
Case Prep: Sacral Fracture / Spinopelvic (Lumbopelvic) Fixation
Case / Approach Snapshot
- Anatomy at risk: unstable columns, cord/roots, dura, vertebral artery or great-vessel/visceral structures by level, fracture lines, and fixation corridors.
- Operative steps: protect the spine during transfer/positioning, confirm levels and reduction goals, decompress when indicated, instrument/reconstruct stability, verify alignment and hardware, and plan ICU/brace/rehab needs; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: neurologic deterioration, reduction failure, vascular/visceral injury, durotomy, blood loss, hardware pullout, infection, and staged anterior/posterior stabilization.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [Denis zone / U-type spinopelvic dissociation] sacral fracture following [high-energy fall/MVC] [± cauda equina/sacral nerve deficit] planned for [lumbopelvic (spinopelvic) fixation / iliosacral screw fixation / sacral decompression].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior thoracolumbar approach — posterior midline/paramedian exposure, lumbopelvic fixation, and closure principles.
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Spondylopelvic dissociation — Sullivan MP. The Orthopedic clinics of North America 2014. PubMed
- Traditional versus Minimally Invasive Spinopelvic Fixation for Sacral Fracture Treatment in Vertically Unstable Pelvic Fractures — Tsai YT. Journal of personalized medicine 2022. PubMed
- Percutaneous lumbopelvic fixation for pathologic sacral fractures and spinopelvic dissociation: patient series — Baksh N. Journal of neurosurgery. Case lessons 2023. PubMed
- Traumatic spinopelvic dissociation or U-shaped sacral fracture: a review of the literature — Yi C. Injury 2012. PubMed
- Minimally Invasive Spinopelvic Fixation for Unstable Bilateral Sacral Fractures — Koshimune K. Clinical spine surgery 2016. PubMed
- Spinopelvic fixation for vertically unstable AO type C pelvic fractures and sacral fractures with spinopelvic dissociation- A systematic review and pooled analysis involving 479 patients — Patel S. Journal of orthopaedics 2022. PubMed
- Robotic-Assisted Minimally Invasive Spinopelvic Fixation for Traumatic Sacral Fractures: Case Series Investigating Early Safety and Efficacy — Hardigan AA. World neurosurgery 2023. PubMed
- Lumbopelvic Fixation for Sacral Insufficiency Fracture Presenting with Sphincter Dysfunction — Maki S. Case reports in orthopedics 2019. PubMed
- Treatment of Unstable Sacral Fracture with Minimally Invasive Spinopelvic Posterior Fixation and an Internal Anterior Fixator in a 95-Year-Old Patient with Diffuse Idiopathic Skeletal Hyperostosis: A Case Report — Sasagawa T. Journal of orthopaedic case reports 2021. PubMed
- A Case of U-shaped Sacral Fracture After Longstanding Spinopelvic Fixation Treated With Percutaneous Sacroiliac Joint Fusion and Iliosacral Osteosynthesis — Ganeshan V. Cureus 2023. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
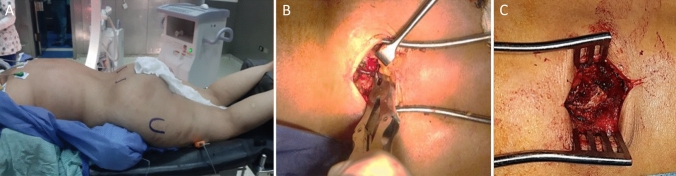 Fig. 1. A Prone position on radiolucent table, marking of PSIS and greater trochanter on each side. B PSIS exposure: starting point located caudal and medial to PSIS (Anatomic entry point). C… Source: Does minimally invasive percutaneous transilial internal fixator became an effective option for sacral fractures? A prospective study with novel implantation technique — European Journal of Trauma and Emergency Surgery 2023; CC BY.
Fig. 1. A Prone position on radiolucent table, marking of PSIS and greater trochanter on each side. B PSIS exposure: starting point located caudal and medial to PSIS (Anatomic entry point). C… Source: Does minimally invasive percutaneous transilial internal fixator became an effective option for sacral fractures? A prospective study with novel implantation technique — European Journal of Trauma and Emergency Surgery 2023; CC BY.
