
Case Prep: Vertebral Osteomyelitis / Discitis — Surgical Management
Case / Approach Snapshot
- Anatomy at risk: the named neural, vascular, bony, CSF, and soft-tissue structures that determine the safe corridor and likely morbidity.
- Operative steps: confirm indication and imaging, position and expose deliberately, complete the core surgical maneuver, verify the result, and close with a complication-prevention plan; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: bleeding, neurologic change, wrong target or level, CSF leak, infection, hardware or reconstruction failure, and a staged or alternate-treatment plan.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [pyogenic/tuberculous] vertebral osteomyelitis-discitis at [T_/L_] [with epidural abscess / deformity / instability / deficit] planned for [biopsy / debridement, decompression, and reconstruction].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior thoracolumbar approach and transthoracic approach — posterior stabilization versus anterior debridement/reconstruction depends on level and column failure.
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Microbial etiology of vertebral osteomyelitis/discitis amid the opioid epidemic — Ammerman SA. Journal of neurosurgery. Spine 2024. PubMed
- Posterior Fixation Without Debridement for Vertebral Body Osteomyelitis and Discitis: A 10-Year Retrospective Review — Lindsay SE. International journal of spine surgery 2023. PubMed
- Clinical prediction for surgical versus nonsurgical interventions in patients with vertebral osteomyelitis and discitis — Lee J. Journal of spine surgery (Hong Kong) 2024. PubMed
- Vertebral Osteomyelitis, Discitis, and Epidural Abscess: A Rare Complication of Cardiobacterium Endocarditis — Yadava SK. Journal of investigative medicine high impact case reports 2018. PubMed
- Management Outcomes after Image-Guided Percutaneous Biopsy for Suspected Vertebral Osteomyelitis-Discitis — Malik DG. AJNR. American journal of neuroradiology 2025. PubMed
- Preclinical models of vertebral osteomyelitis and associated infections: Current models and recommendations for study design — Joyce K. JOR spine 2021. PubMed
- Enterobacter cloacae as sole organism responsible for vertebral osteomyelitis/discitis and vertebral collapse in a patient with intravenous drug abuse — Khine S. BMJ case reports 2023. PubMed
- Management of Refractory Post-operative Osteomyelitis and Discitis: A Case Report — DeLong CA. Cureus 2024. PubMed
- Case report: vertebral osteomyelitis/discitis as a complication of Capnocytophaga canimorsus bacteremia — Nelson MJ. The Journal of emergency medicine 2008. PubMed
- Group B Streptococcus vertebral osteomyelitis-discitis in an immunocompetent adolescent — Trehan I. The Pediatric infectious disease journal 2009. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
 Figure 1.. Magnetic resonance imaging: Discitis/osteomyelitis at L4-L5 with preservation of vertebral body height but an extension of infection into the epidural space, as well as anteriorly and… Source: Vertebral Osteomyelitis, Discitis, and Epidural Abscess: A Rare Complication of Cardiobacterium Endocarditis — Journal of Investigative Medicine High Impact Case Reports 2018; CC BY.
Figure 1.. Magnetic resonance imaging: Discitis/osteomyelitis at L4-L5 with preservation of vertebral body height but an extension of infection into the epidural space, as well as anteriorly and… Source: Vertebral Osteomyelitis, Discitis, and Epidural Abscess: A Rare Complication of Cardiobacterium Endocarditis — Journal of Investigative Medicine High Impact Case Reports 2018; CC BY.
