
Case Prep: Intradural Extramedullary Spinal Tumor Resection (Meningioma / Schwannoma)
Case / Approach Snapshot
- Anatomy at risk: cord, roots, dura, epidural venous plexus, tumor vascular supply, vertebral body/posterior element involvement, and stabilization corridors.
- Operative steps: define oncologic and neurologic goals, localize levels, decompress neural elements, obtain tissue or resect/debulk safely, reconstruct stability, and coordinate radiation/systemic therapy planning; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: major blood loss, neuromonitoring change, durotomy/CSF leak, pathologic instability, wound breakdown after radiation, residual disease strategy, and staged embolization or reconstruction.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [cervical/thoracic/lumbar] intradural extramedullary tumor ([meningioma / schwannoma / neurofibroma]) at [level] presenting with [pain / myelopathy / radiculopathy] planned for laminectomy/laminoplasty for microsurgical resection.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior thoracolumbar approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Surgical resection of an intradural extramedullary spinal tumor — Yunga Tigre J. Neurosurgical focus: Video 2023. PubMed
- Intradural Extramedullary Spinal Tumor Suspected Angiosarcoma Based on Clinical Course and Pathological Findings: A Case Report — Iijima Y. Spine surgery and related research 2022. PubMed
- Large primary Intradural extramedullary spinal tumors: A case report — Hadar AK. International journal of surgery case reports 2023. PubMed
- Primary Intradural Extramedullary Sporadic Spinal Hemangioblastomas: Case Report and Systematic Review — Li D. World neurosurgery 2021. PubMed
- Differentiation of the Intradural Extramedullary Spinal Tumors, Schwannomas, and Meningiomas Utilizing the Contrast Ratio as a Quantitative Magnetic Resonance Imaging Method — Nakamae T. World neurosurgery 2024. PubMed
- Intradural extramedullary tumor location in the axial view affects the alert timing of intraoperative neurophysiologic monitoring — Morito S. Journal of clinical monitoring and computing 2023. PubMed
- Extramedullary Intradural Primary Spinal Angiosarcoma: A Case Study — Catalo M. Cureus 2024. PubMed
- Hydrocephalus Secondary to Intradural Extramedullary Malignant Melanoma of Spinal Cord — Hironaka K. World neurosurgery 2019. PubMed
- Spinal intradural extramedullary cavernous hemangioma — Pétillon P. Neuroradiology 2018. PubMed
- Accuracy of intraoperative neurophysiological monitoring in predicting postoperative neurological decline in intradural extramedullary spinal tumor surgery: a systematic review and meta-analysis — Antkowiak L. Neurosurgical review 2025. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
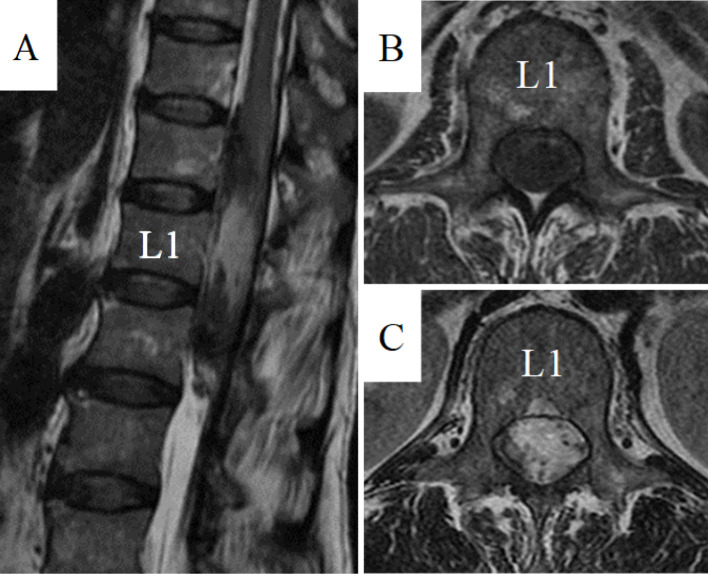 Figure 1.. Preoperative MRIs.Sagittal T2-weighted (A), axial T1-weighted (B), and axial T2-weighted (C) MRIs showing a poorly marginated mass with a T1-low and T2-mosaic pattern located… Source: Intradural Extramedullary Spinal Tumor Suspected Angiosarcoma Based on Clinical Course and Pathological Findings: A Case Report — Spine Surgery and Related Research 2022; CC BY-NC-ND.
