
Case Prep: Intramedullary Spinal Cord Tumor Resection (Ependymoma / Astrocytoma / Hemangioblastoma)
Case / Approach Snapshot
- Anatomy at risk: cord, roots, dura, epidural venous plexus, tumor vascular supply, vertebral body/posterior element involvement, and stabilization corridors.
- Operative steps: define oncologic and neurologic goals, localize levels, decompress neural elements, obtain tissue or resect/debulk safely, reconstruct stability, and coordinate radiation/systemic therapy planning; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: major blood loss, neuromonitoring change, durotomy/CSF leak, pathologic instability, wound breakdown after radiation, residual disease strategy, and staged embolization or reconstruction.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [cervical/thoracic] intramedullary spinal cord tumor ([ependymoma / astrocytoma / hemangioblastoma]) at [levels] presenting with [pain / sensory changes / weakness] planned for laminectomy/laminoplasty and midline myelotomy for microsurgical resection.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior thoracolumbar approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Intraoperative neurophysiology in intramedullary spinal cord tumor surgery — Sala F. Handbook of clinical neurology 2022. PubMed
- The role of intraoperative neurophysiological monitoring in intramedullary spinal cord tumor surgery — Liu K. Chinese neurosurgical journal 2023. PubMed
- Neuromonitoring for Intramedullary Spinal Cord Tumor Surgery — Verla T. World neurosurgery 2016. PubMed
- The evolution of intramedullary spinal cord tumor surgery — Sciubba DM. Neurosurgery 2009. PubMed
- Automatic multiclass intramedullary spinal cord tumor segmentation on MRI with deep learning — Lemay A. NeuroImage. Clinical 2021. PubMed
- Intramedullary Thoracic Spinal Cord Abscess Mimicking an Intramedullary Tumor: A Case Report — Ul Haq N. Cureus 2023. PubMed
- Metastatic Upper Thoracic Intramedullary Spinal Cord Tumor of Ovarian Adenocarcinoma: A Rare Case Report and Literature Review — Heidari V. Cancer reports (Hoboken, N.J.) 2024. PubMed
- Intraoperative Neuromonitoring in Patients with Intramedullary Spinal Cord Tumor: A Systematic Review, Meta-Analysis, and Case Series — Rijs K. World neurosurgery 2019. PubMed
- Spinal Cord Deformities Associated with Intramedullary Spinal Cord Tumors — Hamrick F. Neurosurgery clinics of North America 2026. PubMed
- Spinal Cord Ependymomas — Borges LF. Neurosurgery clinics of North America 2026. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
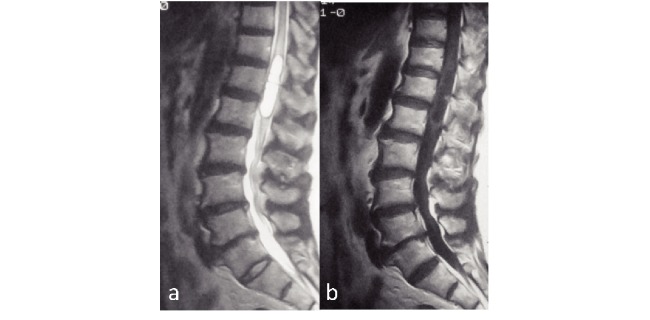 Fig. 1. (a) T2 MRI and (b) Gd-enhanced MRI before the initial surgery (nine years ago), showing the presence of an intramedullary tumor. Source: Tuberculous meningitis with dementia as the presenting symptom after intramedullary spinal cord tumor resection — Nagoya Journal of Medical Science 2015; CC BY-NC-ND.
Fig. 1. (a) T2 MRI and (b) Gd-enhanced MRI before the initial surgery (nine years ago), showing the presence of an intramedullary tumor. Source: Tuberculous meningitis with dementia as the presenting symptom after intramedullary spinal cord tumor resection — Nagoya Journal of Medical Science 2015; CC BY-NC-ND.
