
Case Prep: Penetrating Spine Injury (Gunshot / Stab) Management
Case / Approach Snapshot
- Anatomy at risk: unstable columns, cord/roots, dura, vertebral artery or great-vessel/visceral structures by level, fracture lines, and fixation corridors.
- Operative steps: protect the spine during transfer/positioning, confirm levels and reduction goals, decompress when indicated, instrument/reconstruct stability, verify alignment and hardware, and plan ICU/brace/rehab needs; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: neurologic deterioration, reduction failure, vascular/visceral injury, durotomy, blood loss, hardware pullout, infection, and staged anterior/posterior stabilization.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a penetrating [gunshot / stab] spinal injury at [level] with [complete/incomplete SCI / nerve root deficit / CSF leak / retained fragment] planned for [observation vs decompression/debridement ± stabilization].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior cervical approach or posterior thoracolumbar approach — level-specific posterior decompression, dural repair, and stabilization.
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Penetrating spine injury bisecting thoracic spinal canal with no significant neurological deficits-The midline cord syndrome — Sarkar B. Spinal cord series and cases 2018. PubMed
- Spinal Cord Stimulation for Painful Neuropathic Cauda Equina Syndrome Following Ballistic Penetrating Lumbar Spine Injury: Proof-of-Concept Case — Beucler N. Military medicine 2025. PubMed
- Brown-Séquard Syndrome Following a Thoracic Spine Stab Wound: A Case Report — Moreira TS. Cureus 2023. PubMed
- Penetrating spinal injury with a wooden fragment: a case report and review of the literature — Gul S. Spine 2010. PubMed
- Surgical Considerations and Neurological Outcomes in Ballistic Penetrating Subaxial Cervical Spine Fractures: A Retrospective Analysis — Batbold A. Clinical spine surgery 2025. PubMed
- Brown-Sequard syndrome associated with a spinal cord injury caused by a retained screwdriver: A case report and literature review — Abdulqader MN. Surgical neurology international 2022. PubMed
- Minimally invasive approach to non-missile penetrating spinal injury with resultant retained foreign body: A case report and review of the literature — Moldovan K. Clinical neurology and neurosurgery 2019. PubMed
- Gunshot wound causing complete spinal cord injury without mechanical violation of spinal axis: Case report with review of literature — Patil R. Journal of craniovertebral junction & spine 2015. PubMed
- A case series of penetrating spinal trauma: comparisons to blunt trauma, surgical indications, and outcomes — Morrow KD. Neurosurgical focus 2019. PubMed
- A Unique Case of an Arrow-Related Penetrating Spinal Cord Injury in Kenya and a Comprehensive Literature Review — Chelmis FS. Journal of neurological surgery reports 2026. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
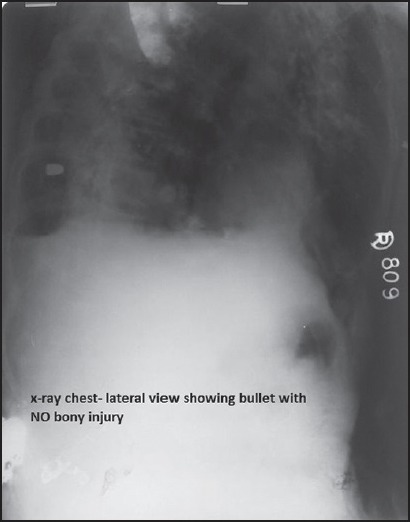 Figure 1. X-ray chest lateral view showing the bullet with no bony injuries Source: Gunshot wound causing complete spinal cord injury without mechanical violation of spinal axis: Case report with review of literature — Journal of Craniovertebral Junction & Spine 2015; CC BY-NC-SA.
Figure 1. X-ray chest lateral view showing the bullet with no bony injuries Source: Gunshot wound causing complete spinal cord injury without mechanical violation of spinal axis: Case report with review of literature — Journal of Craniovertebral Junction & Spine 2015; CC BY-NC-SA.
