
Case Prep: Lumbar Microdiscectomy
Case / Approach Snapshot
- Anatomy at risk: level localization, cord/cauda equina, exiting and traversing roots, dura, vertebral artery or segmental vessels, esophagus/trachea/pleura/viscera by approach, and fusion/instrumentation landmarks.
- Operative steps: position and pad carefully, confirm level, expose the planned corridor, decompress neural elements, reconstruct or instrument when indicated, verify alignment/hardware, and close with attention to hematoma and wound risk; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: wrong level, durotomy, neurologic change, vertebral artery/visceral/pleural injury, graft or hardware problem, epidural hematoma, dysphagia/airway issue, and infection prevention/escalation.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [left/right] [L_-S_] disc herniation causing [L_/S_] radiculopathy presenting with [leg pain/weakness/numbness] [and/or cauda equina syndrome] planned for [left/right] L_-S_ microdiscectomy.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
CNS Video Library
🧭 Operative approach: Posterior thoracolumbar approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Lumbar Microdiscectomy — Truumees E. JBJS essential surgical techniques 2016. PubMed
- Lumbar microdiscectomy and microendoscopic discectomy — Riesenburger RI. Minimally invasive therapy & allied technologies : MITAT : official journal of the Society for Minimally Invasive Therapy 2006. PubMed
- Lumbar microdiscectomy complication rates: a systematic review and meta-analysis — Shriver MF. Neurosurgical focus 2015. PubMed
- Importance of Physiotherapy after Lumbar Microdiscectomy — Cerezci O. Turkish neurosurgery 2023. PubMed
- Lumbar microdiscectomy: a historical perspective and current technical considerations — Koebbe CJ. Neurosurgical focus 2002. PubMed
- [Lumbar microdiscectomy using intraoperative ultrasound] — Aslanukov MN. Khirurgiia 2020. PubMed
- Predictors of Recovery Following Lumbar Microdiscectomy for Sciatica: A Systematic Review and Meta-Analysis of Observational Studies — Rehman Y. Cureus 2023. PubMed
- [Single-segment lumbar microdiscectomy:drainage or not] — Zhang ZC. Zhongguo gu shang = China journal of orthopaedics and traumatology 2021. PubMed
- Stereotactic lumbar microdiscectomy — Koutrouvelis PG. Neurosurgery clinics of North America 1996. PubMed
- Complications of Full-Endoscopic Lumbar Discectomy versus Open Lumbar Microdiscectomy: A Systematic Review and Meta-Analysis — Yang CC. World neurosurgery 2022. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
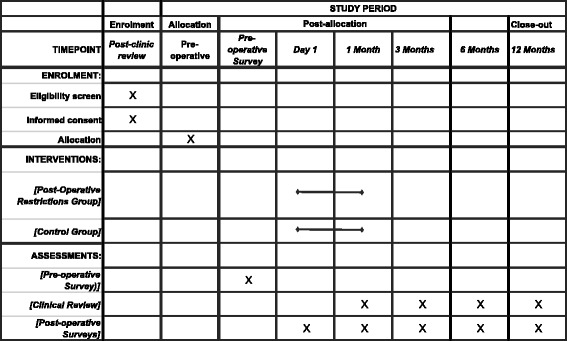 Figure 3. Source: Lumbar microdiscectomy and post-operative activity restrictions: a protocol for a single blinded randomised controlled trial — BMC Musculoskelet Disord. 2017 Jul 20;18:312. doi: 10.1186/s12891-017-1681-3; CC BY.
Figure 3. Source: Lumbar microdiscectomy and post-operative activity restrictions: a protocol for a single blinded randomised controlled trial — BMC Musculoskelet Disord. 2017 Jul 20;18:312. doi: 10.1186/s12891-017-1681-3; CC BY.
 Figure 4. Source: Variability in Opioid Prescription Following Primary Single-Level Lumbar Microdiscectomy — Global Spine J. 2020 Aug 28;12(2):263–6. doi: 10.1177/2192568220950678; CC BY-NC-ND.
