
Case Prep: Cervical Laminoplasty
Case / Approach Snapshot
- Anatomy at risk: level localization, cord/cauda equina, exiting and traversing roots, dura, vertebral artery or segmental vessels, esophagus/trachea/pleura/viscera by approach, and fusion/instrumentation landmarks.
- Operative steps: position and pad carefully, confirm level, expose the planned corridor, decompress neural elements, reconstruct or instrument when indicated, verify alignment/hardware, and close with attention to hematoma and wound risk; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: wrong level, durotomy, neurologic change, vertebral artery/visceral/pleural injury, graft or hardware problem, epidural hematoma, dysphagia/airway issue, and infection prevention/escalation.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with multilevel cervical spondylotic myelopathy / OPLL ([C_-C_]) with preserved lordosis planned for [open-door / French-door] cervical laminoplasty (motion-preserving posterior decompression).
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior cervical approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Cervical laminoplasty: indication, technique, complications — Weinberg DS. Journal of spine surgery (Hong Kong) 2020. PubMed
- Cervical laminoplasty — Steinmetz MP. The spine journal : official journal of the North American Spine Society 2006. PubMed
- Laminoplasty for cervical myelopathy — Ito M. Global spine journal 2012. PubMed
- Cervical Laminoplasty: Indications, Surgical Considerations, and Clinical Outcomes — Cho SK. The Journal of the American Academy of Orthopaedic Surgeons 2018. PubMed
- Cervical Laminoplasty: The History and the Future — Kurokawa R. Neurologia medico-chirurgica 2015. PubMed
- Cervical laminoplasty versus laminectomy and fusion: An umbrella review of postoperative outcomes — Jagtiani P. Neurosurgical review 2023. PubMed
- Deformity Considerations in Cervical Laminoplasty: A Narrative Review — Drain JP. Clinical spine surgery 2025. PubMed
- Cervical laminoplasty: a critical review — Ratliff JK. Journal of neurosurgery 2003. PubMed
- Cervical laminoplasty — Mehdain H. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 2014. PubMed
- Factors predicting loss of cervical lordosis following cervical laminoplasty: A critical review — Alam I. Journal of craniovertebral junction & spine 2020. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
 Fig. 2. Pre-op lateral radiograph. Source: Comparative Effectiveness of Different Types of Cervical Laminoplasty — Evidence-Based Spine-Care Journal 2013; open access.
Fig. 2. Pre-op lateral radiograph. Source: Comparative Effectiveness of Different Types of Cervical Laminoplasty — Evidence-Based Spine-Care Journal 2013; open access.
 Fig. 3. Pre-op magnetic resonance image sagittal view. Source: Comparative Effectiveness of Different Types of Cervical Laminoplasty — Evidence-Based Spine-Care Journal 2013; open access.
Fig. 3. Pre-op magnetic resonance image sagittal view. Source: Comparative Effectiveness of Different Types of Cervical Laminoplasty — Evidence-Based Spine-Care Journal 2013; open access.
 Fig. 4. Pre-op computed tomography sagittal view. Source: Comparative Effectiveness of Different Types of Cervical Laminoplasty — Evidence-Based Spine-Care Journal 2013; open access.
Fig. 4. Pre-op computed tomography sagittal view. Source: Comparative Effectiveness of Different Types of Cervical Laminoplasty — Evidence-Based Spine-Care Journal 2013; open access.
 Fig. 5. Post-op lateral radiograph. Source: Comparative Effectiveness of Different Types of Cervical Laminoplasty — Evidence-Based Spine-Care Journal 2013; open access.
Fig. 5. Post-op lateral radiograph. Source: Comparative Effectiveness of Different Types of Cervical Laminoplasty — Evidence-Based Spine-Care Journal 2013; open access.
 Figure 5. Source: Comparative Effectiveness of Different Types of Cervical Laminoplasty — Evid Based Spine Care J. 2013 Oct;4(2):105–15. doi: 10.1055/s-0033-1357361; open access.
