
Case Prep: Spinal Cord Cavernous Malformation Resection
Case / Approach Snapshot
- Anatomy at risk: cord, roots, dura, posterior elements, segmental and radiculomedullary arteries, venous plexus, and level-specific bony landmarks.
- Operative steps: localize the level, expose while preserving stability, obtain proximal/distal vascular control when relevant, decompress or disconnect/reconstruct the lesion, confirm flow/decompression, and close with CSF-leak prevention; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: neuromonitoring change, bleeding from epidural/foraminal vessels, durotomy, wrong-level exposure, cord swelling/ischemia, instability, and staged/endovascular adjuncts.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [cervical/thoracic] intramedullary spinal cord cavernous malformation presenting with [myelopathy / acute deficit from hemorrhage / sensory changes] planned for laminectomy and midline (or dorsal-presenting) myelotomy for microsurgical resection.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior cervical approach or posterior thoracolumbar approach — posterior myelotomy corridor and closure principles by level.
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Spinal Cord Cavernous Malformation: A Case Report — Izi Z. Global pediatric health 2023. PubMed
- How I do it: resection of spinal cord cavernous malformation — Agosti E. Acta neurochirurgica 2022. PubMed
- A Rare Instance of Spinal Cord Cavernous Malformation With Adjacent Intramedullary Microhemorrhage — Yu L. The Journal of craniofacial surgery 2024. PubMed
- Clinical features and long-term outcomes of pediatric spinal cord cavernous malformation-a report of 18 cases and literature review — Zhang L. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2021. PubMed
- C5-C6 Cervical Spinal Cord Cavernous Malformation Microsurgical Resection: 2-Dimensional Operative Video — Enriquez-Marulanda A. Operative neurosurgery (Hagerstown, Md.) 2019. PubMed
- Natural history of hemorrhagic events in spinal cord cavernous malformation: an updated systematic review and Meta-Analysis — Wadhwa A. Neurosurgical review 2026. PubMed
- Acceptance of Early Surgery for Treatment of Spinal Cord Cavernous Malformation in Contemporary Japan — Kurokawa R. Neurospine 2023. PubMed
- Ascending Spinal Cord Infarction Secondary to Recurrent Spinal Cord Cavernous Malformation Hemorrhage — Huntley GD. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association 2017. PubMed
- Conservative and Surgical Management of Spinal Cord Cavernous Malformations — Ohnishi YI. World neurosurgery: X 2020. PubMed
- Microsurgical resection of symptomatic intramedullary cervical spinal cord cavernous malformation — Dziedzic TA. Neurosurgical focus: Video 2019. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
 Figure 1. Source: The Reality of Benefit in Surgical Removal for Spinal Cord Cavernous Malformation: Commentary on “Acceptance of Early Surgery for Treatment of Spinal Cord Cavernous Malformation in Contemporary Japan” — Neurospine. 2023 Jun 30;20(2):595–6. doi: 10.14245/ns.2346574.287; CC BY-NC.
Figure 1. Source: The Reality of Benefit in Surgical Removal for Spinal Cord Cavernous Malformation: Commentary on “Acceptance of Early Surgery for Treatment of Spinal Cord Cavernous Malformation in Contemporary Japan” — Neurospine. 2023 Jun 30;20(2):595–6. doi: 10.14245/ns.2346574.287; CC BY-NC.
