
Case Prep: Odontoid (Type II) Fracture Fixation
Case / Approach Snapshot
- Anatomy at risk: unstable columns, cord/roots, dura, vertebral artery or great-vessel/visceral structures by level, fracture lines, and fixation corridors.
- Operative steps: protect the spine during transfer/positioning, confirm levels and reduction goals, decompress when indicated, instrument/reconstruct stability, verify alignment and hardware, and plan ICU/brace/rehab needs; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: neurologic deterioration, reduction failure, vascular/visceral injury, durotomy, blood loss, hardware pullout, infection, and staged anterior/posterior stabilization.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a type [II/III] odontoid fracture ([Anderson-D’Alonzo]) following [fall/MVC] planned for [anterior odontoid screw / posterior C1-C2 fusion].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior cervical approach — posterior C1-C2 fixation/exposure principles when anterior odontoid screw is not the chosen strategy.
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Predicting Mortality Following Odontoid Fracture Fixation in Elderly Patients: CAADS-16 Score — ElNemer W. Global spine journal 2025. PubMed
- Outcomes of Odontoid Process Fracture Surgery — Sowa D. Ortopedia, traumatologia, rehabilitacja 2023. PubMed
- Odontoid process type II and III fracture fixation using bone allograft screws versus cannulated screws: a biomechanical study — Benca E. Archives of orthopaedic and trauma surgery 2025. PubMed
- Biomechanics of odontoid fracture fixation. Comparison of the one- and two-screw technique — Sasso R. Spine 1993. PubMed
- Percutaneous anterior odontoid screw fixation technique. A new instrument and a cadaveric study — Kazan S. Acta neurochirurgica 1999. PubMed
- Computed tomographic evaluation of odontoid process: implications for anterior screw fixation of odontoid fractures in an adult population — Daher MT. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 2011. PubMed
- Cervical Spine Navigation and Enabled Robotics: A New Frontier in Minimally Invasive Surgery — Lebl DR. HSS journal : the musculoskeletal journal of Hospital for Special Surgery 2021. PubMed
- Medical devices of the head, neck, and spine — Hunter TB. Radiographics : a review publication of the Radiological Society of North America, Inc 2004. PubMed
- Salvage of failed odontoid fixation through anterior C1/C2 transarticular screws — Salem KM. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 2015. PubMed
- Odontoid Fusion — Walker CT. Acta neurochirurgica. Supplement 2019. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
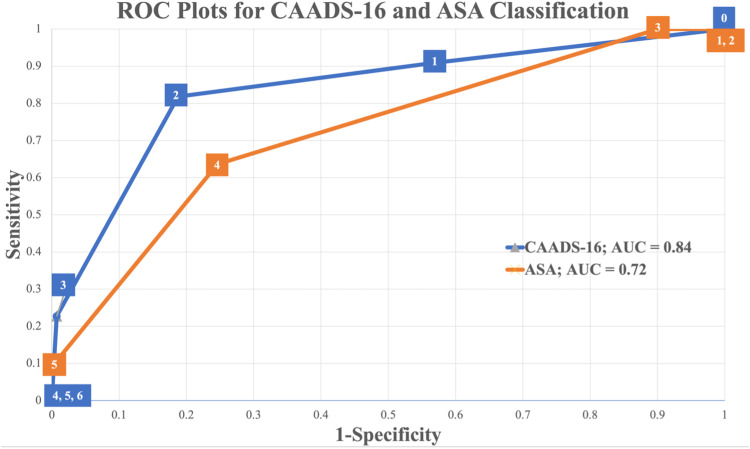 Figure 2.. ROC curves for CAADS-16 score and ASA classification. The AUC is displayed in the legend, and the cut off values are represented in the squares of the curve. The ASA classification was… Source: Predicting Mortality Following Odontoid Fracture Fixation in Elderly Patients: CAADS-16 Score — Global Spine Journal 2023; CC BY-NC-ND.
