
Case Prep: Spinal Arteriovenous Malformation (Intramedullary / Perimedullary)
Case / Approach Snapshot
- Anatomy at risk: cord, roots, dura, posterior elements, segmental and radiculomedullary arteries, venous plexus, and level-specific bony landmarks.
- Operative steps: localize the level, expose while preserving stability, obtain proximal/distal vascular control when relevant, decompress or disconnect/reconstruct the lesion, confirm flow/decompression, and close with CSF-leak prevention; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: neuromonitoring change, bleeding from epidural/foraminal vessels, durotomy, wrong-level exposure, cord swelling/ischemia, instability, and staged/endovascular adjuncts.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [cervical/thoracic] [intramedullary glomus / perimedullary fistulous] spinal AVM presenting with [hemorrhage / myelopathy / radiculopathy] planned for [embolization ± microsurgical resection].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior cervical approach or posterior thoracolumbar approach — posterior midline exposure, durotomy, and closure principles by lesion level.
Neurosurgical Atlas · neuroangio.org · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Treatment of Spinal Arteriovenous Malformation and Fistula — Ehresman J. Neurosurgery clinics of North America 2022. PubMed
- Spinal arteriovenous malformation with a calcified nodule: illustrative case — Liu PC. Journal of neurosurgery. Case lessons 2023. PubMed
- [Spinal arteriovenous malformations] — Udelhoven A. Radiologie (Heidelberg, Germany) 2022. PubMed
- Spinal arteriovenous malformation — Drislane FW. Archives of neurology 2003. PubMed
- Spinal Arteriovenous Malformation Associated with Parkes Weber Syndrome: Report of Two Cases and Literature Review — Li ZF. World neurosurgery 2017. PubMed