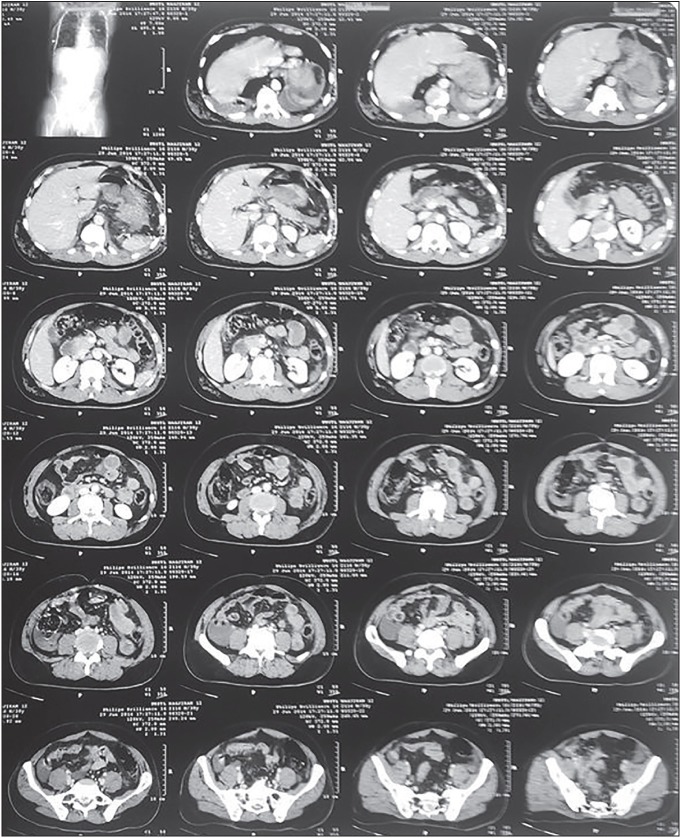 Figure 2. Computed tomography scan of the thorax and abdomen Source: Gunshot wound causing complete spinal cord injury without mechanical violation of spinal axis: Case report with review of literature — Journal of Craniovertebral Junction & Spine 2015; CC BY-NC-SA.
Figure 2. Computed tomography scan of the thorax and abdomen Source: Gunshot wound causing complete spinal cord injury without mechanical violation of spinal axis: Case report with review of literature — Journal of Craniovertebral Junction & Spine 2015; CC BY-NC-SA.
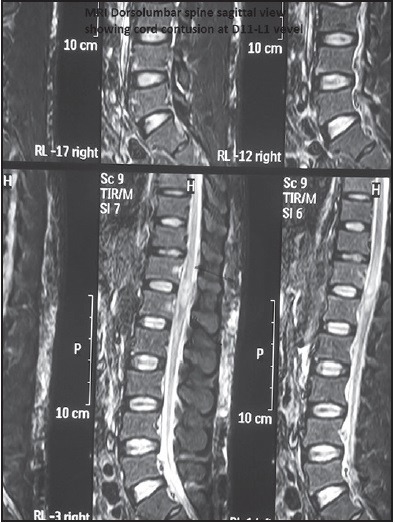 Figure 3. Magnetic resonance imaging dorso-lumbar spine (sagittal view) showing cord contusion at D11-L1 vertebral level Source: Gunshot wound causing complete spinal cord injury without mechanical violation of spinal axis: Case report with review of literature — Journal of Craniovertebral Junction & Spine 2015; CC BY-NC-SA.
Figure 3. Magnetic resonance imaging dorso-lumbar spine (sagittal view) showing cord contusion at D11-L1 vertebral level Source: Gunshot wound causing complete spinal cord injury without mechanical violation of spinal axis: Case report with review of literature — Journal of Craniovertebral Junction & Spine 2015; CC BY-NC-SA.
