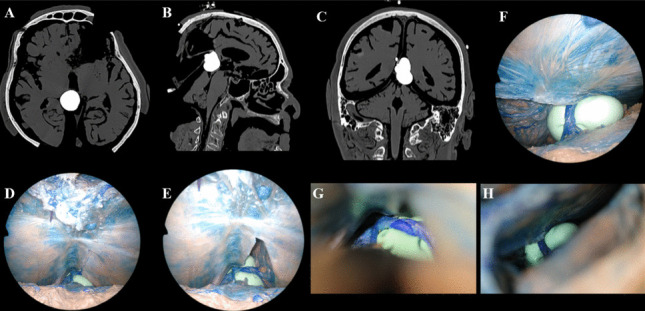 Fig. 4. A–H. Tumor simulation in Head 1 demonstrating exposure with the SCIT and OITA approaches Source: What is the best surgical approach for Pineal Region Tumors? A systematic literature review and anatomical comparative study — Child’s Nervous System 2026; CC BY.
Fig. 4. A–H. Tumor simulation in Head 1 demonstrating exposure with the SCIT and OITA approaches Source: What is the best surgical approach for Pineal Region Tumors? A systematic literature review and anatomical comparative study — Child’s Nervous System 2026; CC BY.
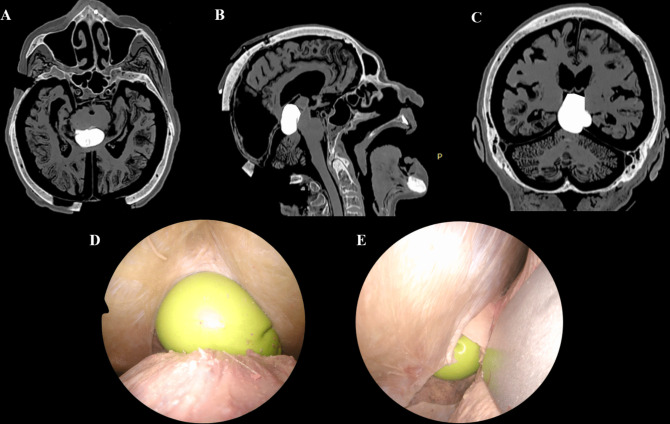 Fig. 5. A–E. Tumor simulation in Head 2 demonstrating exposure with the SCIT and OITA approaches Source: What is the best surgical approach for Pineal Region Tumors? A systematic literature review and anatomical comparative study — Child’s Nervous System 2026; CC BY.
Fig. 5. A–E. Tumor simulation in Head 2 demonstrating exposure with the SCIT and OITA approaches Source: What is the best surgical approach for Pineal Region Tumors? A systematic literature review and anatomical comparative study — Child’s Nervous System 2026; CC BY.
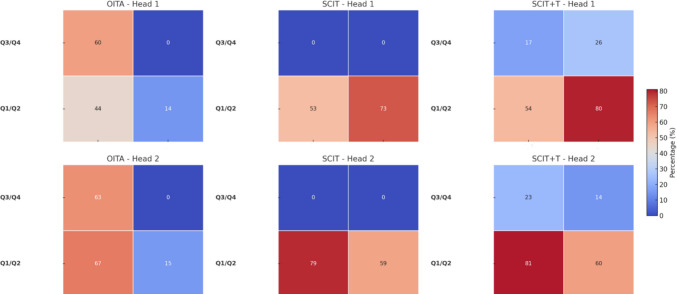 Fig. 7. Heatmap representation of mean exposure volumes across surgical approaches and anatomical quadrants Source: What is the best surgical approach for Pineal Region Tumors? A systematic literature review and anatomical comparative study — Child’s Nervous System 2026; CC BY.
Fig. 7. Heatmap representation of mean exposure volumes across surgical approaches and anatomical quadrants Source: What is the best surgical approach for Pineal Region Tumors? A systematic literature review and anatomical comparative study — Child’s Nervous System 2026; CC BY.
 Fig. 2. After the cervical carotid is clamped at the neck, a temporary clip is applied distal to the aneurysm Source: Paraclinoid aneurysm clipping: how I do it — Acta Neurochirurgica 2025; CC BY.
