
Case Prep: Syringomyelia — Management / Syringosubarachnoid Shunt
Case / Approach Snapshot
- Anatomy at risk: the named neural, vascular, bony, CSF, and soft-tissue structures that determine the safe corridor and likely morbidity.
- Operative steps: confirm indication and imaging, position and expose deliberately, complete the core surgical maneuver, verify the result, and close with a complication-prevention plan; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: bleeding, neurologic change, wrong target or level, CSF leak, infection, hardware or reconstruction failure, and a staged or alternate-treatment plan.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [Chiari-associated / post-traumatic / idiopathic] syringomyelia at [levels] presenting with [dissociated sensory loss / hand weakness / pain / progressive myelopathy] planned for [treatment of underlying cause / syringosubarachnoid shunt].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior cervical approach or posterior thoracolumbar approach — choose by syrinx driver and exposure level.
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Syringosubarachnoid shunt: insertion technique — Amarouche M. British journal of neurosurgery 2023. PubMed
- Ultrasound-guided Syringosubarachnoid Shunt Insertion for Cervicothoracic Syringomyelia — Hussain I. Clinical spine surgery 2020. PubMed
- Syringosubarachnoid shunt for treatment of syringomyelia — Vaquero J. Acta neurochirurgica 1987. PubMed
- Treatment of syringomyelia with a syringosubarachnoid shunt — Tator CH. The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques 1988. PubMed
- Reevaluation of syringosubarachnoid shunt for syringomyelia with Chiari malformation — Iwasaki Y. Neurosurgery 2000. PubMed
- Syrinx shunts for syringomyelia: a systematic review and meta-analysis of syringosubarachnoid, syringoperitoneal, and syringopleural shunting — Rothrock RJ. Journal of neurosurgery. Spine 2021. PubMed
- [Syringosubarachnoid shunt for noncommunicating syringomyelia associated with spinal lipoma: a case report] — Yamamuro S. No shinkei geka. Neurological surgery 2012. PubMed
- Syringosubarachnoid shunt for syringomyelia associated with Chiari I malformation — Hida K. Neurosurgical focus 2001. PubMed
- Polytetrafluoroethylene sponge syringosubarachnoid shunt — Chagla AS. Turkish neurosurgery 2011. PubMed
- Minimally invasive insertion of syringosubarachnoid shunt for posttraumatic syringomyelia: technical case report — O’Toole JE. Neurosurgery 2007. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
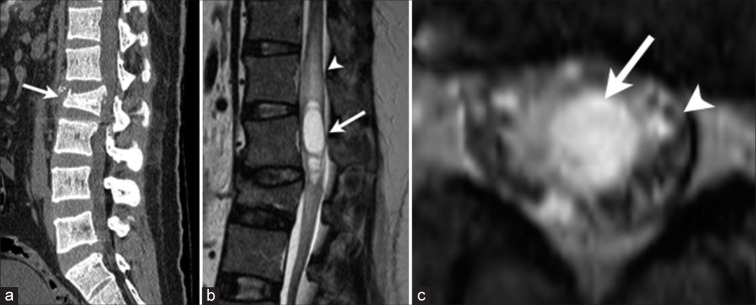 Figure 1:. Preoperative radiological findings. (a) A sagittal view of a plain computed tomography scan demonstrates a burst fracture of the L2 vertebra (arrow). Note that the L2 vertebra is… Source: Cauda equina syndrome due to posttraumatic syringomyelia in conus medullaris – A case report — Surgical Neurology International 2024; CC BY-NC-SA.
Figure 1:. Preoperative radiological findings. (a) A sagittal view of a plain computed tomography scan demonstrates a burst fracture of the L2 vertebra (arrow). Note that the L2 vertebra is… Source: Cauda equina syndrome due to posttraumatic syringomyelia in conus medullaris – A case report — Surgical Neurology International 2024; CC BY-NC-SA.