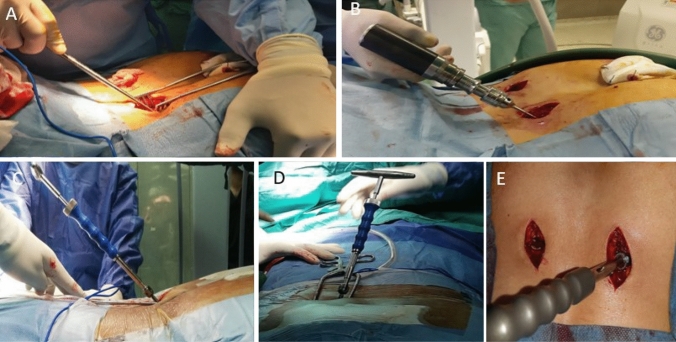 Fig. 2. A Awl used for penetration and creating screw tunnel. B Alternatively, oscillating drill could be used instead. C, D direction of awl in ventral and caudal direction. E Pedicular screw… Source: Does minimally invasive percutaneous transilial internal fixator became an effective option for sacral fractures? A prospective study with novel implantation technique — European Journal of Trauma and Emergency Surgery 2023; CC BY.
Fig. 2. A Awl used for penetration and creating screw tunnel. B Alternatively, oscillating drill could be used instead. C, D direction of awl in ventral and caudal direction. E Pedicular screw… Source: Does minimally invasive percutaneous transilial internal fixator became an effective option for sacral fractures? A prospective study with novel implantation technique — European Journal of Trauma and Emergency Surgery 2023; CC BY.
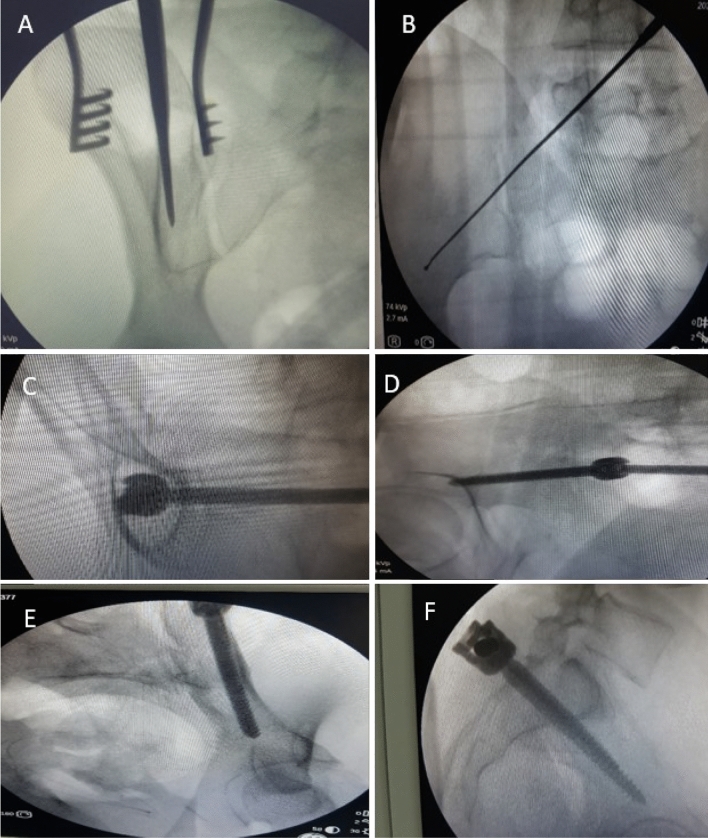 Fig. 3. A Showing Obturator view with awl insertion between the 2 tables. B Screw placement above sciatic notch in iliac view. C Tear drop view, D Iliac outlet view. E Obturator inlet. F True… Source: Does minimally invasive percutaneous transilial internal fixator became an effective option for sacral fractures? A prospective study with novel implantation technique — European Journal of Trauma and Emergency Surgery 2023; CC BY.