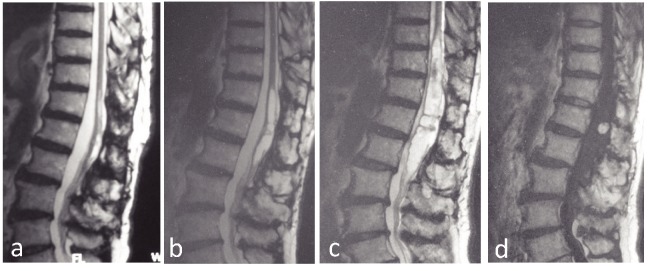 Fig. 2. (a) T2 MRI after the first surgery, showing total resection of the tumor. (b) T2 MRI four years after the first surgery, showing regrowth of the tumor. (c) T2 MRI and (d) Gd enhanced MRI… Source: Tuberculous meningitis with dementia as the presenting symptom after intramedullary spinal cord tumor resection — Nagoya Journal of Medical Science 2015; CC BY-NC-ND.
Fig. 2. (a) T2 MRI after the first surgery, showing total resection of the tumor. (b) T2 MRI four years after the first surgery, showing regrowth of the tumor. (c) T2 MRI and (d) Gd enhanced MRI… Source: Tuberculous meningitis with dementia as the presenting symptom after intramedullary spinal cord tumor resection — Nagoya Journal of Medical Science 2015; CC BY-NC-ND.
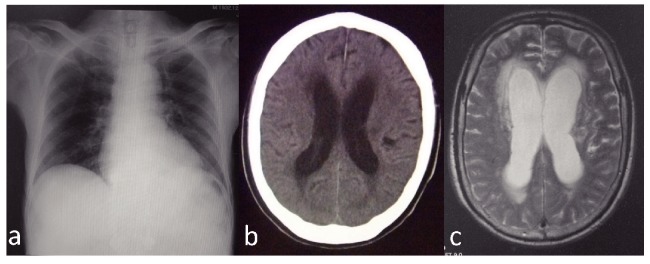 Fig. 3. (a) Normal chest X-ray. (b) Brain CT showing slight ventricle enlargement. (c) Brain MRI showing ventricle enlargement. Source: Tuberculous meningitis with dementia as the presenting symptom after intramedullary spinal cord tumor resection — Nagoya Journal of Medical Science 2015; CC BY-NC-ND.
Fig. 3. (a) Normal chest X-ray. (b) Brain CT showing slight ventricle enlargement. (c) Brain MRI showing ventricle enlargement. Source: Tuberculous meningitis with dementia as the presenting symptom after intramedullary spinal cord tumor resection — Nagoya Journal of Medical Science 2015; CC BY-NC-ND.
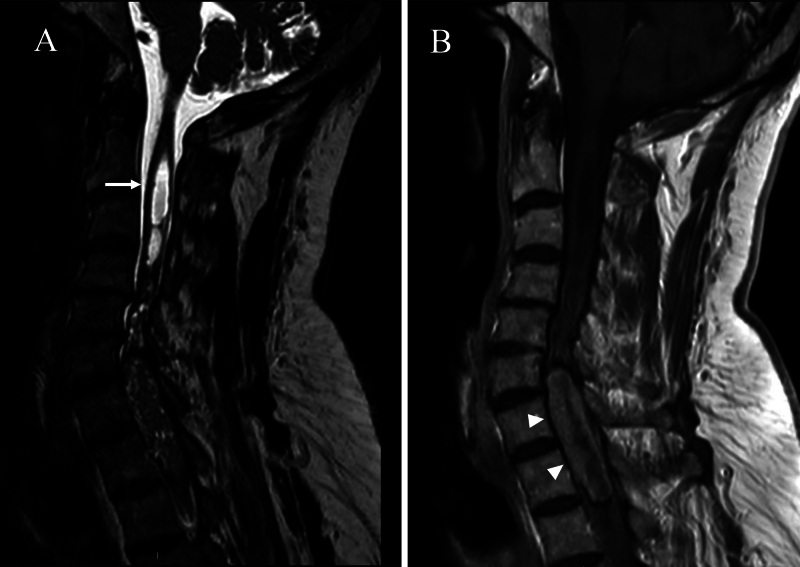 FIG. 1.. Preoperative cervical spine MR images demonstrating an intramedullary mass extending from C6 to T2. A: T2-weighted image showing an associated syringomyelia with cranial extension of the… Source: Anterior intradural CSF collection causing postoperative neurological deterioration after intramedullary tumor resection and associated syringomyelia: illustrative case — Journal of Neurosurgery: Case Lessons 2026; CC BY-NC-ND.
