
Case Prep: Intrathecal Baclofen (ITB) Pump Implantation
Case / Approach Snapshot
- Anatomy at risk: lumbar thecal sac, conus/roots, intrathecal catheter path and tip level, fascial anchor, flank-abdominal tunneling route, pump pocket skin envelope, prior fusion/scoliosis anatomy, CSF space, and refill port orientation.
- Operative steps: confirm severe spasticity indication and trial response, choose catheter entry/tip level, create durable lumbar catheter access, anchor without kinking, tunnel to a body-habitus-appropriate pump pocket, connect/program pump safely, verify CSF/drug pathway, and establish refill/overdose/withdrawal safeguards.
- Rescue plans: failed intrathecal access, catheter kink/disconnection/migration, CSF leak, pocket dehiscence/seroma/infection, baclofen overdose, life-threatening withdrawal from pump/catheter failure or empty reservoir, dosing/refill error, hydrocephalus interaction, and MRI/device-management issues.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with severe [spasticity (cerebral palsy / MS / SCI / TBI / stroke) / refractory chronic pain] planned for intrathecal drug delivery (baclofen) pump implantation [after successful trial].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior thoracolumbar approach — lumbar intrathecal access, fascial closure, and catheter-tunneling context.
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Scoliosis, spinal fusion, and intrathecal baclofen pump implantation — Scannell B. Physical medicine and rehabilitation clinics of North America 2015. PubMed
- Clinical practices in intrathecal baclofen pump implantation in children with cerebral palsy in France — Mietton C. Annals of physical and rehabilitation medicine 2016. PubMed
- Surgical treatment of spasticity: intrathecal baclofen pump implantation under subarachnoid block — Scerrati A. Neurosurgical focus: Video 2020. PubMed
- Complications of intrathecal baclofen pump: prevention and cure — Awaad Y. ISRN neurology 2012. PubMed
- Intrathecal baclofen pump implantation — Clinical privilege white paper 2015. PubMed
- Intrathecal Baclofen Pump Implantation for Type 2 Gaucher Disease — Hori YS. Pediatric neurosurgery 2017. PubMed
- Intrathecal baclofen pump implantation — Clinical privilege white paper 2000. PubMed
- [Radiculopathy following intrathecal baclofen pump implantation] — Roche N. Annales de readaptation et de medecine physique : revue scientifique de la Societe francaise de reeducation fonctionnelle de readaptation et de medecine physique 2006. PubMed
- An algorithmic approach to the management of unrecognized hydrocephalus in pediatric candidates for intrathecal baclofen pump implantation — Hanak BW. Surgical neurology international 2016. PubMed
- Intrathecal baclofen pump implantation in prone position for a cerebral palsy patient with severe scoliosis: a case report — Arishima H. Neuromodulation : journal of the International Neuromodulation Society 2015. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
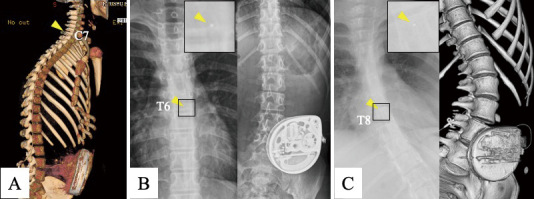 Fig. 1. A) ITB pump implantation was performed 5 years of age. Three-dimensional CT imaging demonstrates an Ascenda catheter with its tip positioned at the C7 vertebral level (yellow arrow… Source: Late-onset Kinking of the Ascenda Catheter following Intrathecal Baclofen Pump Implantation: A Case Report — NMC Case Report Journal 2025; CC BY-NC-ND.
Fig. 1. A) ITB pump implantation was performed 5 years of age. Three-dimensional CT imaging demonstrates an Ascenda catheter with its tip positioned at the C7 vertebral level (yellow arrow… Source: Late-onset Kinking of the Ascenda Catheter following Intrathecal Baclofen Pump Implantation: A Case Report — NMC Case Report Journal 2025; CC BY-NC-ND.
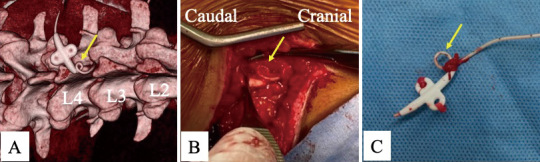 Fig. 2. A) Kinking of the catheter was observed just proximal to the anchor on three dimensional CT (yellow arrow). B) Intraoperatively, a looped and kinked segment of the previously implanted… Source: Late-onset Kinking of the Ascenda Catheter following Intrathecal Baclofen Pump Implantation: A Case Report — NMC Case Report Journal 2025; CC BY-NC-ND.