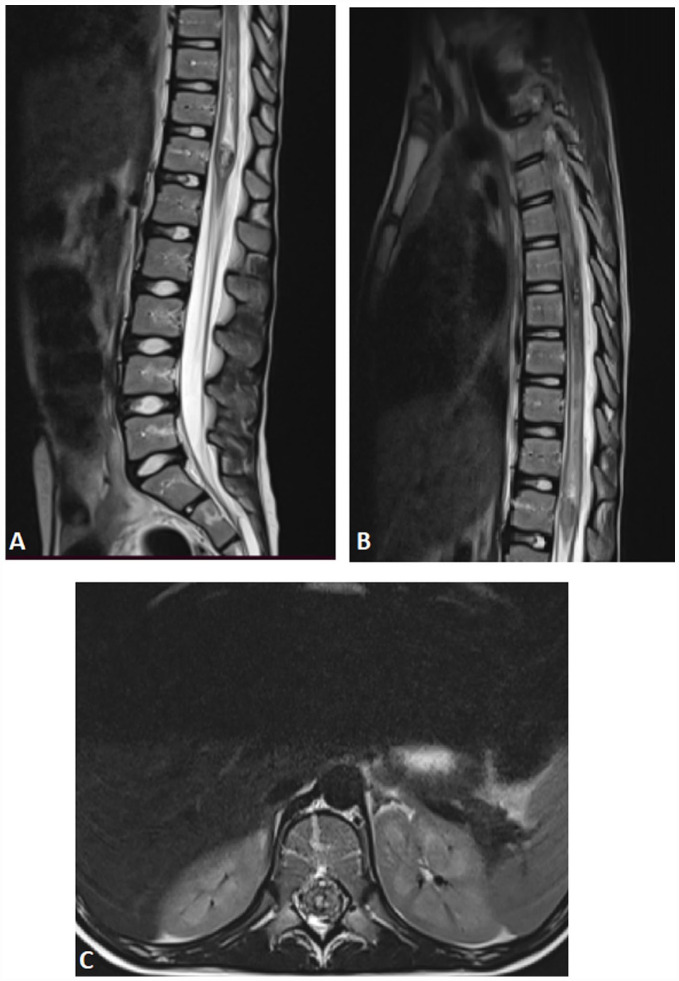 Figure 1.. Sagittal (A and B) and axial (C) T2-W spinal MR images shows 2 focal hyperintensity with hypointense edge with surrounding spinal cord edema, this appearance described as « Popcorn ». Source: Spinal Cord Cavernous Malformation: A Case Report — Global Pediatric Health 2023; CC BY-NC.
Figure 1.. Sagittal (A and B) and axial (C) T2-W spinal MR images shows 2 focal hyperintensity with hypointense edge with surrounding spinal cord edema, this appearance described as « Popcorn ». Source: Spinal Cord Cavernous Malformation: A Case Report — Global Pediatric Health 2023; CC BY-NC.
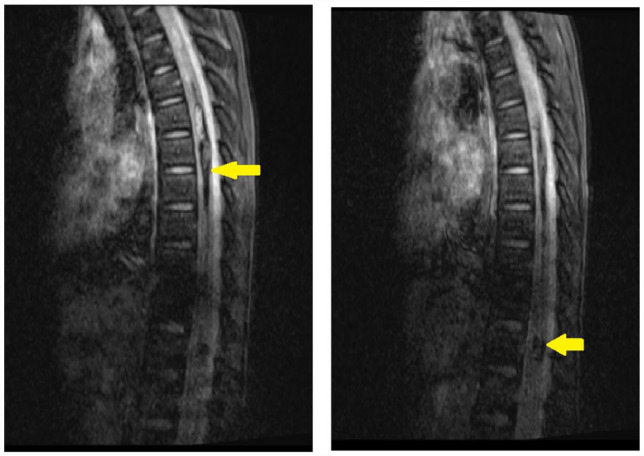 Figure 2.. Susceptibility-weighted imaging gradient echo (GE) shows hypointense lesions “blooming.” Source: Spinal Cord Cavernous Malformation: A Case Report — Global Pediatric Health 2023; CC BY-NC.
Figure 2.. Susceptibility-weighted imaging gradient echo (GE) shows hypointense lesions “blooming.” Source: Spinal Cord Cavernous Malformation: A Case Report — Global Pediatric Health 2023; CC BY-NC.
