
Case Prep: Posterior Cervical Foraminotomy (Laminoforaminotomy)
Case / Approach Snapshot
- Anatomy at risk: level localization, cord/cauda equina, exiting and traversing roots, dura, vertebral artery or segmental vessels, esophagus/trachea/pleura/viscera by approach, and fusion/instrumentation landmarks.
- Operative steps: position and pad carefully, confirm level, expose the planned corridor, decompress neural elements, reconstruct or instrument when indicated, verify alignment/hardware, and close with attention to hematoma and wound risk; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: wrong level, durotomy, neurologic change, vertebral artery/visceral/pleural injury, graft or hardware problem, epidural hematoma, dysphagia/airway issue, and infection prevention/escalation.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [left/right] [C_] cervical radiculopathy due to [foraminal soft disc / foraminal spondylosis] at [C_-C_] planned for [open/minimally invasive] posterior cervical laminoforaminotomy (motion-preserving, no fusion).
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior cervical approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Posterior Endoscopic Cervical Foraminotomy — Bhatia S. Neurosurgery clinics of North America 2020. PubMed
- Posterior Cervical Foraminotomy Via Full-Endoscopic Versus Microendoscopic Approach for Radiculopathy: A Systematic Review and Meta-analysis — Wu PF. Pain physician 2019. PubMed
- Minimally invasive posterior cervical foraminotomy versus the anterior transcorporeal approach for cervical radiculopathy: a systematic review and meta-analysis — Rajjoub R. Journal of neurosurgery. Spine 2024. PubMed
- Cervical radiculopathy — Iyer S. Current reviews in musculoskeletal medicine 2016. PubMed
- Impact of Posterior Cervical Foraminotomy Before or After Cervical Disk Replacement: Current Evidence — Young MW. Clinical spine surgery 2023. PubMed
