
Case Prep: Spinal Dural Arteriovenous Fistula (dAVF) — Surgical Ligation
Case / Approach Snapshot
- Anatomy at risk: cord, roots, dura, posterior elements, segmental and radiculomedullary arteries, venous plexus, and level-specific bony landmarks.
- Operative steps: localize the level, expose while preserving stability, obtain proximal/distal vascular control when relevant, decompress or disconnect/reconstruct the lesion, confirm flow/decompression, and close with CSF-leak prevention; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: neuromonitoring change, bleeding from epidural/foraminal vessels, durotomy, wrong-level exposure, cord swelling/ischemia, instability, and staged/endovascular adjuncts.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [thoracic/lumbar] spinal dural arteriovenous fistula (Type I) at [level] presenting with progressive myelopathy / gait decline / bowel-bladder dysfunction planned for [level] laminectomy for microsurgical disconnection of the fistula [or note endovascular embolization].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior thoracolumbar approach — posterior exposure, durotomy, fistula localization, and closure principles.
Neurosurgical Atlas · neuroangio.org · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Surgical ligation of spinal dural arteriovenous fistula — Sorenson T. Acta neurochirurgica 2018. PubMed
- Craniocervivcal Spinal Dural Arteriovenous Fistula Ligation via a Modified Suboccipital Craniectomy and C1 Laminectomy: Operative Video — Young M. World neurosurgery 2023. PubMed
- Microsurgical Ligation of a Dural Arteriovenous Fistula of the Petrous Apex-A 2-Dimensional Operative Video — Aldea S. World neurosurgery 2022. PubMed
- Spinal dural arteriovenous fistulas presenting as intracranial subarachnoid hemorrhage: A systematic review — Nolan B. Interventional neuroradiology : journal of peritherapeutic neuroradiology, surgical procedures and related neurosciences 2025. PubMed
- Microsurgery of Spinal Dural Arteriovenous Fistula Using Indocyanine Green Video Angiography: 2-Dimensional Operative Video — Yokoyama K. Operative neurosurgery (Hagerstown, Md.) 2019. PubMed
- Open surgical ligation of a thoracic spinal epidural arteriovenous fistula causing thoracic myelopathy: illustrative case — Laing BRW. Journal of neurosurgery. Case lessons 2023. PubMed
- Spinal dural arteriovenous fistula: a case series and review of imaging findings — Fox S. Spinal cord series and cases 2017. PubMed
- Spinal dural arteriovenous fistula formation after scoliosis surgery: case report — Elswick CM. Journal of neurosurgery. Spine 2020. PubMed
- Minimally invasive intradural spinal dural arteriovenous fistula ligation — Patel NP. World neurosurgery 2013. PubMed
- Ruptured spinal dural arteriovenous fistula with subdural hematoma: A case report — Williamson LE. Surgical neurology international 2025. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
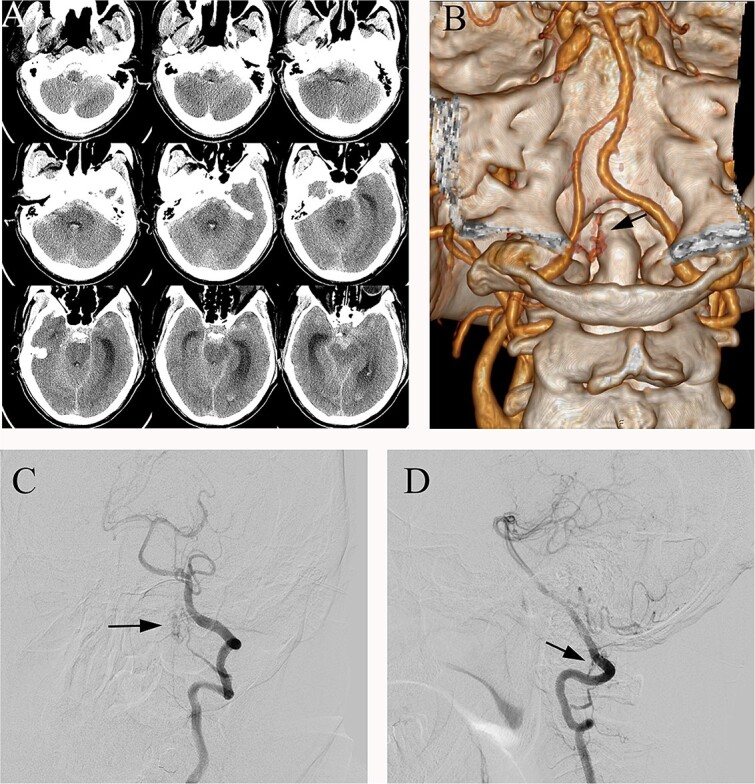 Figure 1. (A) Preoperative head CT, (B) CTA and (C, D) DSA identified the fistula (arrows) in the left lateral dural membrane and confirmed the intradural origin of the drainage vein. Source: Microsurgical treatment of spinal dural arteriovenous fistula with subarachnoid hemorrhage: a case report — Journal of Surgical Case Reports 2025; CC BY-NC.