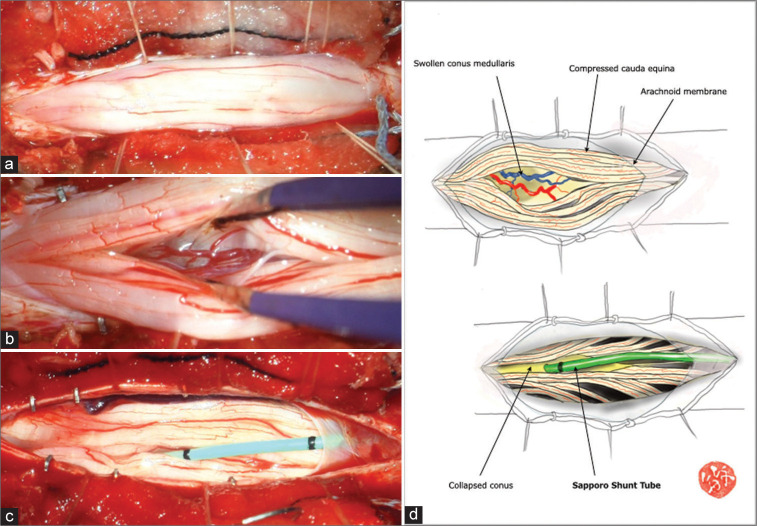 Figure 2:. Intraoperative findings. (a) Following the dural opening, the conus medullaris and cauda equina protruded from the dural sac. Note no adhesive arachnoiditis. (b) The conus medullaris was… Source: Cauda equina syndrome due to posttraumatic syringomyelia in conus medullaris – A case report — Surgical Neurology International 2024; CC BY-NC-SA.
Figure 2:. Intraoperative findings. (a) Following the dural opening, the conus medullaris and cauda equina protruded from the dural sac. Note no adhesive arachnoiditis. (b) The conus medullaris was… Source: Cauda equina syndrome due to posttraumatic syringomyelia in conus medullaris – A case report — Surgical Neurology International 2024; CC BY-NC-SA.
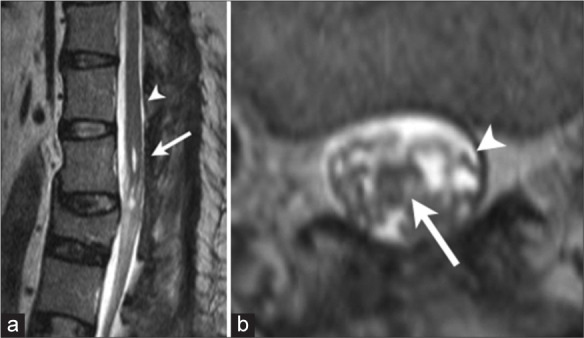 Figure 3:. Postoperative radiological findings. (a) Sagittal view of T2-weighted magnetic resonance imaging (MRI) shows almost complete disappearance of syrinx in the conus medullaris (arrow). Note… Source: Cauda equina syndrome due to posttraumatic syringomyelia in conus medullaris – A case report — Surgical Neurology International 2024; CC BY-NC-SA.
Figure 3:. Postoperative radiological findings. (a) Sagittal view of T2-weighted magnetic resonance imaging (MRI) shows almost complete disappearance of syrinx in the conus medullaris (arrow). Note… Source: Cauda equina syndrome due to posttraumatic syringomyelia in conus medullaris – A case report — Surgical Neurology International 2024; CC BY-NC-SA.
 Figure 4. Source: Cauda equina syndrome due to posttraumatic syringomyelia in conus medullaris – A case report — Surg Neurol Int. 2024 Jul 12;15:243. doi: 10.25259/SNI_386_2024; CC BY-NC-SA.
Figure 4. Source: Cauda equina syndrome due to posttraumatic syringomyelia in conus medullaris – A case report — Surg Neurol Int. 2024 Jul 12;15:243. doi: 10.25259/SNI_386_2024; CC BY-NC-SA.
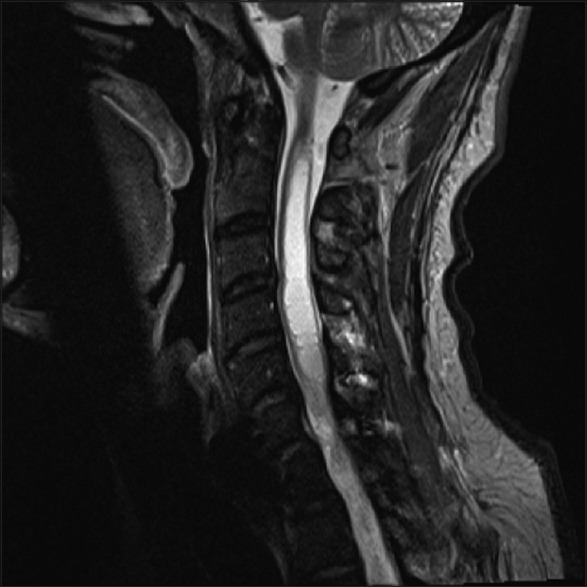 Figure 1. T2-weighted magnetic resonance imaging cervical spine Source: Syringosubarachnoid shunting using a myringotomy tube — Surgical Neurology International 2016; CC BY-NC-SA.