Fig. 2. A) Kinking of the catheter was observed just proximal to the anchor on three dimensional CT (yellow arrow). B) Intraoperatively, a looped and kinked segment of the previously implanted… Source: Late-onset Kinking of the Ascenda Catheter following Intrathecal Baclofen Pump Implantation: A Case Report — NMC Case Report Journal 2025; CC BY-NC-ND.
 Fig. 1. Pump reservoir incisional site on POD 1∗∗Note: photo was taken with patient in the supine position in his hospital bed. Source: Navigating the red: Diagnostic dilemma of erythema and diffuse body rash post- intrathecal baclofen pump implantation — Interventional Pain Medicine 2025; CC BY.
Fig. 1. Pump reservoir incisional site on POD 1∗∗Note: photo was taken with patient in the supine position in his hospital bed. Source: Navigating the red: Diagnostic dilemma of erythema and diffuse body rash post- intrathecal baclofen pump implantation — Interventional Pain Medicine 2025; CC BY.
 Fig. 2. Pump reservoir incision site on POD 37∗∗Note: photo taken while patient seated in his electric wheelchair. Source: Navigating the red: Diagnostic dilemma of erythema and diffuse body rash post- intrathecal baclofen pump implantation — Interventional Pain Medicine 2025; CC BY.
Fig. 2. Pump reservoir incision site on POD 37∗∗Note: photo taken while patient seated in his electric wheelchair. Source: Navigating the red: Diagnostic dilemma of erythema and diffuse body rash post- intrathecal baclofen pump implantation — Interventional Pain Medicine 2025; CC BY.
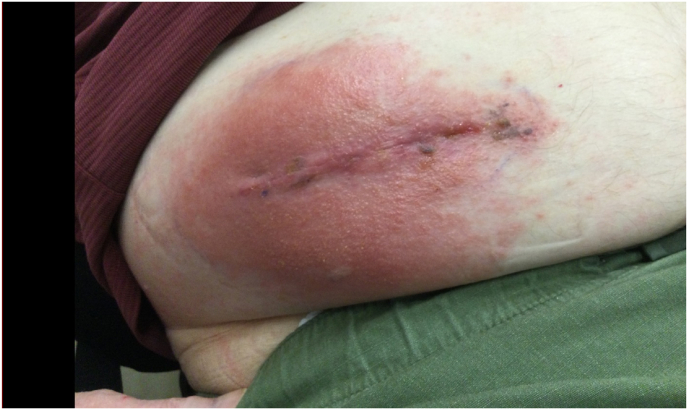 Fig. 3. Pump reservoir incision site on POD 47. Source: Navigating the red: Diagnostic dilemma of erythema and diffuse body rash post- intrathecal baclofen pump implantation — Interventional Pain Medicine 2025; CC BY.
Fig. 3. Pump reservoir incision site on POD 47. Source: Navigating the red: Diagnostic dilemma of erythema and diffuse body rash post- intrathecal baclofen pump implantation — Interventional Pain Medicine 2025; CC BY.
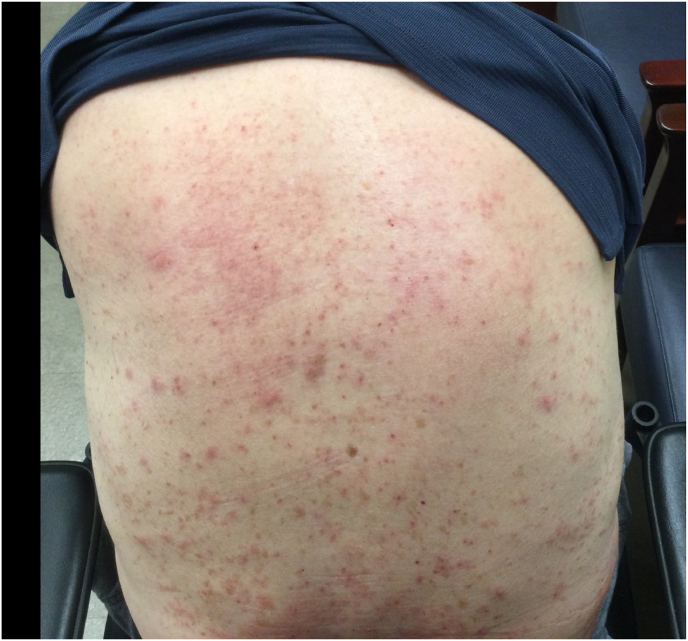 Fig. 4. Posterior trunk cutaneous rash on POD 54. Source: Navigating the red: Diagnostic dilemma of erythema and diffuse body rash post- intrathecal baclofen pump implantation — Interventional Pain Medicine 2025; CC BY.