Figure 2.. ROC curves for CAADS-16 score and ASA classification. The AUC is displayed in the legend, and the cut off values are represented in the squares of the curve. The ASA classification was… Source: Predicting Mortality Following Odontoid Fracture Fixation in Elderly Patients: CAADS-16 Score — Global Spine Journal 2023; CC BY-NC-ND.
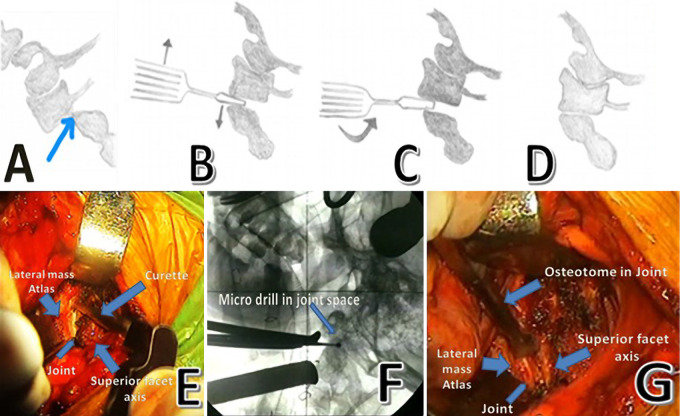 FIG. 1.. A: Identifying the joint space below the lateral mass of the atlas (anatomical drawing). B: Inserting osteotome for manipulation (anatomical drawing). C: Rotating the osteotome to open… Source: Unstable odontoid fractures: technical appraisal of anterior extrapharyangeal open reduction internal fixation for irreducible unstable odontoid fractures. Patient series — Journal of Neurosurgery: Case Lessons 2021; CC BY-NC-ND.
FIG. 1.. A: Identifying the joint space below the lateral mass of the atlas (anatomical drawing). B: Inserting osteotome for manipulation (anatomical drawing). C: Rotating the osteotome to open… Source: Unstable odontoid fractures: technical appraisal of anterior extrapharyangeal open reduction internal fixation for irreducible unstable odontoid fractures. Patient series — Journal of Neurosurgery: Case Lessons 2021; CC BY-NC-ND.
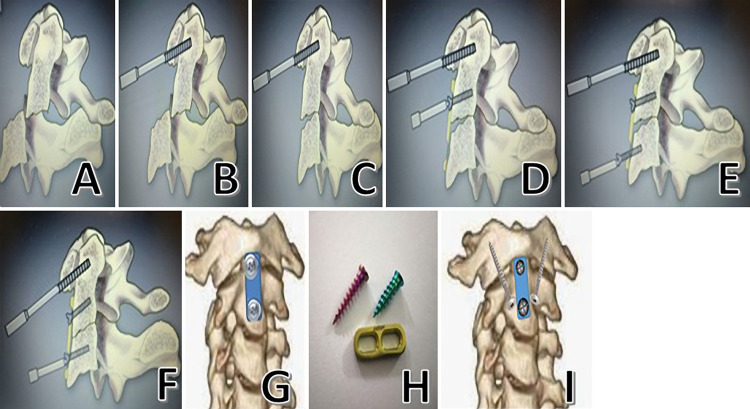 FIG. 2.. A: Posteriorly displaced impacted fracture (anatomical image). B: Impaling the anterior arch of the atlas and distal fracture fragment with a tap (anatomical image). C: Repositioning the… Source: Unstable odontoid fractures: technical appraisal of anterior extrapharyangeal open reduction internal fixation for irreducible unstable odontoid fractures. Patient series — Journal of Neurosurgery: Case Lessons 2021; CC BY-NC-ND.
FIG. 2.. A: Posteriorly displaced impacted fracture (anatomical image). B: Impaling the anterior arch of the atlas and distal fracture fragment with a tap (anatomical image). C: Repositioning the… Source: Unstable odontoid fractures: technical appraisal of anterior extrapharyangeal open reduction internal fixation for irreducible unstable odontoid fractures. Patient series — Journal of Neurosurgery: Case Lessons 2021; CC BY-NC-ND.