Figure 1. (A) Preoperative head CT, (B) CTA and (C, D) DSA identified the fistula (arrows) in the left lateral dural membrane and confirmed the intradural origin of the drainage vein. Source: Microsurgical treatment of spinal dural arteriovenous fistula with subarachnoid hemorrhage: a case report — Journal of Surgical Case Reports 2025; CC BY-NC.
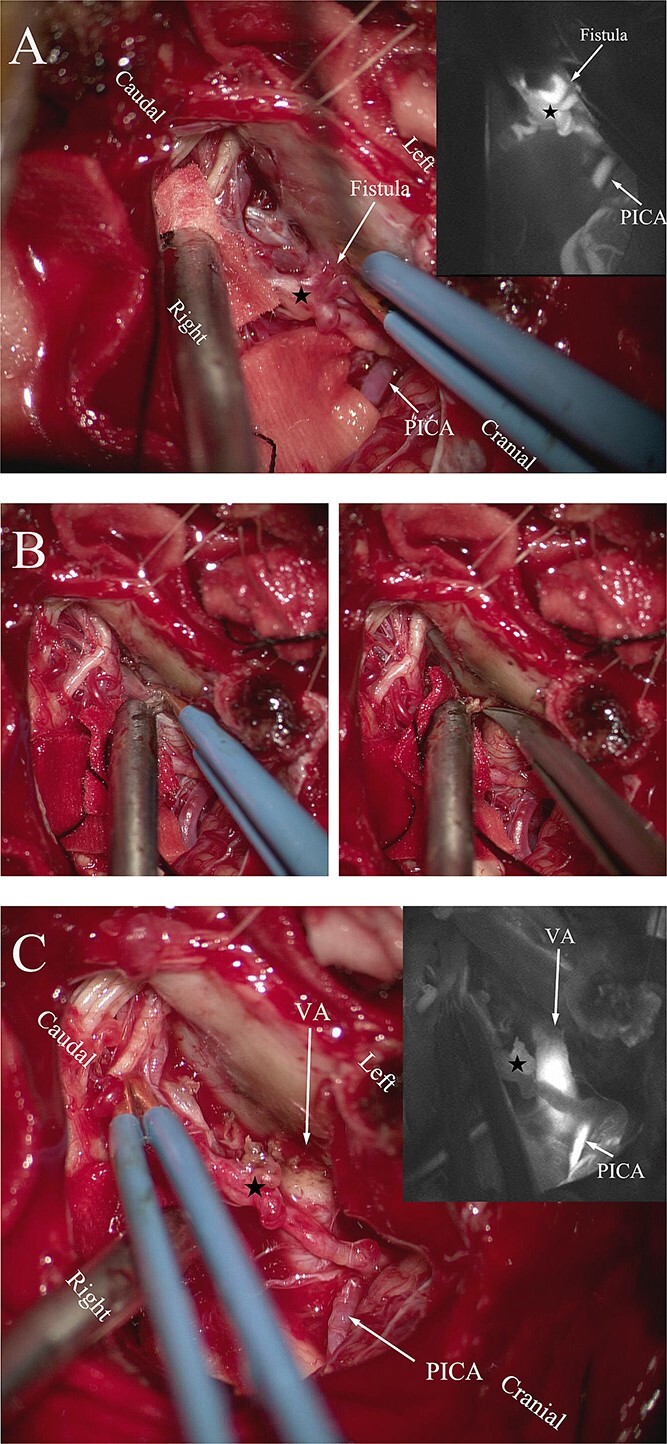 Figure 2. (A) Intraoperative ICG fluorescence imaging demonstrated that the fistula and abnormal drainage vein (asterisk) developed earlier than the posterior inferior cerebellar artery (PICA)…. Source: Microsurgical treatment of spinal dural arteriovenous fistula with subarachnoid hemorrhage: a case report — Journal of Surgical Case Reports 2025; CC BY-NC.