- [Spinal arteriovenous malformation] — Miyamoto S. No shinkei geka. Neurological surgery 2002. PubMed
- [Surgical Treatment for Spinal Arteriovenous Malformation] — Endo T. No shinkei geka. Neurological surgery 2021. PubMed
- Transvenous embolization of conus spinal arteriovenous malformation: illustrative case — Anadani M. Journal of neurosurgery. Case lessons 2023. PubMed
- Multisegmental spinal arteriovenous malformation associated with the Parkes-Weber syndrome: A case report and literature review — Tao L. Medicine 2025. PubMed
- Spinal arteriovenous fistulae: surgical management — Day AL. Handbook of clinical neurology 2017. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
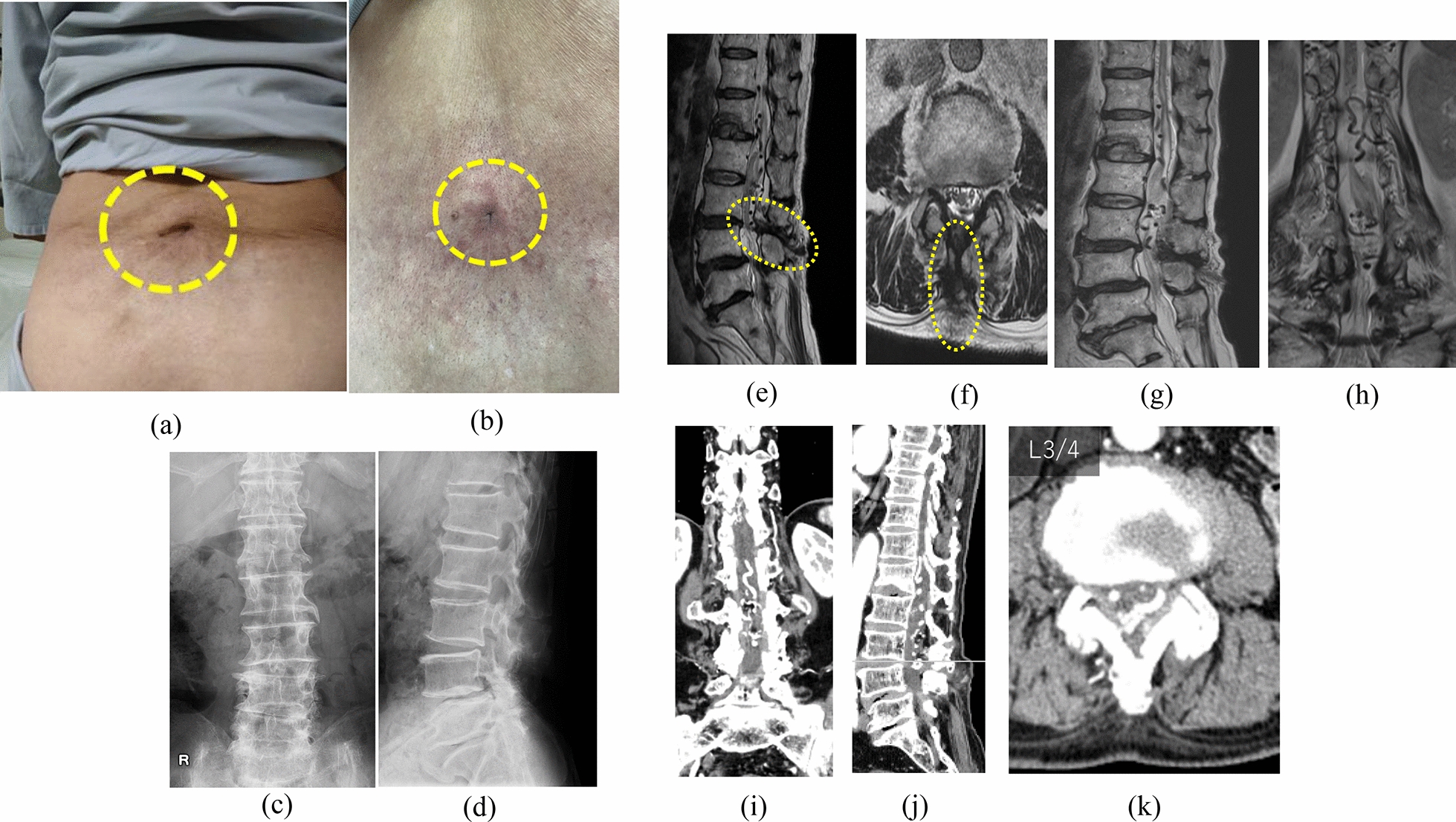 Fig. 1. Preoperative photograph of the patient’s back and radiological findings of the lumbosacral spine. (a, b) Patient exhibited a skin ostium (dotted circle) in the medial lumbar region. (c,… Source: Spinal arteriovenous malformation associated with congenital dermal sinus: a case report — Journal of Medical Case Reports 2025; CC BY-NC-ND.
Fig. 1. Preoperative photograph of the patient’s back and radiological findings of the lumbosacral spine. (a, b) Patient exhibited a skin ostium (dotted circle) in the medial lumbar region. (c,… Source: Spinal arteriovenous malformation associated with congenital dermal sinus: a case report — Journal of Medical Case Reports 2025; CC BY-NC-ND.
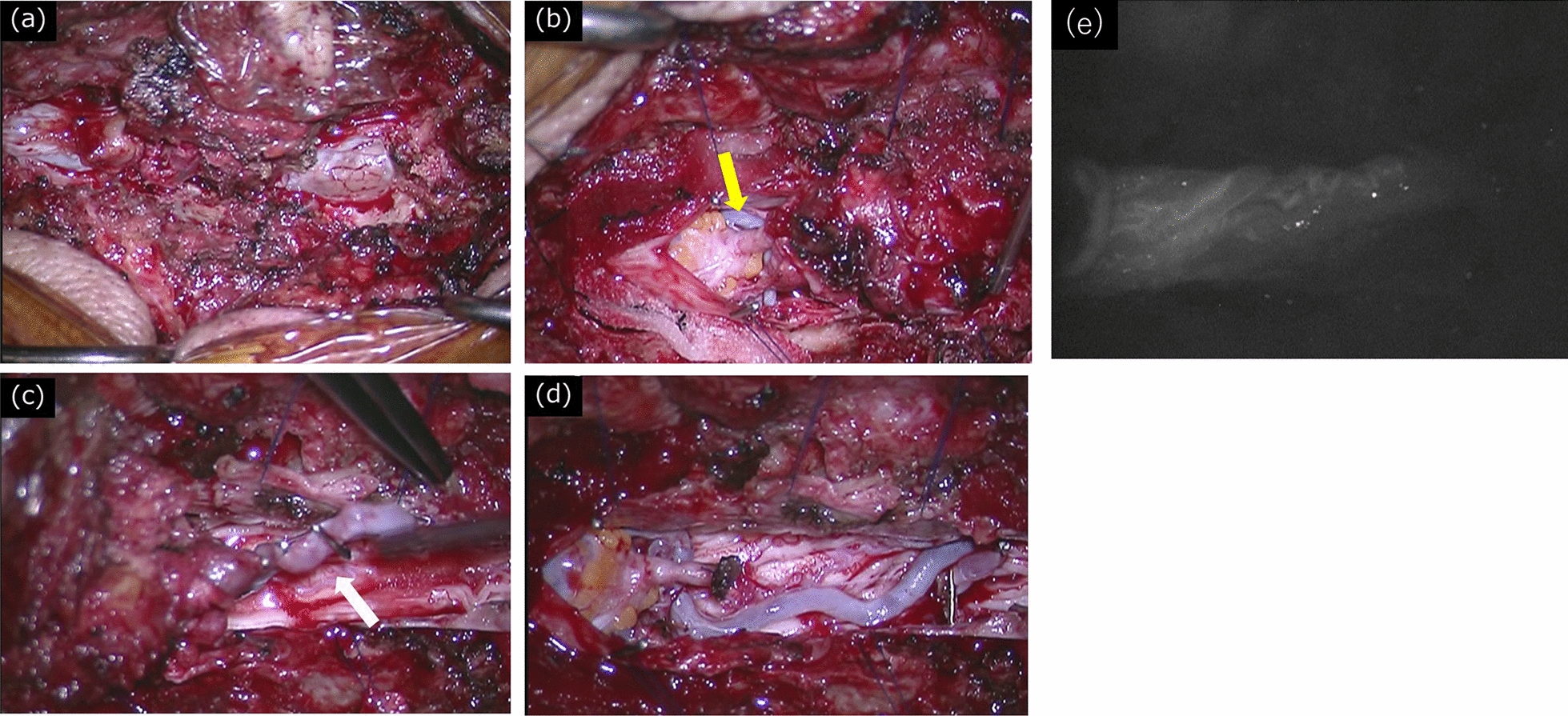 Fig. 2. Surgical site photographs. (a) After L3/4 laminectomy, the cutaneous sinus was continuous with the dura mater. (b) A fatty mass was present on the cephalic side of the dermal sinus. It… Source: Spinal arteriovenous malformation associated with congenital dermal sinus: a case report — Journal of Medical Case Reports 2025; CC BY-NC-ND.
