
Operative Approach: Transpsoas Lateral Approach (LLIF / XLIF / OLIF) to the Lumbar Spine
Case / Approach Snapshot
- Anatomy at risk: corridor-defining nerves, arteries, veins/sinuses, cisterns, bone landmarks, muscle/fascial planes, and closure structures that determine exposure and morbidity.
- Operative steps: confirm position and trajectory, mark landmarks, protect soft tissue and named neurovascular structures, perform the bone/soft-tissue corridor, open/close dura or target compartment deliberately, and verify hemostasis/reconstruction; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: brain relaxation failure, venous or sinus bleeding, cranial nerve/perforator risk, exposure that is too narrow, CSF leak, cosmetic/temporalis/frontalis problems, and conversion to a wider or alternate corridor.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
CNS Video Library
AO Spine / Surgery Reference — lateral approach · Neurosurgical Atlas — Spine · Radiopaedia — XLIF/OLIF · PubMed Central — transpsoas safe zone
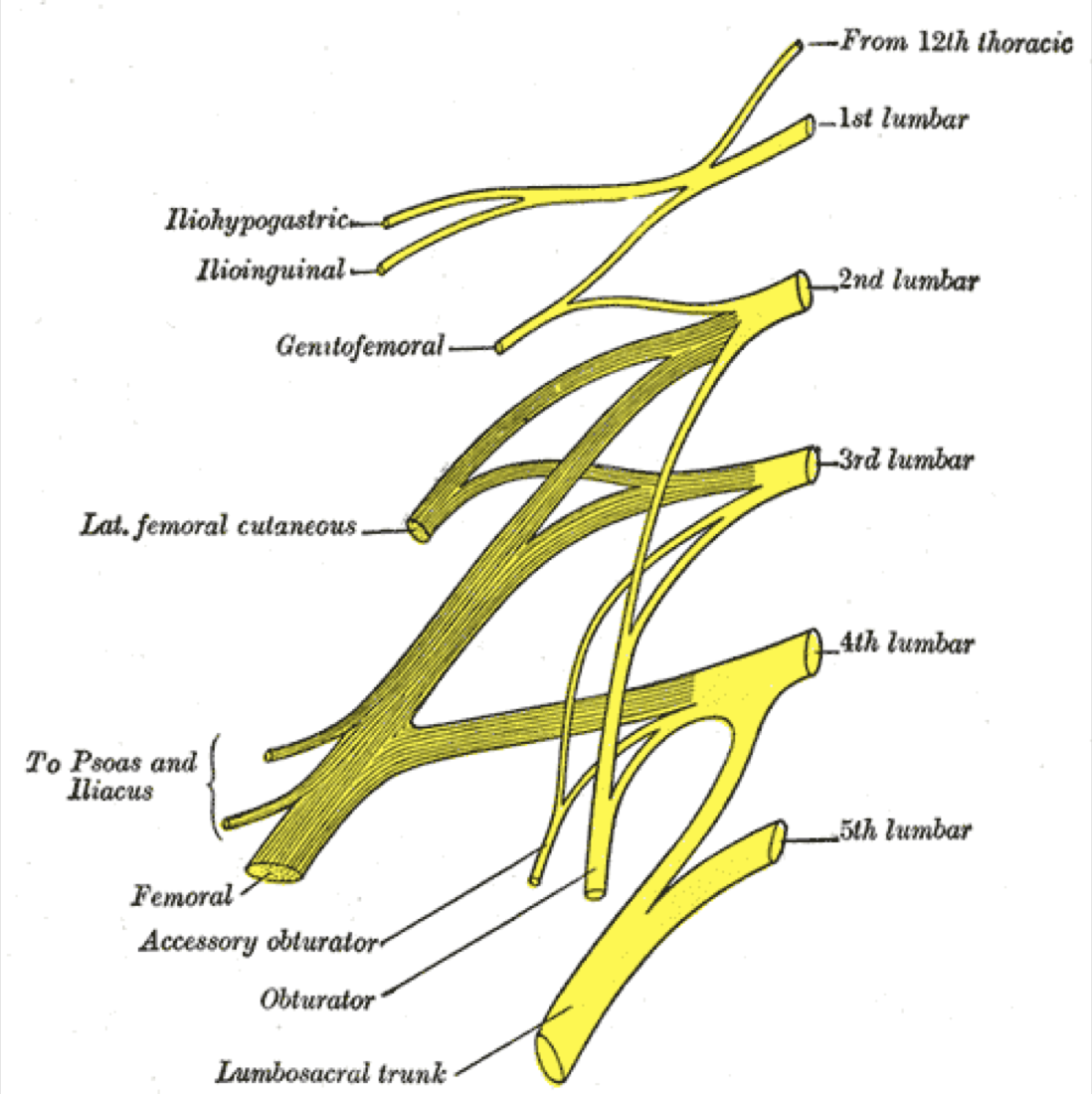
Gray’s Anatomy (1918), public domain — via Wikimedia Commons. The lumbar plexus forms within the psoas; its branches migrate ventrally as you descend, making L4–5 the highest-risk level.