Figure 2. (A) Intraoperative ICG fluorescence imaging demonstrated that the fistula and abnormal drainage vein (asterisk) developed earlier than the posterior inferior cerebellar artery (PICA)…. Source: Microsurgical treatment of spinal dural arteriovenous fistula with subarachnoid hemorrhage: a case report — Journal of Surgical Case Reports 2025; CC BY-NC.
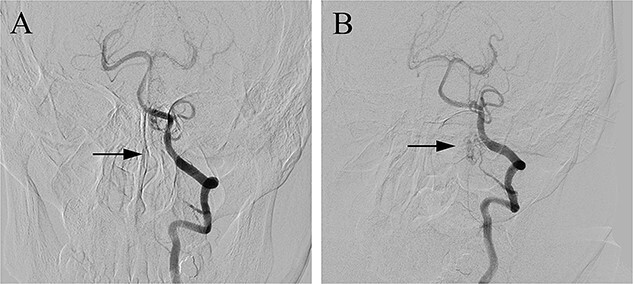 Figure 3. Postoperative DSA (A) confirmed the complete occlusion of the fistula (arrow) when compared with the preoperative DSA (B). Source: Microsurgical treatment of spinal dural arteriovenous fistula with subarachnoid hemorrhage: a case report — Journal of Surgical Case Reports 2025; CC BY-NC.
Figure 3. Postoperative DSA (A) confirmed the complete occlusion of the fistula (arrow) when compared with the preoperative DSA (B). Source: Microsurgical treatment of spinal dural arteriovenous fistula with subarachnoid hemorrhage: a case report — Journal of Surgical Case Reports 2025; CC BY-NC.
 Figure 1. (a) Preoperative T2 magnetic resonance imaging (MRI) of patient 1 showing the serpiginous veins surrounding the thoracic spinal cord most prominent at T7/8 level (arrowed), secondary to… Source: Minimal access microsurgical ligation of spinal dural arteriovenous fistula with tubular retractor — Surgical Neurology International 2015; CC BY-NC-SA.
Figure 1. (a) Preoperative T2 magnetic resonance imaging (MRI) of patient 1 showing the serpiginous veins surrounding the thoracic spinal cord most prominent at T7/8 level (arrowed), secondary to… Source: Minimal access microsurgical ligation of spinal dural arteriovenous fistula with tubular retractor — Surgical Neurology International 2015; CC BY-NC-SA.
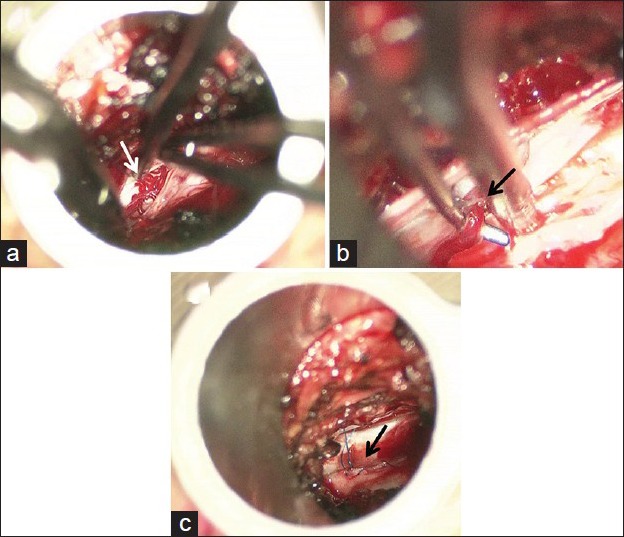 Figure 2. (a) Operative view through the tubular retractor under a surgical microscope, showing dilated serpiginous veins (arrowed) after opening the dura. (b) Dissection of the fistulous point of… Source: Minimal access microsurgical ligation of spinal dural arteriovenous fistula with tubular retractor — Surgical Neurology International 2015; CC BY-NC-SA.