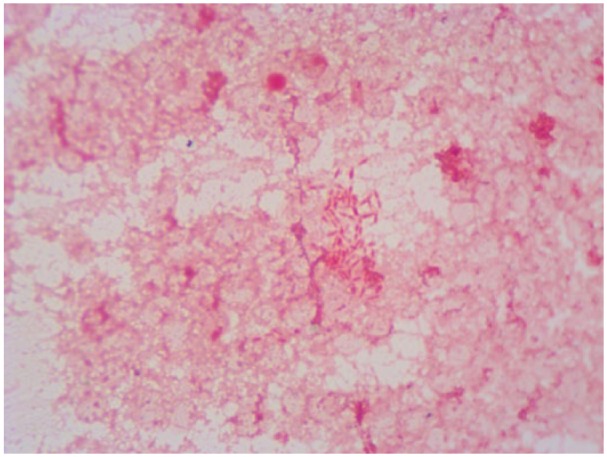 Figure 2.. Gram staining of vertebral biopsy, gram-negative rods. Source: Vertebral Osteomyelitis, Discitis, and Epidural Abscess: A Rare Complication of Cardiobacterium Endocarditis — Journal of Investigative Medicine High Impact Case Reports 2018; CC BY.
Figure 2.. Gram staining of vertebral biopsy, gram-negative rods. Source: Vertebral Osteomyelitis, Discitis, and Epidural Abscess: A Rare Complication of Cardiobacterium Endocarditis — Journal of Investigative Medicine High Impact Case Reports 2018; CC BY.
 Figure 3. Source: Vertebral Osteomyelitis, Discitis, and Epidural Abscess: A Rare Complication of Cardiobacterium Endocarditis — J Investig Med High Impact Case Rep. 2018 Oct 28;6:2324709618807504. doi: 10.1177/2324709618807504; CC BY.
Figure 3. Source: Vertebral Osteomyelitis, Discitis, and Epidural Abscess: A Rare Complication of Cardiobacterium Endocarditis — J Investig Med High Impact Case Rep. 2018 Oct 28;6:2324709618807504. doi: 10.1177/2324709618807504; CC BY.
 Fig. 1. At time of admission- Contrast Enhanced Computed Tomography (CECT) pelvis-axial section showing hypo dense collection concerning for bilateral psoas abscess (as black arrow). Source: A rare case of Streptococcus pyogenes vertebral osteomyelitis in a young, immunocompetent male — IDCases 2025; CC BY-NC-ND.
Fig. 1. At time of admission- Contrast Enhanced Computed Tomography (CECT) pelvis-axial section showing hypo dense collection concerning for bilateral psoas abscess (as black arrow). Source: A rare case of Streptococcus pyogenes vertebral osteomyelitis in a young, immunocompetent male — IDCases 2025; CC BY-NC-ND.
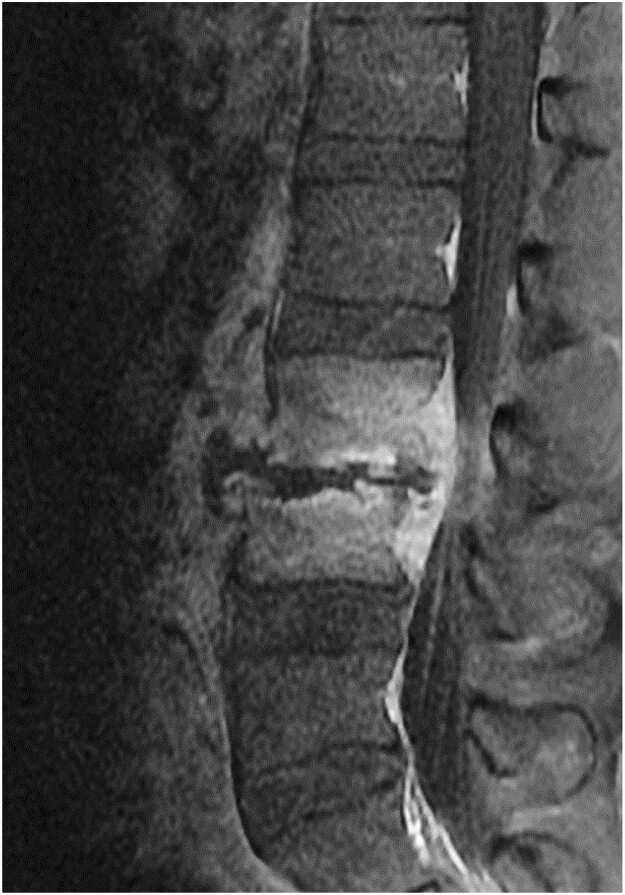 Fig. 2. Magnetic Resonance Imaging (MRI) lumbar spine with contrast –sagittal section revealing cortical erosions L3-L4 vertebral bodies with anterior epidural collection. Source: A rare case of Streptococcus pyogenes vertebral osteomyelitis in a young, immunocompetent male — IDCases 2025; CC BY-NC-ND.