Fig. 3. A Showing Obturator view with awl insertion between the 2 tables. B Screw placement above sciatic notch in iliac view. C Tear drop view, D Iliac outlet view. E Obturator inlet. F True… Source: Does minimally invasive percutaneous transilial internal fixator became an effective option for sacral fractures? A prospective study with novel implantation technique — European Journal of Trauma and Emergency Surgery 2023; CC BY.
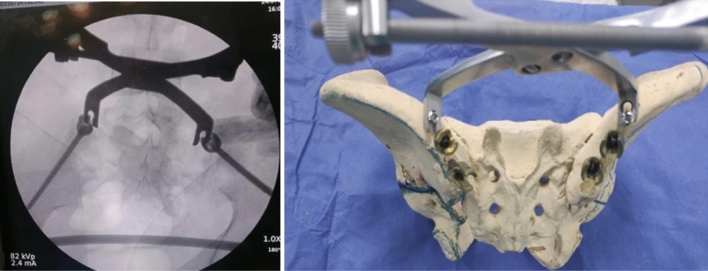 Fig. 4. Fracture reduction methods using pelvic reduction clamps applied over 4.5 cortical screws Source: Does minimally invasive percutaneous transilial internal fixator became an effective option for sacral fractures? A prospective study with novel implantation technique — European Journal of Trauma and Emergency Surgery 2023; CC BY.
Fig. 4. Fracture reduction methods using pelvic reduction clamps applied over 4.5 cortical screws Source: Does minimally invasive percutaneous transilial internal fixator became an effective option for sacral fractures? A prospective study with novel implantation technique — European Journal of Trauma and Emergency Surgery 2023; CC BY.
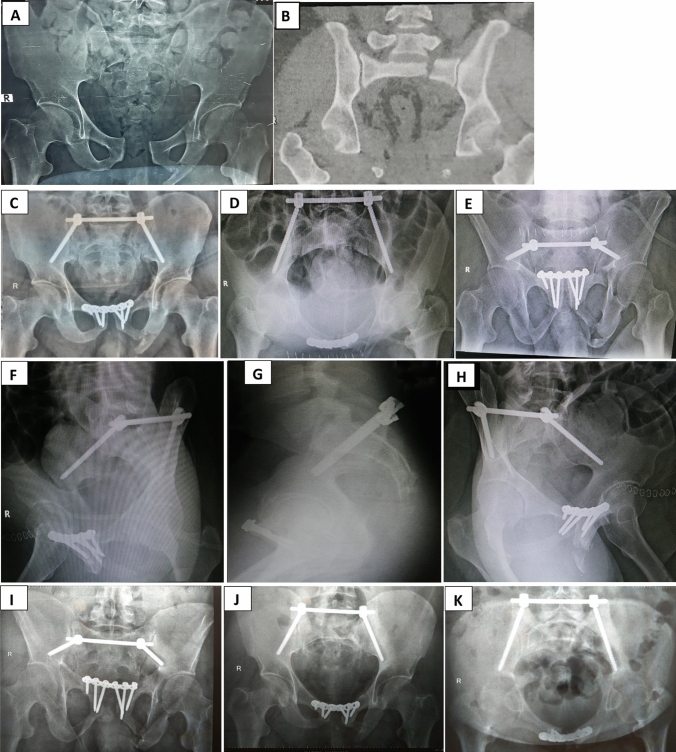 Fig. 5. A Preoperative radiograph showing left fracture sacrum Denis type 2 in 40 years old male. B–H Postoperative radiographic views showing iliac screws accurate trajectory. I–K Final… Source: Does minimally invasive percutaneous transilial internal fixator became an effective option for sacral fractures? A prospective study with novel implantation technique — European Journal of Trauma and Emergency Surgery 2023; CC BY.
Fig. 5. A Preoperative radiograph showing left fracture sacrum Denis type 2 in 40 years old male. B–H Postoperative radiographic views showing iliac screws accurate trajectory. I–K Final… Source: Does minimally invasive percutaneous transilial internal fixator became an effective option for sacral fractures? A prospective study with novel implantation technique — European Journal of Trauma and Emergency Surgery 2023; CC BY.