Fig. 2. After the cervical carotid is clamped at the neck, a temporary clip is applied distal to the aneurysm Source: Paraclinoid aneurysm clipping: how I do it — Acta Neurochirurgica 2025; CC BY.
 Fig. 1. Artist’s illustration showing the exposure of the anterolateral brainstem, vertebral artery, basilar region, and the lower cranial nerves afforded by the far-lateral approach. ©… Source: History and evolution of the far-lateral approach in neurosurgery — Acta Neurochirurgica 2026; CC BY-NC-ND.
Fig. 1. Artist’s illustration showing the exposure of the anterolateral brainstem, vertebral artery, basilar region, and the lower cranial nerves afforded by the far-lateral approach. ©… Source: History and evolution of the far-lateral approach in neurosurgery — Acta Neurochirurgica 2026; CC BY-NC-ND.
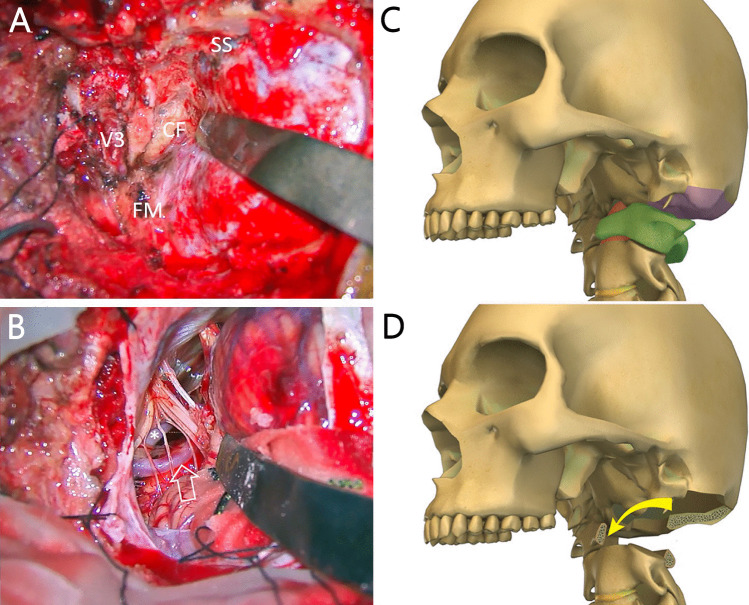 Fig. 5. Variation in bony exposure of the far-lateral approach (FLA). This figure demonstrates adaptations in bony exposure to different targets along the craniovertebral junction. A, B… Source: History and evolution of the far-lateral approach in neurosurgery — Acta Neurochirurgica 2026; CC BY-NC-ND.
Fig. 5. Variation in bony exposure of the far-lateral approach (FLA). This figure demonstrates adaptations in bony exposure to different targets along the craniovertebral junction. A, B… Source: History and evolution of the far-lateral approach in neurosurgery — Acta Neurochirurgica 2026; CC BY-NC-ND.
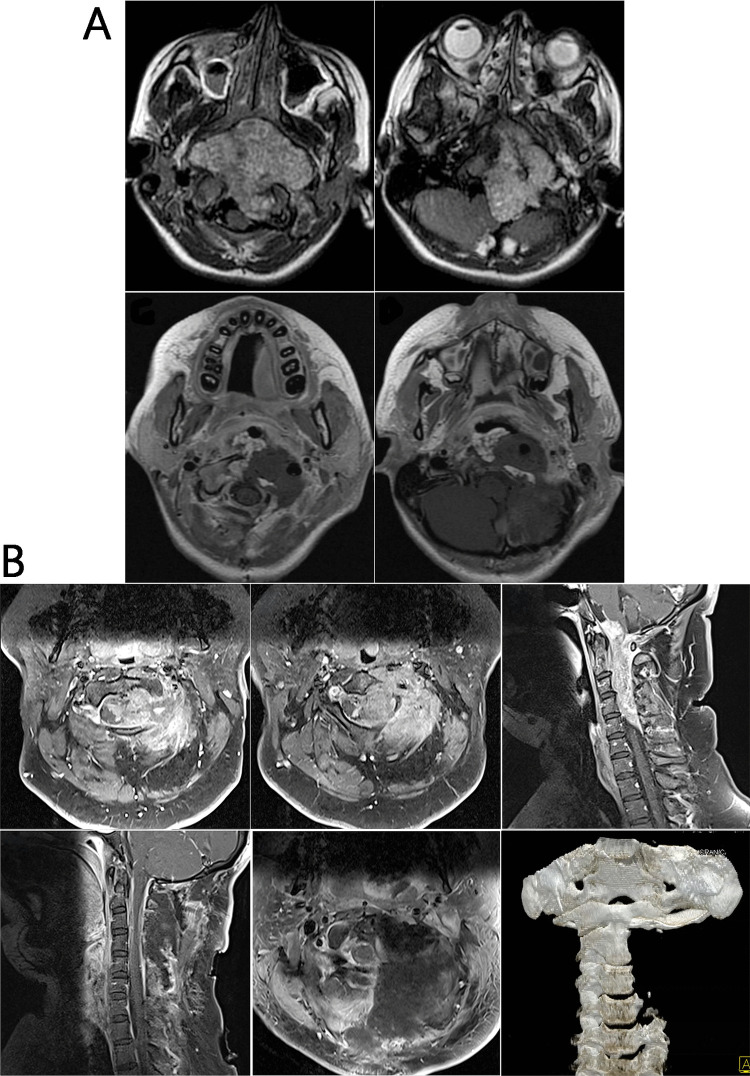 Fig. 6. Examples of cases in which extensions of the far-lateral approach (FLA) are utilized. A This adolescent patient had a massive clival chordoma with brainstem compression. The ELTO… Source: History and evolution of the far-lateral approach in neurosurgery — Acta Neurochirurgica 2026; CC BY-NC-ND.