Fig. 2. Magnetic Resonance Imaging (MRI) lumbar spine with contrast –sagittal section revealing cortical erosions L3-L4 vertebral bodies with anterior epidural collection. Source: A rare case of Streptococcus pyogenes vertebral osteomyelitis in a young, immunocompetent male — IDCases 2025; CC BY-NC-ND.
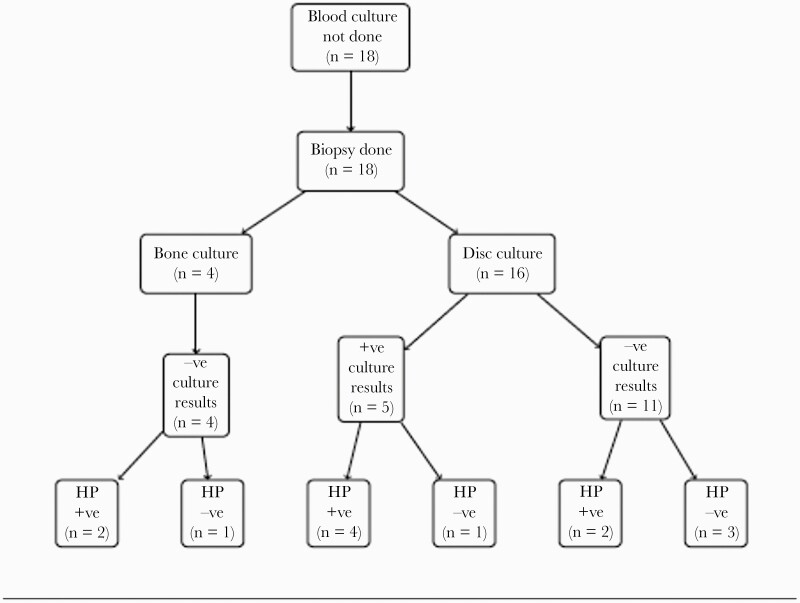 Figure 2.. Patient biopsy findings in a subset of patients without blood cultures obtained. Abbreviations: -ve, negative; +ve, positive; HP, histopathology. Source: Culture Yield in the Diagnosis of Native Vertebral Osteomyelitis: A Single Tertiary Center Retrospective Case Series With Literature Review — Open Forum Infectious Diseases 2022; CC BY-NC-ND.
Figure 2.. Patient biopsy findings in a subset of patients without blood cultures obtained. Abbreviations: -ve, negative; +ve, positive; HP, histopathology. Source: Culture Yield in the Diagnosis of Native Vertebral Osteomyelitis: A Single Tertiary Center Retrospective Case Series With Literature Review — Open Forum Infectious Diseases 2022; CC BY-NC-ND.