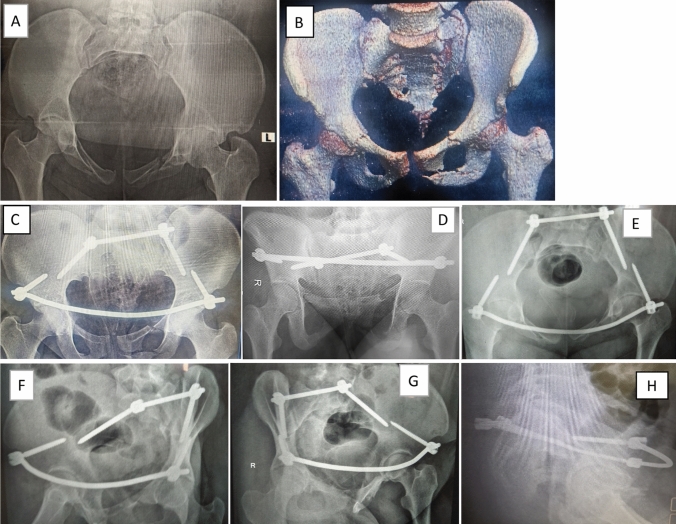 Fig. 6. A, B Preoperative radiograph showing left fracture sacrum Denis type 2 in 21 years old male. C–H Final follow-up different radiographs showing iliac screws accurate trajectory Source: Does minimally invasive percutaneous transilial internal fixator became an effective option for sacral fractures? A prospective study with novel implantation technique — European Journal of Trauma and Emergency Surgery 2023; CC BY.
Fig. 6. A, B Preoperative radiograph showing left fracture sacrum Denis type 2 in 21 years old male. C–H Final follow-up different radiographs showing iliac screws accurate trajectory Source: Does minimally invasive percutaneous transilial internal fixator became an effective option for sacral fractures? A prospective study with novel implantation technique — European Journal of Trauma and Emergency Surgery 2023; CC BY.
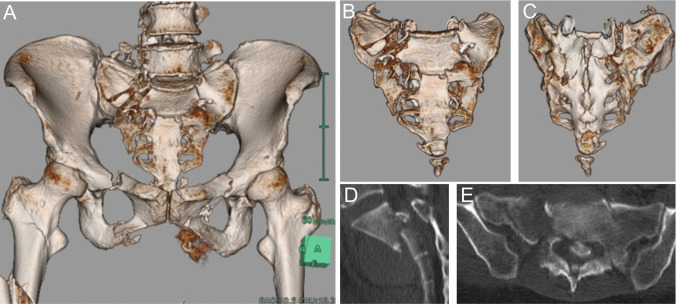 Fig. 1. Computed tomography (CT) on admission (A) Three-dimensional CT reconstruction of the pelvis demonstrating bilateral sacral fractures, bilateral ischiopubic fractures, and right femoral… Source: Modified spinopelvic crab-shaped fixation using offset connectors for a H-shaped sacral fracture with a floating Roy-Camille type 3 transverse component: a case report — Acta Neurochirurgica 2026; CC BY-NC-ND.
Fig. 1. Computed tomography (CT) on admission (A) Three-dimensional CT reconstruction of the pelvis demonstrating bilateral sacral fractures, bilateral ischiopubic fractures, and right femoral… Source: Modified spinopelvic crab-shaped fixation using offset connectors for a H-shaped sacral fracture with a floating Roy-Camille type 3 transverse component: a case report — Acta Neurochirurgica 2026; CC BY-NC-ND.