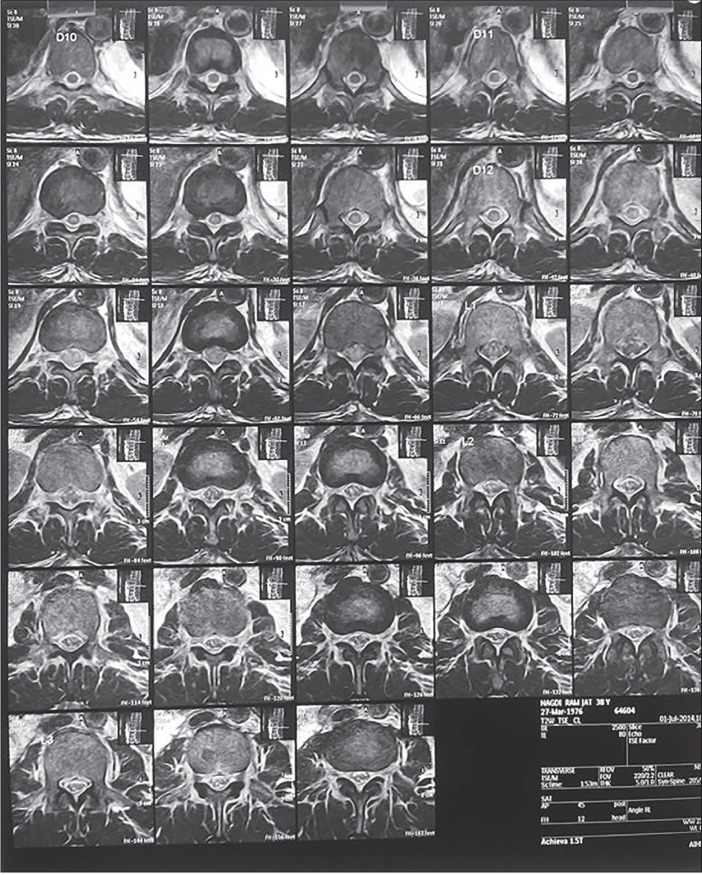 Figure 4. Magnetic resonance imaging dorso-lumbar spine coronal view showing cord contusion at D11-L1 vertebral level Source: Gunshot wound causing complete spinal cord injury without mechanical violation of spinal axis: Case report with review of literature — Journal of Craniovertebral Junction & Spine 2015; CC BY-NC-SA.
Figure 4. Magnetic resonance imaging dorso-lumbar spine coronal view showing cord contusion at D11-L1 vertebral level Source: Gunshot wound causing complete spinal cord injury without mechanical violation of spinal axis: Case report with review of literature — Journal of Craniovertebral Junction & Spine 2015; CC BY-NC-SA.
 Figure 5. Topogram image of computed tomography scan Thorax and abdomen showing bullet in right lateral chest wall Source: Gunshot wound causing complete spinal cord injury without mechanical violation of spinal axis: Case report with review of literature — Journal of Craniovertebral Junction & Spine 2015; CC BY-NC-SA.
Figure 5. Topogram image of computed tomography scan Thorax and abdomen showing bullet in right lateral chest wall Source: Gunshot wound causing complete spinal cord injury without mechanical violation of spinal axis: Case report with review of literature — Journal of Craniovertebral Junction & Spine 2015; CC BY-NC-SA.