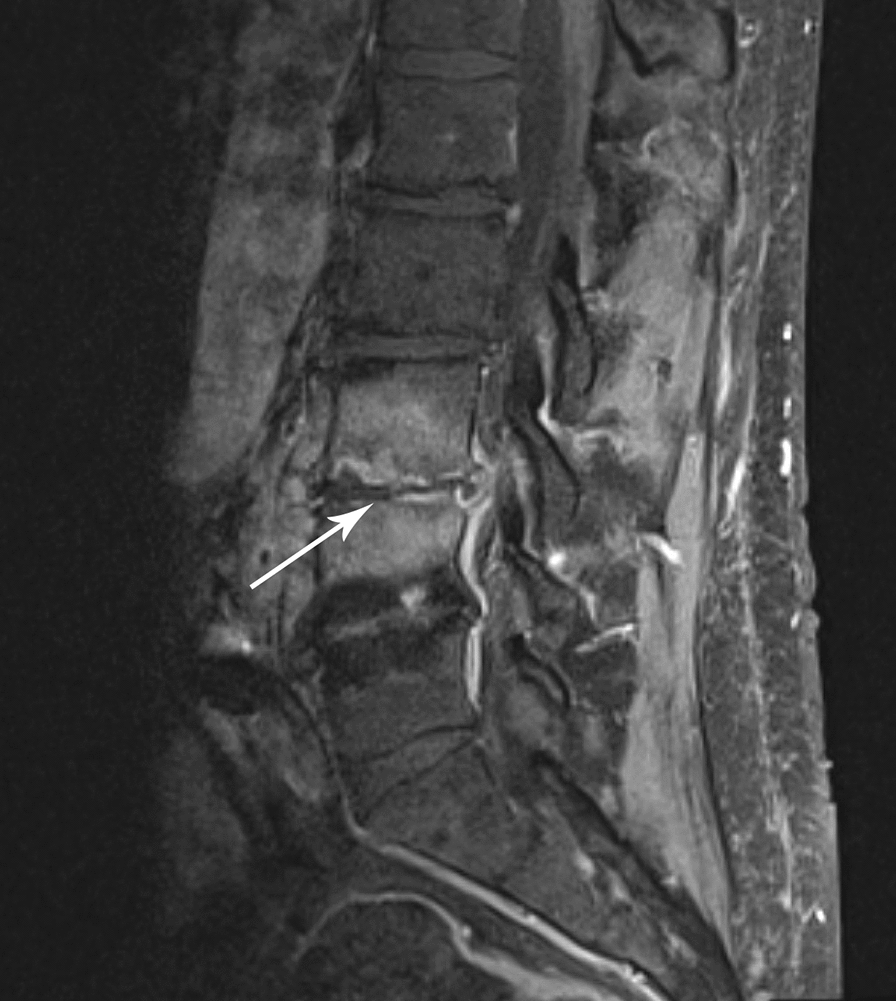 Fig. 1. Magnetic resonance imaging (MRI) of the lumbar spine demonstrating discitis and vertebral osteomyelitis. T1 post-contrast sagittal MRI demonstrating enhancement at the L3–4… Source: An unusual case of Cardiobacterium valvarum causing aortic endograft infection and osteomyelitis — Annals of Clinical Microbiology and Antimicrobials 2021; CC BY.
Fig. 1. Magnetic resonance imaging (MRI) of the lumbar spine demonstrating discitis and vertebral osteomyelitis. T1 post-contrast sagittal MRI demonstrating enhancement at the L3–4… Source: An unusual case of Cardiobacterium valvarum causing aortic endograft infection and osteomyelitis — Annals of Clinical Microbiology and Antimicrobials 2021; CC BY.