Fig. 6. Examples of cases in which extensions of the far-lateral approach (FLA) are utilized. A This adolescent patient had a massive clival chordoma with brainstem compression. The ELTO… Source: History and evolution of the far-lateral approach in neurosurgery — Acta Neurochirurgica 2026; CC BY-NC-ND.
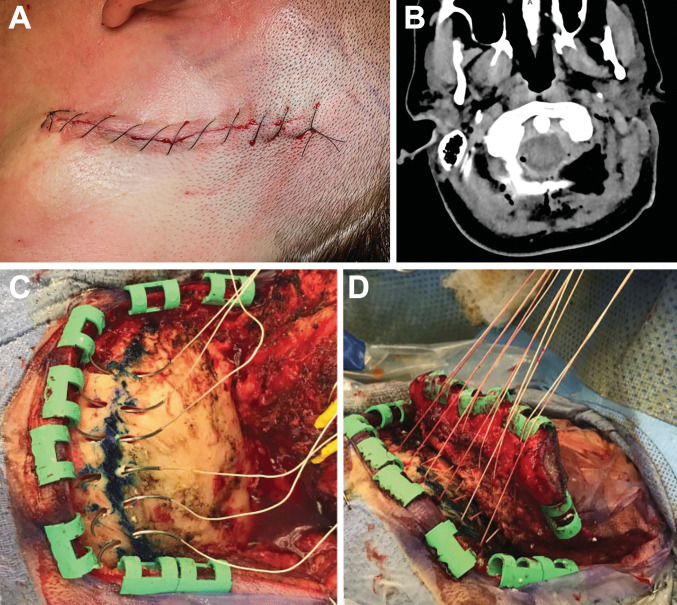 Fig. 7. Variation in closure technique following the far-lateral approach. A Postoperative photograph showing a curvilinear far lateral skin closure using running nylon sutures. B Axial CT image… Source: History and evolution of the far-lateral approach in neurosurgery — Acta Neurochirurgica 2026; CC BY-NC-ND.
Fig. 7. Variation in closure technique following the far-lateral approach. A Postoperative photograph showing a curvilinear far lateral skin closure using running nylon sutures. B Axial CT image… Source: History and evolution of the far-lateral approach in neurosurgery — Acta Neurochirurgica 2026; CC BY-NC-ND.
The posterior cervical approach is the midline corridor to the posterior elements and dorsal cord/roots of the cervical spine. Through the avascular nuchal raphe it exposes the laminae, facets, and lateral masses for laminectomy, laminoplasty, laminoforaminotomy, and posterior instrumented fusion (lateral mass / pedicle screws). It is the approach for multilevel myelopathy with preserved/lordotic alignment, posterior compression, dorsal tumors, and posterior stabilization — chosen over the anterior approach when disease is multilevel/dorsal or when posterior tension-band reconstruction is required.