Figure 1.. Preoperative MRIs.Sagittal T2-weighted (A), axial T1-weighted (B), and axial T2-weighted (C) MRIs showing a poorly marginated mass with a T1-low and T2-mosaic pattern located… Source: Intradural Extramedullary Spinal Tumor Suspected Angiosarcoma Based on Clinical Course and Pathological Findings: A Case Report — Spine Surgery and Related Research 2022; CC BY-NC-ND.
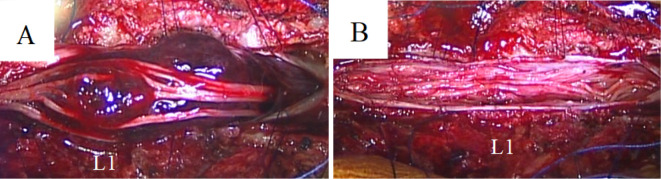 Figure 2.. Intraoperative microscopic views.Intraoperative photographs following laminectomy and durotomy at T12–L2 showing a dark red mass in the subarachnoid space (A). The mass was not connected… Source: Intradural Extramedullary Spinal Tumor Suspected Angiosarcoma Based on Clinical Course and Pathological Findings: A Case Report — Spine Surgery and Related Research 2022; CC BY-NC-ND.
Figure 2.. Intraoperative microscopic views.Intraoperative photographs following laminectomy and durotomy at T12–L2 showing a dark red mass in the subarachnoid space (A). The mass was not connected… Source: Intradural Extramedullary Spinal Tumor Suspected Angiosarcoma Based on Clinical Course and Pathological Findings: A Case Report — Spine Surgery and Related Research 2022; CC BY-NC-ND.
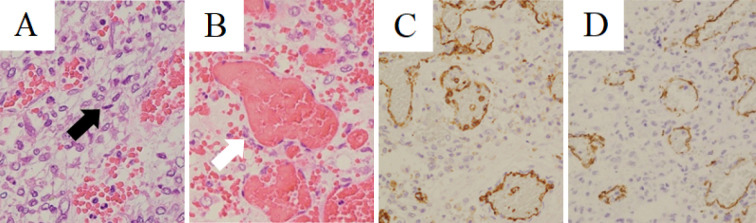 Figure 3.. Histological findings.Hematoxylin and eosin (H&E) staining ×400 (A, B). Cluster of differentiation (CD) 31 staining ×200 (C), and CD34 staining ×200 (D).H&E staining showing atypical… Source: Intradural Extramedullary Spinal Tumor Suspected Angiosarcoma Based on Clinical Course and Pathological Findings: A Case Report — Spine Surgery and Related Research 2022; CC BY-NC-ND.
Figure 3.. Histological findings.Hematoxylin and eosin (H&E) staining ×400 (A, B). Cluster of differentiation (CD) 31 staining ×200 (C), and CD34 staining ×200 (D).H&E staining showing atypical… Source: Intradural Extramedullary Spinal Tumor Suspected Angiosarcoma Based on Clinical Course and Pathological Findings: A Case Report — Spine Surgery and Related Research 2022; CC BY-NC-ND.
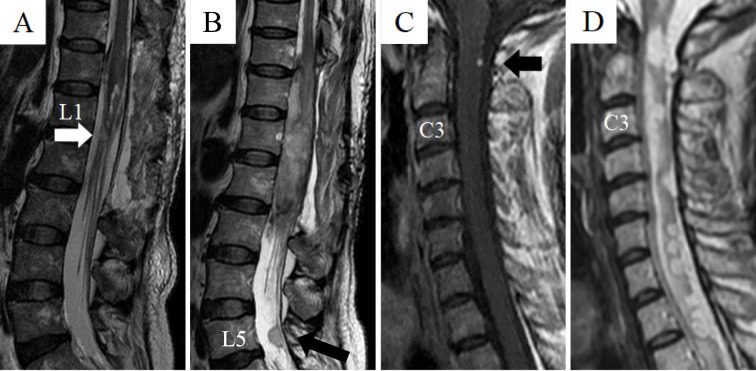 Figure 4.. Postoperative MRIs.Sagittal T2-weighted MRI (A) at 2 weeks after surgery showing the mass was mostly resected, but a small mass is seen below the conus medullaris (white arrow).Sagittal… Source: Intradural Extramedullary Spinal Tumor Suspected Angiosarcoma Based on Clinical Course and Pathological Findings: A Case Report — Spine Surgery and Related Research 2022; CC BY-NC-ND.