Figure 5. Source: Comparative Effectiveness of Different Types of Cervical Laminoplasty — Evid Based Spine Care J. 2013 Oct;4(2):105–15. doi: 10.1055/s-0033-1357361; open access.
 Figure 6. Source: Comparative Effectiveness of Different Types of Cervical Laminoplasty — Evid Based Spine Care J. 2013 Oct;4(2):105–15. doi: 10.1055/s-0033-1357361; open access.
Figure 6. Source: Comparative Effectiveness of Different Types of Cervical Laminoplasty — Evid Based Spine Care J. 2013 Oct;4(2):105–15. doi: 10.1055/s-0033-1357361; open access.
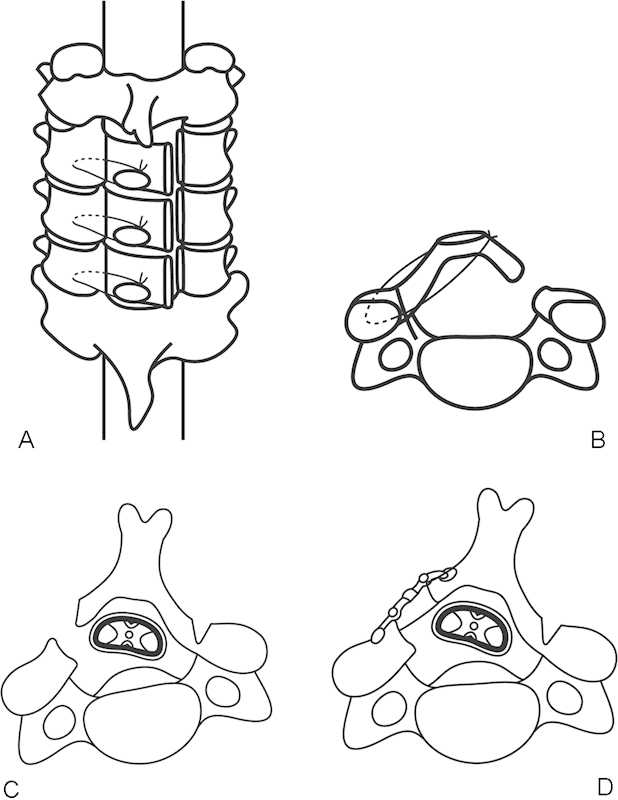 Figure 1. (A) The top view of unilateral open-door laminoplasty (Hirabayashi’s method). Three laminae are lifted bilaterally. (B) The axial view of unilateral open-door laminoplasty. The lamina is… Source: Laminoplasty for Cervical Myelopathy — Global Spine Journal 2012; open access.
Figure 1. (A) The top view of unilateral open-door laminoplasty (Hirabayashi’s method). Three laminae are lifted bilaterally. (B) The axial view of unilateral open-door laminoplasty. The lamina is… Source: Laminoplasty for Cervical Myelopathy — Global Spine Journal 2012; open access.
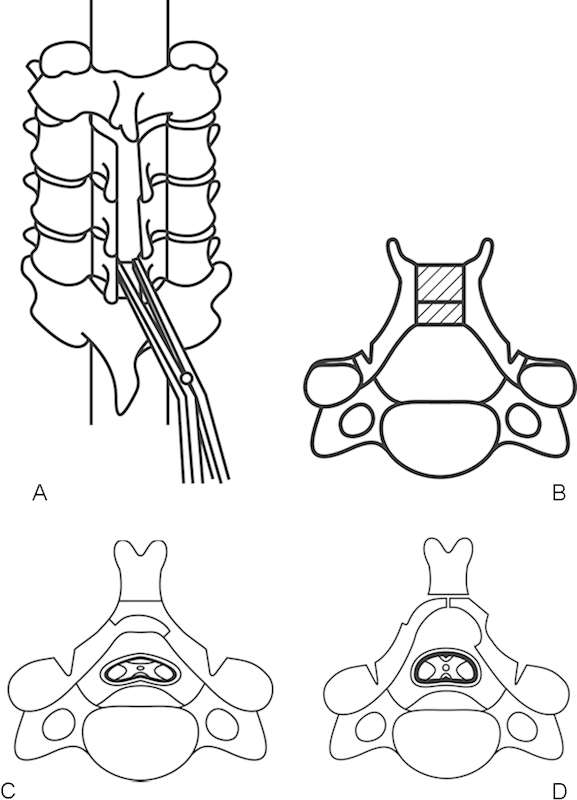 Figure 2. (A) Bilateral open-door laminoplasty. The top view of Kurokawa’s method. The spinous processes and laminae are split at the midline and opened. (B) A block of bone graft is placed… Source: Laminoplasty for Cervical Myelopathy — Global Spine Journal 2012; open access.