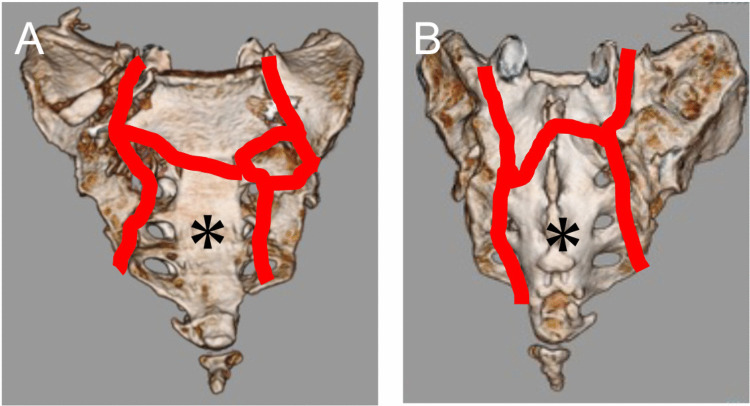 Fig. 2. Schematic depiction of sacral fracture lines (red) The distal sacral fragment (asterisk), classified as Roy-Camille type 3, was a floating fragment. The right side involved Denis zone… Source: Modified spinopelvic crab-shaped fixation using offset connectors for a H-shaped sacral fracture with a floating Roy-Camille type 3 transverse component: a case report — Acta Neurochirurgica 2026; CC BY-NC-ND.
Fig. 2. Schematic depiction of sacral fracture lines (red) The distal sacral fragment (asterisk), classified as Roy-Camille type 3, was a floating fragment. The right side involved Denis zone… Source: Modified spinopelvic crab-shaped fixation using offset connectors for a H-shaped sacral fracture with a floating Roy-Camille type 3 transverse component: a case report — Acta Neurochirurgica 2026; CC BY-NC-ND.
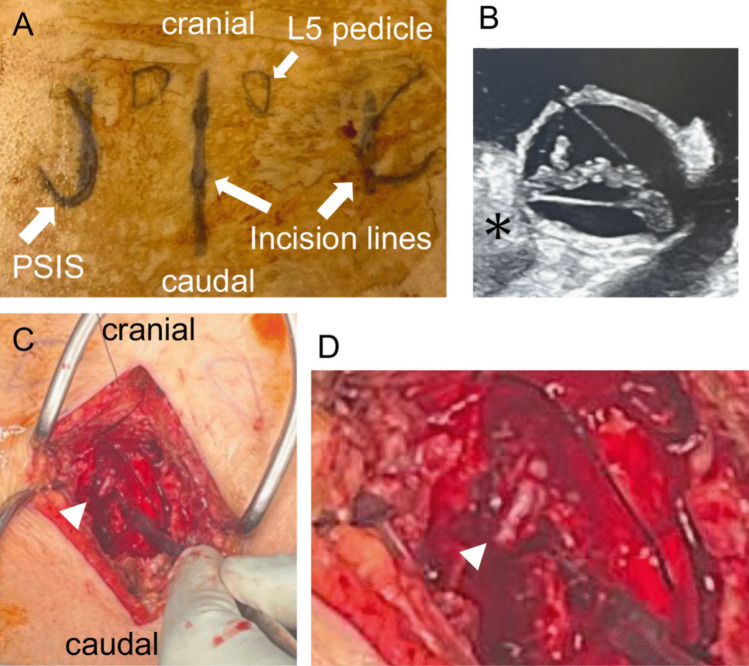 Fig. 3. Preoperative and intraoperative photographs (A) Preoperative photograph showing bilateral 5-cm incisions above the posterior superior iliac spine (PSIS) for placement of L5 pedicle… Source: Modified spinopelvic crab-shaped fixation using offset connectors for a H-shaped sacral fracture with a floating Roy-Camille type 3 transverse component: a case report — Acta Neurochirurgica 2026; CC BY-NC-ND.
Fig. 3. Preoperative and intraoperative photographs (A) Preoperative photograph showing bilateral 5-cm incisions above the posterior superior iliac spine (PSIS) for placement of L5 pedicle… Source: Modified spinopelvic crab-shaped fixation using offset connectors for a H-shaped sacral fracture with a floating Roy-Camille type 3 transverse component: a case report — Acta Neurochirurgica 2026; CC BY-NC-ND.
