
Case Prep: Vertebral Corpectomy and Reconstruction (Metastatic / Primary Vertebral Tumor)
Case / Approach Snapshot
- Anatomy at risk: cord, roots, dura, epidural venous plexus, tumor vascular supply, vertebral body/posterior element involvement, and stabilization corridors.
- Operative steps: define oncologic and neurologic goals, localize levels, decompress neural elements, obtain tissue or resect/debulk safely, reconstruct stability, and coordinate radiation/systemic therapy planning; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: major blood loss, neuromonitoring change, durotomy/CSF leak, pathologic instability, wound breakdown after radiation, residual disease strategy, and staged embolization or reconstruction.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [metastatic / primary] tumor of the [T_/L_] vertebral body with [cord compression / instability / intractable pain] planned for [posterolateral / anterior / combined] corpectomy, decompression, and instrumented reconstruction.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
CNS Video Library
🧭 Operative approach: Transthoracic approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Thoracic corpectomy and vertebral body reconstruction (TCVBR): a systematic review and meta-analysis — Badary A. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 2026. PubMed
- Distractable vertebral cages for reconstruction after cervical corpectomy — Woiciechowsky C. Spine 2005. PubMed
- Transpedicular partial corpectomy without anterior vertebral reconstruction in thoracic spinal metastases — Chen YJ. Spine 2007. PubMed
- Medium Term Outcomes in Palliative Transpedicular Corpectomy with Cement Based Anterior Vertebral Reconstruction Performed for Patients with Spinal Metastasis — Rizkallah M. Spine 2024. PubMed
- Palliative transpedicular partial corpectomy without anterior vertebral reconstruction in lower thoracic and thoracolumbar junction spinal metastases — Chang CC. Journal of orthopaedic surgery and research 2015. PubMed
- Titanium cage reconstruction after cervical corpectomy — Dorai Z. Journal of neurosurgery 2003. PubMed
- The use of an expandable cage for corpectomy reconstruction of vertebral body tumors through a posterior extracavitary approach: a multicenter consecutive case series of prospectively followed patients — Shen FH. The spine journal : official journal of the North American Spine Society 2008. PubMed
- Differences in surgical outcome after anterior corpectomy and reconstruction with an expandable cage with rectangular footplates between thoracolumbar and lumbar osteoporotic vertebral fracture — Terai H. North American Spine Society journal 2021. PubMed