Figure 1. T2-weighted magnetic resonance imaging cervical spine Source: Syringosubarachnoid shunting using a myringotomy tube — Surgical Neurology International 2016; CC BY-NC-SA.
 Figure 2. Myringotomy tube Source: Syringosubarachnoid shunting using a myringotomy tube — Surgical Neurology International 2016; CC BY-NC-SA.
Figure 2. Myringotomy tube Source: Syringosubarachnoid shunting using a myringotomy tube — Surgical Neurology International 2016; CC BY-NC-SA.
 Figure 7. Source: Surgical treatment of idiopathic syringomyelia: Silastic wedge syringosubarachnoid shunting technique — Surg Neurol Int. 2014 Jul 24;5:114. doi: 10.4103/2152-7806.137536; CC BY-NC-SA.
Figure 7. Source: Surgical treatment of idiopathic syringomyelia: Silastic wedge syringosubarachnoid shunting technique — Surg Neurol Int. 2014 Jul 24;5:114. doi: 10.4103/2152-7806.137536; CC BY-NC-SA.
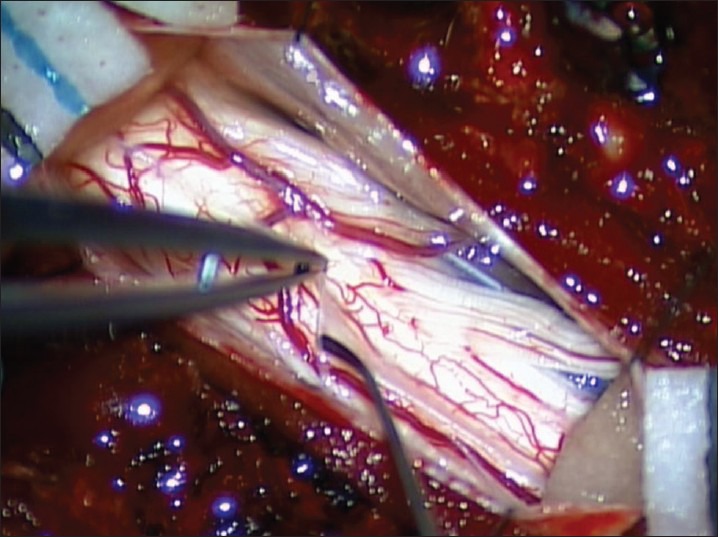 Figure 1. Opening the arachnoid membrane Source: Surgical treatment of idiopathic syringomyelia: Silastic wedge syringosubarachnoid shunting technique — Surgical Neurology International 2014; CC BY-NC-SA.
Figure 1. Opening the arachnoid membrane Source: Surgical treatment of idiopathic syringomyelia: Silastic wedge syringosubarachnoid shunting technique — Surgical Neurology International 2014; CC BY-NC-SA.
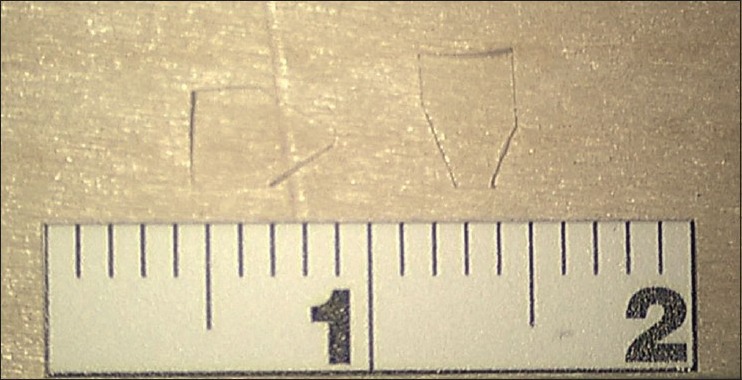 Figure 2. Contoured silastic wedges Source: Surgical treatment of idiopathic syringomyelia: Silastic wedge syringosubarachnoid shunting technique — Surgical Neurology International 2014; CC BY-NC-SA.
Figure 2. Contoured silastic wedges Source: Surgical treatment of idiopathic syringomyelia: Silastic wedge syringosubarachnoid shunting technique — Surgical Neurology International 2014; CC BY-NC-SA.