Figure 2. (A) Bilateral open-door laminoplasty. The top view of Kurokawa’s method. The spinous processes and laminae are split at the midline and opened. (B) A block of bone graft is placed… Source: Laminoplasty for Cervical Myelopathy — Global Spine Journal 2012; open access.
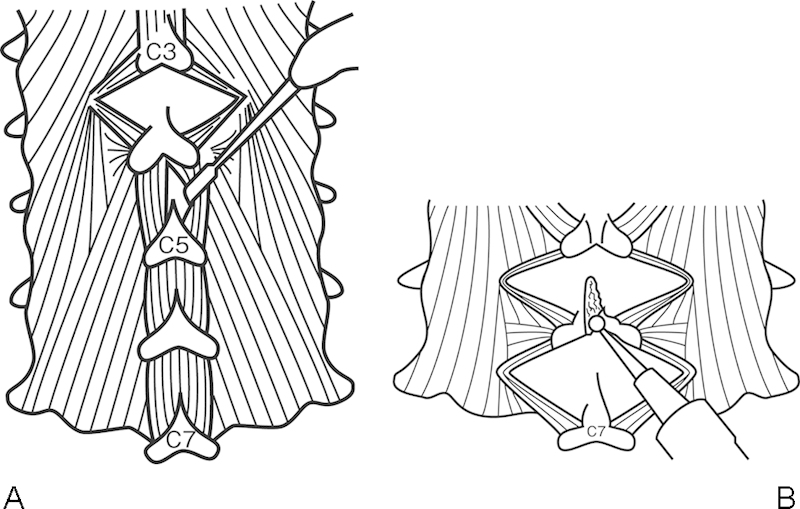 Figure 3. (A) Muscle-preservation approach for cervical laminoplasty (Shiraishi’s method). Divide the interspinalis muscles by a pair of nerve retractors. (B) Split the spinous processes with a… Source: Laminoplasty for Cervical Myelopathy — Global Spine Journal 2012; open access.
Figure 3. (A) Muscle-preservation approach for cervical laminoplasty (Shiraishi’s method). Divide the interspinalis muscles by a pair of nerve retractors. (B) Split the spinous processes with a… Source: Laminoplasty for Cervical Myelopathy — Global Spine Journal 2012; open access.
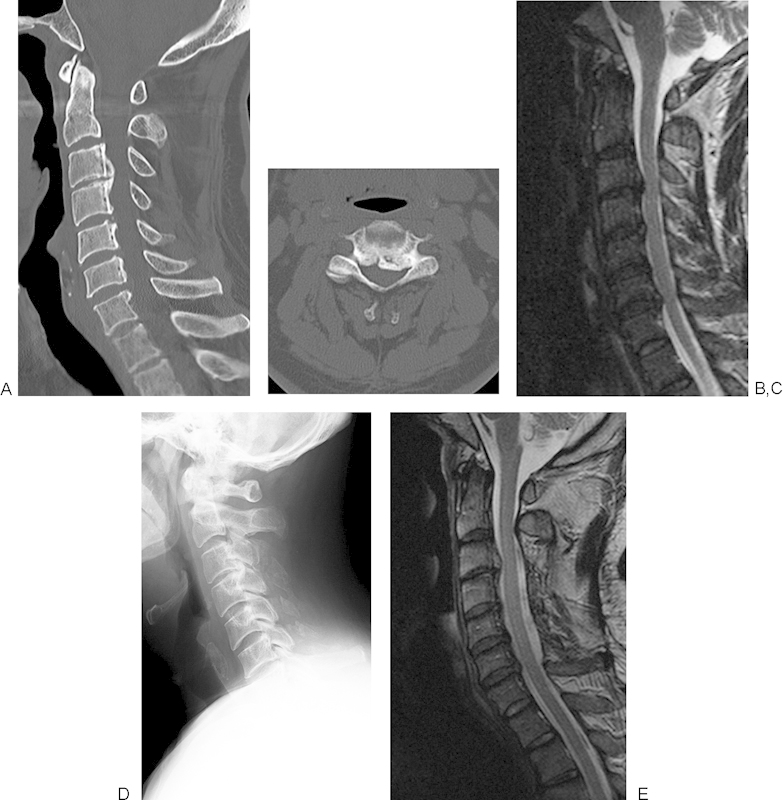 Figure 4. (A) A preoperative sagittal computed tomography (CT) image of the cervical spine of a 62-year-old man shows cervical ossification of the posterior longitudinal ligament (OPLL) from C3 to… Source: Laminoplasty for Cervical Myelopathy — Global Spine Journal 2012; open access.
