
Case Prep: Lumbar Laminectomy for Spinal Stenosis
Case / Approach Snapshot
- Anatomy at risk: level localization, cord/cauda equina, exiting and traversing roots, dura, vertebral artery or segmental vessels, esophagus/trachea/pleura/viscera by approach, and fusion/instrumentation landmarks.
- Operative steps: position and pad carefully, confirm level, expose the planned corridor, decompress neural elements, reconstruct or instrument when indicated, verify alignment/hardware, and close with attention to hematoma and wound risk; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: wrong level, durotomy, neurologic change, vertebral artery/visceral/pleural injury, graft or hardware problem, epidural hematoma, dysphagia/airway issue, and infection prevention/escalation.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [single/multilevel] lumbar spinal stenosis at [L_-L_] presenting with neurogenic claudication [± radiculopathy] planned for lumbar laminectomy/decompression [without fusion].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
CNS Video Library
🧭 Operative approach: Posterior thoracolumbar approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Lumbar spinal stenosis — Genevay S. Best practice & research. Clinical rheumatology 2010. PubMed
- Surgical versus non-surgical treatment for lumbar spinal stenosis — Zaina F. The Cochrane database of systematic reviews 2016. PubMed
- Lumbar spinal stenosis — Lee JY. Instructional course lectures 2013. PubMed
- Lumbar spinal stenosis — Nowakowski P. Physical therapy 1996. PubMed
- Full-endoscopic (bi-portal or uni-portal) versus microscopic lumbar decompression laminectomy in patients with spinal stenosis: systematic review and meta-analysis — Pairuchvej S. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie 2020. PubMed
- Letter to the editor regarding “Full‑endoscopic (bi‑portal or uni‑portal) versus microscopic lumbar decompression laminectomy in patients with spinal stenosis: systematic review and meta‑analysis” — Lin GX. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie 2023. PubMed
- Spinous Process Splitting Laminectomy for Lumbar Spinal Stenosis: 2D Operative Video — Gagliardi M. World neurosurgery 2022. PubMed
- Effect of lumbar laminectomy on spinal sagittal alignment: a systematic review — Hatakka J. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 2021. PubMed
- Stand-alone interspinous spacer versus decompressive laminectomy for treatment of lumbar spinal stenosis — Lauryssen C. Expert review of medical devices 2015. PubMed
- Microendoscopic Lumbar Posterior Decompression Surgery for Lumbar Spinal Stenosis: Literature Review — Suzuki A. Medicina (Kaunas, Lithuania) 2022. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
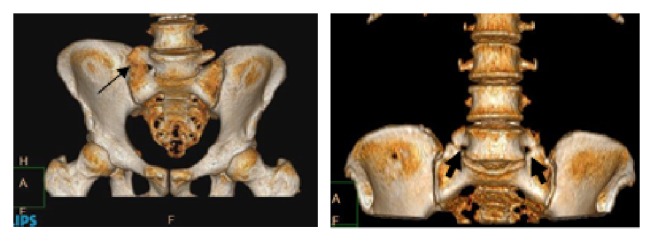 Figure 1. Lumbosacral transitional vertebra as evident in 3-dimensional images: unilateral (left) and bilateral (right) anomalies. Source: Is Lumbosacral Transitional Vertebra Associated with Degenerative Lumbar Spinal Stenosis? — BioMed Research International 2019; CC BY.
Figure 1. Lumbosacral transitional vertebra as evident in 3-dimensional images: unilateral (left) and bilateral (right) anomalies. Source: Is Lumbosacral Transitional Vertebra Associated with Degenerative Lumbar Spinal Stenosis? — BioMed Research International 2019; CC BY.
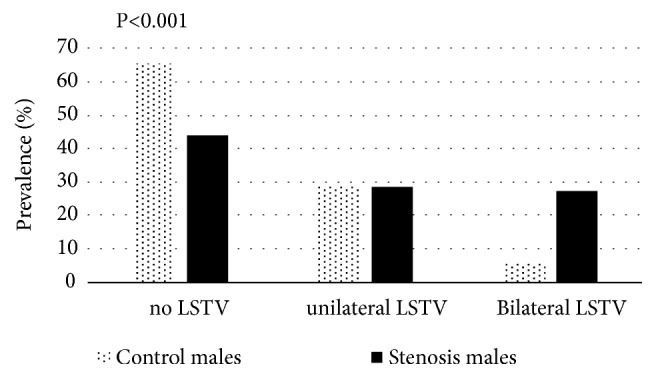 Figure 2. Prevalence (%) of lumbosacral transitional vertebra (LSTV) in the male groups (control vs. stenosis). Source: Is Lumbosacral Transitional Vertebra Associated with Degenerative Lumbar Spinal Stenosis? — BioMed Research International 2019; CC BY.