General Considerations
- What it accesses: laminae, spinous processes, facet joints, lateral masses, the dorsal dura/cord and exiting roots (via foraminotomy), C1 posterior arch and C2 to the cervicothoracic junction.
- Decompression vs decompression + fusion: posterior decompression (laminectomy/laminoplasty) relieves dorsal/multilevel compression; add instrumented fusion when there is instability, kyphosis risk, or after wide facet resection. Laminoplasty preserves the posterior tension band and motion (lower post-laminectomy kyphosis risk) and is favored in younger patients with lordotic alignment.
- Alignment is the key selection rule: posterior decompression relies on the cord drifting dorsally away from anterior compression — it works in lordosis/neutral alignment but fails in fixed kyphosis (the cord stays draped over the front), where an anterior or combined approach is needed.
Indications
- Multilevel cervical spondylotic myelopathy / OPLL with lordotic-neutral alignment → posterior cervical laminectomy & fusion, laminoplasty
- Foraminal radiculopathy (soft lateral disc/foraminal stenosis) → posterior cervical foraminotomy
- Trauma / instability (facet fracture-dislocation) → subaxial cervical fracture; CVJ → occipitocervical fusion
- Dorsal intradural/extradural tumors, infection
Posterior Cervical Decision Table
| Problem | Preferred posterior option | Key caveat |
|---|---|---|
| Multilevel myelopathy, lordotic/neutral alignment | Laminoplasty or laminectomy/fusion | Posterior decompression depends on dorsal cord drift |
| Multilevel myelopathy with instability, kyphosis risk, or neck pain | Laminectomy + fusion | Preserve adjacent facets and restore alignment |
| Young patient with preserved lordosis and motion priority | Laminoplasty | Avoid if significant axial pain/instability/kyphosis |
| Unilateral radiculopathy from foraminal stenosis/lateral disc | Posterior foraminotomy | Avoid excessive facet removal; preserve stability |
| Trauma/facet dislocation/instability | Posterior fixation ± reduction/decompression | CT/CTA defines screw choices and VA risk |
| Fixed kyphosis with anterior compression | Anterior or combined approach | Posterior-only decompression may fail |
Relevant Surgical Anatomy
- Midline raphe / ligamentum nuchae: the avascular plane — staying exactly midline minimizes muscle bleeding and denervation.
- Paraspinal muscles (trapezius, splenius, semispinalis cervicis, multifidus) — elevated subperiosteally; the semispinalis insertion on C2 is preserved when possible (its detachment contributes to post-op kyphosis/pain).
- Lateral mass: the rhomboid of bone between the superior/inferior facets — the screw target (entry ~1 mm medial/inferior to its center; trajectory lateral and superior to avoid the vertebral artery and nerve root — Magerl/An/Roy-Camille variants).
- Vertebral artery: in the foramen transversarium, ventral and medial to the lateral mass — at risk with errant screw trajectory; C1 lateral mass (venous plexus, C2 root/ganglion) and C2 pars/pedicle have their own VA relationships; C7 often takes a pedicle screw (small lateral mass).
- Nerve roots & dura at the laminae/foramina; the cord beneath (no retraction).
Preoperative Evaluation
- MRI (levels, cord signal, dorsal vs ventral compression) and CT (bony anatomy, OPLL, facet/lateral mass size); assess alignment (lordosis vs kyphosis) — decisive for posterior vs anterior.
- CTA / review vertebral artery dominance and anomalies (high-riding VA at C2) before planning C1–C2/pars screws.
- Baseline myelopathy exam; plan instrumentation levels and whether laminoplasty vs laminectomy+fusion.
Preoperative Planning Checklist
- Document Nurick/mJOA-style myelopathy severity, hand function, gait, bowel/bladder symptoms, and baseline deltoid/biceps strength for C5 palsy comparison.
- Review standing or dynamic films for lordosis, instability, and C2-C7 sagittal vertical axis; supine MRI alone can hide kyphotic failure risk.
- On CT, size lateral masses, identify anomalous/hypoplastic pedicles, facet fractures, OPLL, and prior fusion/laminectomy defects.