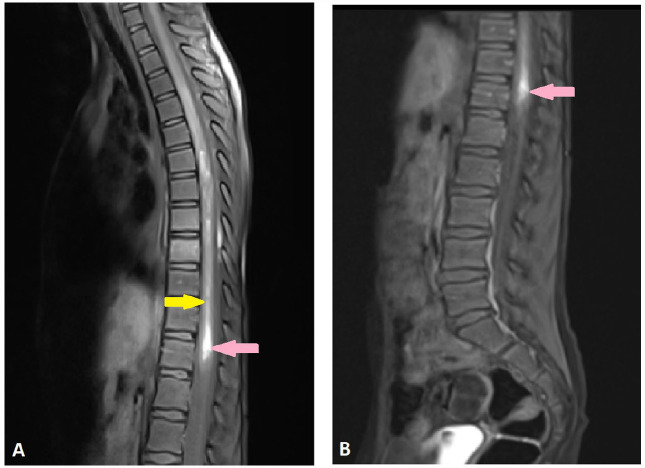 Figure 3.. Sagittal T1-W spinal MR images before (A) and after injection of Gadolinium (B) shows 2 focal hyperintensity with no enhancement (pink arrows), with linear hyperintensity reflect… Source: Spinal Cord Cavernous Malformation: A Case Report — Global Pediatric Health 2023; CC BY-NC.
Figure 3.. Sagittal T1-W spinal MR images before (A) and after injection of Gadolinium (B) shows 2 focal hyperintensity with no enhancement (pink arrows), with linear hyperintensity reflect… Source: Spinal Cord Cavernous Malformation: A Case Report — Global Pediatric Health 2023; CC BY-NC.
 Figure 5. Source: Spinal Cord Cavernous Malformation: A Case Report — Glob Pediatr Health. 2023 Jul 6;10:2333794X231184317. doi: 10.1177/2333794X231184317; CC BY-NC.
Figure 5. Source: Spinal Cord Cavernous Malformation: A Case Report — Glob Pediatr Health. 2023 Jul 6;10:2333794X231184317. doi: 10.1177/2333794X231184317; CC BY-NC.
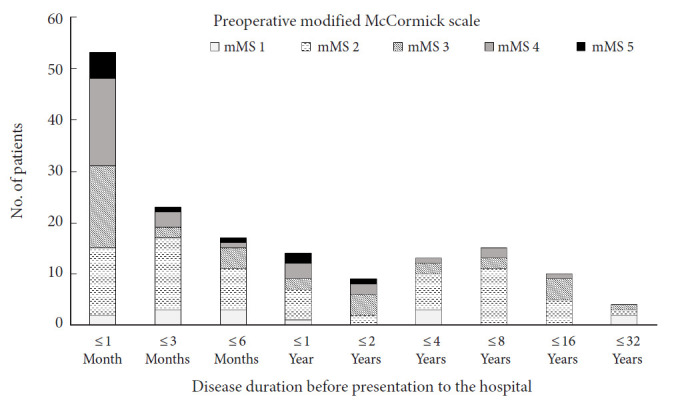 Fig. 1.. Disease duration before presentation to the hospital, stratified by preoperative modified McCormick scale (mMS). Source: Acceptance of Early Surgery for Treatment of Spinal Cord Cavernous Malformation in Contemporary Japan — Neurospine 2023; CC BY-NC.
Fig. 1.. Disease duration before presentation to the hospital, stratified by preoperative modified McCormick scale (mMS). Source: Acceptance of Early Surgery for Treatment of Spinal Cord Cavernous Malformation in Contemporary Japan — Neurospine 2023; CC BY-NC.
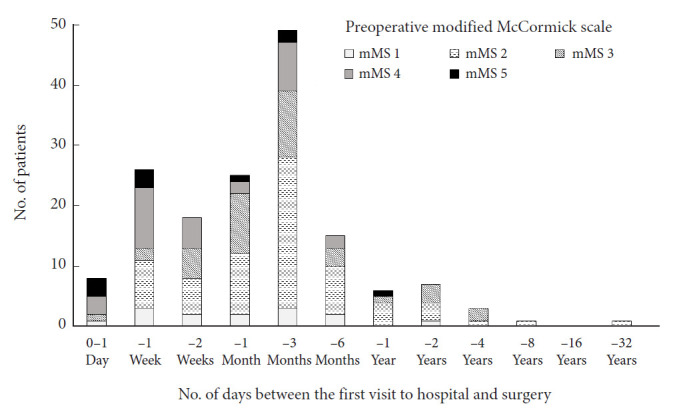 Fig. 2.. Number of days between the first visit to hospital and surgery, stratified by preoperative modified McCormick scale (mMS). Source: Acceptance of Early Surgery for Treatment of Spinal Cord Cavernous Malformation in Contemporary Japan — Neurospine 2023; CC BY-NC.