Figure 4. Source: Variability in Opioid Prescription Following Primary Single-Level Lumbar Microdiscectomy — Global Spine J. 2020 Aug 28;12(2):263–6. doi: 10.1177/2192568220950678; CC BY-NC-ND.
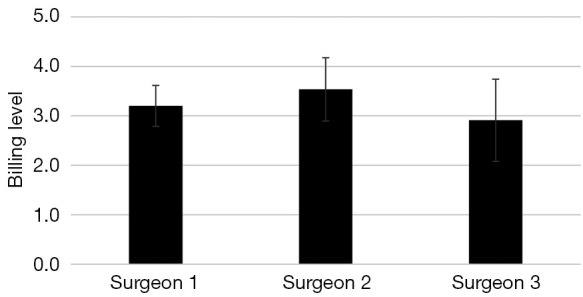 Figure 1. Average billing level and standard deviation for each surgeon for lumbar microdiscectomy from 2018–2019. Source: Differences in evaluation and management coding of outpatient clinic visits for patients undergoing elective spine surgery with use of a standardized template — Journal of Spine Surgery 2023; CC BY-NC-ND.
Figure 1. Average billing level and standard deviation for each surgeon for lumbar microdiscectomy from 2018–2019. Source: Differences in evaluation and management coding of outpatient clinic visits for patients undergoing elective spine surgery with use of a standardized template — Journal of Spine Surgery 2023; CC BY-NC-ND.
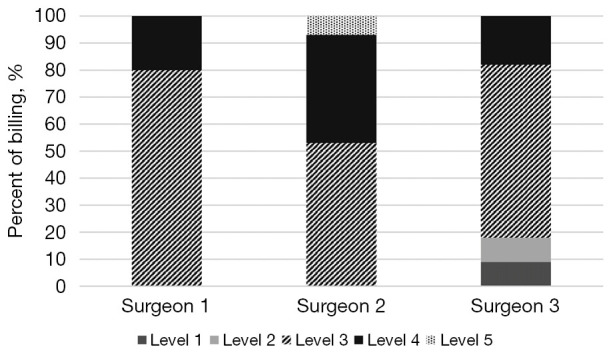 Figure 2. Distribution of billing by each surgeon per level for lumbar microdiscectomy from 2018–2019. Source: Differences in evaluation and management coding of outpatient clinic visits for patients undergoing elective spine surgery with use of a standardized template — Journal of Spine Surgery 2023; CC BY-NC-ND.
Figure 2. Distribution of billing by each surgeon per level for lumbar microdiscectomy from 2018–2019. Source: Differences in evaluation and management coding of outpatient clinic visits for patients undergoing elective spine surgery with use of a standardized template — Journal of Spine Surgery 2023; CC BY-NC-ND.
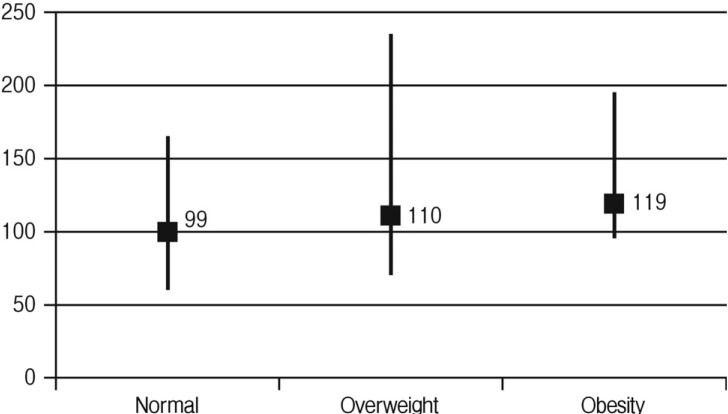 Fig. 1. Average operation time stratified by body mass index. Source: Does Obesity Make an Influence on Surgical Outcomes Following Lumbar Microdiscectomy? — Korean Journal of Spine 2014; CC BY-NC.