FIG. 1.. Preoperative cervical spine MR images demonstrating an intramedullary mass extending from C6 to T2. A: T2-weighted image showing an associated syringomyelia with cranial extension of the… Source: Anterior intradural CSF collection causing postoperative neurological deterioration after intramedullary tumor resection and associated syringomyelia: illustrative case — Journal of Neurosurgery: Case Lessons 2026; CC BY-NC-ND.
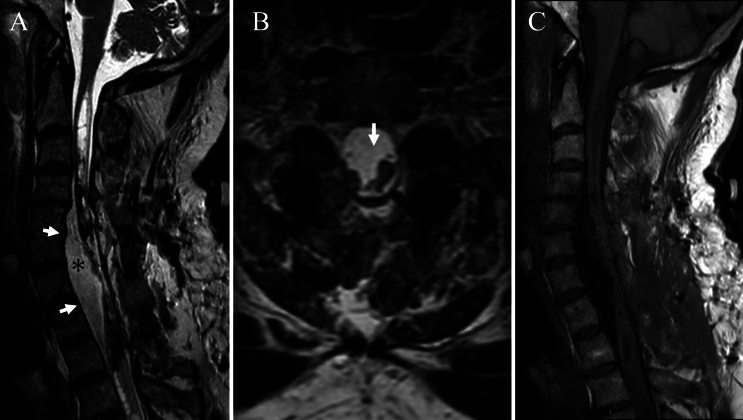 FIG. 2.. Cervical spine MR images demonstrating an anterior intradural fluid collection resulting in dorsal displacement of the spinal cord (arrow). A and B: T2-weighted images showing a… Source: Anterior intradural CSF collection causing postoperative neurological deterioration after intramedullary tumor resection and associated syringomyelia: illustrative case — Journal of Neurosurgery: Case Lessons 2026; CC BY-NC-ND.
FIG. 2.. Cervical spine MR images demonstrating an anterior intradural fluid collection resulting in dorsal displacement of the spinal cord (arrow). A and B: T2-weighted images showing a… Source: Anterior intradural CSF collection causing postoperative neurological deterioration after intramedullary tumor resection and associated syringomyelia: illustrative case — Journal of Neurosurgery: Case Lessons 2026; CC BY-NC-ND.
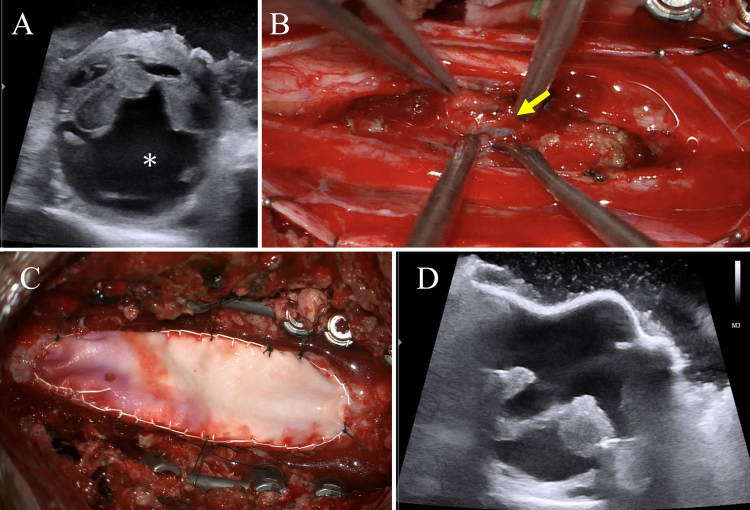 FIG. 3.. Intraoperative findings and ultrasound images. A: Intraoperative ultrasound demonstrating a prominent anterior CSF space compressing the spinal cord posteriorly, consistent with a… Source: Anterior intradural CSF collection causing postoperative neurological deterioration after intramedullary tumor resection and associated syringomyelia: illustrative case — Journal of Neurosurgery: Case Lessons 2026; CC BY-NC-ND.