Figure 2. (a) Operative view through the tubular retractor under a surgical microscope, showing dilated serpiginous veins (arrowed) after opening the dura. (b) Dissection of the fistulous point of… Source: Minimal access microsurgical ligation of spinal dural arteriovenous fistula with tubular retractor — Surgical Neurology International 2015; CC BY-NC-SA.
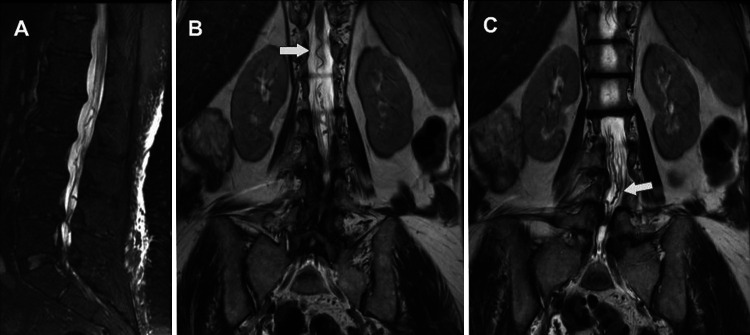 FIG. 1. Sagittal (A) and coronal (B and C) T2-weighted MRI showing abnormal serpentine vasculature at the level of the lumbar cistern (white arrows). Source: Microsurgical intraluminal obliteration of type IV perimedullary arteriovenous fistula with an in situ hemostatic agent: illustrative case — Journal of Neurosurgery: Case Lessons 2023; CC BY-NC-ND.
FIG. 1. Sagittal (A) and coronal (B and C) T2-weighted MRI showing abnormal serpentine vasculature at the level of the lumbar cistern (white arrows). Source: Microsurgical intraluminal obliteration of type IV perimedullary arteriovenous fistula with an in situ hemostatic agent: illustrative case — Journal of Neurosurgery: Case Lessons 2023; CC BY-NC-ND.
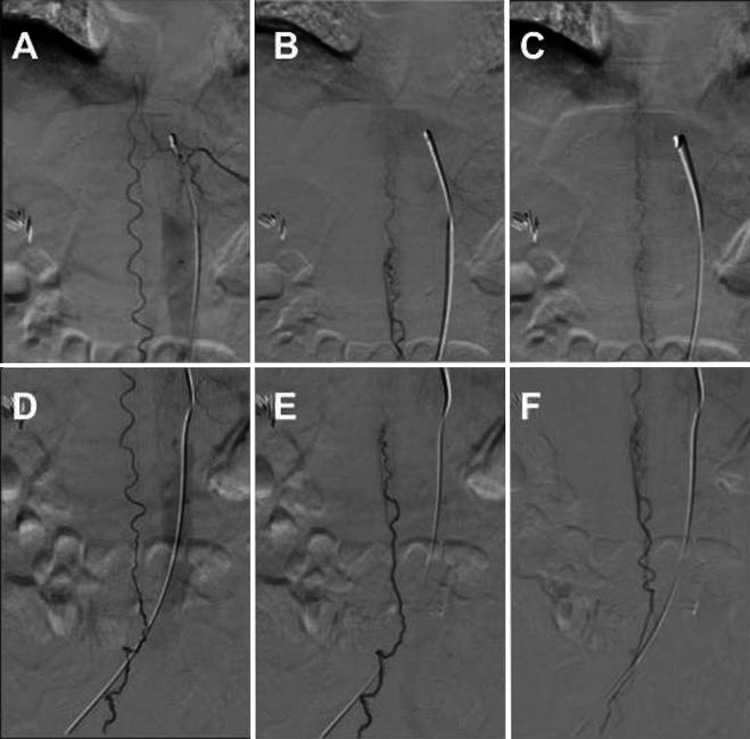 FIG. 2. Diagnostic angiography showing a type IV perimedullary arteriovenous fistula of the distal anterior spinal artery of Adamkiewicz. The flow traveled sequentially from the artery of… Source: Microsurgical intraluminal obliteration of type IV perimedullary arteriovenous fistula with an in situ hemostatic agent: illustrative case — Journal of Neurosurgery: Case Lessons 2023; CC BY-NC-ND.