Figure 2. Prevalence (%) of lumbosacral transitional vertebra (LSTV) in the male groups (control vs. stenosis). Source: Is Lumbosacral Transitional Vertebra Associated with Degenerative Lumbar Spinal Stenosis? — BioMed Research International 2019; CC BY.
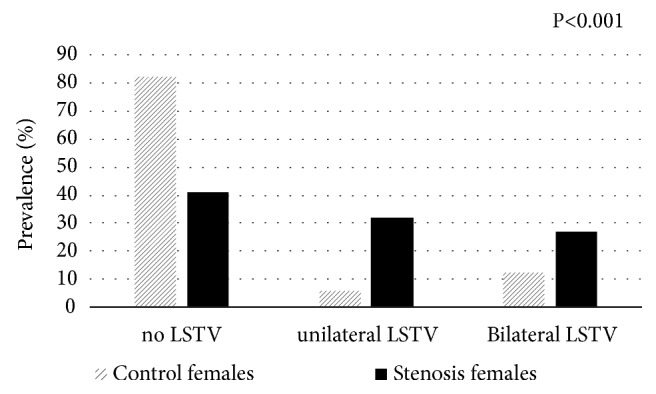 Figure 3. Prevalence (%) of lumbosacral transitional vertebra (LSTV) type in the female groups (control vs. stenosis). Source: Is Lumbosacral Transitional Vertebra Associated with Degenerative Lumbar Spinal Stenosis? — BioMed Research International 2019; CC BY.
Figure 3. Prevalence (%) of lumbosacral transitional vertebra (LSTV) type in the female groups (control vs. stenosis). Source: Is Lumbosacral Transitional Vertebra Associated with Degenerative Lumbar Spinal Stenosis? — BioMed Research International 2019; CC BY.
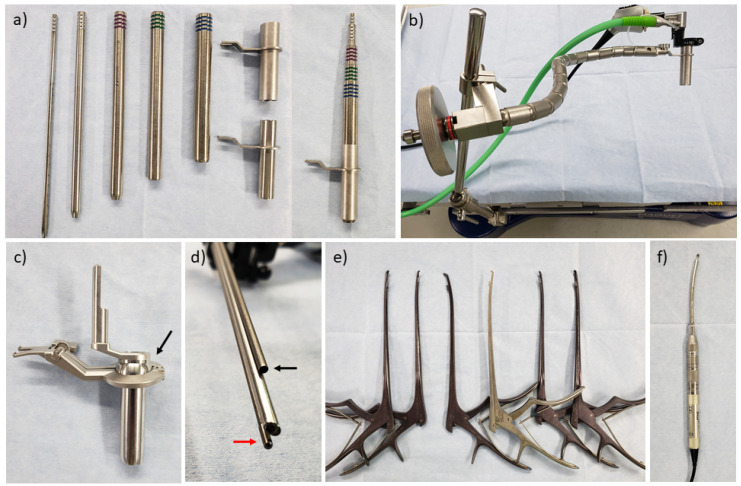 Figure 1. Surgical equipment for tubular microendoscopic decompression surgery. (a) Serial tubular dilator and retractor (METRx®). (b) Flexible arm assembly (METRx®). (c) Tubular retractor of the… Source: Microendoscopic Lumbar Posterior Decompression Surgery for Lumbar Spinal Stenosis: Literature Review — Medicina 2022; CC BY.
Figure 1. Surgical equipment for tubular microendoscopic decompression surgery. (a) Serial tubular dilator and retractor (METRx®). (b) Flexible arm assembly (METRx®). (c) Tubular retractor of the… Source: Microendoscopic Lumbar Posterior Decompression Surgery for Lumbar Spinal Stenosis: Literature Review — Medicina 2022; CC BY.
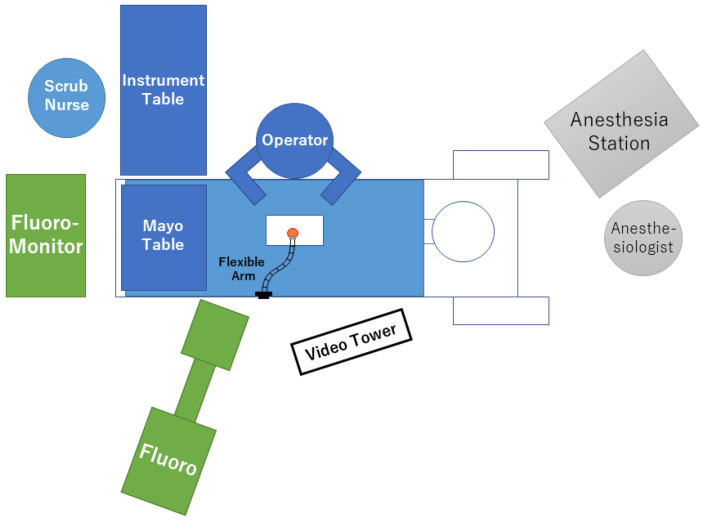 Figure 2. Schematic presentation of the room setup. Source: Microendoscopic Lumbar Posterior Decompression Surgery for Lumbar Spinal Stenosis: Literature Review — Medicina 2022; CC BY.