Fig. 2. Surgical site photographs. (a) After L3/4 laminectomy, the cutaneous sinus was continuous with the dura mater. (b) A fatty mass was present on the cephalic side of the dermal sinus. It… Source: Spinal arteriovenous malformation associated with congenital dermal sinus: a case report — Journal of Medical Case Reports 2025; CC BY-NC-ND.
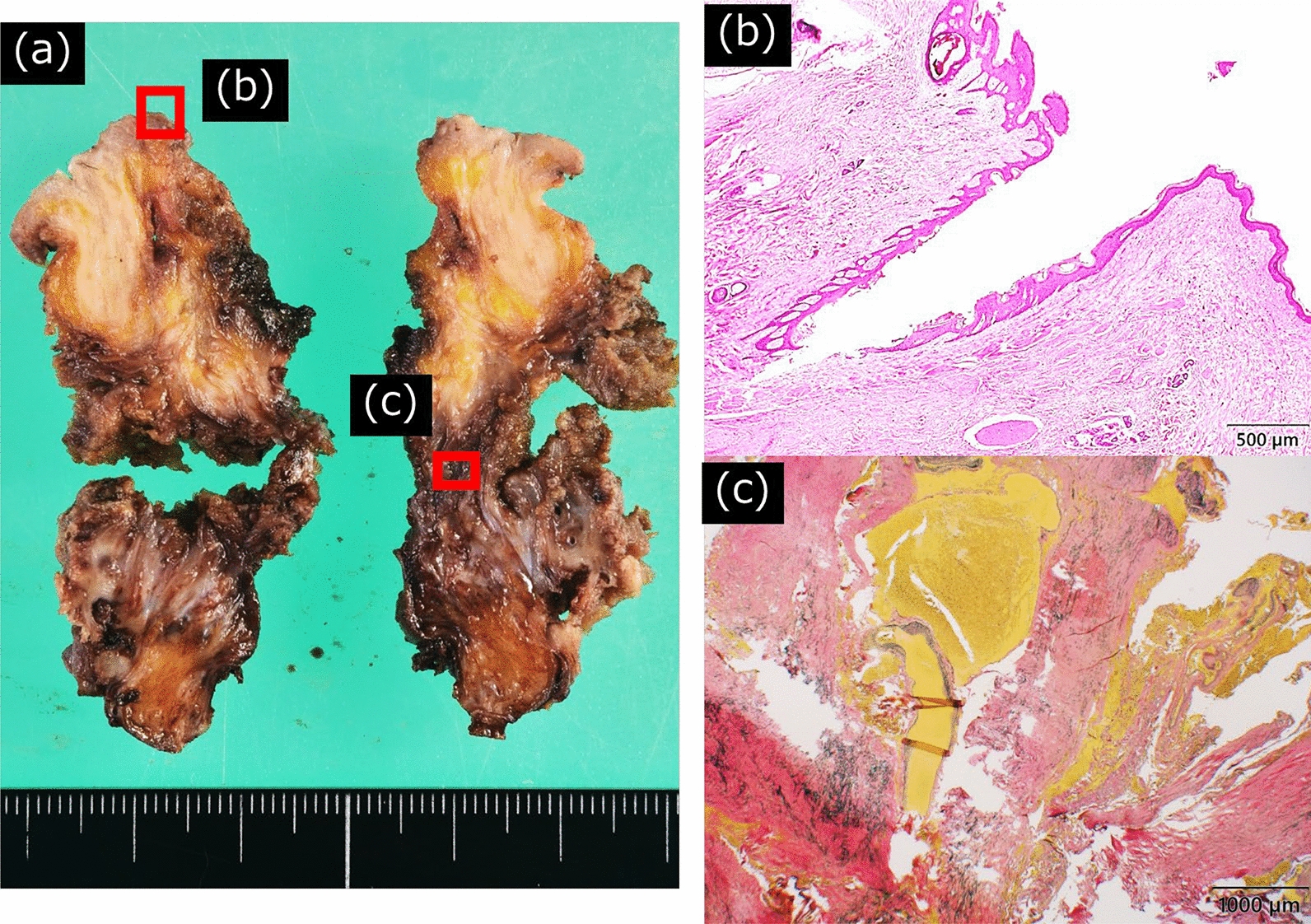 Fig. 3. Histopathological findings. (a) Extracted lesions cut in the sagittal plane. Panels show the areas observed under a microscope. (b) The fistula area showed a luminal structure covered by… Source: Spinal arteriovenous malformation associated with congenital dermal sinus: a case report — Journal of Medical Case Reports 2025; CC BY-NC-ND.