- Endoscopic Posterior Cervical Foraminotomy and Discectomy — Raad M. JBJS essential surgical techniques 2025. PubMed
- Cervical posterior foraminotomy: how i do it — Cossu G. Acta neurochirurgica 2020. PubMed
- Posterior foraminotomy for lateral cervical disc herniation — Mehren C. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 2019. PubMed
- Minimally invasive posterior cervical foraminotomy versus anterior cervical fusion and arthroplasty: Systematic review and updated meta-analysis — Fang H. Brain & spine 2024. PubMed
- Posterior Cervical Foraminotomy Compared with Anterior Cervical Discectomy with Fusion for Cervical Radiculopathy: Two-Year Results of the FACET Randomized Noninferiority Study — Simões de Souza NF. The Journal of bone and joint surgery. American volume 2024. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
 Figure 1. The position of a patient during surgery. Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
Figure 1. The position of a patient during surgery. Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
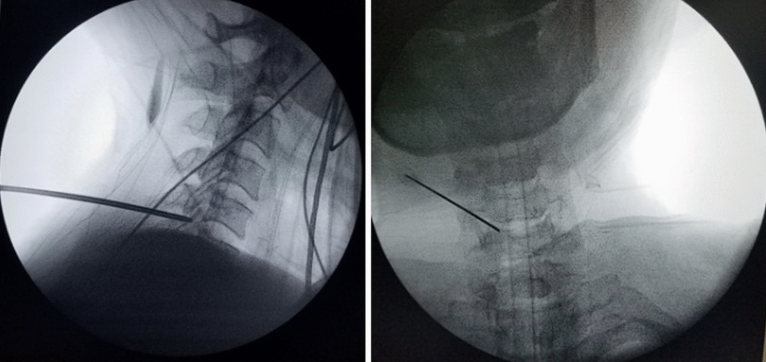 Figure 2. Under fluoroscopic control, the guide wires are inserted through the posterior cervical musculature with the tip directed to the operative disc space. Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
Figure 2. Under fluoroscopic control, the guide wires are inserted through the posterior cervical musculature with the tip directed to the operative disc space. Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
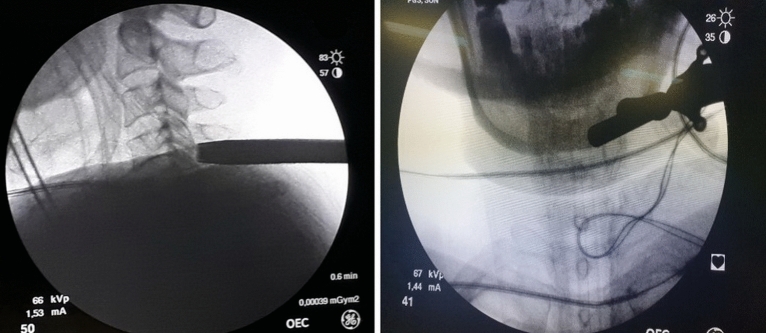 Figure 3. Working channel Insertion. On a string conductor, tubular reamers of increasing diameter were introduced, on which a working cannula with a beveled cut with an external diameter of 7.5… Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