High-Yield Literature
- Transpsoas Approaches to the Lumbar Spine: Lateral and Prone — White MD. Neurosurgery clinics of North America 2023. PubMed
- Minimally invasive lateral transpsoas approach to the lumbar spine: pitfalls and complication avoidance — Graham RB. Neurosurgery clinics of North America 2014. PubMed
- Prone Transpsoas Lateral Lumbar Interbody Fusion for Degenerative Lumbar Spine Disease: Case Series With an Operative Video Using Fluoroscopy-Based Instrument Tracking Guidance — Soliman MAR. Operative neurosurgery (Hagerstown, Md.) 2022. PubMed
- Lateral transpsoas lumbar interbody fusion: outcomes and deformity correction — Dahdaleh NS. Neurosurgery clinics of North America 2014. PubMed
- Endoscopic lateral transpsoas approach to the lumbar spine — Bergey DL. Spine 2004. PubMed
- Transpsoas Approach Nuances — Hlubek RJ. Neurosurgery clinics of North America 2018. PubMed
- Lateral Transpsoas Interbody Fusion — Sullivan TB. International journal of spine surgery 2025. PubMed
- Prone transpsoas lumbar corpectomy: simultaneous posterior and lateral lumbar access for difficult clinical scenarios — Gandhi SD. Journal of neurosurgery. Spine 2021. PubMed
- The lateral transpsoas approach to the lumbar and thoracic spine: A review — Arnold PM. Surgical neurology international 2012. PubMed
- Minimally invasive lateral retroperitoneal transpsoas approach for lumbar corpectomy and fusion with posterior instrumentation — Srinivasan ES. Neurosurgical focus: Video 2022. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
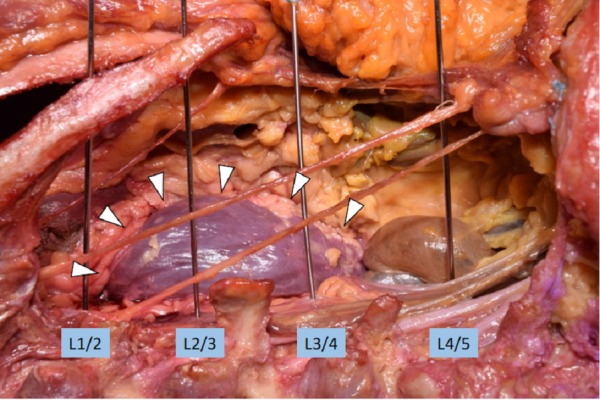 Figure 1. Measurement of the closest distance from the wire for the disc space of L1/2, L2/3 and L3/4 to the kidney (arrowheads). Source: Anatomical Study of the Extreme Lateral Transpsoas Lumbar Interbody Fusion with Application to Minimizing Injury to the Kidney — Cureus 2018; CC BY.
Figure 1. Measurement of the closest distance from the wire for the disc space of L1/2, L2/3 and L3/4 to the kidney (arrowheads). Source: Anatomical Study of the Extreme Lateral Transpsoas Lumbar Interbody Fusion with Application to Minimizing Injury to the Kidney — Cureus 2018; CC BY.
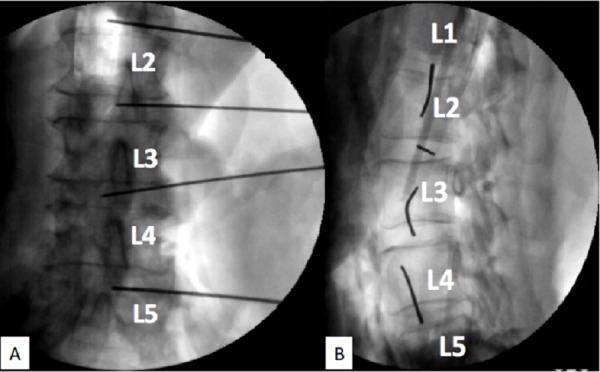 Figure 2. Fluoroscopy of the wire trajectory. Note that all the wires are within disc spaces.A: Lateral viewB: Posterior-anterior view Source: Anatomical Study of the Extreme Lateral Transpsoas Lumbar Interbody Fusion with Application to Minimizing Injury to the Kidney — Cureus 2018; CC BY.
Figure 2. Fluoroscopy of the wire trajectory. Note that all the wires are within disc spaces.A: Lateral viewB: Posterior-anterior view Source: Anatomical Study of the Extreme Lateral Transpsoas Lumbar Interbody Fusion with Application to Minimizing Injury to the Kidney — Cureus 2018; CC BY.