Figure 2. Schematic presentation of the room setup. Source: Microendoscopic Lumbar Posterior Decompression Surgery for Lumbar Spinal Stenosis: Literature Review — Medicina 2022; CC BY.
History of Present Illness
- Chief complaint: Neurogenic claudication — bilateral buttock/leg pain, heaviness, paresthesias with standing/walking, relieved by sitting/flexion (“shopping cart sign”), worse with extension
- Walking tolerance, radicular symptoms, failed conservative management (PT, injections)
- Decompression alone (no fusion) if no instability/deformity/spondylolisthesis with motion
Past Medical History
- Spondylolisthesis (if present with instability → add fusion), prior lumbar surgery
- Vascular claudication (differentiate — pulses, ABI), diabetes, cardiac (pre-op clearance for elderly)
- Standard PMH
Imaging Review
MRI Lumbar
- Central/lateral recess/foraminal stenosis levels, ligamentum flavum hypertrophy, facet hypertrophy, disc bulging
- Cauda equina crowding, redundant nerve roots
X-ray (flexion/extension)
- Instability/spondylolisthesis (determines if fusion needed), alignment
CT
- Bony anatomy, facet morphology, ossification
Labs
- CBC, BMP, Coags, Type and screen
Neurological Examination
- Lower extremity motor/sensory/reflex, gait, often near-normal at rest (dynamic symptoms)
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: Wilson frame, Andrews/knee-chest frame, or Jackson/open-frame table by surgeon preference; flexion opens the interlaminar window and the abdomen must hang free.
- OR setup: radiolucent/Jackson table, fluoroscopy or O-arm/navigation, microscope/loupes for decompression, implant trays/graft ready for fusion, neuromonitoring for myelopathy/cord-risk cases, and postop brace plan confirmed.
- Special needs: arterial line/Foley/type-screen for long fusion/corpectomy, no long paralytic when MEPs are used, MAP/normotension for myelopathy or cord-risk cases, antibiotic redosing, and anticoagulation/DVT plan.
- Immediate postop orders: neuro checks by myotome/sensory level, airway/dysphagia watch for anterior cervical cases, CT/X-rays per construct, drain care, brace/activity orders, DVT prophylaxis timing, bowel regimen, and PT/OT mobilization.
Decompression without Fusion vs With Fusion
- Laminectomy alone: stenosis without instability/deformity
- Add fusion: spondylolisthesis with instability, scoliosis, if facetectomy needed for decompression destabilizes, recurrent stenosis
Position
- OR table/bed: Wilson frame, Andrews/knee-chest frame, or Jackson/open-frame table by surgeon preference; flexion opens the interlaminar window and the abdomen must hang free.