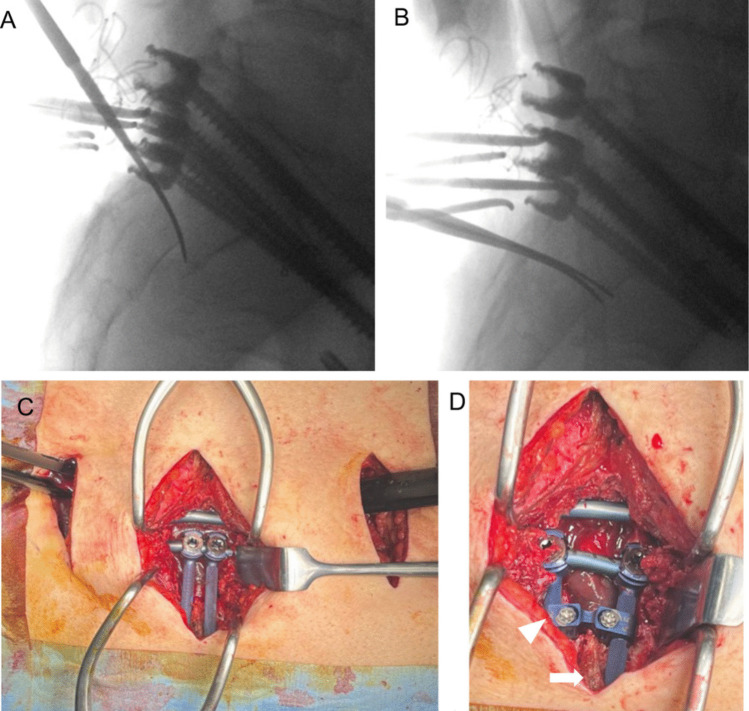 Fig. 4. Reduction maneuver and buttress technique (A) Bilateral neurodissectors were inserted lateral to the dura into the transverse fracture site, with the tips positioned on the ventral… Source: Modified spinopelvic crab-shaped fixation using offset connectors for a H-shaped sacral fracture with a floating Roy-Camille type 3 transverse component: a case report — Acta Neurochirurgica 2026; CC BY-NC-ND.
Fig. 4. Reduction maneuver and buttress technique (A) Bilateral neurodissectors were inserted lateral to the dura into the transverse fracture site, with the tips positioned on the ventral… Source: Modified spinopelvic crab-shaped fixation using offset connectors for a H-shaped sacral fracture with a floating Roy-Camille type 3 transverse component: a case report — Acta Neurochirurgica 2026; CC BY-NC-ND.
History of Present Illness
- Chief complaint: Low back/pelvic/buttock pain, inability to bear weight, ± bowel/bladder/sexual dysfunction and saddle anesthesia (sacral nerve injury)
- Mechanism (high-energy: fall from height, MVC), associated pelvic ring/abdominal/GU injuries (polytrauma)
- U-type/H-type = spinopelvic dissociation (spine separated from pelvis — highly unstable)
Past Medical History
- Associated pelvic/visceral/GU injuries, osteoporosis (insufficiency sacral fractures in elderly — different management), anticoagulation
- Standard PMH
Imaging Review
CT Pelvis/Sacrum (with reconstructions)
- Denis classification (zone I lateral to foramina, zone II through foramina, zone III central/canal — highest neuro risk), transverse component (U/H-type = spinopelvic dissociation)
- Displacement, kyphosis, canal/foraminal compromise, pelvic ring integrity, sacral dysmorphism (screw planning)
MRI
- Sacral nerve roots/cauda, hematoma, neural compression
X-ray (pelvis, inlet/outlet views)
Labs
- CBC, BMP, Coags, type and crossmatch, trauma labs
Neurological Examination
- Sacral nerve roots: perianal sensation, rectal tone, bulbocavernosus reflex, bladder/bowel function, lower extremity motor/sensory; document baseline
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- OR setup: spine table with log-roll precautions, fluoroscopy/O-arm/navigation, traction/Mayfield when cervical, posterior/anterior implant trays, decompression instruments, cell saver/blood for large constructs, and IONM before positioning when feasible.
- Special needs: arterial line, Foley, type/cross, MAP augmentation for acute SCI per local protocol, no long paralytic when MEPs are needed, anticoagulation/reversal plan, and airway strategy for unstable cervical injuries.