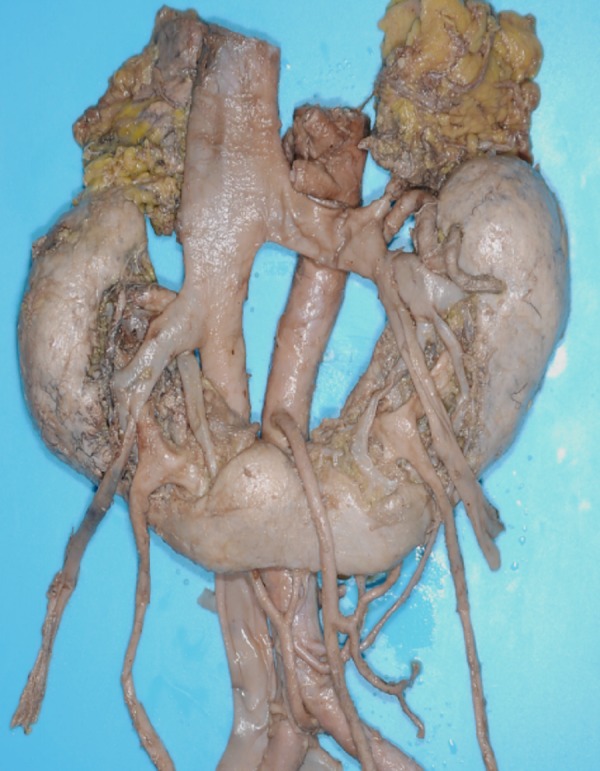 Figure 3. Horseshoe kidney.Slightly lower than normal kidney and often having aberrant renal arteries. Source: Anatomical Study of the Extreme Lateral Transpsoas Lumbar Interbody Fusion with Application to Minimizing Injury to the Kidney — Cureus 2018; CC BY.
Figure 3. Horseshoe kidney.Slightly lower than normal kidney and often having aberrant renal arteries. Source: Anatomical Study of the Extreme Lateral Transpsoas Lumbar Interbody Fusion with Application to Minimizing Injury to the Kidney — Cureus 2018; CC BY.
 Figure 4. Laterally malrotated kidney.Right renal artery entering the laterally faced hilum (arrows). Source: Anatomical Study of the Extreme Lateral Transpsoas Lumbar Interbody Fusion with Application to Minimizing Injury to the Kidney — Cureus 2018; CC BY.
Figure 4. Laterally malrotated kidney.Right renal artery entering the laterally faced hilum (arrows). Source: Anatomical Study of the Extreme Lateral Transpsoas Lumbar Interbody Fusion with Application to Minimizing Injury to the Kidney — Cureus 2018; CC BY.
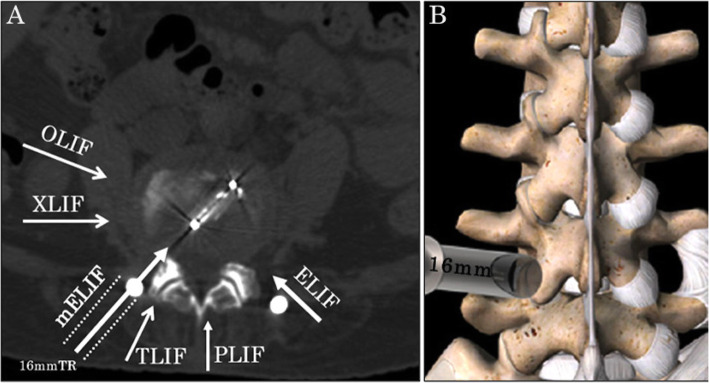 Fig. 1. Schema of the approach. a Schema on a CT axial image. The approach for mELIF is more lateral than that of TLIF. The spinal canal is not surgically invaded. b Drawing from the posterior… Source: Microendoscopy-assisted extraforaminal lumbar interbody fusion for treating single-level spondylodesis — Journal of Orthopaedic Surgery and Research 2021; CC BY.
Fig. 1. Schema of the approach. a Schema on a CT axial image. The approach for mELIF is more lateral than that of TLIF. The spinal canal is not surgically invaded. b Drawing from the posterior… Source: Microendoscopy-assisted extraforaminal lumbar interbody fusion for treating single-level spondylodesis — Journal of Orthopaedic Surgery and Research 2021; CC BY.
 Fig. 2. Fluoroscopic images during surgery. a A tubular retractor with a microendoscope installed posterolaterally on the anteroposterior view. Four percutaneous pedicle screw guide wires were… Source: Microendoscopy-assisted extraforaminal lumbar interbody fusion for treating single-level spondylodesis — Journal of Orthopaedic Surgery and Research 2021; CC BY.
Fig. 2. Fluoroscopic images during surgery. a A tubular retractor with a microendoscope installed posterolaterally on the anteroposterior view. Four percutaneous pedicle screw guide wires were… Source: Microendoscopy-assisted extraforaminal lumbar interbody fusion for treating single-level spondylodesis — Journal of Orthopaedic Surgery and Research 2021; CC BY.
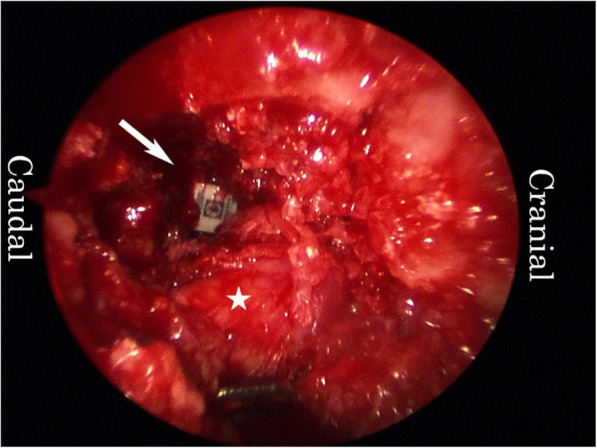 Fig. 3. Endoscopic image. An interbody cage was inserted into the disc space. Arrow head: cage. Asterisk: right L5 exiting nerve root Source: Microendoscopy-assisted extraforaminal lumbar interbody fusion for treating single-level spondylodesis — Journal of Orthopaedic Surgery and Research 2021; CC BY.