Fig. 3. Histopathological findings. (a) Extracted lesions cut in the sagittal plane. Panels show the areas observed under a microscope. (b) The fistula area showed a luminal structure covered by… Source: Spinal arteriovenous malformation associated with congenital dermal sinus: a case report — Journal of Medical Case Reports 2025; CC BY-NC-ND.
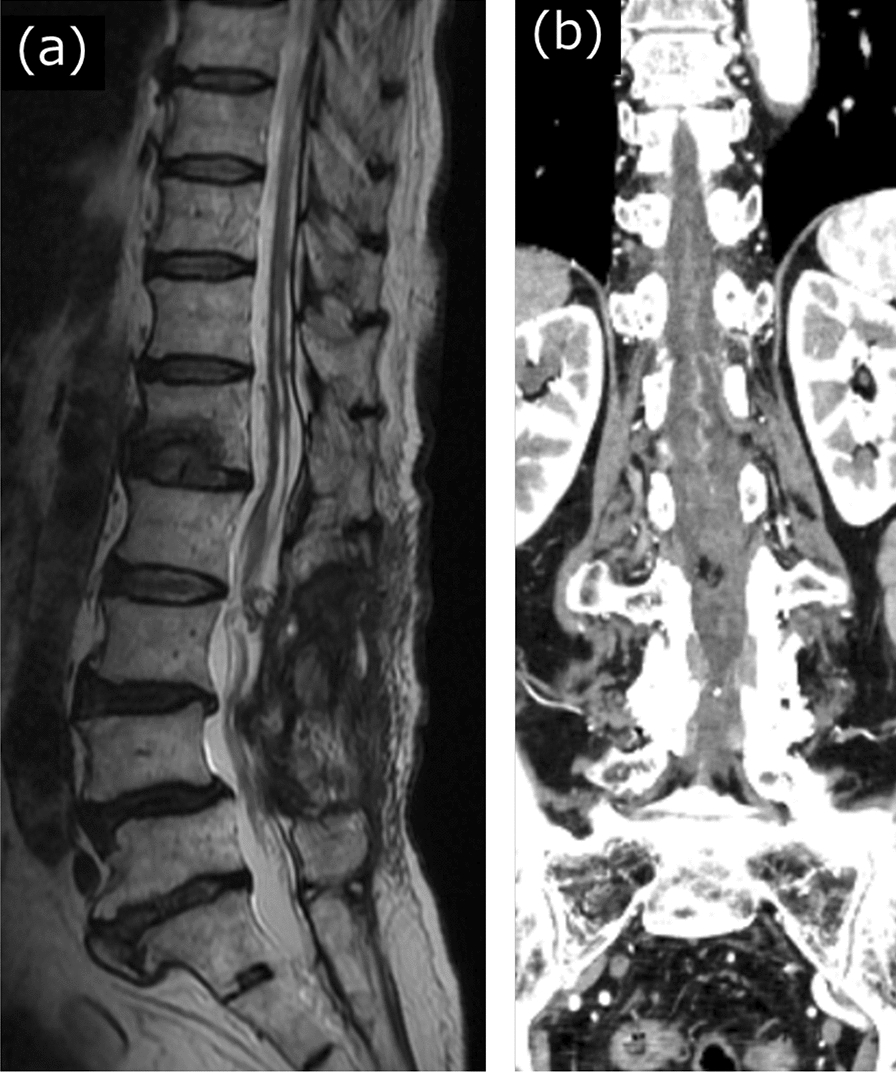 Fig. 4. Postoperative radiological findings. Postoperative (a) magnetic resonance imaging and (b) contrast-enhanced computed tomography at 2.5 months showed that the abnormal vascular shadows… Source: Spinal arteriovenous malformation associated with congenital dermal sinus: a case report — Journal of Medical Case Reports 2025; CC BY-NC-ND.