- For C1-C2/C2 screws, evaluate vertebral artery course, high-riding VA, pars height, pedicle width, and C2 ganglion/venous plexus exposure.
- Decide whether the construct should stop at C7 or cross the cervicothoracic junction; stopping at a weak transition can invite junctional failure in selected patients.
Logistics, OR Setup & Orders
- OR table/bed: Wilson frame, Andrews/knee-chest frame, or Jackson/open-frame table by surgeon preference; flexion opens the interlaminar window and the abdomen must hang free.
- OR setup: Jackson/radiolucent spine table or approach-specific lateral/anterior setup, C-arm/O-arm/navigation availability, microscope/loupes, neuromonitoring leads before positioning, and implant trays opened only after final level/plan confirmation.
- Special needs: arterial line and Foley for long instrumented cases, type/screen or crossmatch for deformity/corpectomy/trauma, antibiotic redosing plan, MAP support for SCI/myelopathy, and no long paralytic when MEPs are needed.
- Immediate postop orders: neuro checks focused on myotomes/sensory level, postop CT/X-rays per construct, brace/activity orders, drain output thresholds, DVT prophylaxis timing, dysphagia/airway monitoring for anterior cervical cases, and rehab mobilization plan.
Anesthesia & Neuromonitoring
- GA, prone; SSEP/MEP and EMG (myelopathy/instrumentation); no long-acting paralytic with MEPs. Careful prone positioning of the myelopathic neck (neutral, avoid hyperextension); MAP support for the compressed cord.
Positioning
- OR table/bed: Wilson frame, Andrews/knee-chest frame, or Jackson/open-frame table by surgeon preference; flexion opens the interlaminar window and the abdomen must hang free.
- Prone, head in Mayfield 3-pin (or a prone headrest), neck neutral (slight flexion opens interlaminar spaces for laminectomy; avoid flexion in instability), reverse Trendelenburg to lower venous pressure/bleeding and keep the field horizontal.
- Tape shoulders down for lower-level fluoroscopy; chest rolls/Wilson-type support; abdomen free; eyes/face protected (prone ION risk). Re-check IONM after final positioning.
Incision & Soft-Tissue Dissection
- Midline incision over the target levels; cut through skin and subcutaneous tissue to the ligamentum nuchae, then split the avascular midline raphe down to the spinous processes — staying precisely midline limits blood loss.
- Subperiosteal dissection of the paraspinal muscles off the laminae out to the lateral masses (only as far lateral as the construct needs; preserve facet capsules at non-fused levels and the C2 semispinalis insertion when possible). Self-retaining retractors.
- Fluoroscopic level localization before bone work.
→ proceed to the procedure-specific steps (laminectomy/fusion, laminoplasty, foraminotomy).
Lateral Mass / Posterior Fixation
- Lateral mass screws (C3–C6) via a Magerl/An-type trajectory: entry ~1 mm medial and inferior to the lateral-mass center, angled ~25–30° laterally and ~15–30° superiorly (parallel to the facet) to stay clear of the vertebral artery (medial/ventral) and nerve root (inferolateral). C7/C2 often take pedicle screws; C1 a lateral-mass screw; rods connect the construct after decortication and grafting.
Decompression and Fixation Sequence
- Confirm level with fluoroscopy after exposure and again before irreversible decompression.
- Place pilot holes/screws before decompression when anatomy is stable and bleeding is controlled; in severe stenosis, avoid maneuvers that transmit force to the cord.
- Perform troughs/laminectomy with a drill until the inner cortex is thin; lift bone away from dura rather than levering into the canal.
- In laminoplasty, create a complete opening-side trough and controlled hinge side; avoid greenstick fracture into the canal.
- In foraminotomy, remove the minimum medial facet needed for root decompression and preserve at least half of the facet whenever possible.
- Decorticate fusion surfaces, place graft, contour rods without excessive lordosis/extension, and check final alignment and screw position.
Intraoperative Rescue
- MEP/SSEP decline: pause, raise MAP, check neck position/anesthesia, remove compressive bone/hematoma, reverse correction/distraction, and obtain imaging if hardware is suspect.
- C5 palsy concern: verify no foraminal tethering at C4-C5/C5 root, avoid over-distraction, and consider targeted foraminotomy when high risk.