Fig. 1. Average operation time stratified by body mass index. Source: Does Obesity Make an Influence on Surgical Outcomes Following Lumbar Microdiscectomy? — Korean Journal of Spine 2014; CC BY-NC.
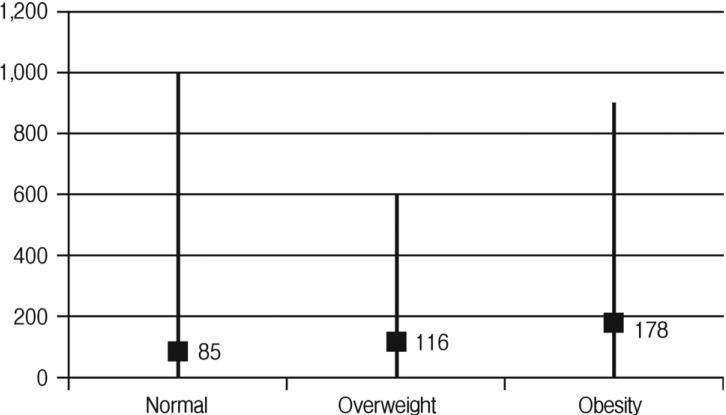 Fig. 2. Averatge estimated blood loss stratified by body mass index. Source: Does Obesity Make an Influence on Surgical Outcomes Following Lumbar Microdiscectomy? — Korean Journal of Spine 2014; CC BY-NC.
Fig. 2. Averatge estimated blood loss stratified by body mass index. Source: Does Obesity Make an Influence on Surgical Outcomes Following Lumbar Microdiscectomy? — Korean Journal of Spine 2014; CC BY-NC.