History of Present Illness
- Chief complaint: Neck pain after trauma; may have minimal/no deficit (or high cervical cord injury)
- Mechanism, neurological status, associated injuries (especially elderly fall — common)
- Anderson-D’Alonzo: Type I (tip, stable), Type II (base — most common, high nonunion), Type III (into body, better union)
- Displacement, angulation, direction; chronicity
Imaging Review
CT cervical (thin-cut, reconstructions)
- Fracture type, displacement, angulation (anterior vs posterior), comminution
- C1-C2 anatomy for screw planning (vertebral artery course, C2 pedicle/pars, C1 lateral mass)
- Transverse atlantal ligament integrity (CT/MRI)
MRI
- Ligament integrity (transverse ligament — if disrupted, screw alone insufficient), cord signal, soft tissue
CTA
- Vertebral artery anatomy (high-riding VA, anomalies — affects C2 screw safety)
X-ray (flexion/extension if stability unclear, with caution)
Labs
- CBC, BMP, Coags, Type and screen
Neurological Examination
- Full exam (high cervical — respiratory, all extremities), document deficits
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- OR setup: spine table with log-roll precautions, fluoroscopy/O-arm/navigation, traction/Mayfield when cervical, posterior/anterior implant trays, decompression instruments, cell saver/blood for large constructs, and IONM before positioning when feasible.
- Special needs: arterial line, Foley, type/cross, MAP augmentation for acute SCI per local protocol, no long paralytic when MEPs are needed, anticoagulation/reversal plan, and airway strategy for unstable cervical injuries.
- Immediate postop orders: serial ASIA/neuro checks, MAP goal/duration if SCI, CT/X-rays for hardware/alignment, brace/collar orders, drain care, DVT prophylaxis timing, bowel/bladder/skin care, and early rehab/SCI consult.
Procedure Selection
- Anterior odontoid screw: preserves C1-C2 rotation; for reducible Type II fractures with favorable oblique pattern (anterosuperior-posteroinferior), intact transverse ligament, good bone; contraindicated in osteoporosis, comminution, irreducible, unfavorable fracture line, disrupted transverse ligament, barrel chest/kyphosis (trajectory)
- Posterior C1-C2 fusion (Goel-Harms C1 lateral mass + C2 pedicle screws; or Magerl transarticular): for irreducible, comminuted, transverse ligament disruption, nonunion, poor bone; sacrifices rotation
- Elderly: rising use of surgical fixation vs hard collar (nonunion common but fibrous union often tolerated)
Position
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- Anterior screw: supine, neck slightly extended, Mayfield/traction for reduction, biplanar fluoroscopy (AP + lateral, open-mouth), radiolucent setup
- Posterior C1-C2: prone, Mayfield, neck neutral, reduce, fluoroscopy/navigation
Key Surgical Steps (Anterior Odontoid Screw)
- Reduce fracture (positioning/traction), confirm on fluoroscopy
- Anterior cervical (Smith-Robinson-type) exposure to C2-C3 level, trajectory from the anteroinferior C2 body
- Entry at anteroinferior C2 endplate, guidewire up the odontoid across the fracture to the tip under biplanar fluoroscopy
- Cannulated drill, tap, place lag screw (1 or 2 screws) to compress fracture across the fracture line into the dens tip
- Confirm compression/reduction and screw position (both fluoro planes)
- Closure
Key Surgical Steps (Posterior C1-C2, Goel-Harms)
- Prone, expose C1 posterior arch and C2
- C1 lateral mass screws (entry below the posterior arch, protect C2 nerve root/venous plexus)
- C2 pedicle/pars screws (assess VA on CTA — high-riding VA contraindicates pedicle screw → use pars/translaminar)
- Reduce C1 on C2, place rods, lock
- Decorticate, bone graft (autograft/allograft) for fusion
- Closure
Critical Anatomy & Structures at Risk
- Vertebral arteries (C2 screw trajectory — high-riding VA; C1-C2 region) — catastrophic
- Spinal cord / cervicomedullary junction — high cervical, narrow margin