FIG. 3.. Intraoperative findings and ultrasound images. A: Intraoperative ultrasound demonstrating a prominent anterior CSF space compressing the spinal cord posteriorly, consistent with a… Source: Anterior intradural CSF collection causing postoperative neurological deterioration after intramedullary tumor resection and associated syringomyelia: illustrative case — Journal of Neurosurgery: Case Lessons 2026; CC BY-NC-ND.
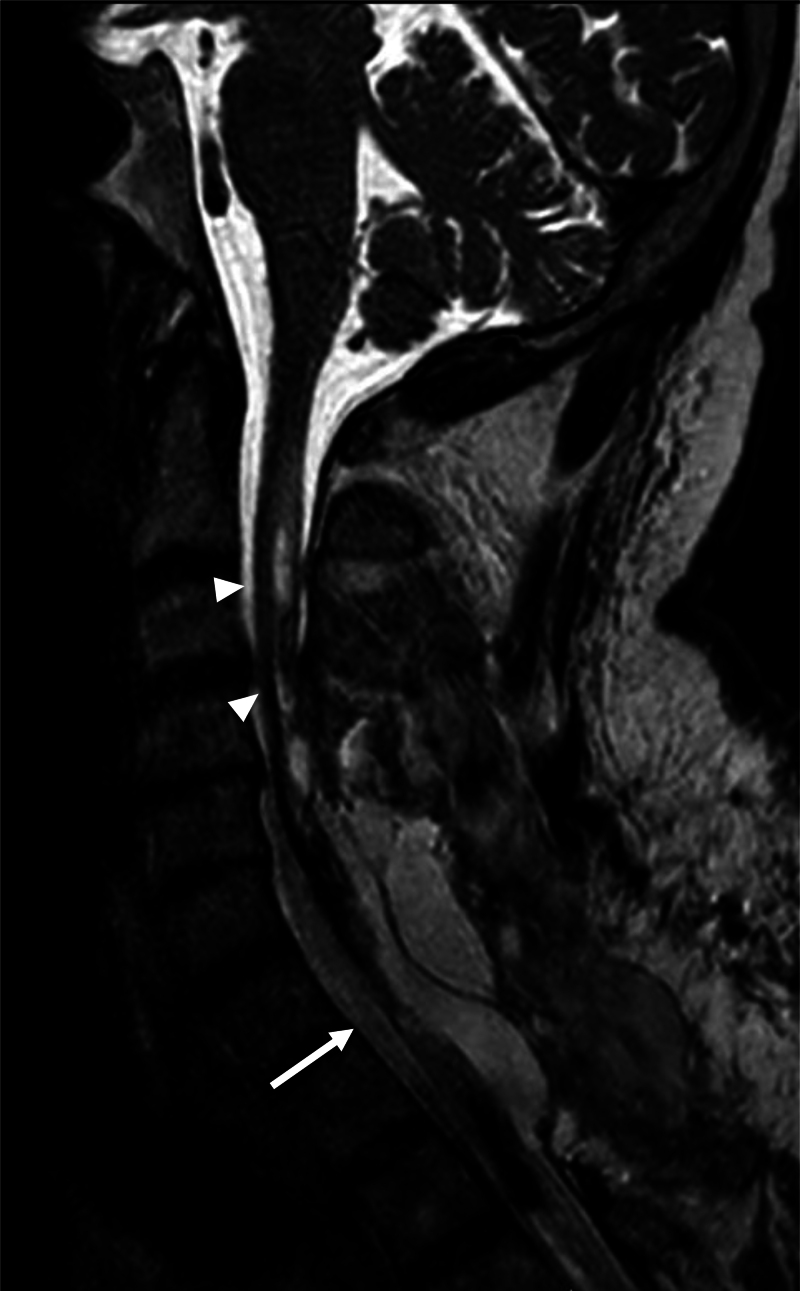 FIG. 4.. Postoperative cervical spine MR image demonstrating restoration of the spinal cord to its normal position (arrow) with a marked reduction in the associated syrinx (arrowheads) compared… Source: Anterior intradural CSF collection causing postoperative neurological deterioration after intramedullary tumor resection and associated syringomyelia: illustrative case — Journal of Neurosurgery: Case Lessons 2026; CC BY-NC-ND.