Fig. 4. Posterior trunk cutaneous rash on POD 54. Source: Navigating the red: Diagnostic dilemma of erythema and diffuse body rash post- intrathecal baclofen pump implantation — Interventional Pain Medicine 2025; CC BY.
 Fig. 5. Pump reservoir site incision at POD 64 showing resolution of erythema and skin lesions. Source: Navigating the red: Diagnostic dilemma of erythema and diffuse body rash post- intrathecal baclofen pump implantation — Interventional Pain Medicine 2025; CC BY.
Fig. 5. Pump reservoir site incision at POD 64 showing resolution of erythema and skin lesions. Source: Navigating the red: Diagnostic dilemma of erythema and diffuse body rash post- intrathecal baclofen pump implantation — Interventional Pain Medicine 2025; CC BY.
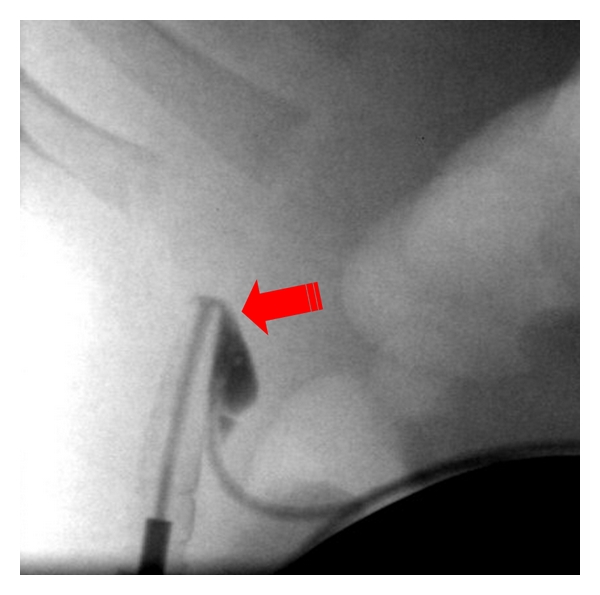 Figure 1. Tear at metal connector to pump within protective silicone covering. Source: Complications of Intrathecal Baclofen Pump: Prevention and Cure — ISRN Neurology 2012; CC BY.
Figure 1. Tear at metal connector to pump within protective silicone covering. Source: Complications of Intrathecal Baclofen Pump: Prevention and Cure — ISRN Neurology 2012; CC BY.
History of Present Illness
- Chief complaint: Severe, disabling spasticity (impairing function, care, comfort, causing pain/contractures) refractory to oral antispasmodics, OR refractory chronic pain (intrathecal opioid/ziconotide)
- Etiology of spasticity (CP, MS, SCI, TBI, stroke, hereditary spastic paraplegia)
- Successful ITB trial (test dose via LP showing meaningful spasticity reduction — Ashworth improvement) required before pump
- Goals (function vs comfort/care/positioning), caregiver involvement
Past Medical History
- Body habitus (pump pocket — thin/pediatric patients), prior spine surgery/fusion (catheter placement), infection risk, bleeding/anticoagulation
- MRI needs, future spine surgery, baseline respiratory/bulbar status (overdose risk)
- Standard PMH
Imaging Review
Spine imaging (if prior surgery/scoliosis)
- Catheter placement feasibility, level, fusion/hardware, scoliosis
Trial documentation
- ITB trial response (test dose LP — Ashworth/spasm reduction)
Candidate and Systems Checklist
- Define the goal: comfort/care, sleep, hygiene, contracture prevention, transfers, gait, pain, or caregiver burden. Too much tone reduction can worsen transfers or standing in selected patients.
- Confirm trial response with objective tone/spasm scores and functional/caregiver observations, not only “felt looser.”
- Screen hydrocephalus in pediatric/CP candidates when head growth, ventriculomegaly, shunt history, or symptoms suggest CSF-dynamics issues.