Fig. 4. Postoperative radiological findings. Postoperative (a) magnetic resonance imaging and (b) contrast-enhanced computed tomography at 2.5 months showed that the abnormal vascular shadows… Source: Spinal arteriovenous malformation associated with congenital dermal sinus: a case report — Journal of Medical Case Reports 2025; CC BY-NC-ND.
 Fig. 1. T spine MR images show about 1.2 cm sized ill-defined intramedullary lesion which has intramedullary nidus and multiple flow voids extension to the dorsal subpial surface is noted in… Source: Spinal Arteriovenous Malformation Masquerating Zoster Sine Herpete — The Korean Journal of Pain 2013; CC BY-NC.
Fig. 1. T spine MR images show about 1.2 cm sized ill-defined intramedullary lesion which has intramedullary nidus and multiple flow voids extension to the dorsal subpial surface is noted in… Source: Spinal Arteriovenous Malformation Masquerating Zoster Sine Herpete — The Korean Journal of Pain 2013; CC BY-NC.
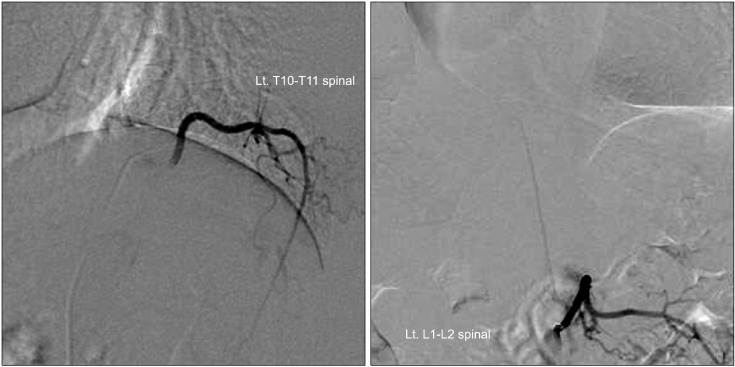 Fig. 2. Spinal angiogram shows spinal cord AVM feeding from anterior spinal artery from left T9 intercostal artery and left L1 lumbar artery (artery of Adamkiewicz) and nidus of T11 level… Source: Spinal Arteriovenous Malformation Masquerating Zoster Sine Herpete — The Korean Journal of Pain 2013; CC BY-NC.
Fig. 2. Spinal angiogram shows spinal cord AVM feeding from anterior spinal artery from left T9 intercostal artery and left L1 lumbar artery (artery of Adamkiewicz) and nidus of T11 level… Source: Spinal Arteriovenous Malformation Masquerating Zoster Sine Herpete — The Korean Journal of Pain 2013; CC BY-NC.
 Figure 1.. A 33-yr-old male with multisegmental spinal arteriovenous malformation and PWS. (A) The computed tomography angiography of both lower extremities of the patient. (B) Localized tissue… Source: Multisegmental spinal arteriovenous malformation associated with the Parkes–Weber syndrome: A case report and literature review — Medicine 2025; CC BY.
Figure 1.. A 33-yr-old male with multisegmental spinal arteriovenous malformation and PWS. (A) The computed tomography angiography of both lower extremities of the patient. (B) Localized tissue… Source: Multisegmental spinal arteriovenous malformation associated with the Parkes–Weber syndrome: A case report and literature review — Medicine 2025; CC BY.