- Comparison of polymethylmethacrylate versus expandable cage in anterior vertebral column reconstruction after posterior extracavitary corpectomy in lumbar and thoraco-lumbar metastatic spine tumors — Eleraky M. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 2011. PubMed
- Cervical spinal stenosis: outcome after anterior corpectomy, allograft reconstruction, and instrumentation — Mayr MT. Journal of neurosurgery 2002. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
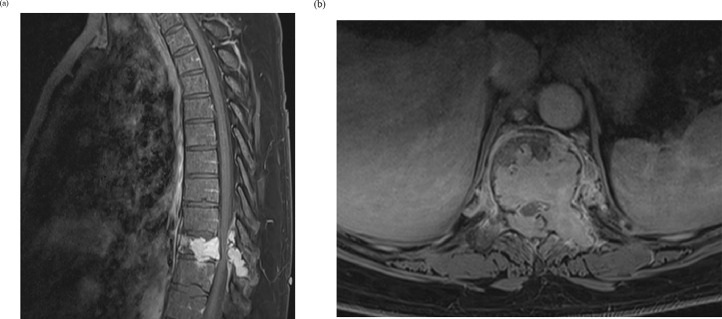 Fig. 1. Sagittal (a) and Axial (b) T1 Post Gadolinium MRI: Expansile lytic lesion involving the T10 vertebral body and posterior elements with pathologic fracture and epidural compression. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
Fig. 1. Sagittal (a) and Axial (b) T1 Post Gadolinium MRI: Expansile lytic lesion involving the T10 vertebral body and posterior elements with pathologic fracture and epidural compression. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
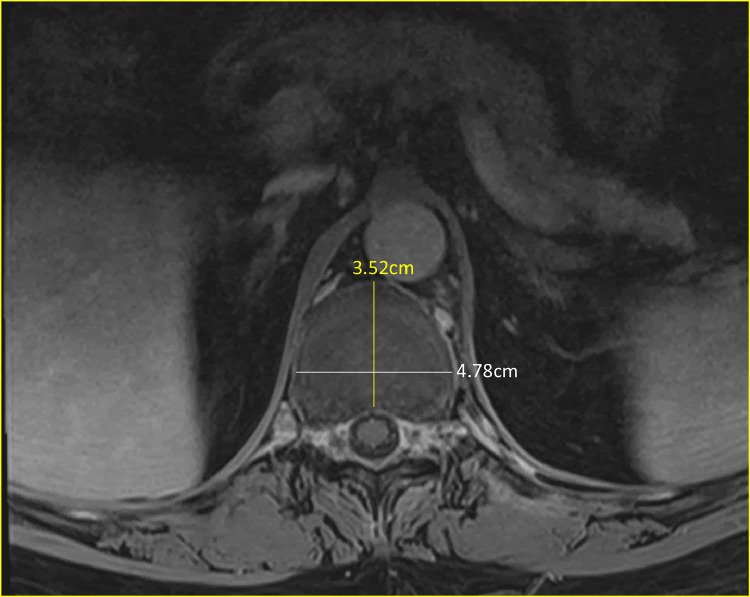 Fig. 2. Axial T1 MRI Thoracic Spine Post-Gadolinium: superior endplate of the caudal T11 vertebral body indicating larger footprint of reconstruction required during VBR. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