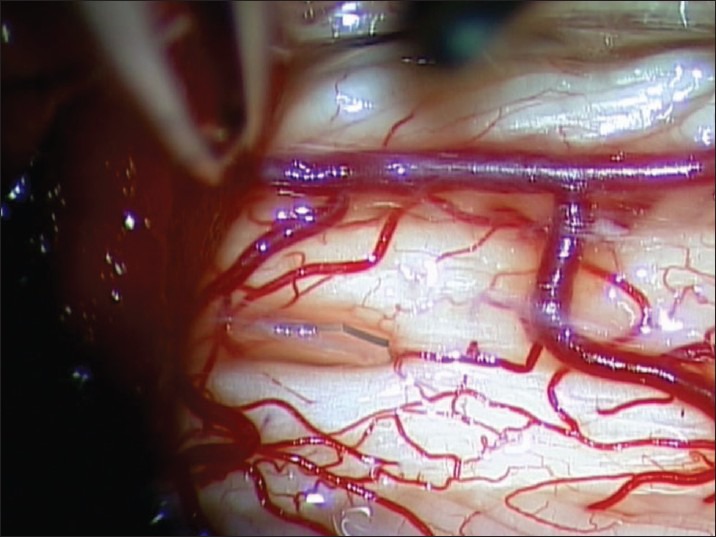 Figure 3. Initial placement of contoured silastic wedge Source: Surgical treatment of idiopathic syringomyelia: Silastic wedge syringosubarachnoid shunting technique — Surgical Neurology International 2014; CC BY-NC-SA.
Figure 3. Initial placement of contoured silastic wedge Source: Surgical treatment of idiopathic syringomyelia: Silastic wedge syringosubarachnoid shunting technique — Surgical Neurology International 2014; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Dissociated (cape-like) sensory loss (loss of pain/temperature, preserved light touch), hand/upper extremity weakness and atrophy, neuropathic pain, scoliosis (children), progressive myelopathy
- Etiology is key (treat the cause, not just the syrinx):
- Chiari I/II (most common — treat with posterior fossa decompression; syrinx usually improves)
- Post-traumatic (tethering/arachnoiditis at injury level — untether/expand)
- Post-infectious/arachnoiditis, tumor-associated, idiopathic
- Progression rate, prior decompression/shunt
Past Medical History
- Prior spinal trauma/SCI, meningitis/arachnoiditis, Chiari, prior posterior fossa or spinal surgery
- Standard PMH
Imaging Review
MRI Brain + Entire Spine (T1, T2, cine CSF flow)
- Syrinx extent/size, location, septations
- Underlying cause: Chiari (tonsillar descent, CSF flow at foramen magnum), tethering/arachnoid scar (post-traumatic — cord tethered, CSF flow block at injury level), tumor (enhancing nodule), basilar invagination
- Cine flow (CSF dynamics at foramen magnum / block level)
Labs
- CBC, BMP, Coags, type and screen
Neurological Examination
- Detailed motor (intrinsic hand), dissociated sensory mapping, reflexes, gait, scoliosis, document baseline
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: radiolucent spine-capable table selected for approach, imaging, instrumentation, patient size, and alignment goals; keep abdomen free for prone cases.
- OR setup: microscope, neuromonitoring, prone positioning pads, ultrasound/navigation if needed, dural repair materials, and CSF-leak management supplies.
- Special needs: Foley for detethering/bladder baseline, urology plan when neurogenic bladder is relevant, MAP/normothermia for cord perfusion, no long paralytic with MEPs, and meticulous skin-pressure protection.
- Immediate postop orders: motor/sensory/bladder checks, flat or activity restrictions per dural closure, wound/CSF-leak watch, pain/spasm regimen, MRI follow-up when indicated, and PT/urology follow-up.
Treat the Cause First (Principle)
- Chiari-associated: posterior fossa decompression (± duraplasty) → restores CSF flow, syrinx usually shrinks (see chiari-decompression)
- Post-traumatic/arachnoiditis: untethering + expansile duraplasty at the block level (restore subarachnoid CSF flow) — preferred over shunt
- Tumor-associated: resect tumor (syrinx resolves)
- Syringo-subarachnoid/peritoneal/pleural shunt: reserved for refractory/progressive syrinx when the cause cannot be addressed or untethering fails (shunts have high failure/complication rates — last resort)
Position
- OR table/bed: radiolucent spine-capable table selected for approach, imaging, instrumentation, patient size, and alignment goals; keep abdomen free for prone cases.