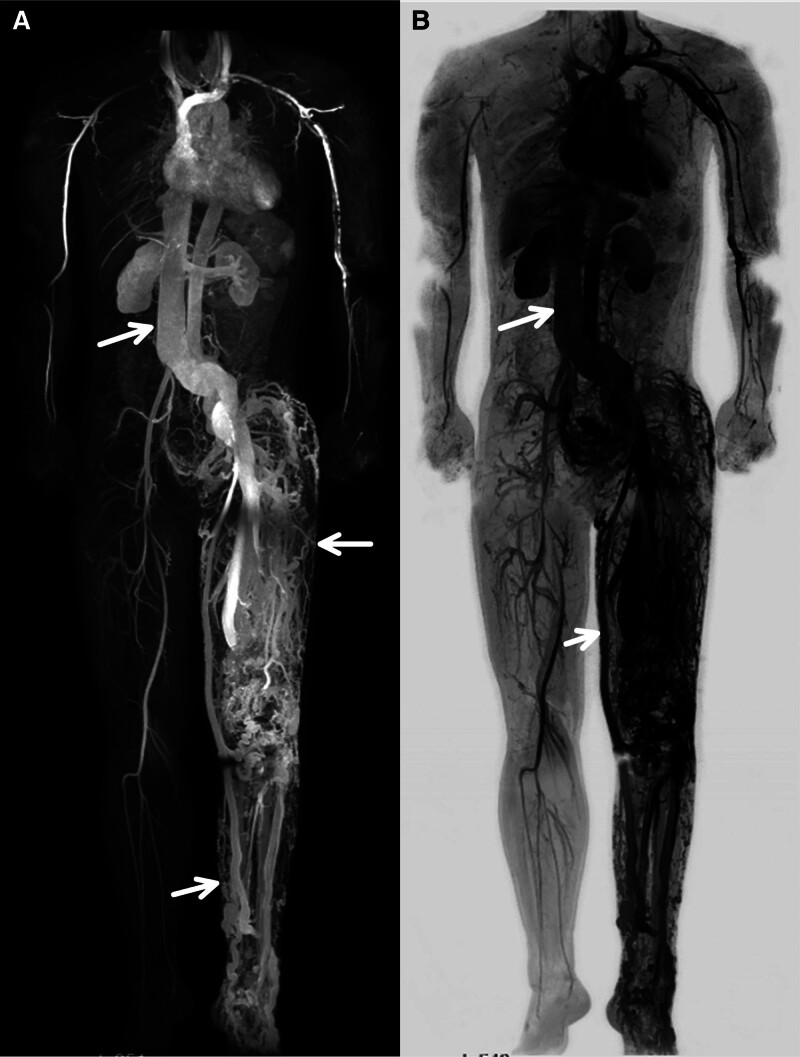 Figure 2.. The patient underwent whole-body angiography using modified DIXON technique combined with CE-MRA and bolus track technique. (A) CE-MRA showed marked dilation of the inferior vena cava… Source: Multisegmental spinal arteriovenous malformation associated with the Parkes–Weber syndrome: A case report and literature review — Medicine 2025; CC BY.
Figure 2.. The patient underwent whole-body angiography using modified DIXON technique combined with CE-MRA and bolus track technique. (A) CE-MRA showed marked dilation of the inferior vena cava… Source: Multisegmental spinal arteriovenous malformation associated with the Parkes–Weber syndrome: A case report and literature review — Medicine 2025; CC BY.
 Figure 3.. (A) CE-MRA showing spinal arteriovenous malformation (T9–L4) before embolization. (B) CE-MRA showed significant improvement of the abnormal connections between the arteries and veins in… Source: Multisegmental spinal arteriovenous malformation associated with the Parkes–Weber syndrome: A case report and literature review — Medicine 2025; CC BY.
Figure 3.. (A) CE-MRA showing spinal arteriovenous malformation (T9–L4) before embolization. (B) CE-MRA showed significant improvement of the abnormal connections between the arteries and veins in… Source: Multisegmental spinal arteriovenous malformation associated with the Parkes–Weber syndrome: A case report and literature review — Medicine 2025; CC BY.
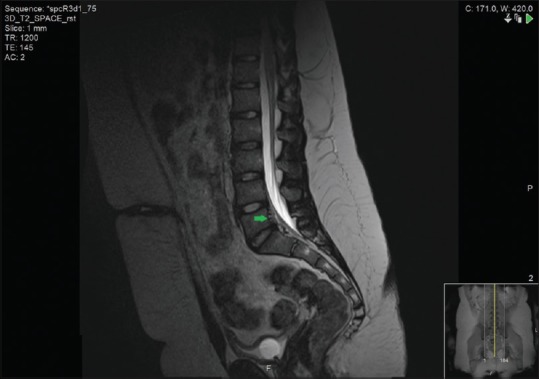 Figure 1. Sagittal view of the spinal magnetic resonance imaging scan which shows an anterior epidural arteriovenous malformation at L4/5 to S2 level (arrow). The thecal canal is obliterated at… Source: Spinal arteriovenous malformation presenting with urinary retention — Urology Annals 2016; CC BY-NC-SA.
Figure 1. Sagittal view of the spinal magnetic resonance imaging scan which shows an anterior epidural arteriovenous malformation at L4/5 to S2 level (arrow). The thecal canal is obliterated at… Source: Spinal arteriovenous malformation presenting with urinary retention — Urology Annals 2016; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Acute deficit from hemorrhage (hematomyelia/SAH), or progressive myelopathy (steal/venous congestion/mass effect)
- Younger patients (vs dAVF), abrupt presentations more common
- Types: intramedullary (glomus/compact, Type II), juvenile (Type III, extensive), perimedullary fistula (Type IV — pial AV fistula)
- Prior hemorrhage, prior embolization/surgery, associated aneurysms
Imaging Review
MRI Spine (T2, GRE, T1±Gad)
- Nidus location (intramedullary vs pial/perimedullary), flow voids, hemorrhage (GRE/SWI), syrinx, cord edema
Spinal DSA (gold standard)
- Angioarchitecture: feeders (anterior/posterior spinal arteries), nidus, draining veins, flow rate, associated aneurysms
- Artery of Adamkiewicz / cord supply relationship (shared supply limits resectability)
- Compact glomus (more resectable) vs diffuse/juvenile (high risk)
Labs
- CBC, BMP, Coags, type and crossmatch
Neurological Examination
- Detailed motor/sensory/sphincter, gait, baseline documentation
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- OR setup: microscope, neuromonitoring, spinal angiography/DSA images loaded, ICG/Doppler, clips/coagulation tools, laminectomy/instrumentation backup, and blood available for vascular lesions.