Fig. 2. Axial T1 MRI Thoracic Spine Post-Gadolinium: superior endplate of the caudal T11 vertebral body indicating larger footprint of reconstruction required during VBR. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
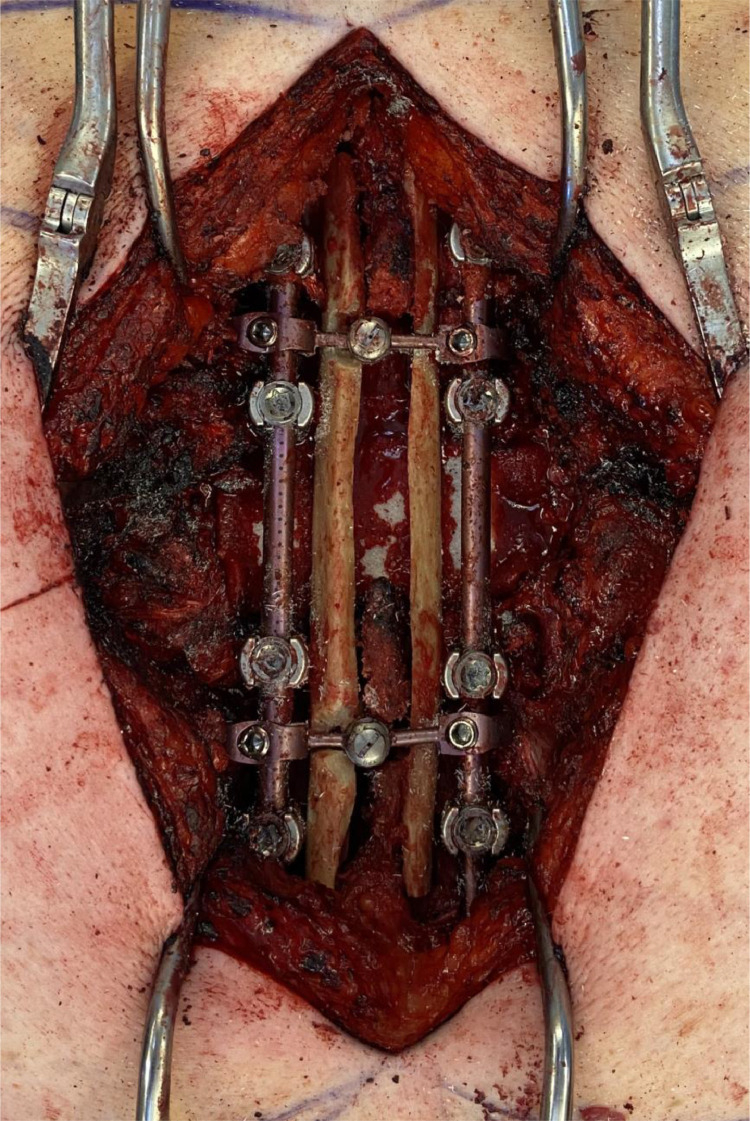 Fig. 3. Intra-operative view of the posterior approach for vertebral body reconstruction. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
Fig. 3. Intra-operative view of the posterior approach for vertebral body reconstruction. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
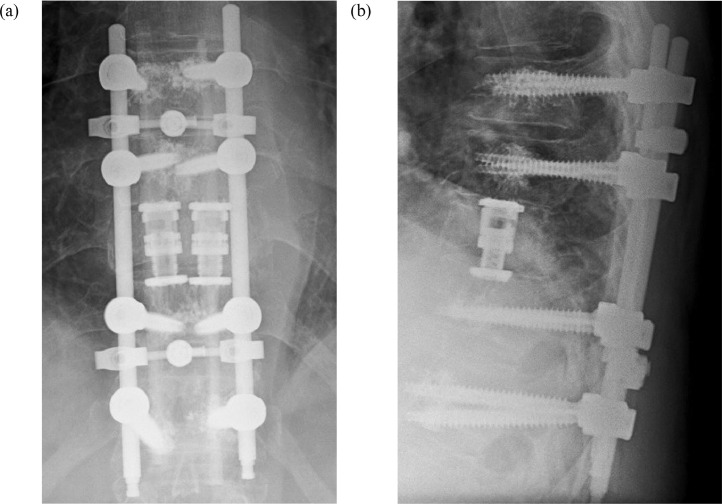 Fig. 4. AP (a) and lateral (b) radiographs of the thoracic spine showing bilateral expandable cage placement during vertebral body reconstruction. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
Fig. 4. AP (a) and lateral (b) radiographs of the thoracic spine showing bilateral expandable cage placement during vertebral body reconstruction. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
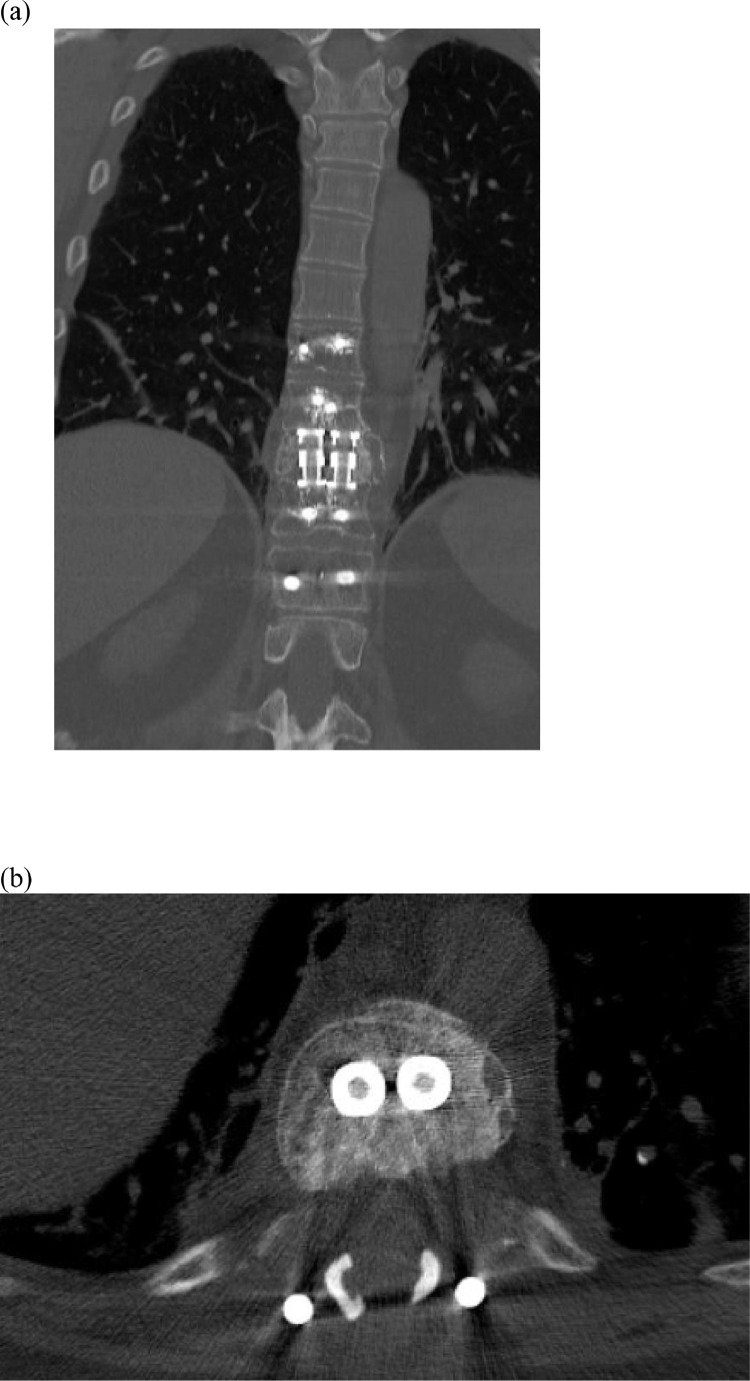 Fig. 5. Coronal (a) and axial (b) CT Thoracic Spine Without IV Contrast at 6-month follow up showing arthrodesis across the corpectomy defect Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
Fig. 5. Coronal (a) and axial (b) CT Thoracic Spine Without IV Contrast at 6-month follow up showing arthrodesis across the corpectomy defect Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