Fig. 3. Endoscopic image. An interbody cage was inserted into the disc space. Arrow head: cage. Asterisk: right L5 exiting nerve root Source: Microendoscopy-assisted extraforaminal lumbar interbody fusion for treating single-level spondylodesis — Journal of Orthopaedic Surgery and Research 2021; CC BY.
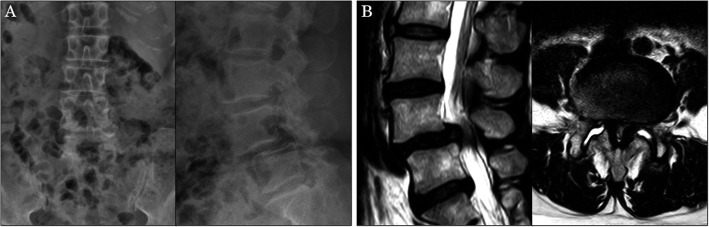 Fig. 4. Images at presentation. a Anteroposterior and lateral X-ray films. Note grade II spondylolisthesis at L4/5. b Sagittal and axial magnetic resonance images. The spinal canal is severely… Source: Microendoscopy-assisted extraforaminal lumbar interbody fusion for treating single-level spondylodesis — Journal of Orthopaedic Surgery and Research 2021; CC BY.
Fig. 4. Images at presentation. a Anteroposterior and lateral X-ray films. Note grade II spondylolisthesis at L4/5. b Sagittal and axial magnetic resonance images. The spinal canal is severely… Source: Microendoscopy-assisted extraforaminal lumbar interbody fusion for treating single-level spondylodesis — Journal of Orthopaedic Surgery and Research 2021; CC BY.
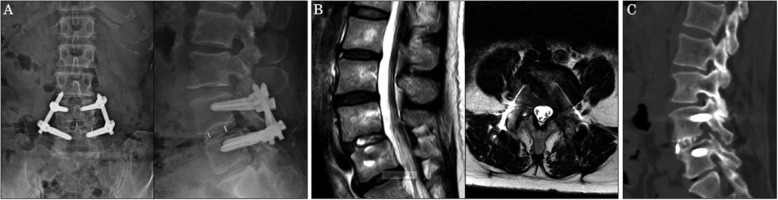 Fig. 5. Images at 1-year post-surgery. a Anteroposterior and lateral X-ray films. Spondylolisthesis was corrected, and the hardware was in place. b Sagittal and axial magnetic resonance images…. Source: Microendoscopy-assisted extraforaminal lumbar interbody fusion for treating single-level spondylodesis — Journal of Orthopaedic Surgery and Research 2021; CC BY.
Fig. 5. Images at 1-year post-surgery. a Anteroposterior and lateral X-ray films. Spondylolisthesis was corrected, and the hardware was in place. b Sagittal and axial magnetic resonance images…. Source: Microendoscopy-assisted extraforaminal lumbar interbody fusion for treating single-level spondylodesis — Journal of Orthopaedic Surgery and Research 2021; CC BY.
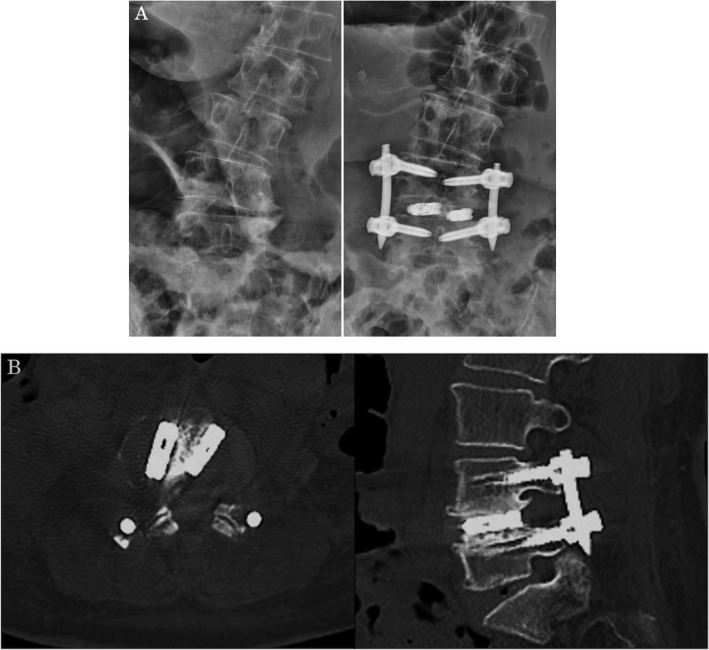 Fig. 6. Insertion of two cages. a Anteroposterior X-ray films before and after surgery. b Computed tomography sagittal and axial images Source: Microendoscopy-assisted extraforaminal lumbar interbody fusion for treating single-level spondylodesis — Journal of Orthopaedic Surgery and Research 2021; CC BY.