Figure 4.. Postoperative MRIs.Sagittal T2-weighted MRI (A) at 2 weeks after surgery showing the mass was mostly resected, but a small mass is seen below the conus medullaris (white arrow).Sagittal… Source: Intradural Extramedullary Spinal Tumor Suspected Angiosarcoma Based on Clinical Course and Pathological Findings: A Case Report — Spine Surgery and Related Research 2022; CC BY-NC-ND.
 Figure 1. Masses present all over the scalp, each averaging about 4×4 cm, with the largest one located in the occipital area of 6×7 cm in dimensions. Source: Rare case of multiple neurofibromas of the scalp and trunk in association with intradural extramedullary spinal tumor: a case report — Annals of Medicine and Surgery 2023; CC BY-NC-ND.
Figure 1. Masses present all over the scalp, each averaging about 4×4 cm, with the largest one located in the occipital area of 6×7 cm in dimensions. Source: Rare case of multiple neurofibromas of the scalp and trunk in association with intradural extramedullary spinal tumor: a case report — Annals of Medicine and Surgery 2023; CC BY-NC-ND.
 Figure 2. MRI of SPINE revealing T11–T12 neurofibroma. Source: Rare case of multiple neurofibromas of the scalp and trunk in association with intradural extramedullary spinal tumor: a case report — Annals of Medicine and Surgery 2023; CC BY-NC-ND.
Figure 2. MRI of SPINE revealing T11–T12 neurofibroma. Source: Rare case of multiple neurofibromas of the scalp and trunk in association with intradural extramedullary spinal tumor: a case report — Annals of Medicine and Surgery 2023; CC BY-NC-ND.
 Figure 3. Excised tumor by total excision from intraspinal region. Source: Rare case of multiple neurofibromas of the scalp and trunk in association with intradural extramedullary spinal tumor: a case report — Annals of Medicine and Surgery 2023; CC BY-NC-ND.
Figure 3. Excised tumor by total excision from intraspinal region. Source: Rare case of multiple neurofibromas of the scalp and trunk in association with intradural extramedullary spinal tumor: a case report — Annals of Medicine and Surgery 2023; CC BY-NC-ND.
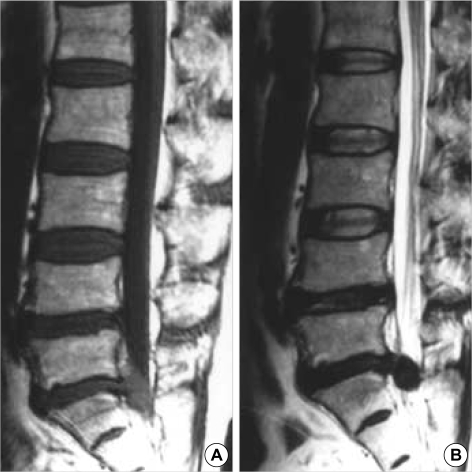 Fig. 1. T1-(A) and T2-weighted (B) sagittal magnetic resonance images demonstrating a mass-like lesion. Source: Intradural Disc Herniation at L5-S1 Mimicking an Intradural Extramedullary Spinal Tumor: A Case Report — Journal of Korean Medical Science 2006; CC BY-NC.
Fig. 1. T1-(A) and T2-weighted (B) sagittal magnetic resonance images demonstrating a mass-like lesion. Source: Intradural Disc Herniation at L5-S1 Mimicking an Intradural Extramedullary Spinal Tumor: A Case Report — Journal of Korean Medical Science 2006; CC BY-NC.
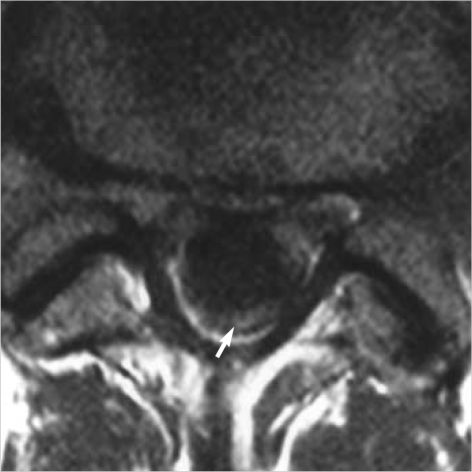 Fig. 2. Contrast-enhanced axial image showing peripheral enhancement of the lesion (arrow). Source: Intradural Disc Herniation at L5-S1 Mimicking an Intradural Extramedullary Spinal Tumor: A Case Report — Journal of Korean Medical Science 2006; CC BY-NC.