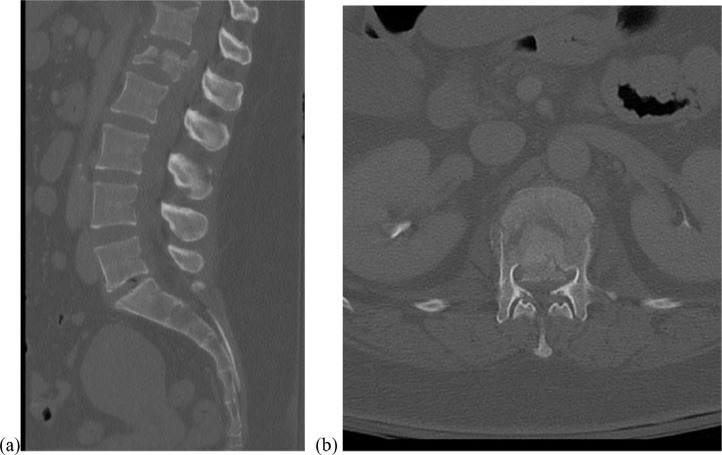 Fig. 6. Representative mid-sagittal (a) and axial (b) CT cuts of L1 burst fracture with significant bony retropulsion. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
Fig. 6. Representative mid-sagittal (a) and axial (b) CT cuts of L1 burst fracture with significant bony retropulsion. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
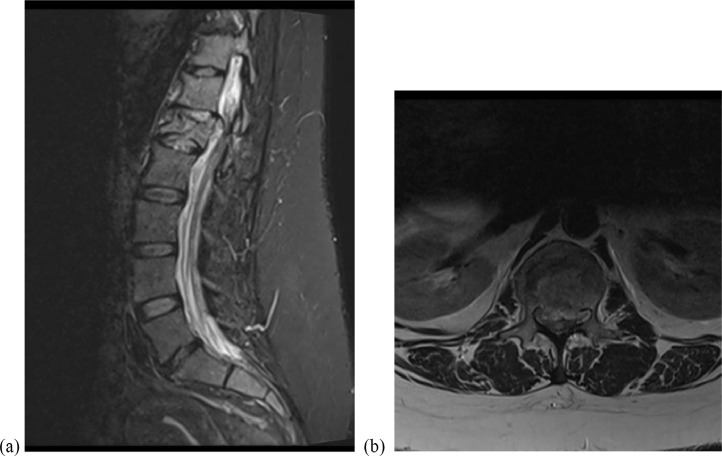 Fig. 7. Representative mid-sagittal STIR MRI (a) and T2 sequence MRI (b) of L1 burst fracture demonstrating cord compression. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
Fig. 7. Representative mid-sagittal STIR MRI (a) and T2 sequence MRI (b) of L1 burst fracture demonstrating cord compression. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
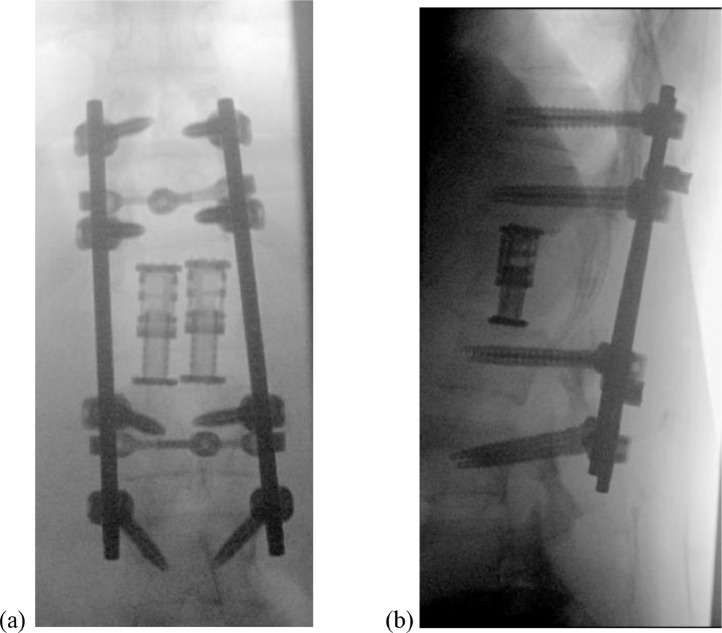 Fig. 8. Final intraoperative AP (a) and lateral (b) radiographs for L1 vertebral body reconstruction with bilateral expandable cages. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
Fig. 8. Final intraoperative AP (a) and lateral (b) radiographs for L1 vertebral body reconstruction with bilateral expandable cages. Source: Dual expandable interbody cage utilization for enhanced stability in vertebral column reconstruction following thoracolumbar corpectomy: A report of two cases — North American Spine Society Journal 2021; CC BY-NC-ND.