- C2 nerve root / venous plexus (C1 lateral mass screw — bleeding)
- Esophagus/airway (anterior approach), hypoglossal/superior laryngeal nerves (high anterior)
- Transverse atlantal ligament (competence determines construct)
Equipment
- Anterior odontoid screw set (cannulated lag screws) OR C1-C2 posterior screw/rod system
- Biplanar fluoroscopy / navigation, traction/reduction tools
- Bone graft (posterior fusion), microscope/loupes
Monitoring
- SSEPs/MEPs (high cervical), especially during positioning/reduction; awake fiberoptic intubation if unstable/myelopathic
Anesthesia
- Awake fiberoptic intubation (unstable C-spine, avoid hyperextension), MAP support, arterial line, in-line stabilization
Potential Complications
- Vertebral artery injury (C2 screw), cord/cervicomedullary injury
- Nonunion (esp. Type II, elderly, anterior screw), screw pullout/malposition
- Dysphagia/airway (anterior), C2 neuralgia, loss of rotation (posterior fusion)
- Hardware failure, adjacent issues
Operative Note Template
Preoperative Diagnosis: Type [II] odontoid (dens) fracture [displaced ___ mm], craniocervical instability
Postoperative Diagnosis: Same
Procedure: [Anterior odontoid screw fixation / Posterior C1-C2 instrumented fusion (Goel-Harms — C1 lateral mass + C2 pedicle screws)] for type [II] odontoid fracture
Surgeon / Assistant: Anesthesia: General endotracheal (awake fiberoptic intubation) EBL / Fluids: Implants: [Cannulated lag odontoid screw(s) / C1 lateral mass and C2 pedicle screws and rods — system/sizes; bone graft] Monitoring: SSEP / MEP — stable [note any change with positioning/reduction] Complications: None
Indications: [Age]yo [M/F] with a type II odontoid fracture after [mechanism], [reducible, intact transverse ligament, favorable fracture line → anterior screw / irreducible/comminuted/disrupted transverse ligament/poor bone → posterior C1-C2 fusion]. CTA showed [no high-riding VA / VA anatomy permitting planned screws]. Risks/benefits/alternatives (including collar immobilization and nonunion risk) discussed.
Description of Procedure: After consent and time-out, awake fiberoptic intubation was performed to protect the unstable cervical spine, and neuromonitoring baselines were confirmed before and after positioning. The fracture was reduced [with positioning/traction] and verified on biplanar fluoroscopy.
Final fluoroscopy confirmed satisfactory reduction and hardware. Neuromonitoring was stable throughout. Closure was performed in layers [± drain]. The patient was awakened, neurologically [at baseline], and transferred in stable condition.
Postoperative Plan
- ICU/step-down, neuro checks (high cervical — respiratory), airway monitoring (anterior — swelling)
- CT postop (screw position, reduction), cervical collar per construct/surgeon
- DVT prophylaxis, pain control, dysphagia/aspiration precautions (anterior)
- Follow-up CT for union; counsel re: nonunion risk; flexion/extension films later
Chief-Level Case Review
Use these as the senior-level mental model for Odontoid (Type II) Fracture Fixation:
- Decision point: Treat physiology while preparing the room: airway, reversal, transfusion, ICP/CPP, sodium/osmolality, temperature, and repeat imaging drive timing as much as the scan finding.
- Technical lever: Know the operative priority: decompression, hemorrhage control, debridement, dural closure, reconstruction, stabilization, or contamination control.
- Bailout: Plan for swelling and coagulopathy: bone flap decision, duraplasty size, drain/EVD need, hemostatic adjuncts, and ICU handoff should be decided early.
- Postop watch: Postop failure modes are predictable: expanding hematoma, malignant edema, seizure, infection, CSF leak, venous sinus injury, and missed associated spine/vascular injury.
Common Pimp Questions
Use these to pressure-test preparation for Odontoid (Type II) Fracture Fixation:
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]