- Check abdominal wall thickness, wheelchair beltline, scoliosis, prior abdominal surgery, G-tube/ostomy, and skin pressure points before selecting the pump pocket.
- Confirm caregiver reliability, refill logistics, emergency access, and who will manage dose titration/refill alarms.
Labs
- CBC, Coags (intrathecal catheter), BMP
Neurological Examination
- Spasticity scales (Modified Ashworth, spasm frequency), motor/function, contractures, document baseline
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: standard OR table or radiolucent spine table depending on percutaneous versus paddle/intrathecal access; confirm fluoroscopy and tunneling access before prep.
- OR setup: fluoroscopy, implant/pump/stimulator inventory verified, programmer/vendor available, sterile tunneling tools, trial leads/catheters as applicable, and pocket-site laterality confirmed.
- Special needs: antibiotic/implant protocol, anticoagulation plan for neuraxial access, baclofen-withdrawal/overdose rescue plan for pumps, device programming orders, and infection-prevention bundle.
- Immediate postop orders: wound/pocket checks, neuro checks for neuraxial hematoma, device programming/initial dose orders, activity restrictions, antibiotics per protocol, pain control, and follow-up for interrogation/refill/programming.
Position
- OR table/bed: standard OR table or radiolucent spine table depending on percutaneous versus paddle/intrathecal access; confirm fluoroscopy and tunneling access before prep.
- Lateral decubitus (catheter via LP-type access + abdominal pump pocket), fluoroscopy; padded
Key Surgical Steps
- Intrathecal catheter: Tuohy needle into the lumbar subarachnoid space (paramedian, L3-4/L4-5), confirm CSF flow
- Thread the intrathecal catheter cephalad to the target level (e.g., T6-T8 for lower extremity spasticity; higher/cervical for upper extremity/generalized) under fluoroscopy
- Anchor the catheter at the lumbar fascia (anti-kink/anti-migration), small paramedian fascial incision
- Abdominal pump pocket: subcutaneous (or subfascial in thin/pediatric) pocket in the lower abdomen
- Tunnel the catheter from the back to the abdominal pocket, connect to the programmable pump (pre-filled with baclofen)
- Confirm CSF flow/connections, program the pump (starting dose), secure pump in pocket
- Closure
- (Some confirm catheter tip with fluoroscopy/contrast myelogram via catheter)
Technical Nuances
- Lumbar entry should be below the conus and away from fused/stenotic levels; use fluoroscopy or ultrasound when anatomy is distorted.
- Tunnel a smooth catheter arc with strain relief at both lumbar anchor and pump pocket; sharp turns become delayed kinks.
- In thin children/adults, consider subfascial pump placement to reduce erosion, but balance pain and surgical morbidity.
- Orient the refill port clearly and document pump location/depth; poor orientation creates future refill risk.
- Prime and program according to device protocol, with independent medication concentration/dose checks before leaving the OR.
- Obtain baseline postoperative radiographs/fluoro images of catheter course and tip level for future malfunction workups.
Critical Anatomy & Structures at Risk
- Spinal cord / nerve roots / conus (catheter — stay subarachnoid, avoid cord; lumbar entry below conus)
- Dura (CSF leak — post-dural-puncture headache, hygroma), catheter tip level (dosing effect)
- Pump pocket (seroma, infection, dehiscence — esp. thin patients)
Equipment
- ITB pump (programmable) + intrathecal catheter + anchor/connectors, Tuohy needle, tunneler
- Fluoroscopy, baclofen (pump fill), programmer
Anesthesia
- General (or spinal/local per patient); antibiotics (implant); positioning
Potential Complications
- Baclofen overdose (drowsiness, respiratory depression, hypotonia, coma — programming/refill errors, dosing) and withdrawal (life-threatening: high fever, rigidity, rhabdomyolysis, rebound spasticity — abrupt interruption from pump failure/empty/catheter problem) — emergencies
- CSF leak / hygroma / PDPH, catheter migration/kink/disconnection/occlusion (under-dosing/withdrawal)
- Infection (pocket/CSF — meningitis; may need explant), seroma, pocket dehiscence
- Pump malfunction, MRI considerations
Equipment/Safety Note
- Establish refill schedule (avoid empty-reservoir withdrawal), program alarms, educate patient/caregiver on withdrawal/overdose signs
Overdose vs Withdrawal
| Syndrome | Typical clues | Immediate priorities |
|---|---|---|
| Baclofen overdose | somnolence, hypotonia, respiratory depression, bradycardia/hypotension, coma | airway/ventilation, pump interrogation, stop/reduce infusion, ICU support, consider CSF aspiration per specialist protocol |
| Baclofen withdrawal | rebound spasticity, pruritus, fever, agitation, autonomic instability, rhabdomyolysis, seizures, organ failure | restore intrathecal baclofen if possible, benzodiazepines/supportive ICU care, troubleshoot pump/catheter/refill, treat hyperthermia/rhabdo |
| Catheter malfunction | loss of effect, withdrawal symptoms, abnormal residual volume, kink/disconnection on imaging | interrogate pump, radiographs/contrast study per protocol, urgent revision if withdrawal risk |
| Pocket infection | erythema, drainage, tenderness, fever, positive cultures | cultures/antibiotics, assess depth; deep hardware infection often requires explant/temporary baclofen bridge |
Troubleshooting Pathway
- Interrogate pump first: reservoir volume, alarm history, dose/concentration, battery, motor stall, and last refill.