- Prone on Jackson/Wilson frame, abdomen free, hips flexed, pressure points padded, eyes free
Key Surgical Steps — Detailed
- Fluoroscopic level confirmation — localize with a spinal needle/marker, counting from the sacrum (and account for transitional anatomy/lumbosacral variants on the preop films); confirm the correct level before bony work
- Midline incision over the target levels; subperiosteal dissection of the paraspinal muscles off the spinous processes and laminae bilaterally (for central decompression), exposing out to the medial facets; place self-retaining retractors; re-confirm level
- Laminectomy: remove the spinous process and laminae at the stenotic level(s) — thin the lamina with a high-speed drill and/or use Kerrison rongeurs; begin in the midline where the canal is roomiest and work laterally; identify the ligamentum flavum as the deep layer protecting the dura
- Remove the hypertrophied ligamentum flavum (a major compressive element) — develop the plane off the underlying dura with a blunt dissector, then resect with Kerrisons, protecting the thecal sac
- Decompress the lateral recesses — undercut the hypertrophied superior articular facets (medial facetectomy), freeing the traversing nerve roots; preserve > 50% of each facet and the pars interarticularis to avoid iatrogenic instability
- Foraminal decompression — follow and decompress the exiting roots into the foramina; confirm each root is free with a probe/Woodson (ball-tip passes freely)
- Confirm adequate decompression — the dura re-expands and pulsates, traversing and exiting roots are free in the recesses/foramina
- (MIS alternative) — unilateral tubular approach with “over-the-top” contralateral decompression: undercut the base of the spinous process and contralateral lamina/ligamentum, decompressing both sides through a unilateral corridor while preserving the midline tension band (less destabilizing)
- Inspect for durotomy (common in tight stenosis with redundant roots/adhesions) — repair primarily (suture ± sealant/patch) if encountered
- Hemostasis of the epidural venous plexus (bipolar, hemostatic matrix, gentle), confirm no compressive hematoma, ± subfascial drain, layered closure
Critical Anatomy & Structures at Risk
- Dura / thecal sac / cauda equina — durotomy risk (esp. adherent in stenosis, redundant roots)
- Nerve roots (traversing and exiting) in lateral recess/foramen
- Pars interarticularis & facets — preserve to avoid iatrogenic instability/spondylolisthesis
- Epidural venous plexus
Equipment
- High-speed drill, Kerrison rongeurs, curettes, rongeurs
- Fluoroscopy, microscope/loupes, bipolar, hemostatic agents
- Tubular retractors (if MIS), drain
Monitoring
- Optional EMG/SSEP (typically not required for routine laminectomy)
Anesthesia
- General, prone precautions, SBP control (bleeding), TXA optional
Potential Complications
- Dural tear/CSF leak (common in stenosis — repair, flat bed rest)
- Iatrogenic instability (excess facet/pars removal → may need fusion)
- Nerve root injury, epidural hematoma (new deficit → emergent MRI/return to OR)
- Recurrent stenosis, incomplete decompression, infection
Operative Note Template
Preoperative Diagnosis: Lumbar spinal stenosis at [L_-L_] with neurogenic claudication [± radiculopathy]
Postoperative Diagnosis: Same
Procedure: Lumbar laminectomy and decompression of the central canal, lateral recesses, and foramina at [L_-L_]
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Specimens: [Ligamentum flavum / bone — or none] Drains: [± subfascial drain] Implants: None Complications: None [/ incidental durotomy, repaired]
Indications: [Age]yo [M/F] with neurogenic claudication [and __ radiculopathy] from multilevel lumbar stenosis at [L-L_], refractory to conservative management (PT, injections), without instability on flexion-extension films. Risks/benefits/alternatives discussed; the patient elected decompression.
Description of Procedure: After consent and time-out, general anesthesia was induced. The patient was positioned prone on a [Jackson/Wilson] frame with the abdomen free and all pressure points and eyes padded. The back was prepped and draped and antibiotics given. The level was confirmed fluoroscopically.
A midline incision was made over [L_-L_] and subperiosteal dissection exposed the laminae bilaterally; the level was re-confirmed. A laminectomy was performed at [levels], thinning the laminae with a high-speed drill and completing with Kerrison rongeurs. The hypertrophied ligamentum flavum was removed off the dura, decompressing the central canal. The lateral recesses were decompressed by undercutting the medial facets (preserving >50% of the facets and the pars), freeing the traversing nerve roots, and the foramina were opened and confirmed patent with a probe. The thecal sac re-expanded and pulsated, and all roots were free. [The dura was inspected and intact / a small durotomy was repaired primarily with sealant.]
Meticulous epidural hemostasis was obtained, [a subfascial drain placed,] and the wound closed in anatomic layers. The patient was awakened neurologically at baseline and transferred to recovery in stable condition.
Postoperative Plan
- Floor, neuro checks, mobilize POD0/1
- If durotomy: flat bed rest 24-48h
- Pain control, DVT prophylaxis (SCDs, early ambulation)
- Activity progression, PT
- Follow-up 2-4 weeks; counsel re: claudication relief, possible need for future fusion if instability develops
Chief-Level Case Review
Use these as the senior-level mental model for Lumbar Laminectomy for Spinal Stenosis:
- Decision point: Localize twice and instrument once: numbering, transitional anatomy, prior hardware, rib count, navigation dataset, and fluoroscopic level confirmation are mandatory.
- Technical lever: Positioning is treatment: table choice, abdomen-free prone setup, alignment goals, shoulders/hips, eyes/plexus pressure, neuromonitoring baselines, and fluoroscopic access all change the case.
- Bailout: Protect neural elements by sequence: decompression before correction when needed, MAP support for cord risk, no long paralytic with MEPs, and immediate response to signal change.
- Postop watch: Finish with construct logic: decompression adequacy, screw purchase, alignment, fusion bed/graft, drain plan, brace/activity orders, postop CT/X-rays, and DVT timing.
Common Pimp Questions
Use these to pressure-test preparation for Lumbar Laminectomy for Spinal Stenosis:
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]