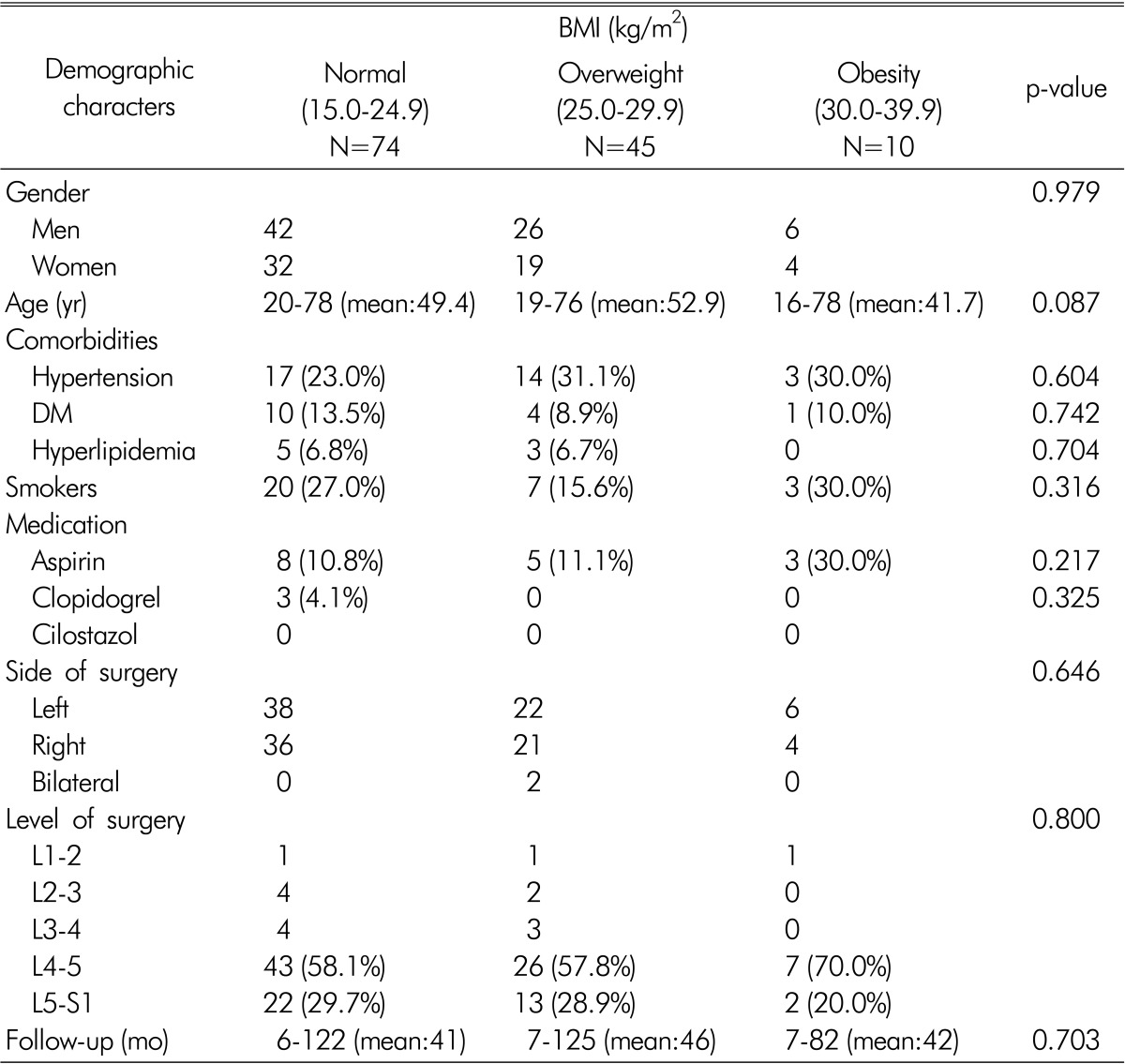 Figure 9. Source: Does Obesity Make an Influence on Surgical Outcomes Following Lumbar Microdiscectomy? — Korean J Spine. 2014 Jun 30;11(2):68–73. doi: 10.14245/kjs.2014.11.2.68; CC BY-NC.
Figure 9. Source: Does Obesity Make an Influence on Surgical Outcomes Following Lumbar Microdiscectomy? — Korean J Spine. 2014 Jun 30;11(2):68–73. doi: 10.14245/kjs.2014.11.2.68; CC BY-NC.
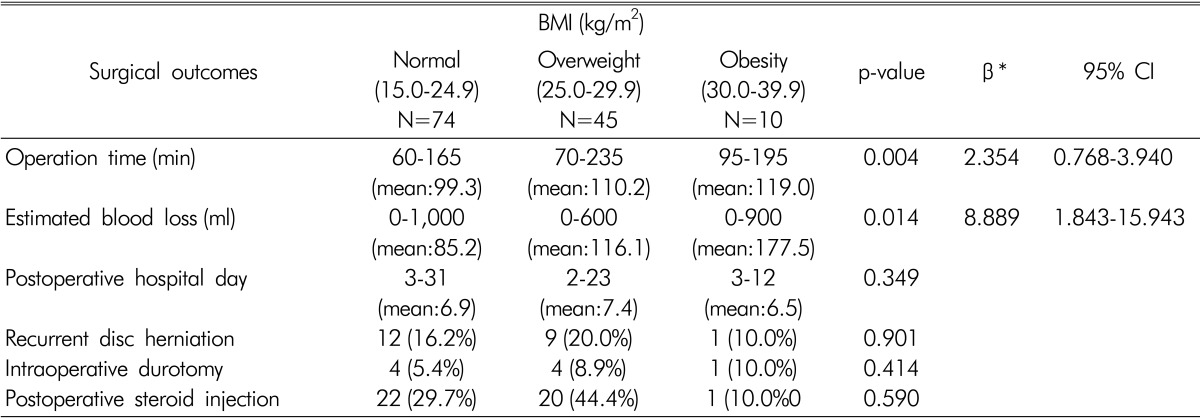 Figure 10. Source: Does Obesity Make an Influence on Surgical Outcomes Following Lumbar Microdiscectomy? — Korean J Spine. 2014 Jun 30;11(2):68–73. doi: 10.14245/kjs.2014.11.2.68; CC BY-NC.