- Immediate postop orders: serial ASIA/neuro checks, MAP goal/duration if SCI, CT/X-rays for hardware/alignment, brace/collar orders, drain care, DVT prophylaxis timing, bowel/bladder/skin care, and early rehab/SCI consult.
Diagnosis & Indication / Approach
- Indication: Unstable sacral fracture / spinopelvic dissociation, displacement/deformity, neurological deficit (decompression), inability to mobilize
- Spinopelvic (lumbopelvic) fixation: pedicle screws (L4-L5/S1) connected to iliac screws — bridges spine to pelvis for U-type dissociation
- Iliosacral (SI) screws: percutaneous, for certain zone I/II and pelvic ring; sacral decompression (laminectomy/foraminotomy) for zone III with neural deficit
- Coordinate with orthopedic trauma (pelvic ring)
Classification and Construct Choice
- Denis zone, Roy-Camille/U-type morphology, vertical instability, lumbosacral kyphosis, pelvic-ring injury, and neurologic deficit determine whether this is a pelvic screw case or a spinopelvic fixation case.
- Percutaneous iliosacral/transsacral screws may be enough for stable corridors without spinopelvic dissociation; U-type dissociation, vertical shear, severe comminution, or inability to mobilize usually needs lumbopelvic fixation.
- Decompression is most compelling for progressive deficit or imaging-proven root/canal compression; chronic complete sacral deficits may not recover, so decompression should be weighed against wound and stability needs.
- Decide early with orthopedic trauma who owns pelvic-ring reduction, anterior fixation, weight-bearing restrictions, and timing around abdominal/urologic injuries.
Imaging and Neurologic Checklist
- CT pelvis with inlet/outlet/sagittal reconstructions: sacral corridors, foraminal compromise, transverse component, kyphosis, comminution, and safe S1/S2 screw pathways.
- MRI when neurologic deficit is unexplained or root compression/epidural hematoma changes decompression urgency.
- Document saddle sensation, rectal tone, bulbocavernosus reflex, voluntary anal contraction, bladder scan/catheter status, and sexual function baseline when possible.
Position
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- Prone, Jackson table, fluoroscopy (pelvis — inlet/outlet/lateral), IONM; careful with associated injuries
Key Surgical Steps (Lumbopelvic Fixation)
- Posterior midline (and/or paramedian for iliac screws) exposure of lumbar spine and posterior pelvis
- Pedicle screws at L4/L5/S1; iliac screws (entry at PSIS, aimed toward AIIS, between inner/outer tables — fluoroscopic “teardrop” view) ± S2-alar-iliac (S2AI) screws
- Reduce the sacral fracture/dissociation (restore alignment, lumbosacral kyphosis)
- Sacral decompression (laminectomy/foraminotomy) if neural compression/deficit — decompress sacral roots
- Connect rods spine-to-pelvis, lock, confirm reduction/hardware (fluoroscopy/CT)
- Decorticate/graft as appropriate, drain, closure
- (± Iliosacral screws for pelvic ring, with ortho)
Critical Anatomy & Structures at Risk
- Sacral nerve roots / cauda equina (zone III, foraminal) — bowel/bladder/sexual function
- Iliac screw corridors — between inner/outer tables (avoid sciatic notch, hip joint, pelvic viscera/vessels)
- L5 nerve root (anterior sacral ala), presacral vessels/structures, sacroiliac joint
Equipment
- Spinopelvic system (pedicle + iliac/S2AI screws, rods, connectors), fluoroscopy/navigation
- Decompression instruments, bone graft, cell saver, crossmatched blood
Monitoring
- EMG (sacral roots), SSEPs, MEPs
Anesthesia
- Arterial line, crossmatched blood, MAP support (if neural injury), prone precautions, coordinate trauma
Potential Complications
- Sacral nerve injury / persistent bowel-bladder-sexual dysfunction
- Hardware prominence (iliac screws — symptomatic), screw malposition (notch/joint/vessels)
- Wound complications/infection (posterior pelvis, polytrauma), nonunion, loss of reduction
- Blood loss, associated pelvic injury complications
Intraoperative and Postoperative Rescue
- Poor fluoroscopic corridor: stop and obtain better inlet/outlet/lateral imaging or navigation; sacral dysmorphism makes “standard” screw angles unsafe.