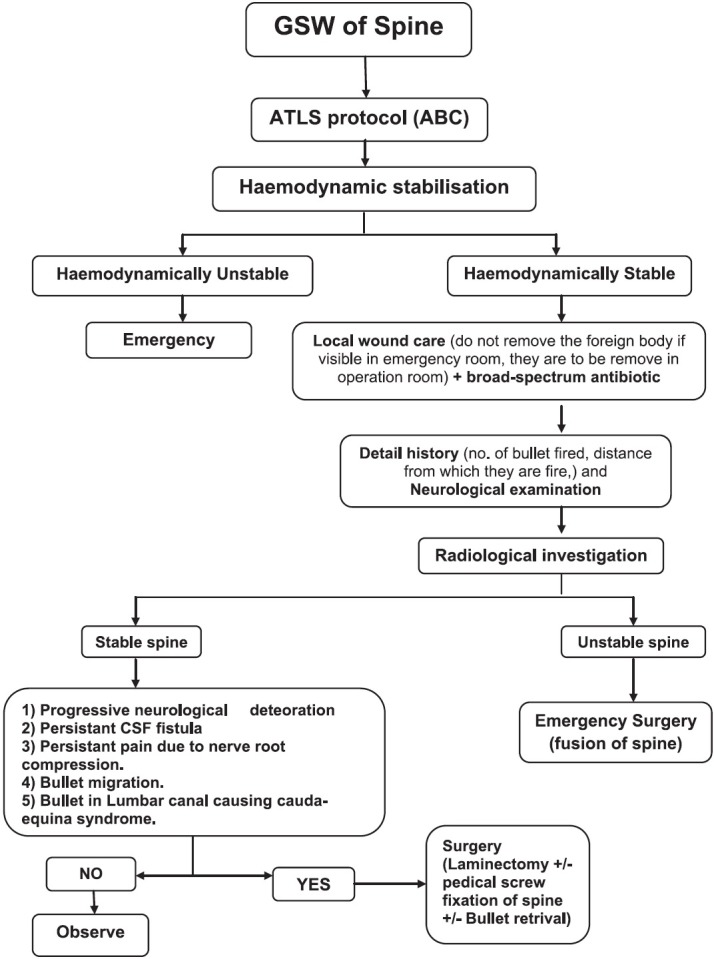 Figure 6. Systematic management of GSW of spine Source: Gunshot wound causing complete spinal cord injury without mechanical violation of spinal axis: Case report with review of literature — Journal of Craniovertebral Junction & Spine 2015; CC BY-NC-SA.
Figure 6. Systematic management of GSW of spine Source: Gunshot wound causing complete spinal cord injury without mechanical violation of spinal axis: Case report with review of literature — Journal of Craniovertebral Junction & Spine 2015; CC BY-NC-SA.
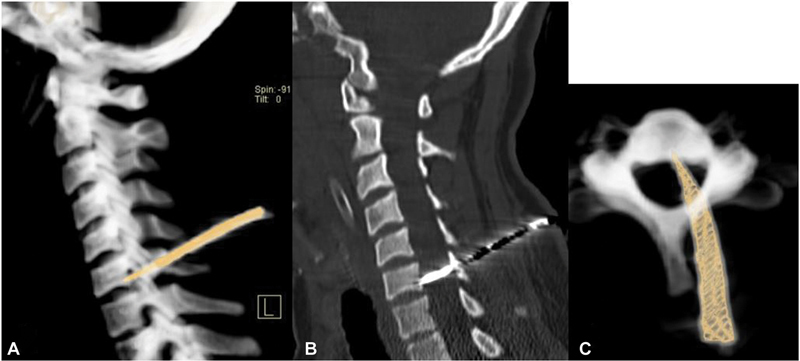 Fig. 1. Computed tomography cervical spine: ( A , B ) Sagittal images showing the path of impaled knife passing through C5 lamina, across the spinal canal onto C6 vertebral body. ( C ) Axial… Source: Role of Whole-Body Computed Tomography Scan to Avoid Missed Foreign Body in Patients with Multiple Stab Injury: A Rare Case of Retained Impaled Knife Blade with Intact Neurology — Asian Journal of Neurosurgery 2022; CC BY-NC-ND.
Fig. 1. Computed tomography cervical spine: ( A , B ) Sagittal images showing the path of impaled knife passing through C5 lamina, across the spinal canal onto C6 vertebral body. ( C ) Axial… Source: Role of Whole-Body Computed Tomography Scan to Avoid Missed Foreign Body in Patients with Multiple Stab Injury: A Rare Case of Retained Impaled Knife Blade with Intact Neurology — Asian Journal of Neurosurgery 2022; CC BY-NC-ND.