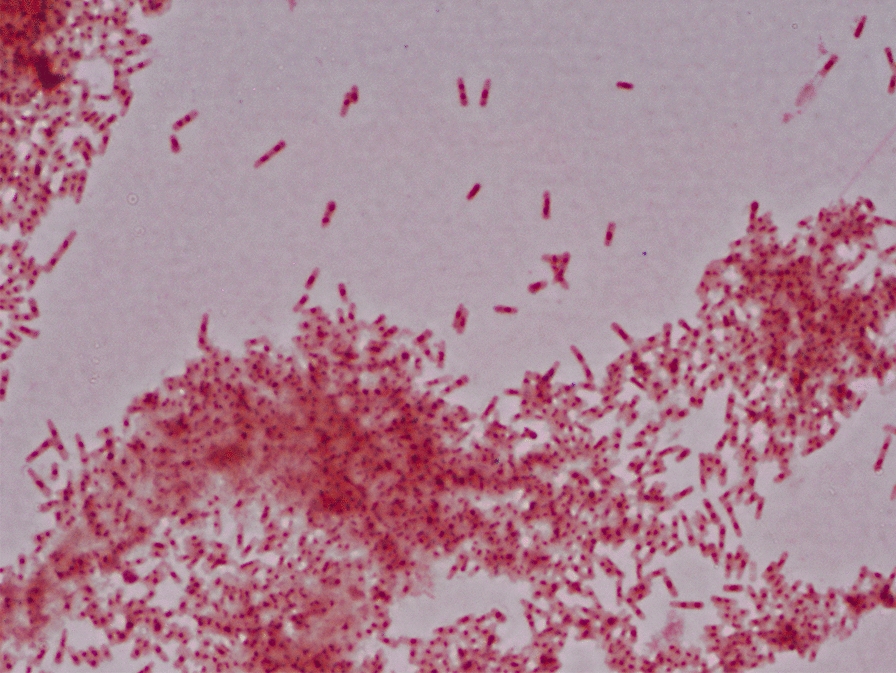 Fig. 2. Gram staining. Microscopic morphology in gram staining of blood culture after 96 h of aerobic incubation at 37 °C demonstrating bipolar-staining gram-negative bacilli. 16S ribosomal RNA… Source: An unusual case of Cardiobacterium valvarum causing aortic endograft infection and osteomyelitis — Annals of Clinical Microbiology and Antimicrobials 2021; CC BY.
Fig. 2. Gram staining. Microscopic morphology in gram staining of blood culture after 96 h of aerobic incubation at 37 °C demonstrating bipolar-staining gram-negative bacilli. 16S ribosomal RNA… Source: An unusual case of Cardiobacterium valvarum causing aortic endograft infection and osteomyelitis — Annals of Clinical Microbiology and Antimicrobials 2021; CC BY.
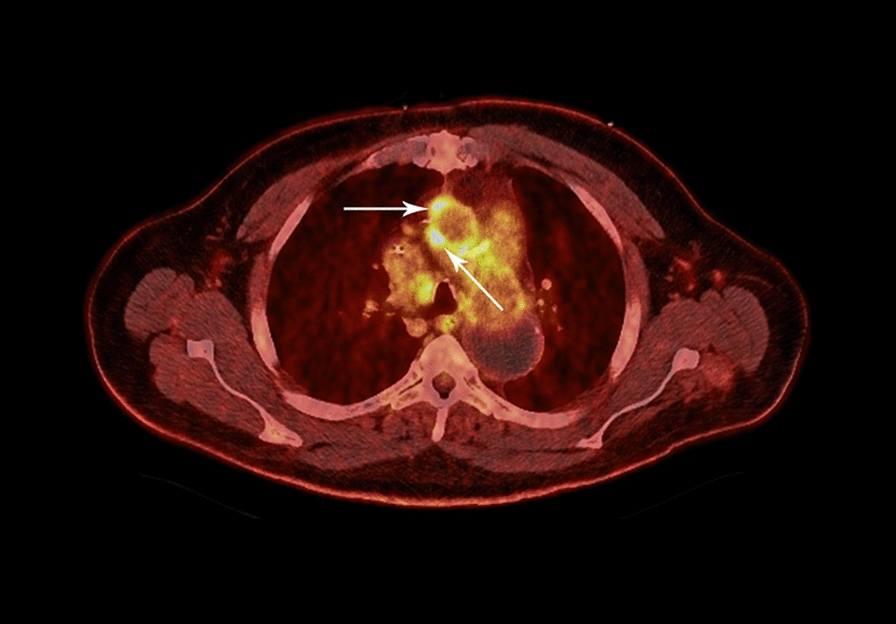 Fig. 3. Positron emission tomography–computed tomography (PET/CT) of the chest. Hypermetabolic soft tissue (arrows) along the right lateral and anterior aspect of the ascending aortic endograft… Source: An unusual case of Cardiobacterium valvarum causing aortic endograft infection and osteomyelitis — Annals of Clinical Microbiology and Antimicrobials 2021; CC BY.