Fig. 2.. Number of days between the first visit to hospital and surgery, stratified by preoperative modified McCormick scale (mMS). Source: Acceptance of Early Surgery for Treatment of Spinal Cord Cavernous Malformation in Contemporary Japan — Neurospine 2023; CC BY-NC.
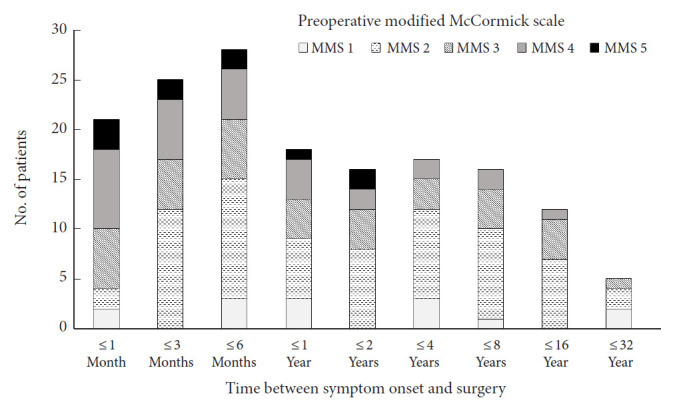 Fig. 3.. Time between symptom onset and surgery, stratified by preoperative modified McCormick scale (mMS). Source: Acceptance of Early Surgery for Treatment of Spinal Cord Cavernous Malformation in Contemporary Japan — Neurospine 2023; CC BY-NC.
Fig. 3.. Time between symptom onset and surgery, stratified by preoperative modified McCormick scale (mMS). Source: Acceptance of Early Surgery for Treatment of Spinal Cord Cavernous Malformation in Contemporary Japan — Neurospine 2023; CC BY-NC.
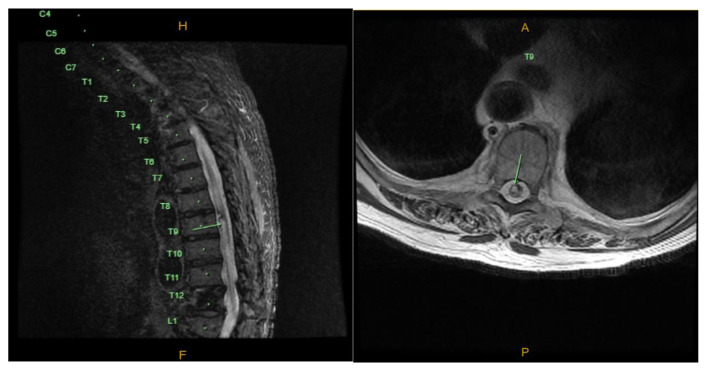 Fig. 1. MRI demonstrating cavernous malformation in Short Tau Inversion Recovery sagittal and T2 axial views. Source: Spontaneous Hemorrhage of Thoracic Cavernous Malformation Leading to Bilateral Lower Extremity Paralysis — Journal of Community Hospital Internal Medicine Perspectives 2023; CC BY-NC.
Fig. 1. MRI demonstrating cavernous malformation in Short Tau Inversion Recovery sagittal and T2 axial views. Source: Spontaneous Hemorrhage of Thoracic Cavernous Malformation Leading to Bilateral Lower Extremity Paralysis — Journal of Community Hospital Internal Medicine Perspectives 2023; CC BY-NC.