Fig. 6. Insertion of two cages. a Anteroposterior X-ray films before and after surgery. b Computed tomography sagittal and axial images Source: Microendoscopy-assisted extraforaminal lumbar interbody fusion for treating single-level spondylodesis — Journal of Orthopaedic Surgery and Research 2021; CC BY.
The transpsoas lateral approach reaches the lumbar disc spaces (L1–2 through L4–5) from the side, through a retroperitoneal, trans-psoas corridor, to place a large interbody cage spanning the strong apophyseal ring. That big cage gives powerful indirect decompression, deformity (coronal) correction, and fusion with minimal posterior muscle disruption. Its defining hazard is the lumbar plexus, which runs within the psoas — so the approach is built around neuromonitoring and disc-level “safe zones.” (The OLIF/anterior-to-psoas variant slips in front of the psoas to avoid traversing the plexus, trading off vascular proximity.)
General Considerations
- What it accesses: L1–2 to L4–5 disc spaces laterally (NOT L5–S1 — the iliac crest blocks it; use ALIF or TLIF there). Often combined with posterior percutaneous screws.
- Why a lateral cage: a wide cage resting on the dense apophyseal ring restores disc/foraminal height (indirect decompression), corrects coronal deformity, and fuses — with far less posterior muscle damage than open PLIF/TLIF.
- The plexus rule: the lumbar plexus lies in the posterior third of the disc/vertebral body in the upper levels but the nerves shift anteriorly at L4–5, narrowing the safe window — hence continuous/triggered EMG and docking in the mid-to-posterior disc “safe zone” (Moro zones), with caution at L4–5.
- OLIF (anterior-to-psoas): an oblique retroperitoneal window in front of the psoas avoids traversing the plexus but works next to the great vessels/segmental vessels — a different risk profile.
Indications
- Degenerative disc disease, spondylolisthesis, adjacent-segment disease, recurrent stenosis needing indirect decompression → XLIF/OLIF
- Adult degenerative scoliosis / coronal deformity (powerful interbody correction) → adult deformity
- Selected trauma/tumor/infection requiring anterior column support
Relative contraindications
- L5–S1 (iliac crest), severe rotatory scoliosis/retroperitoneal scarring, a “rising/high” psoas with anteriorly displaced plexus, prior retroperitoneal surgery.
Relevant Surgical Anatomy
- Layers (lateral, retroperitoneal): skin → external oblique → internal oblique → transversus abdominis → retroperitoneal fat → psoas major.
- Lumbar plexus: forms within the psoas; femoral nerve and the motor components are dorsal; the genitofemoral nerve runs on the ventral/anterior surface of the psoas (groin/anterior-thigh symptoms if injured). Subcostal/iliohypogastric/ilioinguinal nerves cross the abdominal-wall corridor.
- Anterior structures: aorta/IVC and iliac vessels, segmental vessels, sympathetic chain, ureter, and bowel — anterior to the working zone (OLIF concern).
- Disc/endplate: target the apophyseal ring; violate the endplate → subsidence.
Preoperative Evaluation
- MRI: plexus position and psoas morphology (axial — a “rising psoas” pushes nerves anterior), level, vascular anatomy; side selection (usually approach the concavity in scoliosis, away from great vessels). Standing films for alignment.
- Confirm L5–S1 is not the target; assess iliac crest height vs L4–5.
Case-Selection and Side Strategy
- Best fit: L1-2 through L4-5 disc access for indirect decompression, coronal correction, disc-height restoration, and large-footprint interbody support when posterior-only access is less attractive.
- Caution/avoid: high iliac crest at L4-5, severe psoas migration/rising psoas, plexus anterior to the disc target, active infection through the corridor, retroperitoneal scarring, anomalous vessels, or severe central stenosis where indirect decompression is unlikely.
- Side selection balances deformity concavity, vascular position, prior abdominal/retroperitoneal surgery, symptoms, and the working-room available between rib, iliac crest, and plexus.
- Plan supplemental posterior fixation when instability, deformity correction, spondylolisthesis, osteoporosis, or multilevel constructs make standalone lateral cage failure likely.
Logistics, OR Setup & Orders
- OR table/bed: radiolucent lateral-decubitus table with iliac crest near the table break, true AP/lateral fluoroscopy, hips/knees flexed, and secure taping.
- OR setup: Jackson/radiolucent spine table or approach-specific lateral/anterior setup, C-arm/O-arm/navigation availability, microscope/loupes, neuromonitoring leads before positioning, and implant trays opened only after final level/plan confirmation.
- Special needs: arterial line and Foley for long instrumented cases, type/screen or crossmatch for deformity/corpectomy/trauma, antibiotic redosing plan, MAP support for SCI/myelopathy, and no long paralytic when MEPs are needed.
- Immediate postop orders: neuro checks focused on myotomes/sensory level, postop CT/X-rays per construct, brace/activity orders, drain output thresholds, DVT prophylaxis timing, dysphagia/airway monitoring for anterior cervical cases, and rehab mobilization plan.