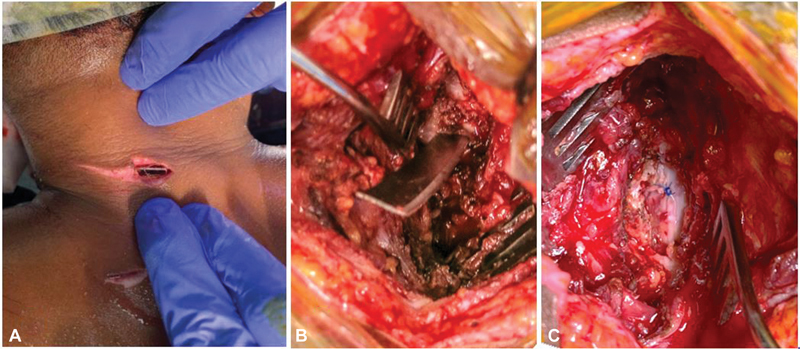 Fig. 2. Intraoperative images showing ( A ) incised wound over the posterior aspect of the neck with a visible broken knife blade below the skin, ( B ) wound exploration around knife blade that… Source: Role of Whole-Body Computed Tomography Scan to Avoid Missed Foreign Body in Patients with Multiple Stab Injury: A Rare Case of Retained Impaled Knife Blade with Intact Neurology — Asian Journal of Neurosurgery 2022; CC BY-NC-ND.
Fig. 2. Intraoperative images showing ( A ) incised wound over the posterior aspect of the neck with a visible broken knife blade below the skin, ( B ) wound exploration around knife blade that… Source: Role of Whole-Body Computed Tomography Scan to Avoid Missed Foreign Body in Patients with Multiple Stab Injury: A Rare Case of Retained Impaled Knife Blade with Intact Neurology — Asian Journal of Neurosurgery 2022; CC BY-NC-ND.
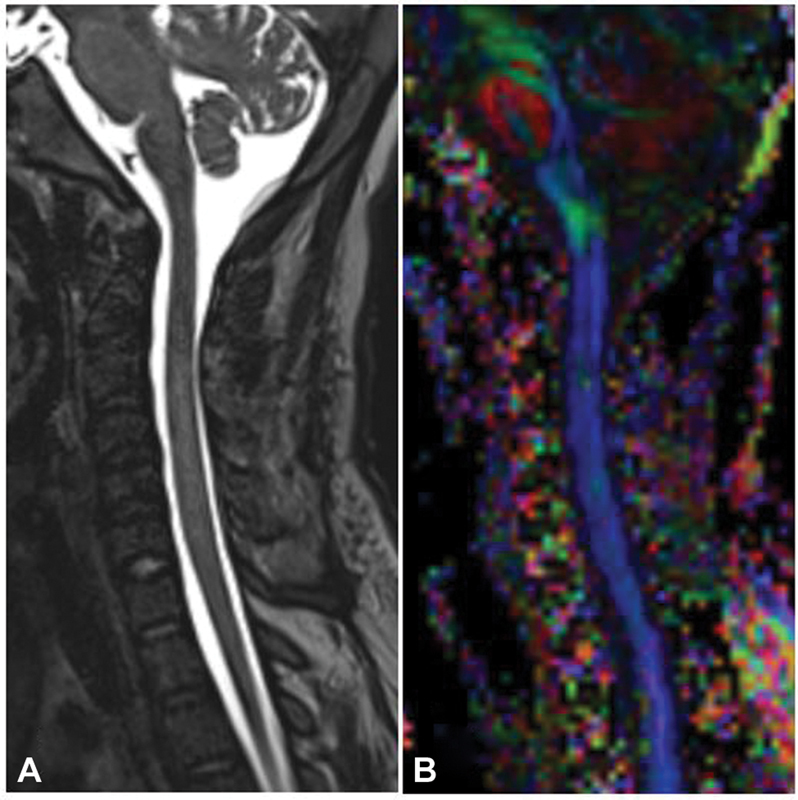 Fig. 3. Postoperative magnetic resonance imaging: ( A ) Sagittal T2-weighted sequence with normal cord without evidence of cerebrospinal fluid leak and ( B ) diffusion tensor imaging… Source: Role of Whole-Body Computed Tomography Scan to Avoid Missed Foreign Body in Patients with Multiple Stab Injury: A Rare Case of Retained Impaled Knife Blade with Intact Neurology — Asian Journal of Neurosurgery 2022; CC BY-NC-ND.