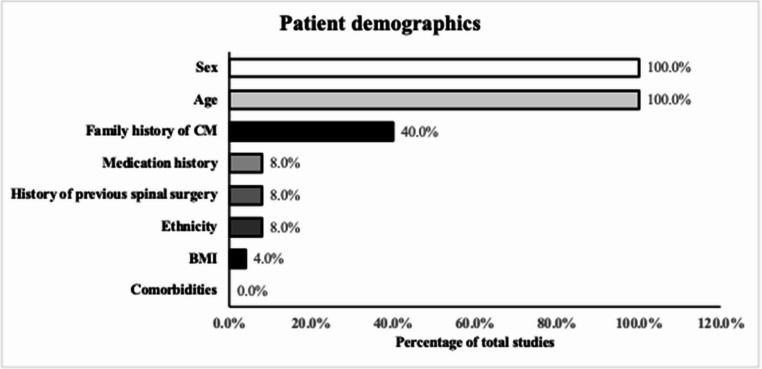 Fig. 2. Proportion of included studies reporting demographic variables Source: Reporting practices of baseline and surgical variables in spinal cavernous malformation surgery: a systematic review — Neurosurgical Review 2026; CC BY.
Fig. 2. Proportion of included studies reporting demographic variables Source: Reporting practices of baseline and surgical variables in spinal cavernous malformation surgery: a systematic review — Neurosurgical Review 2026; CC BY.
History of Present Illness
- Chief complaint: Stepwise or acute myelopathy/sensory-motor deficits from recurrent micro-hemorrhage
- Number of symptomatic hemorrhages (rebleed risk rises after first), pattern (stepwise decline with partial recovery)
- Familial (multiple lesions, CCM genes), prior radiation
Imaging Review
MRI (T2, GRE/SWI, T1±Gad)
- “Popcorn”/mulberry lesion with hemosiderin rim, blooming on GRE/SWI
- Location within cord, does it reach the pial/ependymal surface? (presenting to surface = safer resection corridor)
- Associated DVA (preserve), syrinx, multiple lesions (familial)
- Non-enhancing (vs tumor)
Surface-Presentation and Entry-Zone Read
- Dorsal midline presentation: safest route is dorsal median sulcus myelotomy, using pial/hemosiderin staining and dorsal vein anatomy to stay midline.
- Dorsolateral presentation: use the lesion’s pial presentation or dorsal root entry zone rather than forcing a midline split across functional dorsal columns.
- Ventral/deep lesion: conservative management or delayed surgery may be safer unless recurrent hemorrhage/progression justifies a higher-risk route.
- Associated DVA: preserve it; cavernoma removal is the goal, not venous obliteration.
- Recent hemorrhage: edema and blood products may help define a gliotic plane but can also make cord swollen and monitoring fragile; timing should balance recovery from acute deficit with rebleed risk and surgical plane clarity.
Labs
- CBC, BMP, Coags, type and screen
Neurological Examination
- Meticulous motor/sensory (dorsal columns, spinothalamic) baseline, reflexes, gait, sphincter
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: radiolucent spine-capable table selected for approach, imaging, instrumentation, patient size, and alignment goals; keep abdomen free for prone cases.
- OR setup: microscope, neuromonitoring, spinal angiography/DSA images loaded, ICG/Doppler, clips/coagulation tools, laminectomy/instrumentation backup, and blood available for vascular lesions.
- Special needs: arterial line, Foley, MAP support for cord perfusion, no long paralytic with MEPs, CSF drainage plan only when indicated, and coordination with endovascular/staged treatment.
- Immediate postop orders: ICU neuro checks with motor/sensory/sphincter focus, MAP target, MRI/angiography confirmation plan, drain/hematoma watch, steroid/pain regimen, DVT timing, and rehab planning.