- Special needs: arterial line, Foley, MAP support for cord perfusion, no long paralytic with MEPs, CSF drainage plan only when indicated, and coordination with endovascular/staged treatment.
- Immediate postop orders: ICU neuro checks with motor/sensory/sphincter focus, MAP target, MRI/angiography confirmation plan, drain/hematoma watch, steroid/pain regimen, DVT timing, and rehab planning.
Diagnosis & Indication
- Indication: Hemorrhage, progressive deficit, accessible nidus; multimodal management (embolization to reduce flow/target deep feeders, then microsurgery for compact dorsal/pial lesions)
- High-risk anterior/intramedullary nidi with shared ASA supply may be managed by partial embolization/observation (cure not always achievable safely)
- Perimedullary fistulas (Type IV): disconnect the fistulous point (surgery or embolization)
Type-Specific Treatment Logic
| Lesion pattern | Usual strategy | Key operative principle |
|---|---|---|
| Type I dural AVF mimic/overlap | Usually treated as a fistula rather than a true intramedullary AVM | Disconnect the arterialized draining vein at the dural sleeve; do not chase congested intradural veins. |
| Type II glomus AVM | Multimodal; embolize selected deep/high-flow feeders, then microsurgery if compact and accessible | Circumferential pial dissection, feeders first, draining vein last; accept subtotal if ASA/perforators or IONM make cure unsafe. |
| Type III juvenile/diffuse AVM | Rarely cured surgically; staged/palliative treatment for hemorrhage source, venous hypertension, or progressive myelopathy | Define the goal before treatment: cure, flow reduction, aneurysm treatment, or decompression are different operations. |
| Type IV perimedullary fistula | Embolization or microsurgical disconnection depending on anatomy | Obliterate the fistulous point while preserving ASA/PSA flow and normal pial vessels. |
Angiographic Planning Checklist
- Identify the ASA, paired posterior spinal arteries, radiculomedullary contributors, and artery of Adamkiewicz before any embolization or clip/coagulation decision.
- Map whether feeders are terminal to the nidus/fistula or en-passage to normal cord; shared supply is a major reason to stop short of cure.
- Mark flow aneurysms, pseudoaneurysms, venous outflow stenosis, and thrombosed/ectatic draining veins that may explain hemorrhage or progressive congestion.
- Decide whether preoperative embolization is meant to reduce flow, treat a high-risk aneurysm, open a surgical plane, or serve as definitive therapy.
- Plan intraoperative confirmation: ICG for surface flow, Doppler for high-flow fistulae, and intraoperative DSA when residual deep nidus or ambiguous venous drainage would change management.
Position
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- Prone, Mayfield/foam, IONM baseline; per level
Key Surgical Steps
- Preoperative/staged embolization (reduce nidus flow, target inaccessible feeders)
- Laminectomy at the lesion level, midline durotomy
- Identify the nidus/fistula on the dorsal/pial cord surface (ICG, DSA correlation)
- Perimedullary fistula: identify and coagulate/clip the single fistulous point between feeding artery and draining vein (preserve normal vessels)
- Glomus AVM: circumferential pial dissection, coagulate feeders progressively, preserve anterior spinal artery and normal perforators, take draining vein last; intramedullary component dissected in pial plane with IONM guidance — accept subtotal if cord function threatened
- ICG / intraoperative DSA to confirm obliteration
- Watertight dural closure
Critical Anatomy & Structures at Risk
- Anterior spinal artery and sulcal perforators — cord infarction if sacrificed
- Spinal cord parenchyma (intramedullary dissection) — motor/sensory tracts
- Draining veins (preserve until feeders controlled — as cranial AVM principles)
- Dura, nerve roots
Equipment
- Microscope, ICG / intraoperative DSA, micro-clips, fine bipolar, micro-instruments
- Embolization (neuro-IR, preop/staged), CUSA (selected), dural substitute
Monitoring
- SSEPs, MEPs, D-wave (cord); essential
Anesthesia
- Arterial line, MAP support, crossmatched blood, no paralytic (IONM), prone precautions
Potential Complications
- Cord infarction (ASA/perforator injury), hemorrhage
- Worsened myelopathy, incomplete obliteration/recurrence
- CSF leak, venous infarction (premature vein occlusion)
Intraoperative Rescue Plans
- MEP/SSEP/D-wave decline: pause dissection, raise MAP, irrigate warm saline, release retraction, verify no temporary clip or coagulated pial vessel compromises normal cord supply, and reassess whether subtotal treatment is safer.