Fig. 2. Contrast-enhanced axial image showing peripheral enhancement of the lesion (arrow). Source: Intradural Disc Herniation at L5-S1 Mimicking an Intradural Extramedullary Spinal Tumor: A Case Report — Journal of Korean Medical Science 2006; CC BY-NC.
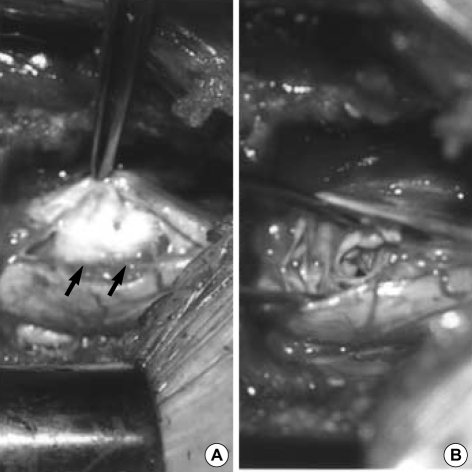 Fig. 3. Intraoperative photograph (A) outlining the peripheral displacement of the adherent cauda equine nerve roots (arrows) by the large intradural disc fragment. Intraoperative photograph (B)… Source: Intradural Disc Herniation at L5-S1 Mimicking an Intradural Extramedullary Spinal Tumor: A Case Report — Journal of Korean Medical Science 2006; CC BY-NC.
Fig. 3. Intraoperative photograph (A) outlining the peripheral displacement of the adherent cauda equine nerve roots (arrows) by the large intradural disc fragment. Intraoperative photograph (B)… Source: Intradural Disc Herniation at L5-S1 Mimicking an Intradural Extramedullary Spinal Tumor: A Case Report — Journal of Korean Medical Science 2006; CC BY-NC.
History of Present Illness
- Chief complaint: Nocturnal/positional back pain, progressive myelopathy (gait, weakness, sensory level), radiculopathy
- Duration/progression (usually slow); bowel/bladder
- Schwannoma: radicular onset (nerve root origin); Meningioma: thoracic, female, myelopathy; NF2 (multiple schwannomas/meningiomas), NF1 (neurofibromas)
Imaging Review
MRI (T1±Gad, T2) entire spine
- Intradural extramedullary location (displaces cord, CSF cap sign)
- Level, size, enhancement (meningioma: dural tail, broad dural base, may calcify; schwannoma: nerve root origin, dumbbell through foramen, cystic)
- Cord compression/signal change, dumbbell extension through neural foramen (schwannoma — may need combined/lateral approach)
- Multiple lesions (NF2)
CT
- Bony anatomy, calcification (meningioma), foraminal widening (dumbbell schwannoma), planning instrumentation if facet/stability compromised
Labs
- CBC, BMP, Coags, Type and screen
Neurological Examination
- Detailed motor/sensory (sensory level), reflexes, myelopathy signs, bowel/bladder, gait
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- OR setup: microscope, fluoroscopy/navigation, neuromonitoring, tumor debulking/microsurgical set, dural repair materials, instrumentation/corpectomy trays as indicated, and blood available.
- Special needs: arterial line/Foley for long cases, dexamethasone for cord edema when indicated, MAP support for myelopathy/cord manipulation, oncology/radiation plan, and pathology/frozen specimen workflow.
- Immediate postop orders: frequent motor/sensory exams, MAP support if cord manipulation or deficit, MRI/CT/X-rays per tumor/construct, steroid taper, drain/dural-leak precautions, brace/activity, DVT timing, and oncology/radiation follow-up.