- Lateral mass breach: redirect immediately; do not accept a medial/inferior trajectory that threatens root/VA.
- Vertebral artery bleeding: maintain tamponade, avoid blind bipolar, pack with hemostatic material, obtain vascular help/endovascular backup, and preserve neurologic perfusion.
- Dural tear: expose enough dura for repair, primary suture when possible, patch/sealant adjunct, Valsalva, and drain strategy tailored to repair quality.
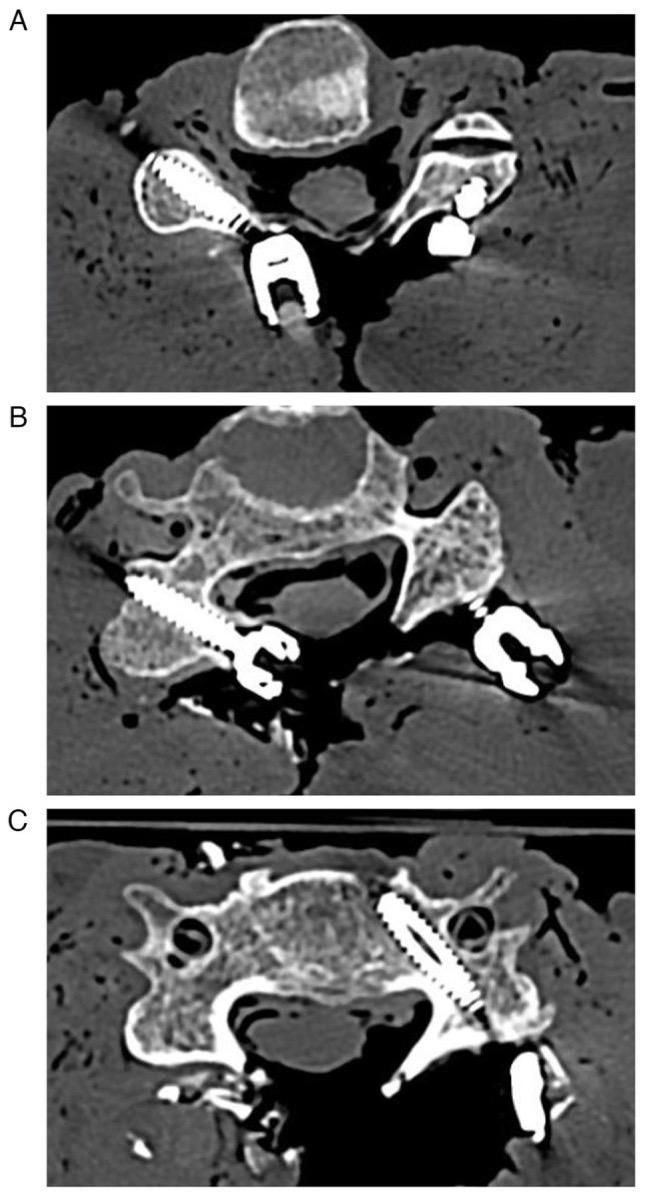
Attallah M, et al. *Med Int. 2024;4(4):159 — CC BY 4.0. Axial CT illustrating lateral-mass screw placement and trajectory relative to the foramen transversarium.*
Closure
- Meticulous hemostasis; layered closure of the deep fascia/muscle, then fascia, subcutaneous, skin — the posterior cervical wound is closure-dependent for infection/dehiscence prevention; a subfascial drain is commonly used. Re-approximate the nuchal musculature/C2 attachments.
Nuances & Pitfalls (surgeon-level)
- Stay midline in the raphe — straying into muscle causes troublesome bleeding and denervation atrophy/pain.
- Vertebral artery & nerve root are the screw hazards — respect the lateral/superior trajectory; check CT for a high-riding VA before C2 pars/pedicle screws.
- Post-laminectomy kyphosis: laminectomy without fusion in a young or kyphosis-prone patient risks swan-neck deformity — favor laminoplasty or laminectomy + fusion; preserve the C2/C7 muscular attachments.
- C5 palsy (deltoid/biceps) after posterior decompression — counsel; usually recovers; foraminotomy/avoiding over-distraction may reduce it.