- Compare aspirated reservoir volume with expected volume; mismatch suggests refill/programming or delivery problem.
- Image the entire catheter from pump to intrathecal tip; kinks and disconnections hide at anchors/connectors.
- If contrast study is needed, aspirate catheter access port first when protocol requires it to avoid bolus overdose.
- Treat suspected withdrawal while diagnosing; waiting for perfect proof can be dangerous.
Operative Note Template
Preoperative Diagnosis: Severe [spasticity (CP/MS/SCI/TBI) / refractory pain] with successful ITB trial
Postoperative Diagnosis: Same
Procedure: Intrathecal baclofen pump implantation with intrathecal catheter (tip at [level]) and [abdominal] pump pocket
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Fluoroscopy, Tuohy needle, tunneler, programmer Implants: Programmable ITB pump + intrathecal catheter, baclofen (pump fill) Complications: None
Indications: [Age]yo [M/F] with severe disabling spasticity refractory to oral agents, with a positive ITB test dose (Ashworth/spasm reduction). Risks (overdose/withdrawal, CSF leak, infection, catheter problems) discussed; refill schedule planned.
Description of Procedure: After consent and time-out, general anesthesia was induced and the patient positioned in lateral decubitus with fluoroscopy. A Tuohy needle accessed the lumbar subarachnoid space (paramedian, [L3-4/L4-5]) with CSF return confirmed, and the intrathecal catheter threaded cephalad to [T6-T8] under fluoroscopy and anchored to the lumbar fascia. A subcutaneous abdominal pump pocket was created, the catheter tunneled and connected to the programmable pump (pre-filled with baclofen), CSF flow/connections confirmed, and the pump programmed at the starting dose.
Closure was performed. The patient was monitored for overdose (respiratory depression) and CSF leak, with a refill schedule established and caregiver education on overdose/withdrawal recognition.
Postoperative Plan
- Floor/monitored (overdose risk early), neuro/respiratory checks
- Watch for overdose (somnolence, respiratory depression — have flumazenil? no; supportive, consider CSF aspiration, physostigmine historically) and withdrawal (rigidity, fever)
- CSF leak precautions (flat if PDPH/leak), wound/pocket monitoring (seroma/infection)
- Refill schedule established, dose titration in clinic, caregiver education (withdrawal/overdose emergency recognition)
- Spasticity reassessment, follow-up; document pump/MRI parameters
Chief-Level Case Review
Use these as the senior-level mental model for Intrathecal Baclofen (ITB) Pump Implantation:
- Decision point: Localize twice and instrument once: numbering, transitional anatomy, prior hardware, rib count, navigation dataset, and fluoroscopic level confirmation are mandatory.
- Technical lever: Positioning is treatment: table choice, abdomen-free prone setup, alignment goals, shoulders/hips, eyes/plexus pressure, neuromonitoring baselines, and fluoroscopic access all change the case.
- Bailout: Protect neural elements by sequence: decompression before correction when needed, MAP support for cord risk, no long paralytic with MEPs, and immediate response to signal change.
- Postop watch: Finish with construct logic: decompression adequacy, screw purchase, alignment, fusion bed/graft, drain plan, brace/activity orders, postop CT/X-rays, and DVT timing.
Common Pimp Questions
Use these to pressure-test preparation for Intrathecal Baclofen (ITB) Pump Implantation:
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]