- Premature draining vein occlusion: stop further feeder work, evaluate cord swelling and residual shunt flow with ICG/DSA, restore outflow if reversible, and avoid trapping a pressurized nidus.
- ASA/perforator uncertainty: do not coagulate until the vessel is proven lesional; use micro-Doppler/ICG/DSA correlation and leave a remnant if normal supply remains plausible.
- Residual shunt on ICG/DSA: localize whether it is a surgically accessible surface fistula, deep nidus, or normal transit; extend exposure only if the added risk is justified.
- Cord swelling or hemorrhage: achieve gentle tamponade, maintain perfusion, evacuate compressive clot only when the plane is clear, and be prepared for duraplasty rather than tight closure.
Operative Note Template
Preoperative Diagnosis: [Cervical/thoracic] spinal AVM ([intramedullary glomus / perimedullary fistula]) [with prior hemorrhage]
Postoperative Diagnosis: Same
Procedure: [Level] laminectomy and microsurgical resection/disconnection of spinal AVM [following embolization]
Surgeon / Assistant: Anesthesia: General endotracheal, no paralytic EBL / Fluids / Blood products: [crossmatched] Adjuncts: Microscope, ICG/intraoperative DSA, micro-clips, fine bipolar; MEP/SSEP/D-wave; MAP support Implants: Dural substitute, sealant Complications: None
Indications: [Age]yo [M/F] with a symptomatic spinal AVM at [level] presenting with [hemorrhage/myelopathy]. [Staged embolization preceded surgery.] Risks (cord infarction, hemorrhage, deficit) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced (MAP support, no paralytic) and MEP/SSEP/D-wave monitoring established. [Preoperative embolization had reduced nidus flow.] The patient was positioned prone; a laminectomy was performed over the lesion and a midline durotomy made under the microscope.
The nidus/fistula was identified on the dorsal/pial surface (ICG, DSA correlation). [Perimedullary fistula (Type IV): the single fistulous point between feeding artery and draining vein was coagulated/clipped, preserving normal vessels.] [Glomus AVM: circumferential pial dissection with progressive feeder control, preserving the anterior spinal artery and perforators, taking the draining vein last.] ICG [/intraoperative DSA] confirmed obliteration with preserved normal cord vessels. A watertight dural closure was performed with sealant.
Closure was completed in layers. The patient was transferred to the ICU with MAP support and CSF-leak precautions.
Postoperative Plan
- ICU, neuro checks q1h (motor/sensory/sphincter), MAP support, CSF leak precautions
- Postop DSA (confirm obliteration), MRI
- DVT prophylaxis (mechanical), rehab, bowel/bladder management
- Surveillance imaging (recurrence, esp. partial treatment)
Chief-Level Case Review
Use these as the senior-level mental model for Spinal Arteriovenous Malformation (Intramedullary / Perimedullary):
- Decision point: The operation is won or lost on control: identify inflow, outflow, perforators, collateral options, and the fastest route to temporary control before exposing the lesion itself.
- Technical lever: Do not accept a cosmetic result over physiology: ICG/Doppler/DSA, branch patency, perforator preservation, and parent-vessel caliber matter more than how the clip or resection bed looks.
- Bailout: Have a rupture or ischemia script ready: lower pressure, suction strategy, temporary occlusion time, heparin/reversal plan, bypass/reconstruction threshold, and postop BP targets.
- Postop watch: Postop danger is delayed: vasospasm, thromboembolism, hyperperfusion, hemorrhage, edema, hydrocephalus, and seizure plans need explicit orders.
Common Pimp Questions
Use these to pressure-test preparation for Spinal Arteriovenous Malformation (Intramedullary / Perimedullary):
- What is the proximal-control plan before the lesion is manipulated?
- Which branch, perforator, or venous structure is most likely to be injured in this exposure?
- What are the intraoperative rupture steps, including temporary clip, suction, BP, and backup clip strategy?
- What confirms treatment success: ICG, Doppler, puncture/deflation, DSA, or postoperative CTA?
- What postoperative BP, vasospasm, antiplatelet, or anticoagulation issue changes the orders tonight?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Preferred approach side, sylvian split style, and cisternal-opening sequence: [attending-specific]
- Temporary clip threshold, burst-suppression preference, and BP during occlusion: [attending-specific]
- Clip manufacturer/shape sequence and whether Doppler, ICG, puncture, or intraop DSA is routine: [attending-specific]
- Antiplatelet/anticoagulation reversal and restart timing: [attending-specific]