Diagnosis & Indication
- Indication: Symptomatic hemorrhage(s), progressive deficit, lesion reaching or near a surface; resect to prevent further hemorrhage
- Conservative if deep, asymptomatic, no surface presentation (surgical morbidity vs natural history)
- Complete resection required (residual → rebleed); preserve associated DVA
Operate vs Observe
| Scenario | Usual strategy |
|---|---|
| Symptomatic hemorrhage with lesion at/near pial surface | Favor microsurgical resection once medically optimized |
| Recurrent stepwise deficits or repeated hemorrhage | Favor resection if a safe entry zone exists |
| Mild single event, deep ventral lesion, stable recovery | Consider observation with close MRI/exam follow-up |
| Familial/multiple cavernomas | Treat only the symptomatic culprit lesion; screen neuraxis/brain |
| Progressive myelopathy with enlarging lesion/syrinx | Favor resection if corridor risk is acceptable |
The central decision is not “cavernoma equals surgery.” It is whether the natural-history risk now exceeds the morbidity of entering that specific spinal cord surface.
Position
- OR table/bed: radiolucent spine-capable table selected for approach, imaging, instrumentation, patient size, and alignment goals; keep abdomen free for prone cases.
- Prone, Mayfield/foam, IONM baseline (MEP, SSEP, D-wave); per level
Key Surgical Steps
- Laminectomy over the lesion (navigation/level localization), ultrasound to confirm
- Midline durotomy, tack-up
- Identify the safest entry: where the cavernoma presents to the pial surface (hemosiderin staining), or midline myelotomy (dorsal median sulcus) / dorsal root entry zone for lesions not reaching surface
- Myelotomy, enter the lesion, internally debulk
- Circumferential dissection in the gliotic/hemosiderin plane, deliver the cavernoma completely
- Preserve the associated DVA (do NOT coagulate — venous infarction)
- Hemostasis (gentle), inspect for complete removal
- Watertight dural closure, sealant
Myelotomy and Resection Nuances
- Confirm level with fluoroscopy/navigation and ultrasound before durotomy; a one-level error in an intramedullary case is catastrophic.
- Open the pia sharply and anchor with fine pial sutures; traction should be on pia/lesion capsule, not normal cord.
- Stay in the hemosiderin/gliotic plane. If normal cord fibers start stretching, stop and re-find the capsule-plane interface.
- Use low-current bipolar sparingly; cavernomas are low-flow lesions, and thermal injury to adjacent tracts is often worse than patient bleeding.
- Remove old clot and mulberry components completely, then inspect the cavity with the microscope angled around all poles.
- Do not chase hemosiderin-stained gliosis as if it were residual cavernoma; the residual risk is lesion tissue, not the stain.
Neuromonitoring Response
- SSEP drop during dorsal column split: pause, irrigate, reduce traction, raise MAP, and narrow the myelotomy.
- MEP/D-wave change: stop resection, raise MAP, reverse any mechanical distortion, remove compressive clot/cottonoid, and wait for recovery before proceeding.
- Stable D-wave with MEP change: may predict recoverable deficit, but still treat it as a warning; do not use it as permission for aggressive traction.
- No reliable baseline: make the corridor and resection more conservative; the anatomy must carry the safety margin.
Critical Anatomy & Structures at Risk
- Spinal cord tracts — dorsal columns (myelotomy), corticospinal
- Associated DVA — preserve
- Anterior spinal artery / perforators (ventral lesions)
- Dura (CSF leak)
Equipment
- Microscope, ultrasound, micro-instruments, fine bipolar, pial sutures
- Navigation/fluoroscopy, dural substitute, sealant
Monitoring
- SSEPs, MEPs, D-wave, EMG
Anesthesia
- MAP > 85, arterial line, no paralytic (IONM), prone precautions
Potential Complications
- Neurological worsening — dorsal column (proprioception/sensory, often transient), motor
- Incomplete resection → rebleed; DVA injury → venous infarction
- CSF leak, deformity (post-laminectomy)
Rescue Plans
- Cavity bleeding: use gentle irrigation, small cottonoids, patience, and focal bipolar only on lesion remnants; avoid coagulating the DVA or normal cord surface.
- Suspected residual: inspect with angled microscope, ultrasound, and postoperative MRI; if uncertain but monitoring is worsening, stop rather than converting a small residual into a major deficit.
- Cord swelling: loosen retraction, maintain MAP/oxygenation, avoid hypotension, consider steroids per surgeon preference, and close without constrictive grafting.