Fig. 3. Postoperative magnetic resonance imaging: ( A ) Sagittal T2-weighted sequence with normal cord without evidence of cerebrospinal fluid leak and ( B ) diffusion tensor imaging… Source: Role of Whole-Body Computed Tomography Scan to Avoid Missed Foreign Body in Patients with Multiple Stab Injury: A Rare Case of Retained Impaled Knife Blade with Intact Neurology — Asian Journal of Neurosurgery 2022; CC BY-NC-ND.
 Figure 1. A computed tomography scan depicting the penetrating object crossing the T8 vertebral body (blue arrow). Source: Brown-Séquard Syndrome Following a Thoracic Spine Stab Wound: A Case Report — Cureus 2023; CC BY.
Figure 1. A computed tomography scan depicting the penetrating object crossing the T8 vertebral body (blue arrow). Source: Brown-Séquard Syndrome Following a Thoracic Spine Stab Wound: A Case Report — Cureus 2023; CC BY.
History of Present Illness
- Chief complaint: Penetrating trauma with neurological deficit
- Mechanism (handgun/high-velocity rifle/stab), trajectory, associated visceral/vascular injuries (thoracoabdominal — often take priority)
- Most civilian gunshot SCIs are managed non-operatively (surgery often doesn’t improve neuro outcome and adds risk) — selective indications
- Hemodynamic stability, other injuries
Past Medical History
- Associated injuries (vascular, visceral, airway), tetanus status, anticoagulation
- Standard PMH; trauma ATLS workup
Imaging Review
CT (spine + trauma pan-scan)
- Fragment/bullet location and trajectory, bony injury, canal involvement, retained fragments, instability (less common with GSW than blunt), associated injuries
- Caution: MRI only if confirmed non-ferromagnetic fragment (most modern bullets are, but verify) — risk of migration/heating
MRI (if MRI-safe)
- Cord injury, hematoma, compression by fragment/disc
CT angiography
- Vascular injury (vertebral/carotid, great vessels)
Labs
- CBC, BMP, Coags, type and crossmatch, trauma labs, tetanus
Neurological Examination
- Complete ASIA exam, level, complete vs incomplete, sacral sparing, sphincter; serial
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- OR setup: spine table with log-roll precautions, fluoroscopy/O-arm/navigation, traction/Mayfield when cervical, posterior/anterior implant trays, decompression instruments, cell saver/blood for large constructs, and IONM before positioning when feasible.
- Special needs: arterial line, Foley, type/cross, MAP augmentation for acute SCI per local protocol, no long paralytic when MEPs are needed, anticoagulation/reversal plan, and airway strategy for unstable cervical injuries.
- Immediate postop orders: serial ASIA/neuro checks, MAP goal/duration if SCI, CT/X-rays for hardware/alignment, brace/collar orders, drain care, DVT prophylaxis timing, bowel/bladder/skin care, and early rehab/SCI consult.