Fig. 3. Positron emission tomography–computed tomography (PET/CT) of the chest. Hypermetabolic soft tissue (arrows) along the right lateral and anterior aspect of the ascending aortic endograft… Source: An unusual case of Cardiobacterium valvarum causing aortic endograft infection and osteomyelitis — Annals of Clinical Microbiology and Antimicrobials 2021; CC BY.
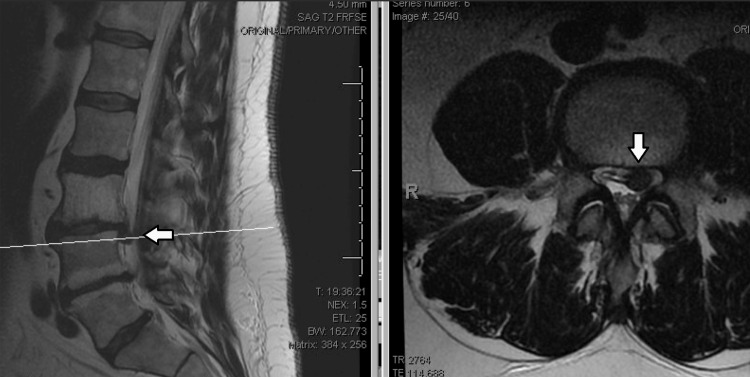 Figure 1. Pre-operative MRI Scan of Lumbar Spine, with Arrows Denoting L3/4 Disc HerniationPre-operative MRI demonstrating multilevel spondylosis and a focal disc herniation at L3-4. Source: Management of Refractory Post-operative Osteomyelitis and Discitis: A Case Report — Cureus 2024; CC BY.
Figure 1. Pre-operative MRI Scan of Lumbar Spine, with Arrows Denoting L3/4 Disc HerniationPre-operative MRI demonstrating multilevel spondylosis and a focal disc herniation at L3-4. Source: Management of Refractory Post-operative Osteomyelitis and Discitis: A Case Report — Cureus 2024; CC BY.
History of Present Illness
- Chief complaint: Insidious severe focal back pain (often nocturnal, unrelenting), fever, malaise; ± neurological deficit, deformity
- Risk factors: IVDU, diabetes, immunocompromise, bacteremia, recent procedure, TB exposure (Pott disease)
- Duration (often delayed diagnosis), source of infection
Past Medical History
- IVDU, diabetes, immunocompromise, endocarditis, TB risk, brucella exposure, recent instrumentation
- Standard PMH
Imaging Review
MRI with contrast
- Disc + adjacent endplate/vertebral body involvement (T2 hyperintense disc/marrow, endplate destruction, enhancement) — distinguishes infection (crosses disc) from tumor (spares disc)
- Epidural/paraspinal/psoas abscess, cord/thecal compression, vertebral collapse, deformity (kyphosis)
- TB: large paraspinal/psoas abscess, multilevel, relative disc sparing, subligamentous spread, gibbus
CT
- Bony destruction, instability, deformity, fusion planning, CT-guided biopsy target
X-ray (alignment, deformity)
Labs
- Blood cultures, CBC, ESR/CRP (trend), BMP, Coags, type and screen
- CT-guided biopsy (organism — before antibiotics if stable), AFB/fungal/brucella, HIV, glucose/HbA1c
- Quantiferon/PPD (TB)
Neurological Examination
- Motor/sensory (level), reflexes, sphincter, gait, spinal deformity/tenderness
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: radiolucent spine-capable table selected for approach, imaging, instrumentation, patient size, and alignment goals; keep abdomen free for prone cases.