Anesthesia & Neuromonitoring
- GA; continuous and triggered EMG is mandatory (femoral/plexus), with no long-acting paralytic; fluoroscopy. Some add MEP/SSEP for deformity.
Positioning
- OR table/bed: radiolucent lateral-decubitus table with iliac crest near the table break, true AP/lateral fluoroscopy, hips/knees flexed, and secure taping.
- True 90° lateral decubitus, secured to the table (tape at iliac crest, chest, legs); break/flex the table at the level to open the space between the iliac crest and ribs (and lengthen the lateral abdominal wall). Obtain true orthogonal AP and lateral fluoroscopy (the implant trajectory depends on it). Pad the down-side, axillary roll, flex the hip slightly to relax the psoas/plexus.
Approach & Docking
- Lateral skin incision over the target disc (± a second posterolateral incision for finger-guided retroperitoneal access); bluntly split the abdominal-wall muscles and enter the retroperitoneal space, sweeping the peritoneum/contents anteriorly.
- Palpate the psoas and the transverse process; dock the initial dilator on the disc at the safe zone (mid-to-posterior body; more anterior caution at L4–5) under fluoroscopy.
- Traverse the psoas with sequential dilators under continuous/triggered EMG — advance slowly, redirect if EMG thresholds drop (plexus nearby); seat the retractor and expose the disc.
Discectomy & Interbody
- Complete discectomy, release the contralateral annulus (for correction/cage width), prepare endplates without violating them (subsidence), and place a wide lateral cage on the apophyseal ring (lordotic/large footprint). ± lateral plate and/or posterior percutaneous pedicle screws. Confirm position on fluoroscopy.
Closure
- Confirm hemostasis and an intact peritoneum; allow the psoas to fall back; close the abdominal-wall layers and skin. No drain typically.
Bony anatomy (vertebra / pedicle detail)
Retroperitoneal corridor & psoas anatomy
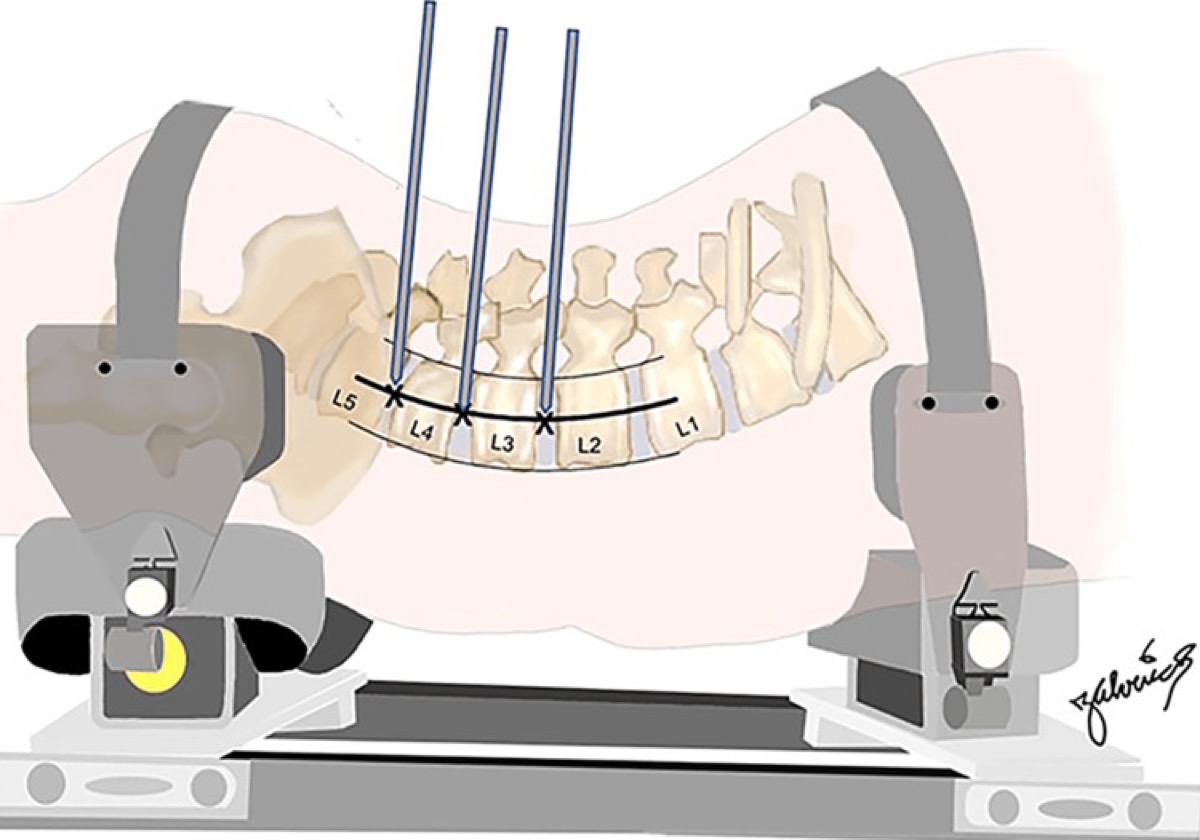
Cureus 2023;15(7):e41733 — CC BY 4.0.