Diagnosis & Indication (Selective Surgery)
- Non-operative (most): complete SCI without ongoing compression, stable, no CSF leak, no migrating fragment
- Surgical indications:
- Incomplete/progressive deficit with a compressive fragment/hematoma in the canal (decompress)
- CSF leak / dural laceration (repair)
- Instability (uncommon with GSW; more with high-velocity/blunt) → stabilize
- Migrating fragment, infection/abscess, fragment in canal with deteriorating function
- Cauda equina compression (better recovery potential — decompress)
- Bowel-transgressing trajectory: antibiotics (contamination); fragment removal from canal controversial
- Goals: decompress salvageable neural tissue, repair dura, debride, stabilize if unstable
Position
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- Per level/approach (usually posterior for canal decompression); prone; IONM if incomplete
Key Surgical Steps
- Trauma stabilization / associated injury priority first (vascular, visceral)
- Approach the canal (laminectomy) at the injured level
- Decompress — remove the compressive fragment/bone/disc/hematoma from the canal (only if it will help — incomplete deficit/cauda)
- Dural repair if CSF leak/laceration (primary or graft — prevent fistula/pseudomeningocele/meningitis)
- Debride devitalized/contaminated tissue (esp. bowel-contaminated trajectory)
- Stabilize if unstable (instrumentation)
- Copious irrigation, closure; antibiotics
Critical Anatomy & Structures at Risk
- Spinal cord / cauda / nerve roots (already injured)
- Vascular structures along trajectory (vertebral, great vessels)
- Dura (leak/fistula), adjacent viscera (trajectory), lead toxicity (rare, intra-articular/CSF fragments)
Equipment
- Decompression/instrumentation sets, microscope, dural repair materials
- Copious irrigation, fluoroscopy, culture media (contaminated)
Monitoring
- SSEPs/MEPs (incomplete injuries)
Anesthesia
- Trauma/resuscitation, MAP support (SCI), crossmatched blood, antibiotics, tetanus, coordinate trauma/vascular
Potential Complications
- CSF fistula/pseudomeningocele/meningitis, infection (contaminated)
- No neurological improvement (complete injuries), worsening (manipulation)
- Vascular injury, instability, lead toxicity (rare), associated-injury complications
Operative Note Template
Preoperative Diagnosis: Penetrating [gunshot/stab] spinal injury at [level] with [incomplete SCI / CSF leak / canal fragment / instability]
Postoperative Diagnosis: Same
Procedure: [Level] laminectomy for decompression [± dural repair, debridement, instrumented stabilization] for penetrating spinal injury
Surgeon / Assistant: [± trauma/vascular] Anesthesia: General endotracheal EBL / Fluids / Blood products: [crossmatched] Adjuncts: Fluoroscopy, microscope; SSEP/MEP (incomplete injuries); culture media (contaminated) Implants: [Dural graft; instrumentation if unstable], antibiotics, tetanus Complications: None
Indications: [Age]yo [M/F] with a penetrating spinal injury at [level]. Surgery was indicated for [an incomplete/progressive deficit with a compressive canal fragment/hematoma / CSF leak / instability / contaminated trajectory], after trauma stabilization and management of associated injuries. Risks discussed.
Description of Procedure: After trauma stabilization and consent/time-out, general anesthesia was induced [with MAP support for SCI] and neuromonitoring established [for the incomplete injury]. The patient was positioned [prone] and a laminectomy performed at [level] to access the canal. The compressive [fragment/bone/hematoma] was removed and the neural elements decompressed. [A dural laceration was repaired primarily/with graft to prevent a fistula.] [Devitalized/contaminated tissue was debrided.] [Instrumented stabilization was performed for instability.] The field was copiously irrigated and antibiotics administered.
Closure was performed in layers. The patient was transferred to the ICU with serial ASIA exams, MAP support, antibiotics, and CSF-leak precautions.
Postoperative Plan
- ICU, ASIA exams, MAP support, antibiotics (broad if contaminated), tetanus
- CSF leak monitoring, CT postop
- DVT prophylaxis (timing per bleeding/injuries), bowel/bladder/skin care, SCI rehab
- Coordinate trauma/vascular/general surgery; psychosocial support
- Follow-up imaging; counsel re: prognosis by completeness of injury
Chief-Level Case Review
Use these as the senior-level mental model for Penetrating Spine Injury (Gunshot / Stab) Management:
- Decision point: Treat physiology while preparing the room: airway, reversal, transfusion, ICP/CPP, sodium/osmolality, temperature, and repeat imaging drive timing as much as the scan finding.
- Technical lever: Know the operative priority: decompression, hemorrhage control, debridement, dural closure, reconstruction, stabilization, or contamination control.
- Bailout: Plan for swelling and coagulopathy: bone flap decision, duraplasty size, drain/EVD need, hemostatic adjuncts, and ICU handoff should be decided early.
- Postop watch: Postop failure modes are predictable: expanding hematoma, malignant edema, seizure, infection, CSF leak, venous sinus injury, and missed associated spine/vascular injury.
Common Pimp Questions
Use these to pressure-test preparation for Penetrating Spine Injury (Gunshot / Stab) Management:
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]