FIG. 2. Diagnostic angiography showing a type IV perimedullary arteriovenous fistula of the distal anterior spinal artery of Adamkiewicz. The flow traveled sequentially from the artery of… Source: Microsurgical intraluminal obliteration of type IV perimedullary arteriovenous fistula with an in situ hemostatic agent: illustrative case — Journal of Neurosurgery: Case Lessons 2023; CC BY-NC-ND.
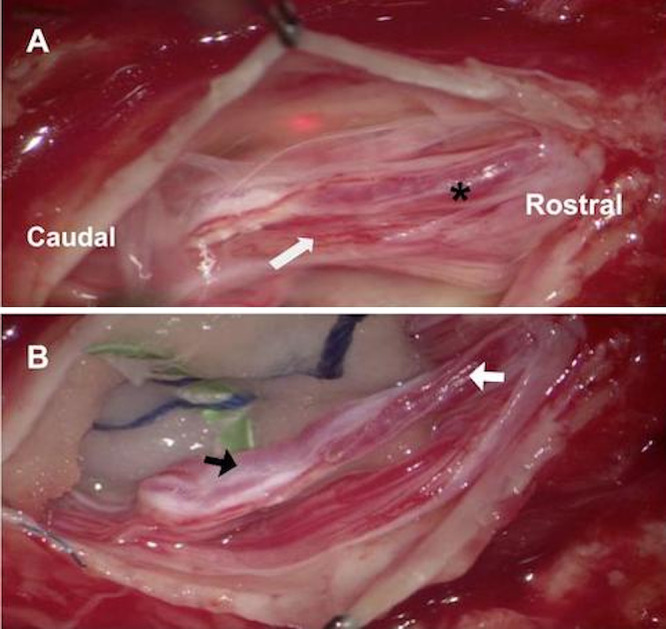 FIG. 3. A: White arrow indicates nerve roots tightly attached to the fistulous vessel (asterisk). B: Black arrow indicates an arterialized vessel with caudal flow. White arrow indicates an… Source: Microsurgical intraluminal obliteration of type IV perimedullary arteriovenous fistula with an in situ hemostatic agent: illustrative case — Journal of Neurosurgery: Case Lessons 2023; CC BY-NC-ND.
FIG. 3. A: White arrow indicates nerve roots tightly attached to the fistulous vessel (asterisk). B: Black arrow indicates an arterialized vessel with caudal flow. White arrow indicates an… Source: Microsurgical intraluminal obliteration of type IV perimedullary arteriovenous fistula with an in situ hemostatic agent: illustrative case — Journal of Neurosurgery: Case Lessons 2023; CC BY-NC-ND.