Figure 10. Source: Does Obesity Make an Influence on Surgical Outcomes Following Lumbar Microdiscectomy? — Korean J Spine. 2014 Jun 30;11(2):68–73. doi: 10.14245/kjs.2014.11.2.68; CC BY-NC.
History of Present Illness
- Chief complaint: Radicular leg pain (sciatica) / weakness / numbness
- Duration:
- Distribution: Dermatomal pattern
- L4: Anterior thigh, medial leg
- L5: Lateral leg, dorsum of foot, great toe
- S1: Posterior leg, lateral foot, sole
- Severity (VAS pain score):
- Worse with: Sitting, bending, Valsalva
- Better with: Standing, lying down
- Motor deficit: Foot drop (L5), plantarflexion weakness (S1)
- Failed conservative management: Duration ___, modalities tried (PT, NSAIDs, oral steroids, epidural injections)
- Red flags (cauda equina syndrome):
- Saddle anesthesia
- Bowel/bladder dysfunction (retention > incontinence)
- Bilateral leg symptoms
- Progressive motor deficit
- If CES → EMERGENT SURGERY
Past Medical History
- Prior lumbar surgery (same or adjacent level)
- Diabetes (neuropathy may confound exam)
- Peripheral vascular disease
- Obesity (BMI)
- Smoking
- Workers’ compensation / litigation (may affect outcomes)
- Allergies:
- Medications:
Imaging Review
MRI Lumbar Spine
- Herniation level: L_-S_ (most common: L4-5 and L5-S1)
- Herniation type: Protrusion / extrusion / sequestration
- Herniation location: Central / paracentral / foraminal / far lateral (extra-foraminal)
- Paracentral (most common): Compresses traversing nerve root (e.g., L4-5 paracentral → L5 root)
- Foraminal/far lateral: Compresses exiting nerve root (e.g., L4-5 far lateral → L4 root)
- Fragment migration: Superior / inferior / lateral
- Canal stenosis: Central canal size
- Nerve root compression: Degree of root impingement
- Cord signal (if conus level):
- Other levels: Assess for additional pathology
- Modic changes: Endplate changes at involved level
CT Lumbar Spine (if MRI contraindicated)
- Bony anatomy
- Disc calcification
- Facet arthropathy
X-rays Lumbar Spine (AP, Lateral, Flexion/Extension)
- Alignment
- Spondylolisthesis (if listhesis present, may need fusion instead)
- Disc height
- Dynamic instability
Labs
- CBC
- BMP
- Coagulation
- Type and screen (rarely needed)
- HbA1c (if diabetic)
- UA (if CES symptoms)
- Post-void residual (if bladder symptoms)
Neurological Examination
Motor (Myotomal)
- L2: Hip flexion (iliopsoas) ___/5
- L3: Knee extension (quadriceps) ___/5
- L4: Ankle dorsiflexion (tibialis anterior) ___/5
- L5: Great toe extension (EHL) __/5, hip abduction __/5
- S1: Ankle plantarflexion (gastroc/soleus) ___/5, toe walking
Sensory (Dermatomal)
- L4: Medial leg
- L5: Lateral leg, dorsum of foot, first webspace
- S1: Lateral foot, sole, posterior calf
- Perianal sensation (CES screening):
Reflexes
- Patellar (L3-4):
- Achilles (S1):
- Babinski:
Provocative Tests
- Straight leg raise (SLR): Positive at ___ degrees (ipsilateral)
- Contralateral SLR: Positive (highly specific for disc herniation)
- Femoral nerve stretch test (L2-4 levels):
CES Screening
- Perianal sensation:
- Rectal tone:
- Post-void residual:
- Bladder/bowel function:
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: Wilson frame, Andrews/knee-chest frame, or Jackson/open-frame table by surgeon preference; flexion opens the interlaminar window and the abdomen must hang free.
- OR setup: radiolucent/Jackson table, fluoroscopy or O-arm/navigation, microscope/loupes for decompression, implant trays/graft ready for fusion, neuromonitoring for myelopathy/cord-risk cases, and postop brace plan confirmed.