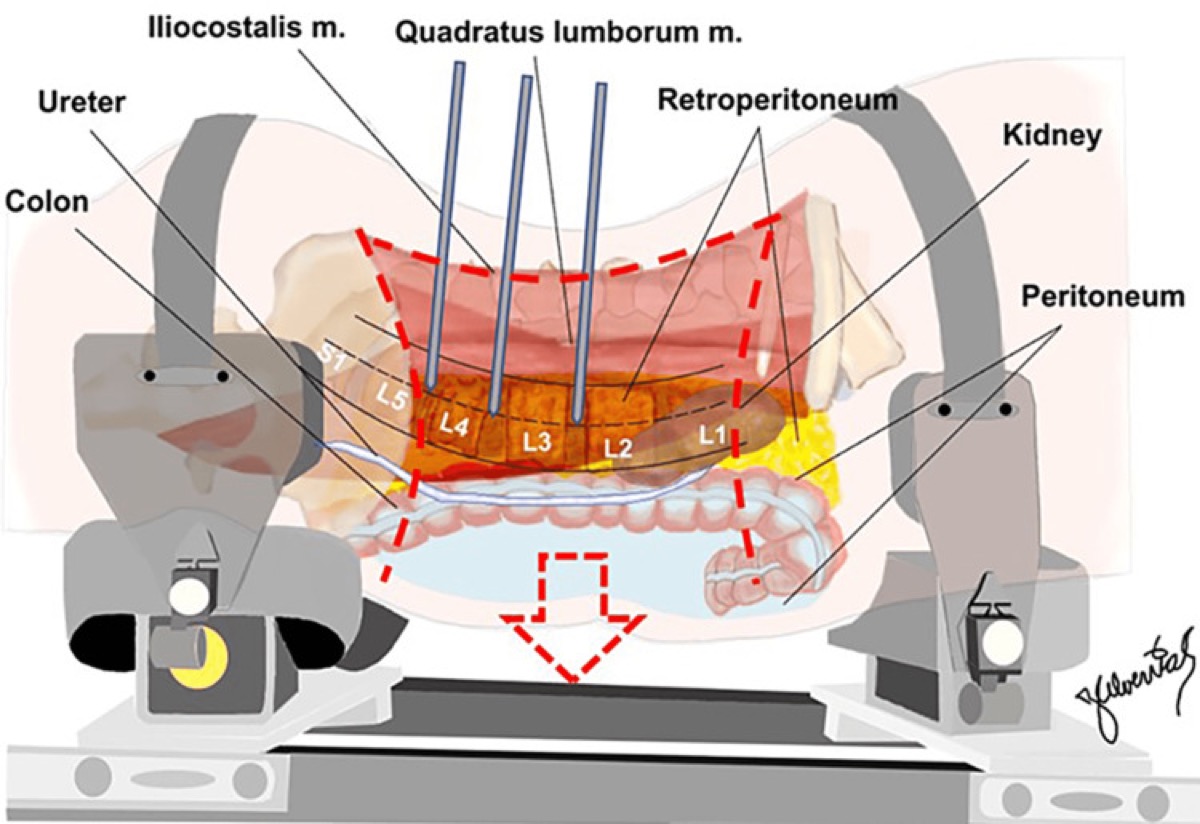
Cureus 2023;15(7):e41733 — CC BY 4.0.
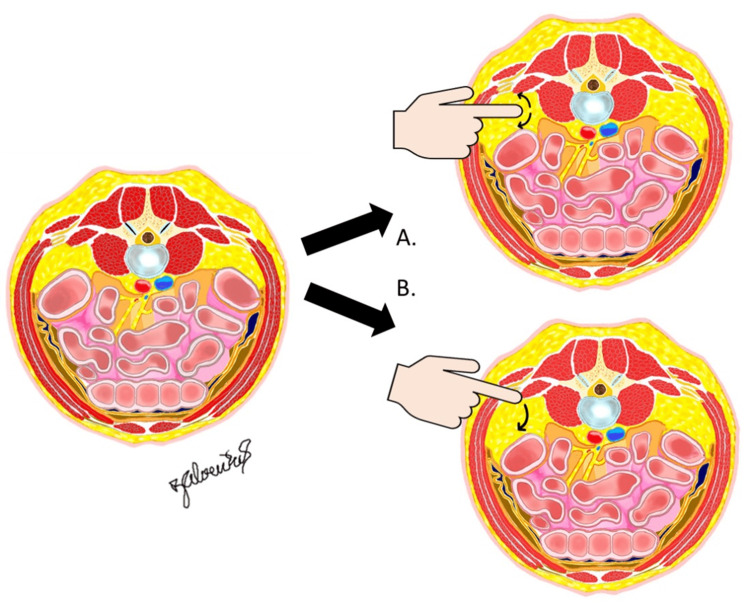
Cureus 2023;15(7):e41733 — CC BY 4.0.