Figure 4. (A) A preoperative sagittal computed tomography (CT) image of the cervical spine of a 62-year-old man shows cervical ossification of the posterior longitudinal ligament (OPLL) from C3 to… Source: Laminoplasty for Cervical Myelopathy — Global Spine Journal 2012; open access.
History of Present Illness
- Chief complaint: Cervical myelopathy from multilevel dorsal compression
- Laminoplasty advantages: decompresses multiple levels while preserving motion and avoiding fusion morbidity; lower kyphosis/instability risk than laminectomy alone
- Requires preserved lordosis (cord drifts back); avoid in kyphosis, significant neck pain (fusion may be better), or instability
Past Medical History
- Cervical alignment (lordosis required), axial neck pain severity (laminoplasty doesn’t address mechanical pain well)
- RA, instability (relative contraindications), smoking
- Standard PMH
Imaging Review
X-ray (lateral, flexion/extension)
- Lordosis preserved (key), no instability, K-line (OPLL)
MRI
- Multilevel dorsal cord compression, T2 signal, levels
CT
- OPLL, laminar/lateral mass anatomy, canal dimensions
Labs
- CBC, BMP, Coags, Type and screen, HbA1c
Neurological Examination
- Full myelopathy exam (mJOA/Nurick), myotomal/dermatomal, gait
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: radiolucent spine-capable table selected for approach, imaging, instrumentation, patient size, and alignment goals; keep abdomen free for prone cases.
- OR setup: radiolucent/Jackson table, fluoroscopy or O-arm/navigation, microscope/loupes for decompression, implant trays/graft ready for fusion, neuromonitoring for myelopathy/cord-risk cases, and postop brace plan confirmed.
- Special needs: arterial line/Foley/type-screen for long fusion/corpectomy, no long paralytic when MEPs are used, MAP/normotension for myelopathy or cord-risk cases, antibiotic redosing, and anticoagulation/DVT plan.
- Immediate postop orders: neuro checks by myotome/sensory level, airway/dysphagia watch for anterior cervical cases, CT/X-rays per construct, drain care, brace/activity orders, DVT prophylaxis timing, bowel regimen, and PT/OT mobilization.
Position
- OR table/bed: radiolucent spine-capable table selected for approach, imaging, instrumentation, patient size, and alignment goals; keep abdomen free for prone cases.