- Screw breach or triggered EMG change: remove/reposition, check CT if uncertain, and prioritize root safety over construct convenience.
- Reduction worsens neuromonitoring: release correction, raise MAP, reassess root/canal compression, and decide whether decompression is needed before final locking.
- Posterior wound risk: minimize dead space, consider drains/negative-pressure dressing in polytrauma or degloving injury, and coordinate timing if fecal/urogenital contamination exists.
- Persistent bladder/bowel dysfunction: involve urology/rehab early, trend post-void residuals, bowel program, and counsel that sacral neurologic recovery is variable and often slow.
- Hardware prominence/pain after union: evaluate fusion/fracture healing before elective iliac screw removal or revision to lower-profile S2AI fixation.
Operative Note Template
Preoperative Diagnosis: [Denis zone __ / U-type] sacral fracture with spinopelvic dissociation [± sacral nerve deficit]
Postoperative Diagnosis: Same
Procedure: Lumbopelvic (spinopelvic) instrumented fixation [L_-ilium] [with sacral decompression] for sacral fracture / spinopelvic dissociation
Surgeon / Assistant: [± orthopedic trauma] Anesthesia: General endotracheal EBL / Fluids / Blood products: [crossmatched] Adjuncts: Fluoroscopy (inlet/outlet/lateral)/navigation; EMG (sacral roots)/SSEP/MEP Implants: Pedicle screws (L4/L5/S1), iliac/S2AI screws, rods, bone graft Complications: None
Indications: [Age]yo [M/F] with an unstable [U-type] sacral fracture/spinopelvic dissociation after high-energy trauma [with sacral nerve deficit — bowel/bladder/saddle]. Associated pelvic/visceral injuries were managed with the trauma team. Risks discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and neuromonitoring (including sacral-root EMG) established. The patient was positioned prone on a Jackson table with fluoroscopy. A posterior midline [± paramedian] exposure of the lumbar spine and posterior pelvis was performed. Pedicle screws (L4/L5/S1) and iliac/S2-alar-iliac screws were placed under fluoroscopic inlet/outlet/lateral guidance, staying within bone and avoiding the sacral foramina, canal, and sciatic notch.
The sacral fracture/dissociation was reduced and lumbosacral alignment restored. [A sacral laminectomy/foraminotomy decompressed the sacral roots for the neurological deficit.] Rods connected the spine to the pelvis and were locked; reduction and hardware were confirmed on fluoroscopy/CT. Neuromonitoring remained stable.
Hemostasis was obtained, a drain placed, and closure performed in layers. The patient was transferred to the [ICU] with sacral-function monitoring.
Postoperative Plan
- ICU/floor per trauma, neuro checks (sacral function), MAP support if neural injury
- CT postop (hardware, reduction), weight-bearing per ortho/construct
- DVT prophylaxis (high risk — pelvic trauma), bowel/bladder management (urology), wound monitoring
- Rehab, follow-up imaging; counsel re: recovery of sacral function (variable)
Chief-Level Case Review
Use these as the senior-level mental model for Sacral Fracture / Spinopelvic (Lumbopelvic) Fixation:
- Decision point: Treat physiology while preparing the room: airway, reversal, transfusion, ICP/CPP, sodium/osmolality, temperature, and repeat imaging drive timing as much as the scan finding.
- Technical lever: Know the operative priority: decompression, hemorrhage control, debridement, dural closure, reconstruction, stabilization, or contamination control.
- Bailout: Plan for swelling and coagulopathy: bone flap decision, duraplasty size, drain/EVD need, hemostatic adjuncts, and ICU handoff should be decided early.
- Postop watch: Postop failure modes are predictable: expanding hematoma, malignant edema, seizure, infection, CSF leak, venous sinus injury, and missed associated spine/vascular injury.
Common Pimp Questions
Use these to pressure-test preparation for Sacral Fracture / Spinopelvic (Lumbopelvic) Fixation:
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]