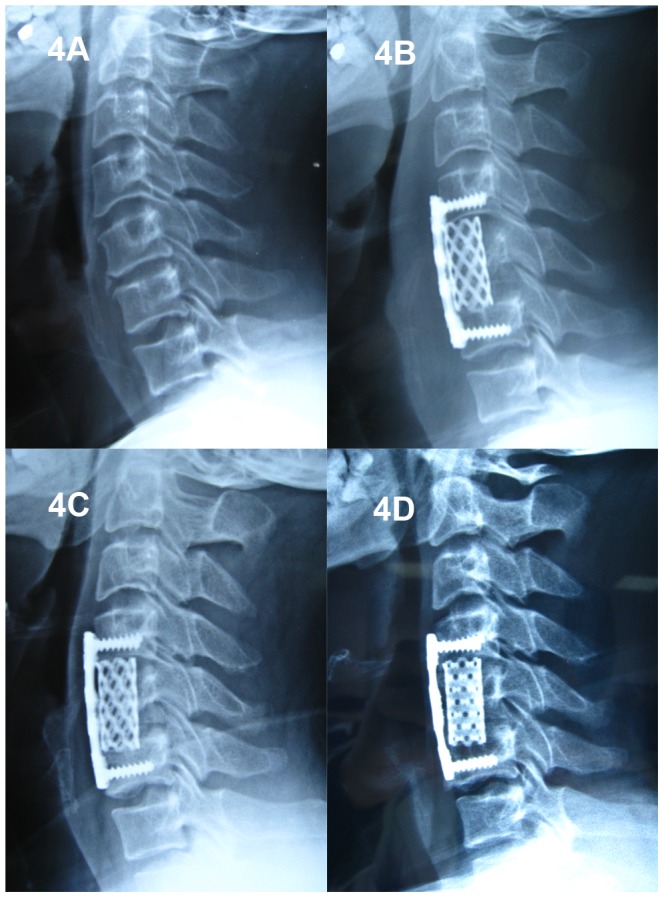 Figure 4. A 53-year-old male who underwent 1-level corpectomy with a titanium mesh cage used for cervical reconstruction.The preoperative cervical X-ray film (4A) and immediately postoperative… Source: Evaluation of Anterior Cervical Reconstruction with Titanium Mesh Cages versus Nano-Hydroxyapatite/Polyamide66 Cages after 1- or 2-Level Corpectomy for Multilevel Cervical Spondylotic Myelopathy: A Retrospective Study of 117 Patients — PLoS ONE 2014; CC BY.
Figure 4. A 53-year-old male who underwent 1-level corpectomy with a titanium mesh cage used for cervical reconstruction.The preoperative cervical X-ray film (4A) and immediately postoperative… Source: Evaluation of Anterior Cervical Reconstruction with Titanium Mesh Cages versus Nano-Hydroxyapatite/Polyamide66 Cages after 1- or 2-Level Corpectomy for Multilevel Cervical Spondylotic Myelopathy: A Retrospective Study of 117 Patients — PLoS ONE 2014; CC BY.
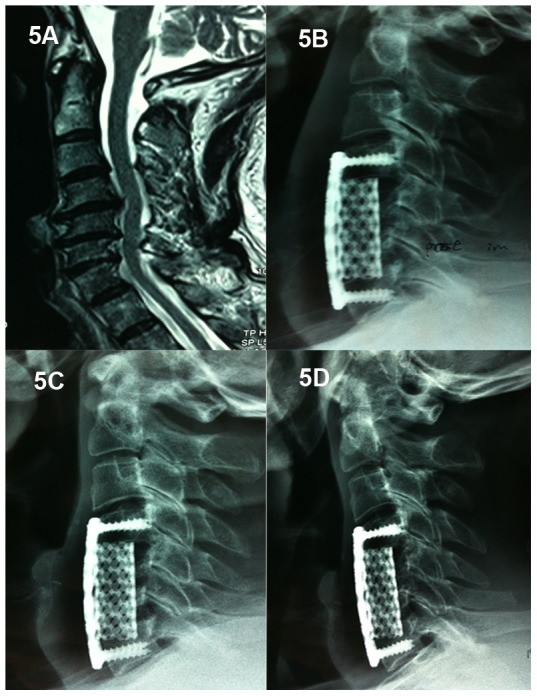 Figure 5. A 46-year-old male who underwent 2-level corpectomy with a titanium mesh cage used for cervical reconstruction.A cervical MRI scan (5A) shows multi-level disc herniations (C4/5, C5/6,… Source: Evaluation of Anterior Cervical Reconstruction with Titanium Mesh Cages versus Nano-Hydroxyapatite/Polyamide66 Cages after 1- or 2-Level Corpectomy for Multilevel Cervical Spondylotic Myelopathy: A Retrospective Study of 117 Patients — PLoS ONE 2014; CC BY.