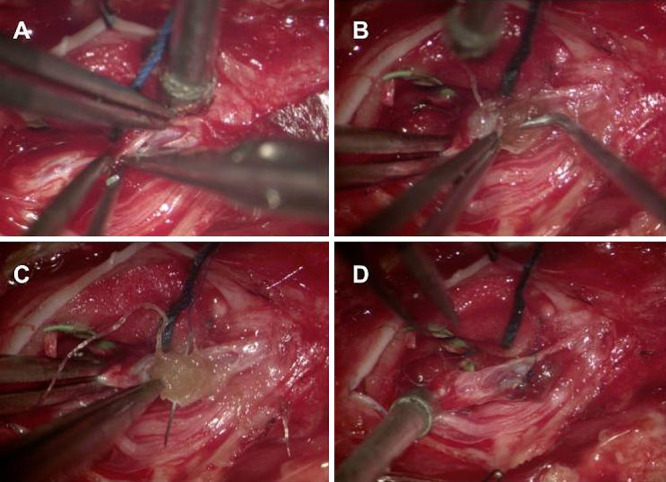 FIG. 4. Vessel obliteration. A: The assistant uses forceps for proximal and distal control during arteriotomy. B: Packing with the hemostatic agent in the lumen of the artery. C: Securing the… Source: Microsurgical intraluminal obliteration of type IV perimedullary arteriovenous fistula with an in situ hemostatic agent: illustrative case — Journal of Neurosurgery: Case Lessons 2023; CC BY-NC-ND.
FIG. 4. Vessel obliteration. A: The assistant uses forceps for proximal and distal control during arteriotomy. B: Packing with the hemostatic agent in the lumen of the artery. C: Securing the… Source: Microsurgical intraluminal obliteration of type IV perimedullary arteriovenous fistula with an in situ hemostatic agent: illustrative case — Journal of Neurosurgery: Case Lessons 2023; CC BY-NC-ND.
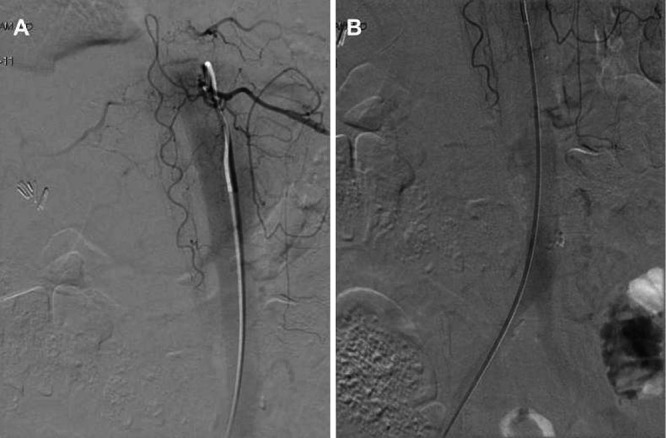 FIG. 5. A and B: Postoperative angiography shows the resolution and obliteration of type IV perimedullary arteriovenous fistula. Source: Microsurgical intraluminal obliteration of type IV perimedullary arteriovenous fistula with an in situ hemostatic agent: illustrative case — Journal of Neurosurgery: Case Lessons 2023; CC BY-NC-ND.
FIG. 5. A and B: Postoperative angiography shows the resolution and obliteration of type IV perimedullary arteriovenous fistula. Source: Microsurgical intraluminal obliteration of type IV perimedullary arteriovenous fistula with an in situ hemostatic agent: illustrative case — Journal of Neurosurgery: Case Lessons 2023; CC BY-NC-ND.
History of Present Illness
- Chief complaint: Progressive ascending myelopathy — gait difficulty, lower extremity weakness/numbness, bowel/bladder dysfunction, erectile dysfunction
- Classic: older male, insidious, stepwise/progressive, worse with activity/standing (venous congestion) — Foix-Alajouanine syndrome (subacute necrotic myelopathy) if advanced/untreated
- Often misdiagnosed/delayed (mimics degenerative myelopathy, demyelination, tumor)
- Symptom duration (longer/more severe = less reversible)
Past Medical History
- Prior spinal imaging/misdiagnoses, prior intervention
- Anticoagulant/antiplatelet
- Standard PMH
Imaging Review
MRI Spine (T2, T1±Gad)
- Cord T2 hyperintensity (central, longitudinally extensive — venous congestion/edema), cord expansion
- Flow voids (dilated perimedullary veins) on dorsal cord surface (T2) — hallmark
- Enhancement of cord (chronic venous hypertension)
Spinal DSA (gold standard)
- Identify the fistula level and feeding radicular artery (dural branch of a segmental/radicular artery feeds an intradural radicular vein at the nerve root sleeve)
- Map the arterial feeder, the draining vein, exclude additional fistulas
- Critically identify the artery of Adamkiewicz and spinal cord arterial supply (must NOT be the feeder being sacrificed)
- Differentiate Type I dAVF from intramedullary AVM (perimedullary fistula, glomus AVM)
Labs
- CBC, BMP, Coags, type and screen
Neurological Examination
- Detailed motor/sensory (sensory level), reflexes, gait, bowel/bladder, sphincter tone — document baseline (recovery depends on pre-op severity/duration)
- Aminoff-Logue scale (gait/micturition disability)
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: radiolucent spine-capable table selected for approach, imaging, instrumentation, patient size, and alignment goals; keep abdomen free for prone cases.