- OR setup: fluoroscopy/navigation, decompression and instrumentation trays, culture swabs/containers for aerobic/anaerobic/fungal/AFB studies, drain, and blood availability for multilevel debridement or corpectomy.
- Special needs: antibiotic timing coordinated with cultures unless unstable, ID consult plan, arterial line if septic or major deformity/corpectomy, MAP support for cord compromise, and hardware strategy in contaminated fields.
- Immediate postop orders: neuro checks, organism-directed antibiotics, drain/wound care, ESR/CRP and culture follow-up, CT/X-rays when hardware placed, brace/activity, DVT timing, and nutrition/glycemic optimization.
Diagnosis & Indication
- Most pyogenic osteomyelitis/discitis is treated medically (CT-guided biopsy for organism + 6+ weeks IV antibiotics + bracing)
- Surgical indications: neurological deficit/cord compression (epidural abscess), instability/deformity/progressive collapse, failure of medical therapy, need for open biopsy (non-diagnostic aspirate), intractable pain from instability, significant bony destruction
- Goals: debride infection, decompress, restore stability/alignment, obtain definitive cultures
Medical Versus Operative Decision
- Before incision, define the driver: neurologic compression, sepsis/source control, mechanical instability, progressive kyphosis, uncontrolled pain, organism diagnosis, or failure of antibiotics.
- Stable neurologically intact patients often need biopsy, cultures, bracing, and ID-directed antibiotics rather than urgent instrumentation.
- Hold antibiotics until cultures when the patient is stable; do not delay antibiotics for culture purity in sepsis, neurologic decline, or epidural abscess with systemic illness.
- Screen for organism clues: IV drug use, dialysis, immunosuppression, TB/endemic exposure, brucella exposure, recent bacteremia/endocarditis, urinary source, and prior spine surgery/hardware.
Reconstruction Strategy
- Instrumentation can be appropriate in an infected field when instability/deformity demands it; eradication depends more on debridement, stability, and organism-directed therapy than on avoiding metal.
- Anterior debridement/reconstruction best addresses disc/body destruction and kyphosis; posterior fixation best provides stability and deformity control; combined/staged approaches are common when both are needed.
- Plan biopsy and culture labels before antibiotics in the room: multiple deep tissue samples, not swabs, with aerobic/anaerobic/fungal/AFB/pathology as indicated.
Position & Approach
- Anterior (debride infected disc/body, reconstruct anterior column) ± posterior instrumentation (stabilize, correct deformity); or posterolateral/combined
- Lateral (thoracic, lung deflation) or prone (posterior); IONM baseline
Key Surgical Steps
- Obtain cultures/biopsy first (multiple samples: aerobic, anaerobic, fungal, AFB, path)
- Debride infected disc, necrotic bone, abscess (anterior column); decompress neural elements
- Anterior reconstruction: structural graft (autograft/allograft) or cage (titanium acceptable in infection) to restore the anterior column and correct kyphosis
- Posterior instrumented fusion (often staged/combined) for stability and deformity correction
- Copious irrigation; consider local antibiotics; drain
- Closure
Critical Anatomy & Structures at Risk
- Spinal cord/thecal sac (compression, deformity)
- Great vessels/segmental arteries (anterior), Adamkiewicz (thoracolumbar)
- Dura (CSF leak), spinal stability/alignment
Equipment
- Culture media (incl. AFB/fungal/brucella), debridement instruments, copious irrigation
- Anterior reconstruction (cage/graft) + instrumentation, fluoroscopy/navigation
- Microscope, drain, vascular backup (anterior)
Monitoring
- SSEPs, MEPs (deficit/deformity)
Anesthesia
- Sepsis/MAP management, lung isolation (anterior thoracic), arterial line, crossmatch, antibiotic timing vs cultures
Potential Complications
- Persistent/recurrent infection (inadequate debridement), sepsis
- Hardware infection/failure, pseudarthrosis, progressive deformity
- Neurological injury, CSF leak, vascular/pulmonary (anterior)
Rescue and Follow-Up Logic
- Culture-negative infection: confirm antibiotics were held if safe, review pathology, consider repeat biopsy/open biopsy, and broaden workup for TB/fungal/brucella/malignancy before committing to empiric long courses.