Figure 5. A 46-year-old male who underwent 2-level corpectomy with a titanium mesh cage used for cervical reconstruction.A cervical MRI scan (5A) shows multi-level disc herniations (C4/5, C5/6,… Source: Evaluation of Anterior Cervical Reconstruction with Titanium Mesh Cages versus Nano-Hydroxyapatite/Polyamide66 Cages after 1- or 2-Level Corpectomy for Multilevel Cervical Spondylotic Myelopathy: A Retrospective Study of 117 Patients — PLoS ONE 2014; CC BY.
History of Present Illness
- Chief complaint: Mechanical/axial pain, progressive myelopathy/radiculopathy, deformity
- Known primary (lung, breast, prostate, renal, myeloma) vs primary bone tumor (chordoma, GCT, osteosarcoma)
- Onset/progression of neurological deficit (timing affects recovery), ambulatory status
- Frameworks: NOMS (Neurologic, Oncologic, Mechanical, Systemic), SINS (Spinal Instability Neoplastic Score), ESCC (epidural cord compression grade)
Imaging Review
MRI whole spine (T1±Gad, T2, STIR)
- Vertebral body involvement, epidural cord compression (ESCC grade), cord signal, multilevel disease, paraspinal extension
CT
- Bony destruction, SINS (instability), pedicle/posterior element involvement, planning instrumentation
CTA / Angiography + Embolization
- Preoperative embolization for hypervascular tumors (renal cell, thyroid, others) — reduces blood loss
- Vascular anatomy, artery of Adamkiewicz (thoracolumbar)
Staging
- Primary workup/staging, biopsy if unknown primary
Labs
- CBC, BMP, Coags, Type and crossmatch (2-4+ units), calcium (myeloma), tumor markers as indicated
Neurological Examination
- Detailed motor/sensory level, reflexes, ambulation, bowel/bladder, performance status
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- OR setup: microscope, fluoroscopy/navigation, neuromonitoring, tumor debulking/microsurgical set, dural repair materials, instrumentation/corpectomy trays as indicated, and blood available.
- Special needs: arterial line/Foley for long cases, dexamethasone for cord edema when indicated, MAP support for myelopathy/cord manipulation, oncology/radiation plan, and pathology/frozen specimen workflow.
- Immediate postop orders: frequent motor/sensory exams, MAP support if cord manipulation or deficit, MRI/CT/X-rays per tumor/construct, steroid taper, drain/dural-leak precautions, brace/activity, DVT timing, and oncology/radiation follow-up.
Goals & Approach
- Goals: Circumferential cord decompression, mechanical stabilization, local tumor control, pain/function — separation surgery (decompress + stabilize, leave margin) increasingly favored + postop SRS for mets; en bloc spondylectomy for primary/isolated curable tumors
- Approach: posterolateral transpedicular (single-stage, common for thoracic mets), anterior (corpectomy with direct access), or combined/360-degree
Position
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- Prone (posterolateral) or lateral/supine (anterior thoracic/lumbar — may need thoracic/access surgeon); Mayfield/pinned; IONM baseline
Key Surgical Steps (Posterolateral Transpedicular Corpectomy)
- Level localization, midline incision, expose posterior elements
- Pedicle screw instrumentation above and below (typically 2 levels each side) for reconstruction
- Laminectomy at involved level, identify and protect cord/thecal sac
- Transpedicular/costotransversectomy access: remove pedicle(s), facets, rib head (thoracic) to reach the vertebral body laterally/anteriorly
- Ligate the involved nerve root (thoracic — sacrificable) for working corridor if needed
- Corpectomy: piecemeal removal of tumor/vertebral body, circumferential decompression of the thecal sac (remove posterior body/epidural tumor)
- Anterior column reconstruction: expandable cage / PMMA + mesh in the corpectomy defect
- Place rods, secure construct, restore alignment, compress/distract as needed
- Confirm decompression and hardware on fluoroscopy