- OR setup: microscope, neuromonitoring, spinal angiography/DSA images loaded, ICG/Doppler, clips/coagulation tools, laminectomy/instrumentation backup, and blood available for vascular lesions.
- Special needs: arterial line, Foley, MAP support for cord perfusion, no long paralytic with MEPs, CSF drainage plan only when indicated, and coordination with endovascular/staged treatment.
- Immediate postop orders: ICU neuro checks with motor/sensory/sphincter focus, MAP target, MRI/angiography confirmation plan, drain/hematoma watch, steroid/pain regimen, DVT timing, and rehab planning.
Diagnosis & Indication
- Working diagnosis: Spinal dural AVF (Type I), the most common spinal vascular malformation
- Indication: Symptomatic dAVF — disconnect to halt/reverse venous congestion (early treatment → better recovery)
- Treatment options: Microsurgical disconnection (durable, high cure rate) vs endovascular embolization (Onyx/glue — less durable if feeder also supplies cord; surgery preferred if embolization risky or fails)
Position
- OR table/bed: radiolucent spine-capable table selected for approach, imaging, instrumentation, patient size, and alignment goals; keep abdomen free for prone cases.
- Prone, Mayfield/foam, chest rolls, abdomen free, reverse Trendelenburg; IONM baseline
- Level localization (fluoroscopy) — fistula level confirmed from DSA
Approach: Laminectomy / Hemilaminectomy at the Fistula Level
Key Surgical Steps
- Fluoroscopic localization of the exact fistula level (from DSA — the radicular feeder enters at a specific nerve root sleeve)
- Midline incision, laminectomy (or hemilaminectomy) at the fistula level (± adjacent)
- Open dura in the midline, tack up; identify the arterialized (red), tortuous draining vein on the dorsal cord surface at the nerve root sleeve (arterialized vein is the giveaway — should be blue, but is red/engorged)
- Trace the fistula to the intradural draining vein at the dural root sleeve where the dural feeder connects
- Temporary clip the draining vein → confirm with ICG/inspection that the arterialized vein darkens (deflates/becomes blue) — confirms correct fistula and that this is the draining vein, not a normal cord vein
- Coagulate and divide the intradural draining vein at the point it exits the dura (the fistulous connection) — definitive disconnection
- Confirm with ICG videoangiography — no further early venous filling
- Watertight dural closure, sealant, closure
Critical Anatomy & Structures at Risk
- Anterior spinal artery / artery of Adamkiewicz — must NOT be sacrificed (would cause cord infarction); DSA confirms feeder is dural, not the radiculomedullary artery
- Normal cord draining veins — disconnect only the fistulous vein (temporary clip test confirms)
- Spinal cord (already congested/fragile), nerve roots
- Dura (CSF leak)
Equipment
- Microscope, ICG videoangiography, micro-instruments, temporary aneurysm clips, fine bipolar
- Fluoroscopy (localization), dural substitute, sealant
- Intraoperative DSA capability (selected)
Monitoring
- SSEPs, MEPs
Anesthesia
- MAP support (cord perfusion), arterial line, prone precautions, no paralytic (IONM)
Potential Complications
- Failure to disconnect / wrong vein / recurrence (incomplete or wrong level — DSA correlation and ICG/temporary clip test prevent)
- Cord infarction (if a radiculomedullary artery mistaken for the dural feeder)
- CSF leak, worsened myelopathy, no improvement (advanced/chronic disease)
- Persistent venous hypertension if additional fistula missed
Operative Note Template
Preoperative Diagnosis: Spinal dural arteriovenous fistula (Type I) at [level] Procedure: [Level] laminectomy and microsurgical disconnection of spinal dural AV fistula
Surgeon / Assistant: Anesthesia: General endotracheal, no paralytic EBL / Fluids: Adjuncts: Microscope, ICG videoangiography, temporary aneurysm clips, fluoroscopy; SSEP/MEP; MAP support Implants: Dural substitute, sealant Complications: None
Indications: [Age]yo [M/F] with a spinal dural AV fistula (Type I) at [level] (DSA-confirmed) presenting with progressive congestive myelopathy. Microsurgical disconnection was chosen [over/after embolization]. Risks (cord infarction, no improvement if advanced) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced (MAP support, no paralytic) and neuromonitoring established. The patient was positioned prone and the exact fistula level confirmed fluoroscopically per the DSA. A laminectomy/hemilaminectomy was performed at the fistula level and a midline durotomy made under the microscope.