- Dural closure under tension: graft generously and test with Valsalva; postoperative CSF leak around a spinal cord myelotomy is an avoidable second hit.
- Postoperative decline: urgent MRI for hematoma/residual compression, maintain MAP, reverse coagulopathy, and return to OR for compressive hematoma or tight closure.
Operative Note Template
Preoperative Diagnosis: [Cervical/thoracic] intramedullary spinal cord cavernous malformation [with prior hemorrhage]
Postoperative Diagnosis: Same
Procedure: [Level] laminectomy with myelotomy and microsurgical resection of intramedullary cavernous malformation
Surgeon / Assistant: Anesthesia: Total IV anesthesia, no paralytic EBL / Fluids: Adjuncts: Microscope, ultrasound, pial sutures, fine bipolar; MEP/SSEP/D-wave/EMG; MAP > 85 Implants: Dural substitute, sealant Complications: None
Indications: [Age]yo [M/F] with a symptomatic intramedullary cavernous malformation at [level] after [≥1–2 hemorrhages/progressive deficit] reaching/near a surface. Resection was planned to prevent rebleed. Risks (dorsal-column/motor deficit, DVA injury) discussed.
Description of Procedure: After consent and time-out, TIVA was induced (MAP > 85, no paralytic) and MEP/SSEP/D-wave monitoring established. The patient was positioned prone; a laminectomy was performed over the lesion and ultrasound confirmed localization. A midline durotomy was made and the cord exposed.
The lesion was approached [at its pial presentation / via a midline myelotomy] and entered; it was internally debulked and dissected circumferentially in the gliotic/hemosiderin plane and removed completely. The associated developmental venous anomaly was identified and preserved. Hemostasis was gentle and complete removal confirmed. A watertight dural closure was performed with sealant.
Closure was completed in layers. The patient was transferred with MAP support and CSF-leak precautions; transient dorsal-column dysfunction was anticipated.
Postoperative Plan
- ICU, neuro checks q1h (sensory/motor/proprioception), MAP support, CSF leak precautions
- MRI postop (complete resection), expect possible transient dorsal column dysfunction
- Rehab/PT-OT, DVT prophylaxis (mechanical)
- Familial: genetics, screen neuraxis/brain for other cavernomas; follow-up MRI
Chief-Level Case Review
Use these as the senior-level mental model for Spinal Cord Cavernous Malformation Resection:
- Decision point: The operation is won or lost on control: identify inflow, outflow, perforators, collateral options, and the fastest route to temporary control before exposing the lesion itself.
- Technical lever: Do not accept a cosmetic result over physiology: ICG/Doppler/DSA, branch patency, perforator preservation, and parent-vessel caliber matter more than how the clip or resection bed looks.
- Bailout: Have a rupture or ischemia script ready: lower pressure, suction strategy, temporary occlusion time, heparin/reversal plan, bypass/reconstruction threshold, and postop BP targets.
- Postop watch: Postop danger is delayed: vasospasm, thromboembolism, hyperperfusion, hemorrhage, edema, hydrocephalus, and seizure plans need explicit orders.
Common Pimp Questions
Use these to pressure-test preparation for Spinal Cord Cavernous Malformation Resection:
- What is the proximal-control plan before the lesion is manipulated?
- Which branch, perforator, or venous structure is most likely to be injured in this exposure?
- What are the intraoperative rupture steps, including temporary clip, suction, BP, and backup clip strategy?
- What confirms treatment success: ICG, Doppler, puncture/deflation, DSA, or postoperative CTA?
- What postoperative BP, vasospasm, antiplatelet, or anticoagulation issue changes the orders tonight?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Preferred approach side, sylvian split style, and cisternal-opening sequence: [attending-specific]
- Temporary clip threshold, burst-suppression preference, and BP during occlusion: [attending-specific]
- Clip manufacturer/shape sequence and whether Doppler, ICG, puncture, or intraop DSA is routine: [attending-specific]
- Antiplatelet/anticoagulation reversal and restart timing: [attending-specific]