- Special needs: arterial line/Foley/type-screen for long fusion/corpectomy, no long paralytic when MEPs are used, MAP/normotension for myelopathy or cord-risk cases, antibiotic redosing, and anticoagulation/DVT plan.
- Immediate postop orders: neuro checks by myotome/sensory level, airway/dysphagia watch for anterior cervical cases, CT/X-rays per construct, drain care, brace/activity orders, DVT prophylaxis timing, bowel regimen, and PT/OT mobilization.
Diagnosis & Indication
- Working diagnosis: [L_-S_] disc herniation with [L_/S_] radiculopathy
- Surgical indication: Failed conservative management (> 6 weeks) with concordant imaging and symptoms; OR progressive motor deficit; OR cauda equina syndrome (emergent)
- Goals: Decompress nerve root by removing herniated disc fragment
- NOT a fusion procedure — motion preserved
Position
- OR table/bed: Wilson frame, Andrews/knee-chest frame, or Jackson/open-frame table by surgeon preference; flexion opens the interlaminar window and the abdomen must hang free.
- Patient position: Prone on a Wilson frame (or Jackson table, or Andrews frame)
- Abdomen: Must be FREE/hanging — reduces epidural venous engorgement and bleeding
- Wilson frame: curved to open lumbar interspaces
- Jackson table: padded frame, abdomen free
- Head: On horseshoe headrest or foam, eyes free, ETT secured
- Arms: On armboards, elbows padded, < 90 degrees abduction
- Legs: Slightly flexed at hips and knees
- Chest bolsters/pads: Support chest, keep abdomen free
- Key: Check that abdomen is truly free — palpate or slide hand under
Incision
- Type: Small (2-3 cm) midline posterior incision centered over the interspace
- Level confirmed with: Fluoroscopy (AP view, spinal needle placed on spinous process or interspinous ligament)
- Skin marking: Navigation or fluoroscopy mark the disc level
Approach: Posterior Midline Microsurgical
Key Surgical Steps
- Fluoroscopic level confirmation — CRITICAL; wrong-level surgery is a never event
- Place needle on spinous process, obtain AP fluoroscopy
- Count from sacrum (most reliable landmark)
- For L5-S1: palpate sacral promontory/lumbosacral junction
- Midline incision — 2-3 cm centered over interlaminar window
- Subperiosteal dissection — detach paraspinal muscles from spinous process and lamina on the AFFECTED SIDE ONLY
- Self-retaining retractor (McCulloch, tubular retractor for MIS)
- Identify interlaminar window:
- Superior lamina (partial inferior edge)
- Inferior lamina (partial superior edge)
- Ligamentum flavum between
- Laminotomy: Remove inferior edge of superior lamina with Kerrison rongeur or drill to expose the ligamentum flavum adequately
- Preserve as much facet joint as possible (> 50% lateral facet must remain to prevent instability)
- Ligamentum flavum removal: Detach from deep surface of superior lamina, elevate, and excise with Kerrison rongeur, exposing the epidural space
- Identify the traversing nerve root — should be visible crossing the disc space
- Retract nerve root medially (gently, with nerve root retractor)
- Identify disc herniation:
- Epidural: Fragment may be visible under the root
- Subligamentous: Open the posterior longitudinal ligament over the bulge
- Sequestered: Fragment may have migrated superiorly or inferiorly
- Remove disc fragment:
- Incise annulus (if subligamentous)
- Remove herniated fragment with pituitary rongeur
- Enter the disc space and remove loose fragments
- Explore for free fragments — check cephalad and caudad to the nerve root, and laterally in the axilla of the root
- Do NOT aggressively curette the disc space (not a fusion — preserve disc height)
- Confirm root decompression:
- Nerve root should be freely mobile
- Pass nerve hook around the root (360-degree check)
- Root should be pulsatile (thecal sac pulsation transmitted)
- Hemostasis: Bipolar, Gelfoam, thrombin-soaked Gelfoam for epidural bleeding
- Closure:
- Irrigate
- Fascia: 0 or 2-0 Vicryl
- Subcutaneous: 3-0 Vicryl
- Skin: 4-0 Monocryl subcuticular + Dermabond OR staples
Critical Anatomy & Structures at Risk
- Traversing nerve root — the root being decompressed; retract gently (medially)
- Exiting nerve root — exits under the pedicle ABOVE (e.g., L4 root exits at L4-5 above the disc); at risk if dissection is too lateral/cephalad
- Thecal sac / cauda equina — medial to the working corridor
- Epidural veins — can cause significant bleeding; bipolar, Gelfoam
- Facet joint — preserve > 50% to prevent iatrogenic instability
- Great vessels (aorta/IVC/iliac) — anterior to disc space; rare but CATASTROPHIC vascular injury if pituitary rongeur passes through anterior annulus. Do NOT plunge instruments anteriorly
Equipment
- Operating microscope OR loupes + headlight
- C-arm fluoroscopy (for level confirmation)
- McCulloch retractor set (or tubular retractor for MIS)
- Kerrison rongeurs (2mm, 3mm, 4mm)
- Pituitary rongeurs (various angles)
- Curettes (angled, straight)
- Nerve root retractors (small, medium)
- Nerve hook
- Penfield dissectors
- High-speed drill (if bony decompression needed)
- Bipolar forceps
- Hemostatic agents (Gelfoam, thrombin, Surgicel)
Monitoring
- Standard ASA monitors
- EMG monitoring (triggered — optional but recommended)
- No SSEPs/MEPs typically needed for standard microdiscectomy
Anesthesia Considerations
- General endotracheal anesthesia
- Foley catheter (if CES or expected long case)
- Cefazolin 2g IV
- Dexamethasone 10 mg IV (optional — reduces root edema)
- No paralytic after intubation (if EMG monitoring)
- SBP control (reduce epidural bleeding)
- Verify abdomen is free after positioning
Potential Complications & Contingencies
- Dural tear / CSF leak — primary repair if possible (5-0 or 6-0 Prolene); if not, Duragen + fibrin glue + muscle patch. Flat bed rest x 48-72h post-op
- Nerve root injury — gentle retraction only; if motor worse post-op, MRI to rule out hematoma
- Wrong-level surgery — prevent with meticulous fluoroscopic confirmation; count from sacrum
- Recurrent herniation — 5-15% risk; counsel pre-op. If recurrent: repeat discectomy or consider fusion
- Epidural hematoma — meticulous hemostasis; if new deficit post-op → emergent MRI → return to OR
- Vascular injury (anterior disc penetration) — EXTREMELY rare but fatal; if sudden hypotension after disc space entry → emergent vascular surgery consultation, laparotomy
- Discitis/infection — fever, worsening back pain at 2-4 weeks; MRI with gadolinium, ESR/CRP
Operative Note Template
Preoperative Diagnosis: [Left/Right] L_-S_ disc herniation with [L_/S_] radiculopathy
Postoperative Diagnosis: Same
Procedure: [Left/Right] L_-S_ microsurgical lumbar discectomy
Surgeon: Assistant: Anesthesia: General endotracheal anesthesia
EBL: Minimal (___ mL) Fluids: Specimens: Disc material (send to pathology if concern for infection/tumor) Drains: None Complications: None Implants: None
Indications: The patient is a [age]yo [M/F] with [left/right] [L_/S_] radiculopathy due to a [left/right] L_-S_ [paracentral/foraminal] disc herniation. The patient failed [duration] of conservative management including [PT, NSAIDs, epidural injections]. [The patient presented with progressive L5 foot drop / cauda equina syndrome requiring urgent surgery.] After discussion of risks, benefits, and alternatives, the patient elected to proceed with microsurgical discectomy.
Description of Procedure: After informed consent was verified and the surgical site was marked, the patient was brought to the operating room. General endotracheal anesthesia was induced. The patient was carefully log-rolled to the prone position on a [Wilson frame / Jackson table]. The abdomen was confirmed to be free and hanging. All pressure points were padded, the eyes were free of pressure, and the endotracheal tube was secured. A time-out was performed.