The arterialized (red), tortuous draining vein was identified on the dorsal cord surface at the dural nerve-root sleeve. A temporary clip was applied to the draining vein and the arterialized vein confirmed to darken/deflate (verifying the correct fistulous vein, not a normal cord vein). The intradural draining vein was then coagulated and divided at its dural exit, disconnecting the fistula. ICG videoangiography confirmed obliteration with no early venous filling. A watertight dural closure was performed with sealant.
Closure was completed in layers. The patient was transferred with MAP support and CSF-leak precautions; gradual recovery of myelopathy over months was anticipated.
Postoperative Plan
- ICU/step-down, neuro checks (motor/sensory/sphincter), MAP support, CSF leak precautions
- MRI (resolution of cord edema over weeks-months), postop DSA to confirm obliteration
- DVT prophylaxis (mechanical), bowel/bladder management, urology if needed
- Rehab — gait/strength recovery is gradual and depends on pre-op severity; counsel realistic expectations
- Follow-up imaging; monitor for recurrence (recurrent symptoms → repeat DSA)
Chief-Level Case Review
Use these as the senior-level mental model for Spinal Dural Arteriovenous Fistula (dAVF) — Surgical Ligation:
- Decision point: The operation is won or lost on control: identify inflow, outflow, perforators, collateral options, and the fastest route to temporary control before exposing the lesion itself.
- Technical lever: Do not accept a cosmetic result over physiology: ICG/Doppler/DSA, branch patency, perforator preservation, and parent-vessel caliber matter more than how the clip or resection bed looks.
- Bailout: Have a rupture or ischemia script ready: lower pressure, suction strategy, temporary occlusion time, heparin/reversal plan, bypass/reconstruction threshold, and postop BP targets.
- Postop watch: Postop danger is delayed: vasospasm, thromboembolism, hyperperfusion, hemorrhage, edema, hydrocephalus, and seizure plans need explicit orders.
Common Pimp Questions
Use these to pressure-test preparation for Spinal Dural Arteriovenous Fistula (dAVF) — Surgical Ligation:
- What is the proximal-control plan before the lesion is manipulated?
- Which branch, perforator, or venous structure is most likely to be injured in this exposure?
- What are the intraoperative rupture steps, including temporary clip, suction, BP, and backup clip strategy?
- What confirms treatment success: ICG, Doppler, puncture/deflation, DSA, or postoperative CTA?
- What postoperative BP, vasospasm, antiplatelet, or anticoagulation issue changes the orders tonight?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Preferred approach side, sylvian split style, and cisternal-opening sequence: [attending-specific]
- Temporary clip threshold, burst-suppression preference, and BP during occlusion: [attending-specific]
- Clip manufacturer/shape sequence and whether Doppler, ICG, puncture, or intraop DSA is routine: [attending-specific]
- Antiplatelet/anticoagulation reversal and restart timing: [attending-specific]