FIG. 4.. Postoperative cervical spine MR image demonstrating restoration of the spinal cord to its normal position (arrow) with a marked reduction in the associated syrinx (arrowheads) compared… Source: Anterior intradural CSF collection causing postoperative neurological deterioration after intramedullary tumor resection and associated syringomyelia: illustrative case — Journal of Neurosurgery: Case Lessons 2026; CC BY-NC-ND.
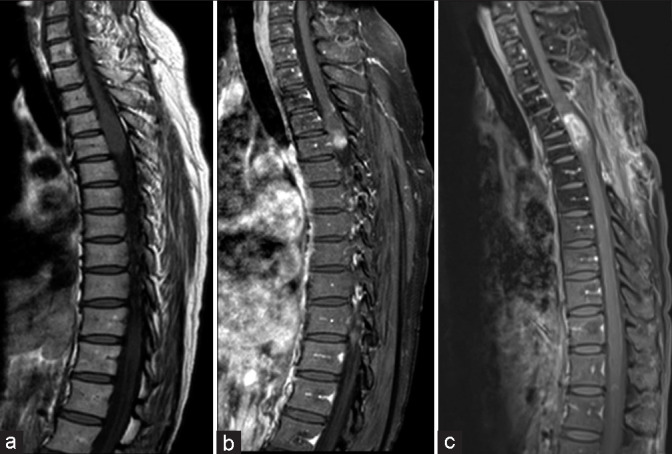 Figure 1:. (a and b) Preoperative images – T1 pre- and postcontrast of thoracic spine and (c) one year postoperative – T1 postcontrast of thoracic spine. Source: Primary thoracic intramedullary spinal cord tumor with likely metastases of glial origin to the lumbosacral vertebrae: Illustrative case — Surgical Neurology International 2023; CC BY-NC-SA.
Figure 1:. (a and b) Preoperative images – T1 pre- and postcontrast of thoracic spine and (c) one year postoperative – T1 postcontrast of thoracic spine. Source: Primary thoracic intramedullary spinal cord tumor with likely metastases of glial origin to the lumbosacral vertebrae: Illustrative case — Surgical Neurology International 2023; CC BY-NC-SA.
 Figure 2:. (a) 18 months postoperatively – T2 noncontrast of thoracic spine, (b) 20 months postoperatively – T1 with contrast of thoracic spine, and 3 years postoperatively showing progression (c)… Source: Primary thoracic intramedullary spinal cord tumor with likely metastases of glial origin to the lumbosacral vertebrae: Illustrative case — Surgical Neurology International 2023; CC BY-NC-SA.
Figure 2:. (a) 18 months postoperatively – T2 noncontrast of thoracic spine, (b) 20 months postoperatively – T1 with contrast of thoracic spine, and 3 years postoperatively showing progression (c)… Source: Primary thoracic intramedullary spinal cord tumor with likely metastases of glial origin to the lumbosacral vertebrae: Illustrative case — Surgical Neurology International 2023; CC BY-NC-SA.
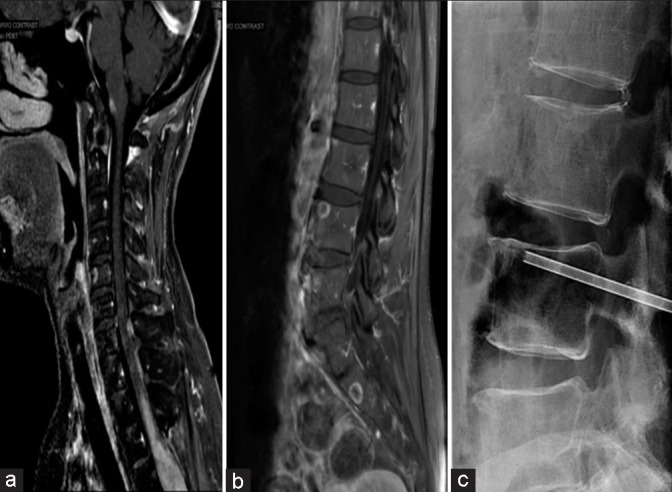 Figure 3:. (a) Three years postoperatively – T1 with the contrast of cervical spine, (b) 3 years postoperatively – T1 with the contrast of lumbar spine, and (c) X-ray-guided biopsy of L4 vertebral… Source: Primary thoracic intramedullary spinal cord tumor with likely metastases of glial origin to the lumbosacral vertebrae: Illustrative case — Surgical Neurology International 2023; CC BY-NC-SA.