- Prone, Mayfield/foam, IONM baseline; per target (foramen magnum for Chiari, syrinx level for shunt/untethering)
Key Surgical Steps (Syringosubarachnoid Shunt — refractory cases)
- Laminectomy at the level of maximal syrinx (thinnest cord/dorsal)
- Midline durotomy, identify the dorsally expanded cord
- Myelotomy at the dorsal midline (or dorsal root entry zone) into the syrinx cavity (thinnest point — ultrasound-guided)
- Drain syrinx; place a small shunt catheter from the syrinx cavity into the subarachnoid space (syringo-subarachnoid), secure to pia
- (Alternative distal: peritoneal/pleural if subarachnoid inadequate)
- Watertight dural closure (expansile duraplasty to maintain subarachnoid space)
- Untethering (post-traumatic): lyse arachnoid adhesions at the block, expansile duraplasty to re-establish CSF flow (often preferred to shunting)
Critical Anatomy & Structures at Risk
- Spinal cord tracts — myelotomy (dorsal columns), already compromised cord
- Anterior spinal artery (ventral)
- Dura/subarachnoid space (shunt patency, CSF flow), arachnoid (adhesions)
Equipment
- Microscope, ultrasound (syrinx localization), syrinx shunt catheter, micro-instruments, fine bipolar
- Dural substitute (duraplasty), sealant
Monitoring
- SSEPs, MEPs, EMG
Anesthesia
- MAP support, no paralytic (IONM), prone precautions
Potential Complications
- Shunt failure/obstruction (syrinx shunts commonly fail — recurrence)
- Neurological worsening (myelotomy), CSF leak
- Recurrence/progression if underlying cause not addressed
- Tethering/arachnoiditis (re-block)
Operative Note Template
Preoperative Diagnosis: [Chiari-associated / post-traumatic / idiopathic] syringomyelia at [levels]
Postoperative Diagnosis: Same
Procedure: [Posterior fossa decompression / Untethering with expansile duraplasty / Syringosubarachnoid shunt placement] for syringomyelia at [levels]
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Microscope, ultrasound (syrinx localization); SSEP/MEP/EMG Implants: Dural substitute (duraplasty) [/ syrinx shunt catheter], sealant Complications: None
Indications: [Age]yo [M/F] with [progressive] syringomyelia from [etiology] causing [dissociated sensory loss/weakness/pain]. The strategy was cause-directed [posterior fossa decompression for Chiari / untethering for post-traumatic block / shunt for refractory progressive syrinx]. Risks discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and neuromonitoring established. The patient was positioned prone. [Chiari: a foramen magnum decompression with duraplasty was performed to restore CSF flow.] [Post-traumatic: a laminectomy at the block level with arachnoid lysis and expansile duraplasty re-established subarachnoid CSF flow.] [Refractory syrinx: a laminectomy was performed at the maximal/thinnest point of the syrinx, a midline (or DREZ) myelotomy made under ultrasound guidance, the syrinx drained, and a small shunt catheter placed from the syrinx into the subarachnoid space.] A watertight dural closure [/ expansile duraplasty] was performed with sealant.
Closure was completed in layers. The patient was transferred with CSF-leak precautions; gradual (months) syrinx collapse was anticipated.
Postoperative Plan
- Step-down/ICU, neuro checks, CSF leak precautions, MAP support
- MRI at 3-6 months (syrinx should shrink over months — not immediately), cine flow
- Pain management (neuropathic — gabapentinoids), rehab
- DVT prophylaxis (mechanical)
- Counsel: syrinx collapse is gradual; goal is to halt progression; monitor for recurrence/shunt failure; address scoliosis (peds, ortho)
Chief-Level Case Review
Use these as the senior-level mental model for Syringomyelia — Management / Syringosubarachnoid Shunt:
- Decision point: Trajectory and hardware choice should follow the failure mode: obstruction, infection, overdrainage, loculation, slit ventricle, distal failure, or wrong pressure setting.
- Technical lever: Document the system: entry point, catheter target/depth, valve type and setting, distal site, antibiotic-impregnated hardware, and what imaging confirms placement.
- Bailout: Rescue plan is practical: poor CSF return, bloody CSF, malposition, distal access failure, abdominal/pleural complication, or inability to safely pass the catheter.
- Postop watch: Postop orders must be unambiguous: drain height/rate/max output, valve setting, clamp parameters, imaging, antibiotics, ICP/neuro checks, and overdrainage precautions.
Common Pimp Questions
Use these to pressure-test preparation for Syringomyelia — Management / Syringosubarachnoid Shunt:
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]