- Neurologic decline on antibiotics: urgent MRI for epidural abscess, deformity, or collapse; medical therapy does not protect the cord from mechanical compression.
- Persistent bacteremia: search for endocarditis, line infection, psoas/paraspinal abscess, infected hardware, and inadequate source control.
- Progressive kyphosis/collapse: reassess stability and alignment even if inflammatory markers improve; pain and deformity can be mechanical treatment failures.
- Hardware concern in infection: distinguish expected postoperative enhancement from loosening, abscess, or nonunion using symptoms, ESR/CRP trend, CT, MRI with metal reduction, and organism status.
Operative Note Template
Preoperative Diagnosis: [Pyogenic/tuberculous] vertebral osteomyelitis-discitis at [T_/L_] [with epidural abscess/deformity/instability/deficit]
Postoperative Diagnosis: Same
Procedure: [Anterior debridement, decompression and reconstruction / Posterior instrumented fusion / Combined] for vertebral osteomyelitis-discitis at [level]
Surgeon / Assistant: Anesthesia: General endotracheal [lung isolation if anterior thoracic] EBL / Fluids / Blood products: [crossmatched] Adjuncts: Fluoroscopy/navigation; SSEP/MEP; culture media (incl. AFB/fungal/brucella); MAP support Implants: Anterior cage/graft + instrumentation [titanium acceptable in infection], drain Complications: None
Indications: [Age]yo [M/F] with vertebral osteomyelitis-discitis at [level] with [neurological deficit/instability/deformity/failed medical therapy], indicating surgery. Risks discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced [with lung isolation for the anterior thoracic approach] and neuromonitoring established. Multiple cultures/biopsies (aerobic, anaerobic, fungal, AFB) were obtained. The infected disc and necrotic bone were debrided and the neural elements decompressed. [Anterior reconstruction was performed with a structural graft/cage to restore the anterior column and correct kyphosis.] [Posterior instrumented fusion provided stability and deformity correction.] The field was copiously irrigated and a drain placed.
Closure was performed. The patient was transferred with ID-directed IV antibiotics (prolonged; multidrug for TB), serial neuro exams, and inflammatory-marker trending.
Postoperative Plan
- ICU/floor, neuro checks, ID consult — organism-directed IV antibiotics 6+ weeks (longer for TB — multidrug), trend ESR/CRP
- CT/X-ray (hardware, alignment, fusion), brace per surgeon
- DVT prophylaxis, address risk factors (glucose, addiction medicine), nutrition
- Monitor for recurrence/instability; follow-up imaging and labs; rehab
Chief-Level Case Review
Use these as the senior-level mental model for Vertebral Osteomyelitis / Discitis — Surgical Management:
- Decision point: Localize twice and instrument once: numbering, transitional anatomy, prior hardware, rib count, navigation dataset, and fluoroscopic level confirmation are mandatory.
- Technical lever: Positioning is treatment: table choice, abdomen-free prone setup, alignment goals, shoulders/hips, eyes/plexus pressure, neuromonitoring baselines, and fluoroscopic access all change the case.
- Bailout: Protect neural elements by sequence: decompression before correction when needed, MAP support for cord risk, no long paralytic with MEPs, and immediate response to signal change.
- Postop watch: Finish with construct logic: decompression adequacy, screw purchase, alignment, fusion bed/graft, drain plan, brace/activity orders, postop CT/X-rays, and DVT timing.
Common Pimp Questions
Use these to pressure-test preparation for Vertebral Osteomyelitis / Discitis — Surgical Management:
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]