Figure 3:. (a) Three years postoperatively – T1 with the contrast of cervical spine, (b) 3 years postoperatively – T1 with the contrast of lumbar spine, and (c) X-ray-guided biopsy of L4 vertebral… Source: Primary thoracic intramedullary spinal cord tumor with likely metastases of glial origin to the lumbosacral vertebrae: Illustrative case — Surgical Neurology International 2023; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Central cord-type symptoms — dysesthetic pain, sensory changes, progressive weakness, gait
- Duration (slow), bowel/bladder, dissociated sensory loss
- Tumor clues: ependymoma (central, well-circumscribed, plane, adults — most resectable), astrocytoma (infiltrative, eccentric, children, less resectable), hemangioblastoma (VHL, pial-based, vascular, syrinx)
Imaging Review
MRI (T1±Gad, T2) entire cord
- Intramedullary (cord expansion), enhancement pattern, extent (levels), syrinx/cyst (rostral/caudal), hemorrhage
- Ependymoma (central, symmetric, cleavage plane, cap sign); astrocytoma (eccentric, infiltrative, indistinct); hemangioblastoma (intense enhancing nodule, flow voids, pial, VHL)
- VHL screening (hemangioblastoma)
Angiography
- Consider for vascular hemangioblastoma (feeders, embolization)
Labs
- CBC, BMP, Coags, Type and screen; VHL workup if hemangioblastoma
Neurological Examination
- Detailed motor/sensory (dorsal columns, spinothalamic), reflexes, gait, bowel/bladder — meticulous baseline (resection risks dorsal column/motor decline)
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- OR setup: microscope, fluoroscopy/navigation, neuromonitoring, tumor debulking/microsurgical set, dural repair materials, instrumentation/corpectomy trays as indicated, and blood available.
- Special needs: arterial line/Foley for long cases, dexamethasone for cord edema when indicated, MAP support for myelopathy/cord manipulation, oncology/radiation plan, and pathology/frozen specimen workflow.
- Immediate postop orders: frequent motor/sensory exams, MAP support if cord manipulation or deficit, MRI/CT/X-rays per tumor/construct, steroid taper, drain/dural-leak precautions, brace/activity, DVT timing, and oncology/radiation follow-up.
Diagnosis & Indication
- Indication: Symptomatic/progressive intramedullary tumor; goal is maximal safe resection (ependymoma/hemangioblastoma often resectable with plane; astrocytoma → debulk/biopsy, infiltrative)
- IONM-guided — resection limited by MEP/D-wave changes
Position
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- Prone, Mayfield (cervical) or pinned; neutral; reverse Trendelenburg; IONM baseline (MEP, SSEP, D-wave)
Key Surgical Steps
- Level localization (fluoroscopy), laminectomy or laminoplasty over tumor + 1 level above/below
- Ultrasound — confirm tumor extent, syrinx, choose myelotomy length
- Midline durotomy, tack-up, preserve arachnoid then open
- Inspect cord — identify midline (dorsal median sulcus/raphe between dorsal columns), often widened cord, may see discoloration/vessels
- Midline myelotomy through the dorsal median sulcus (minimizes dorsal column injury) over tumor length; pial sutures gently retract
- Tumor resection:
- Ependymoma: identify cleavage plane, internally debulk (CUSA), circumferentially dissect from cord, coagulate ventral feeders, deliver en bloc/piecemeal — aim gross total
- Astrocytoma: internally debulk, no clear plane — partial resection/debulk, avoid aggressive pursuit (motor loss)
- Hemangioblastoma: do NOT enter nodule (vascular); circumferential pial dissection, coagulate feeders, remove nodule en bloc; drain associated syrinx
- Continuous IONM — stop/pause if MEP/D-wave drop
- Hemostasis (gentle — bipolar near cord), do NOT pack cavity tightly
- Watertight dural closure, sealant, ± laminoplasty reconstruction