- Hemostasis (tumor bleeding — embolization helps), drain, closure
Critical Anatomy & Structures at Risk
- Spinal cord — compression, manipulation; MAP support
- Segmental/radicular arteries (artery of Adamkiewicz, thoracolumbar left) — cord infarction
- Great vessels (anterior, esp. lumbar/anterior approach), pleura/lung (thoracic), aorta
- Nerve roots (thoracic sacrificable; lumbar must preserve)
- Dura (epidural tumor adherence — CSF leak)
Equipment
- Pedicle screw/rod system, expandable cage / PMMA-mesh for reconstruction
- High-speed drill, Kerrison, curettes, tumor instruments
- Fluoroscopy/navigation, cell saver (caution in tumor — controversial), crossmatched blood
- Preop embolization, hemostatic agents, dural repair materials
Monitoring
- SSEPs, MEPs, EMG
Anesthesia
- Arterial line, central access, crossmatched blood/massive transfusion ready, MAP > 85, prone/positioning precautions, possible thoracic/access surgeon
Potential Complications
- Major hemorrhage (vascular tumors — embolize preop)
- Neurological injury (cord/root/vascular)
- Hardware failure/pseudarthrosis (osteoporotic/irradiated bone, limited life expectancy), adjacent fracture
- CSF leak, wound complications (irradiated/immunocompromised field), infection
- Approach-specific (pleural, vascular, bowel)
Operative Note Template
Preoperative Diagnosis: [Metastatic/primary] tumor of [T_/L_] with epidural cord compression [ESCC __] and instability [SINS __]
Postoperative Diagnosis: Same
Procedure: [T_/L_] [posterolateral transpedicular] corpectomy with circumferential decompression and instrumented reconstruction (pedicle screws + expandable cage)
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids / Blood products: [crossmatched 2–4 units; cell saver] Adjuncts: Fluoroscopy/navigation, high-speed drill; SSEP/MEP/EMG; MAP > 85; preoperative embolization Implants: Pedicle screws/rods, expandable cage/PMMA, bone graft Complications: None
Indications: [Age]yo [M/F] with [a metastatic/primary] tumor at [T_/L_] causing epidural cord compression [and instability]. [Preoperative embolization was performed for the vascular tumor.] Separation surgery/decompression with stabilization was planned (adjuvant radiation to follow for mets). Risks (hemorrhage, neurological injury, hardware failure) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced (MAP > 85, crossmatched blood/cell saver) and neuromonitoring established. The patient was positioned prone and the levels confirmed. Pedicle screws were placed above and below for reconstruction. A laminectomy was performed and the cord/thecal sac protected.
Via a transpedicular/costotransversectomy corridor [with ligation of the involved thoracic nerve root], the pedicle(s) were removed and a corpectomy performed, achieving circumferential decompression by removing the posterior vertebral body and epidural tumor. An expandable cage [/PMMA-mesh] reconstructed the anterior column, rods were secured, and alignment confirmed on fluoroscopy. Hemostasis was obtained (embolization-assisted). Neuromonitoring remained stable.
A drain was placed and closure performed in layers. The patient was transferred to the ICU with MAP support and serial neuro/hemoglobin monitoring.
Postoperative Plan
- ICU, neuro checks q1h, MAP support, monitor blood loss/Hgb
- X-ray/CT postop (hardware, alignment), drain management
- DVT prophylaxis (balance bleeding/tumor), brace per surgeon
- Postoperative radiation (SRS/EBRT) for mets after wound healing (~2-3 weeks); oncology coordination
- Pathology; restage; rehab; goals-of-care for advanced disease
Chief-Level Case Review
Use these as the senior-level mental model for Vertebral Corpectomy and Reconstruction (Metastatic / Primary Vertebral Tumor):
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Vertebral Corpectomy and Reconstruction (Metastatic / Primary Vertebral Tumor):
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]