- Prone, Mayfield, neutral/slight flexion preserving lordosis, reverse Trendelenburg, shoulders taped, eyes protected
- IONM check after positioning
Technique Variants
- Open-door (Hirabayashi): hinge on one side (greenstick trough), open the other side, prop open with plates/spacers
- French-door (double-door): midline split, hinge bilaterally, open like double doors with central spacer
Key Surgical Steps (Open-door)
- Midline incision, subperiosteal exposure of laminae (preserve facet capsules/muscle attachments where possible)
- Fluoroscopic level confirmation
- Hinge side: create a partial-thickness trough at lamina-lateral mass junction (outer cortex through, inner cortex intact = greenstick hinge) with high-speed drill
- Open side: complete trough through both cortices (contralateral lamina-lateral mass junction)
- Carefully lift/open the laminar door (hinge bends), gently elevating lamina away from cord — release ligamentum/adhesions, avoid cord pressure
- Maintain the open position with mini-plates/spacers (or sutures/bone struts) at each opened level
- Confirm decompression; foraminotomy if needed
- Hemostasis, drain, layered closure
Critical Anatomy & Structures at Risk
- Spinal cord — during opening (avoid downward pressure), epidural bleeding
- C5 nerve root — C5 palsy (as with laminectomy)
- Hinge fracture (complete fracture → instability of that door)
- Facets (preserve — avoid fusion/instability)
Equipment
- High-speed drill (key for troughs/hinge), Kerrison
- Laminoplasty plates/spacers (open-door) or bone strut/spacer (French-door), fluoroscopy
- Hemostatic agents, drain
Monitoring
- SSEPs, MEPs, EMG; check after positioning and during door opening
Anesthesia
- MAP > 85, no paralytic (IONM), prone precautions (eyes), TXA
Potential Complications
- C5 palsy (deltoid/biceps weakness, usually recovers)
- Hinge fracture / door closure (reclosure → recurrent stenosis)
- Axial neck pain, reduced ROM/stiffness, kyphosis
- Epidural hematoma, CSF leak, infection, inadequate decompression
Operative Note Template
Preoperative Diagnosis: Multilevel cervical spondylotic myelopathy [/ OPLL] [C_-C_] with preserved lordosis
Postoperative Diagnosis: Same
Procedure: [Open-door (Hirabayashi) / French-door] cervical laminoplasty [C_-C_]
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Adjuncts: High-speed drill, fluoroscopy; SSEP/MEP/EMG Implants: Laminoplasty mini-plates/spacers Monitoring: SSEP/MEP — stable Complications: None
Indications: [Age]yo [M/F] with multilevel cervical myelopathy and preserved lordosis, suitable for motion-preserving posterior decompression. Risks (C5 palsy, axial pain, hinge fracture) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and neuromonitoring established with stable baselines after prone positioning in Mayfield (neutral lordosis preserved). A midline exposure of the laminae [C_-C_] was performed and levels confirmed.
A hinge trough (partial-thickness greenstick) was created at one lamina–lateral mass junction and an open-side trough (full-thickness) at the contralateral junction with the high-speed drill. The laminar “door” was gently opened, elevating the laminae off the cord and releasing adhesions, and maintained open with mini-plates/spacers at each level. Decompression was confirmed and foraminotomies performed as needed. The facets were preserved to avoid instability/fusion.
Hemostasis was obtained, a drain placed, and closure performed in layers. The patient was awakened [at baseline] and transferred with C5-palsy precautions.
Postoperative Plan
- Step-down/floor, neuro checks q2h (C5 palsy watch)
- Early mobilization, soft collar briefly, early ROM exercises (reduce stiffness)
- X-rays POD1, drain management, DVT prophylaxis
- Pain control, follow-up imaging; counsel re: axial pain/stiffness and C5 palsy
Chief-Level Case Review
Use these as the senior-level mental model for Cervical Laminoplasty:
- Decision point: Localize twice and instrument once: numbering, transitional anatomy, prior hardware, rib count, navigation dataset, and fluoroscopic level confirmation are mandatory.
- Technical lever: Positioning is treatment: table choice, abdomen-free prone setup, alignment goals, shoulders/hips, eyes/plexus pressure, neuromonitoring baselines, and fluoroscopic access all change the case.
- Bailout: Protect neural elements by sequence: decompression before correction when needed, MAP support for cord risk, no long paralytic with MEPs, and immediate response to signal change.
- Postop watch: Finish with construct logic: decompression adequacy, screw purchase, alignment, fusion bed/graft, drain plan, brace/activity orders, postop CT/X-rays, and DVT timing.
Common Pimp Questions
Use these to pressure-test preparation for Cervical Laminoplasty:
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]