Position
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- Prone (most), Mayfield (cervical/upper thoracic) or pinned/horseshoe; chest rolls, abdomen free, reverse Trendelenburg
- IONM baseline after positioning
Approach: Posterior Laminectomy / Laminoplasty (± facetectomy for dumbbell)
Key Surgical Steps
- Fluoroscopic level localization (count carefully — wrong-level is a never event; thoracic especially hard)
- Midline incision, subperiosteal exposure, laminectomy or laminoplasty over the tumor (laminoplasty in children/long-segment to preserve stability)
- Confirm with ultrasound (tumor localization, cord)
- Midline durotomy under microscope, dural tack-up sutures, preserve arachnoid then open
- Identify tumor and its relationship to cord/roots
- Schwannoma: identify the parent rootlet (often non-functional dorsal rootlet); internally debulk (CUSA), dissect capsule off cord/roots, sacrifice the involved rootlet if needed, deliver tumor; dumbbell: may need facetectomy + foraminal/lateral extension (± fusion)
- Meningioma: internal debulking, dissect from cord (arachnoid plane), coagulate and resect/coagulate dural base (Simpson — resect involved dura with duraplasty, or coagulate base [Simpson II] to lower CSF leak risk)
- Confirm cord decompression, hemostasis
- Watertight dural closure (± dural graft for meningioma base), sealant
- ± Instrumented fusion if facetectomy/laminectomy destabilized (esp. cervical, dumbbell, multilevel)
- Closure
Critical Anatomy & Structures at Risk
- Spinal cord — manipulation/retraction (myelopathy); dorsal midline entry only if needed
- Nerve roots — functional roots preserved; schwannoma parent root often sacrificable
- Radicular/segmental arteries (esp. thoracic — artery of Adamkiewicz, T8-L1 left) — cord infarction
- Dura — watertight closure (CSF leak/pseudomeningocele)
- Spinal stability (facetectomy)
Equipment
- Microscope, ultrasound, CUSA, microsurgical instruments, fine bipolar
- Dural substitute, sealant, fixation set (if fusion), hemostatic agents
Monitoring
- SSEPs, MEPs, EMG (essential — cord and roots), D-wave for intramedullary-adjacent
Anesthesia
- MAP > 85 (cord perfusion), no paralytic (IONM), arterial line, prone precautions, type and screen
Potential Complications
- Neurological worsening (cord/root manipulation, vascular)
- CSF leak/pseudomeningocele (dural closure)
- Spinal instability/deformity (post-laminectomy, esp. cervical/pediatric)
- Recurrence (meningioma — base management), infection
Operative Note Template
Preoperative Diagnosis: [Cervical/thoracic/lumbar] intradural extramedullary tumor ([meningioma/schwannoma]) at [level]
Postoperative Diagnosis: Same (pending pathology)
Procedure: [Level] laminectomy/laminoplasty for microsurgical resection of intradural extramedullary tumor [with instrumented fusion]
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Microscope, ultrasound, CUSA, fluoroscopy; SSEP/MEP/EMG; MAP support Implants: Dural substitute, sealant; [fusion hardware if facetectomy] Complications: None
Indications: [Age]yo [M/F] with a symptomatic intradural extramedullary tumor at [level] causing [myelopathy/radiculopathy/pain]. Risks (neurological worsening, CSF leak, instability) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced (MAP support) and neuromonitoring established. The patient was positioned prone [in Mayfield for cervical/upper-thoracic]; the level was confirmed fluoroscopically. A laminectomy/laminoplasty was performed over the tumor and ultrasound confirmed localization. A midline durotomy was made under the microscope and tacked up.
The tumor was identified relative to the cord and roots. [Schwannoma: the non-functional parent rootlet was identified by stimulation, the tumor internally debulked and dissected off the cord/roots, and the involved rootlet sacrificed.] [Meningioma: the tumor was internally debulked and dissected off the cord in the arachnoid plane, and the dural base resected/coagulated (Simpson) with duraplasty.] Radicular/segmental arteries were preserved. A watertight dural closure was performed with sealant. [Instrumented fusion was added for facetectomy-related instability.]
Closure was completed in layers. The patient was transferred with MAP support and CSF-leak precautions, neurologically [at baseline].
Postoperative Plan
- ICU/step-down, neuro checks q1-2h (motor/sensory)
- CSF leak precautions (flat if durotomy concern), MAP support
- MRI postop (resection), watch pseudomeningocele
- DVT prophylaxis (mechanical; chemical delayed), pain control
- Pathology (WHO grade meningioma); follow-up MRI; PT/rehab
Chief-Level Case Review
Use these as the senior-level mental model for Intradural Extramedullary Spinal Tumor Resection (Meningioma / Schwannoma):
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Intradural Extramedullary Spinal Tumor Resection (Meningioma / Schwannoma):
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]