The lower back was prepped and draped in standard sterile fashion. Cefazolin [2g] was administered. The appropriate surgical level was confirmed with AP fluoroscopy using a spinal needle placed at the [L_-S_] interspinous space [counting from the sacrum].
Incision: A [2.5 cm] midline incision was made centered over the [L_-S_] interspace. Dissection was carried through the thoracolumbar fascia. The paraspinal muscles were elevated subperiosteally from the spinous process and lamina on the [left/right] side. A self-retaining retractor was placed.
Laminotomy and decompression: The interlaminar window at [L_-S_] was identified. Using a [Kerrison rongeur / high-speed drill], the inferior edge of the [L_] lamina was removed to expose the ligamentum flavum. The ligamentum flavum was detached from the undersurface of the lamina and excised, exposing the epidural space. [The facet joint was preserved.]
Discectomy: Under the operating microscope, the traversing [L_/S_] nerve root was identified. The root was gently retracted medially. A [large/moderate] [paracentral/foraminal] disc fragment was identified [compressing the nerve root / extruded into the epidural space / migrated cephalad-caudad]. The fragment was removed with a pituitary rongeur. The posterior longitudinal ligament was incised and the annular defect was explored. Additional loose disc material was removed from the disc space. A nerve hook was passed around the nerve root [superiorly, inferiorly, and laterally], confirming complete decompression. The nerve root was freely mobile and pulsatile.
Hemostasis: Hemostasis was achieved with bipolar cautery and [Gelfoam / thrombin-soaked Gelfoam]. The wound was irrigated with antibiotic-containing saline.
Closure: The thoracolumbar fascia was closed with [0 Vicryl] interrupted sutures. The subcutaneous tissue was closed with [3-0 Vicryl]. The skin was closed with [4-0 Monocryl subcuticular suture and Dermabond / staples]. A sterile dressing was applied.
Postoperative: The patient was carefully log-rolled to the supine position, awakened from anesthesia, extubated, and found to have [improved leg pain / intact motor function / baseline neurological status]. The patient was transferred to the PACU in stable condition.
Postoperative Plan
- Same-day discharge (ambulatory surgery) OR overnight observation
- Neuro checks in PACU: Motor and sensory in lower extremities
- Activity: Ambulate same day; no heavy lifting > 10-15 lbs x 6 weeks
- Wound care: Keep dry x 48h; Dermabond will peel off naturally
- Pain: Acetaminophen, NSAIDs, limited narcotics, ice
- DVT prophylaxis: Early ambulation; SCDs if admitted
- Diet: Regular
- If CES presentation: Foley, check post-void residual; may need short-term bladder management
- If dural tear: Flat bed rest x 48-72h, monitor for headache
- Return precautions: Fever, new weakness, bowel/bladder dysfunction, wound drainage, severe worsening pain
- Follow-up: Clinic 2-4 weeks
- Physical therapy: Start at 4-6 weeks post-op
- Expected outcomes: 85-95% good/excellent pain relief for radiculopathy; motor recovery varies (the longer the deficit persisted pre-op, the less likely full recovery)
Chief-Level Case Review
Use these as the senior-level mental model for Lumbar Microdiscectomy:
- Decision point: Localize twice and instrument once: numbering, transitional anatomy, prior hardware, rib count, navigation dataset, and fluoroscopic level confirmation are mandatory.
- Technical lever: Positioning is treatment: table choice, abdomen-free prone setup, alignment goals, shoulders/hips, eyes/plexus pressure, neuromonitoring baselines, and fluoroscopic access all change the case.
- Bailout: Protect neural elements by sequence: decompression before correction when needed, MAP support for cord risk, no long paralytic with MEPs, and immediate response to signal change.
- Postop watch: Finish with construct logic: decompression adequacy, screw purchase, alignment, fusion bed/graft, drain plan, brace/activity orders, postop CT/X-rays, and DVT timing.
Common Pimp Questions
Use these to pressure-test preparation for Lumbar Microdiscectomy:
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]