- Closure
Critical Anatomy & Structures at Risk
- Spinal cord parenchyma — dorsal columns (myelotomy → proprioceptive/sensory loss), corticospinal tracts (motor)
- Anterior spinal artery / sulcal arteries (ventral) — cord infarction
- Pial vessels, syrinx
- Dura (CSF leak)
Equipment
- Microscope, ultrasound, CUSA (low settings), fine microinstruments/bipolar, pial sutures
- Dural substitute, sealant, laminoplasty hardware, ICG (hemangioblastoma)
Monitoring
- MEPs, SSEPs, D-wave (essential), EMG — D-wave preservation predicts motor recovery even if transient MEP loss
Anesthesia
- MAP > 85-90 (cord perfusion), no paralytic, arterial line, total IV anesthesia (IONM-friendly), prone precautions
Potential Complications
- Neurological decline — dorsal column (sensory/proprioception, common transient), motor (worse with astrocytoma/aggressive resection)
- CSF leak/pseudomeningocele
- Cord infarction (anterior spinal artery), hemorrhage
- Spinal deformity (post-laminectomy, esp. children — laminoplasty mitigates), recurrence
Operative Note Template
Preoperative Diagnosis: [Cervical/thoracic] intramedullary spinal cord tumor ([ependymoma/astrocytoma/hemangioblastoma]) at [levels]
Postoperative Diagnosis: Same (pending pathology)
Procedure: [Levels] laminectomy/laminoplasty with midline myelotomy and microsurgical resection of intramedullary tumor
Surgeon / Assistant: Anesthesia: Total IV anesthesia (IONM-friendly), no paralytic EBL / Fluids: Adjuncts: Microscope, ultrasound, CUSA (low), ICG (hemangioblastoma), pial sutures; MEP/SSEP/D-wave; MAP > 85–90 Implants: Dural substitute, sealant; [laminoplasty hardware] Complications: None
Indications: [Age]yo [M/F] with an intramedullary spinal cord tumor at [levels] causing [progressive myelopathy/sensory change]. Maximal safe resection under IONM guidance was planned. Risks (dorsal-column/motor deficit, CSF leak) discussed.
Description of Procedure: After consent and time-out, total IV anesthesia was induced (MAP > 85–90, no paralytic) and MEP/SSEP/D-wave monitoring established. The patient was positioned prone; a laminectomy/laminoplasty was performed over the tumor plus a level above/below, and ultrasound defined the extent. A midline durotomy was made and the cord exposed.
A midline myelotomy through the dorsal median sulcus was performed and the tumor addressed [ependymoma: cleavage plane developed, internally debulked, dissected circumferentially and removed for gross-total; astrocytoma: internally debulked without an aggressive pursuit of indistinct margins; hemangioblastoma: pial dissection with feeder coagulation and en-bloc nodule removal without entering it]. The anterior spinal artery and pial vessels were preserved; resection was paused/limited per MEP/D-wave changes. A watertight dural closure was performed with sealant [and laminoplasty reconstruction].
Closure was completed in layers. The patient was transferred with MAP support and CSF-leak precautions; transient dorsal-column dysfunction was anticipated.
Postoperative Plan
- ICU, neuro checks q1h (motor/sensory/proprioception), MAP support
- Flat/CSF leak precautions, MRI postop (resection)
- Expect possible transient dorsal column dysfunction; PT/OT/rehab early
- DVT prophylaxis (mechanical), pain (dysesthetic — gabapentinoids)
- Pathology/grade; VHL workup (hemangioblastoma); adjuvant therapy per pathology; surveillance MRI; deformity surveillance
Chief-Level Case Review
Use these as the senior-level mental model for Intramedullary Spinal Cord Tumor Resection (Ependymoma / Astrocytoma / Hemangioblastoma):
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Intramedullary Spinal Cord Tumor Resection (Ependymoma / Astrocytoma / Hemangioblastoma):
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]