- Alignment rule: don’t decompress posteriorly in fixed kyphosis (cord won’t drift back).
- Prone positioning: protect eyes (ischemic optic neuropathy), keep the myelopathic neck neutral, lower venous pressure (reverse Trendelenburg) to reduce epidural bleeding.
Complications
C5 palsy; post-laminectomy kyphosis; vertebral artery or nerve root injury (screws); dural tear/CSF leak; wound infection / dehiscence (higher than anterior); axial neck pain; pseudarthrosis; epidural hematoma; positioning injuries (ION, pressure).
Cross-links
- Procedures: posterior cervical laminectomy & fusion · laminoplasty · posterior cervical foraminotomy · occipitocervical fusion · subaxial cervical fracture
- Related corridors: anterior-cervical-approach.md · posterior-thoracolumbar-approach.md
Figure Use & Attribution
About the figures. Copyrighted operative figures/videos are linked (Neurosurgical Atlas, AO Spine / Surgery Reference); embedded images are public-domain (Gray’s Anatomy) or CC‑BY (open-access), credited beneath each image. See media-sources.md and figures/CREDITS.md.
Technique references: AO Spine / Surgery Reference — Posterior cervical · Neurosurgical Atlas — Spine · Radiopaedia — cervical
Chief-Level Corridor Review
Use these as the senior-level mental model for Posterior Cervical Approach (Laminectomy / Laminoplasty / Foraminotomy / Lateral Mass Fixation):
- Decision point: Define the exposure goal before incision: target, working angles, proximal/distal control, and the structure that cannot tolerate retraction.
- Technical lever: Know the first irreversible step: bone removal, dural opening, vascular control, or muscle/fascial division that commits the corridor.
- Bailout: Verbalize the bailout: extend exposure, change trajectory, add CSF drainage, obtain proximal control, convert to a larger corridor, or stop for imaging.
- Postop watch: Protect closure from the start: vascularized tissue, watertight dural/reconstruction plan, dead-space control, and drain strategy should be chosen before the final intradural step.
Common Pimp Questions
Use these to pressure-test preparation for Posterior Cervical Approach (Laminectomy / Laminoplasty / Foraminotomy / Lateral Mass Fixation):
- What patient position and head rotation make gravity work for this corridor?
- What named nerve, vessel, sinus, or muscle/fascial plane is most commonly injured?
- What bone work or soft-tissue step creates the exposure rather than simply using more retraction?
- What is the bailout if exposure is inadequate, bleeding occurs, or the brain is tight?
- What closure maneuver prevents the signature complication of this approach?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Exact head rotation/flexion/extension and pin placement: [attending-specific]
- Skin incision length, flap type, and muscle/fascial preservation technique: [attending-specific]
- Drill, rongeur, endoscope, microscope, retractor, and navigation preferences: [attending-specific]
- Drain use, closure materials, watertightness threshold, and postop imaging routine: [attending-specific]
Case Guides Using This Approach
- Cervical Laminoplasty
- Odontoid (Type II) Fracture Fixation
- Penetrating Spine Injury (Gunshot / Stab) Management
- Posterior Cervical Foraminotomy (Laminoforaminotomy)
- Posterior Cervical Laminectomy and Fusion
- Spinal Arteriovenous Malformation (Intramedullary / Perimedullary)
- Spinal Cord Cavernous Malformation Resection
- Spinal Epidural Abscess — Decompression & Drainage
- Subaxial Cervical Spine Fracture / Dislocation Fixation
- Syringomyelia — Management / Syringosubarachnoid Shunt
- Traumatic Central Cord Syndrome
References
- Roy-Camille R, Saillant G, Mazel C. Internal fixation of the unstable cervical spine by a posterior osteosynthesis with plates and screws. (lateral mass technique).
- Magerl F, Seemann PS. Stable posterior fusion of the atlas and axis by transarticular screw fixation. 1987.
- An HS, et al. Anatomic considerations for plate-screw fixation of the cervical spine. Spine. 1991.
- AO Foundation. Posterior approach and lateral mass fixation, cervical spine. AO Spine / Surgery Reference. link
- Attallah M, et al. (lateral mass screw biomechanics / trajectory). Med Int. 2024;4(4):159. CC BY 4.0. (figure embedded above) — PMC11097134