Nuances & Pitfalls (surgeon-level)
- The lumbar plexus is the case. Use continuous + triggered EMG, dock in the safe zone, traverse the psoas slowly, and respect L4–5 (plexus most anterior). Expect transient hip-flexor/psoas weakness and anterior-thigh numbness; warn the patient.
- Genitofemoral nerve on the anterior psoas → groin/anterior-thigh dysesthesia; avoid anterior dissection on the psoas surface.
- Endplate violation → subsidence; prepare carefully and size the cage to the ring.
- Great vessels/segmental vessels and ureter are anterior (OLIF especially) — know where they are; control segmental bleeding.
- Side selection & table break determine the whole case — true lateral and true orthogonal fluoro are non-negotiable.
- Not for L5–S1 (iliac crest) — plan ALIF/TLIF there.
Intraoperative Rescue Logic
- Low triggered EMG threshold while dilating: stop, withdraw to a safe depth, redirect more anterior/posterior per anatomy and fluoroscopy, and abandon the level if no safe corridor exists.
- Loss of true AP/lateral fluoroscopy: reposition before docking or cage insertion; oblique imaging can make a safe-looking trajectory violate endplate, canal, or anterior vessels.
- Peritoneal breach: inspect bowel/contents, close or consult general surgery if significant, and do not leave the cage corridor contaminated or unstable.
- Segmental/great-vessel bleeding: pack, maintain exposure, avoid blind bipolar deep to psoas, and obtain vascular help early for brisk anterior bleeding.
- Endplate fracture/subsidence during trialing: upsize footprint only if safe, reduce distraction, consider supplemental posterior fixation, and avoid forcing lordosis through weak bone.
- Postoperative femoral neuropathy: check psoas hematoma with imaging if severe/progressive, document quadriceps/iliopsoas strength, and distinguish expected transient psoas irritation from compressive injury.
Complications
Lumbar plexus / femoral nerve injury (quadriceps/hip-flexor weakness), anterior-thigh numbness & groin pain (genitofemoral), transient psoas weakness; cage subsidence; vascular injury (great/segmental vessels — OLIF), ureteral/bowel injury; retroperitoneal hematoma; incisional hernia/abdominal-wall pseudohernia (flank bulge); pseudarthrosis.
Cross-links
- Procedures: XLIF / OLIF · ALIF · adult deformity
- Related corridors: posterior-thoracolumbar-approach.md · transthoracic-approach.md
Figure Use & Attribution
About the figures. Copyrighted operative figures/videos are linked (Neurosurgical Atlas, AO Spine / Surgery Reference); embedded images are public-domain (Gray’s Anatomy), credited beneath each image. See media-sources.md and figures/CREDITS.md.
Technique references: AO Spine / Surgery Reference — Lateral lumbar · Neurosurgical Atlas — Spine · Radiopaedia — LLIF
Chief-Level Corridor Review
Use these as the senior-level mental model for Transpsoas Lateral Approach (LLIF / XLIF / OLIF) to the Lumbar Spine:
- Decision point: Define the exposure goal before incision: target, working angles, proximal/distal control, and the structure that cannot tolerate retraction.
- Technical lever: Know the first irreversible step: bone removal, dural opening, vascular control, or muscle/fascial division that commits the corridor.
- Bailout: Verbalize the bailout: extend exposure, change trajectory, add CSF drainage, obtain proximal control, convert to a larger corridor, or stop for imaging.
- Postop watch: Protect closure from the start: vascularized tissue, watertight dural/reconstruction plan, dead-space control, and drain strategy should be chosen before the final intradural step.
Common Pimp Questions
Use these to pressure-test preparation for Transpsoas Lateral Approach (LLIF / XLIF / OLIF) to the Lumbar Spine:
- What patient position and head rotation make gravity work for this corridor?
- What named nerve, vessel, sinus, or muscle/fascial plane is most commonly injured?
- What bone work or soft-tissue step creates the exposure rather than simply using more retraction?
- What is the bailout if exposure is inadequate, bleeding occurs, or the brain is tight?
- What closure maneuver prevents the signature complication of this approach?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Exact head rotation/flexion/extension and pin placement: [attending-specific]
- Skin incision length, flap type, and muscle/fascial preservation technique: [attending-specific]
- Drill, rongeur, endoscope, microscope, retractor, and navigation preferences: [attending-specific]
- Drain use, closure materials, watertightness threshold, and postop imaging routine: [attending-specific]
Case Guides Using This Approach
References
- Ozgur BM, Aryan HE, Pimenta L, Taylor WR. Extreme lateral interbody fusion (XLIF): a novel surgical technique for anterior lumbar interbody fusion. Spine J. 2006;6(4):435–443.
- Moro T, Kikuchi S, Konno S, Yaginuma H. An anatomic study of the lumbar plexus with respect to retroperitoneal endoscopic surgery. Spine. 2003;28(5):423–428.
- Uribe JS, et al. Defining the safe working zones using the lumbar plexus for lateral transpsoas approaches. J Neurosurg Spine. 2011.
- Benglis DM, Vanni S, Levi AD. An anatomical study of the lumbosacral plexus as related to the lateral transpsoas approach. J Neurosurg Spine. 2009.
- AO Foundation. Lateral lumbar interbody fusion. AO Spine / Surgery Reference. link