Figure 3. Working channel Insertion. On a string conductor, tubular reamers of increasing diameter were introduced, on which a working cannula with a beveled cut with an external diameter of 7.5… Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
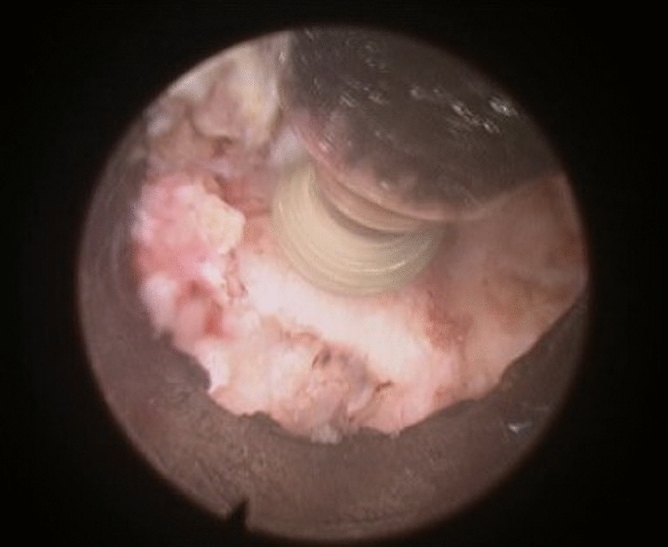 Figure 4. Bone Resection. Laminotomy and facetectomy are performed with 3.0 mm diamond boron, from “V-point” to the periphery. Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
Figure 4. Bone Resection. Laminotomy and facetectomy are performed with 3.0 mm diamond boron, from “V-point” to the periphery. Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
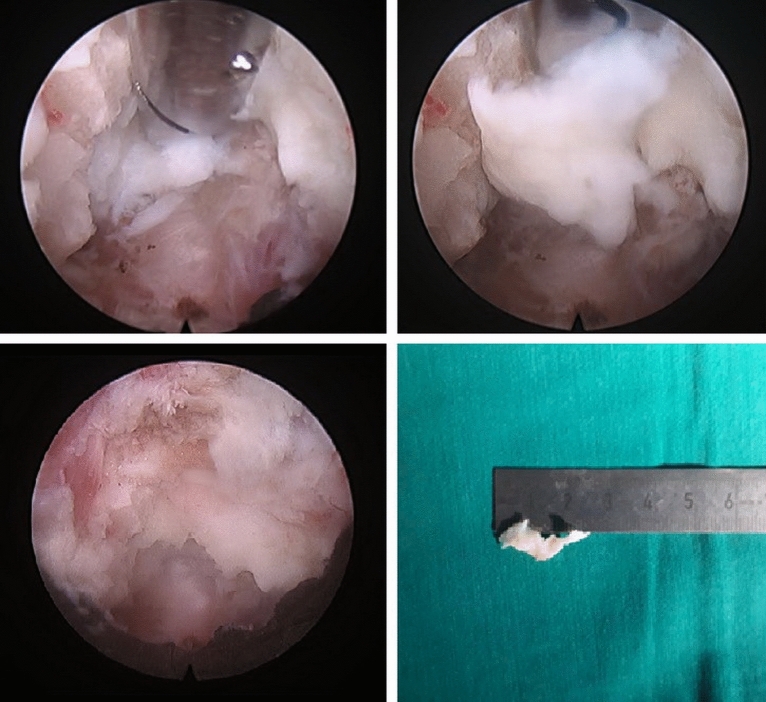 Figure 5. Preparation and removal of the herniated material. Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
Figure 5. Preparation and removal of the herniated material. Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
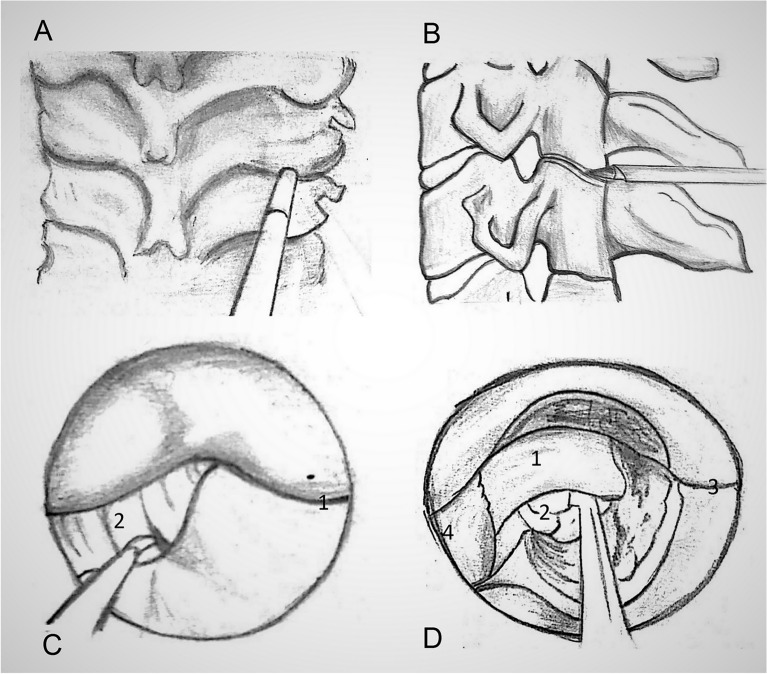 Figure 6. Surgical diagrams for Endoscopic Posterior Cervical Foraminotomy and Discectomy techniques: A and B localize of working cannula. C The facet joint is identified by removing the overlying… Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
Figure 6. Surgical diagrams for Endoscopic Posterior Cervical Foraminotomy and Discectomy techniques: A and B localize of working cannula. C The facet joint is identified by removing the overlying… Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
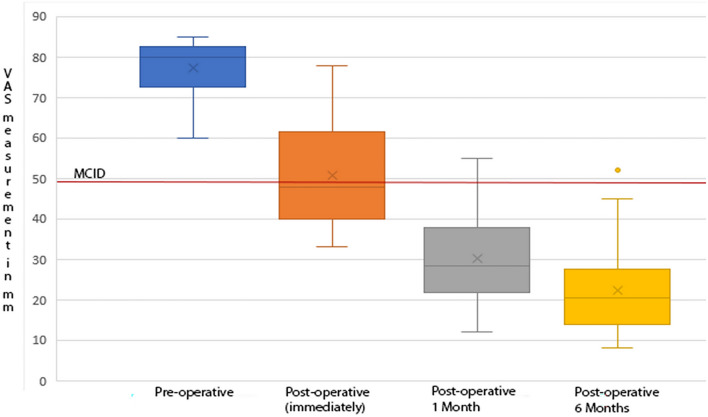 Figure7. Neck pain intensity on visual analogue scale (VAS- Neck) before and after surgery. Minimal clinically important differences (MCID) = 28 mm. Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
Figure7. Neck pain intensity on visual analogue scale (VAS- Neck) before and after surgery. Minimal clinically important differences (MCID) = 28 mm. Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
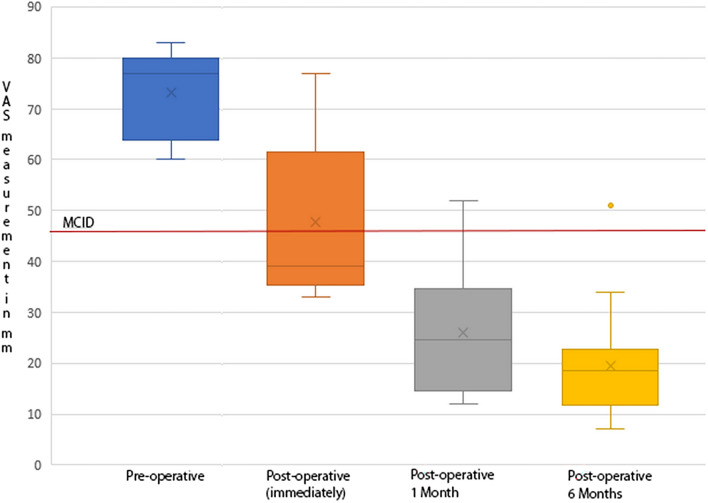 Figure 8. Arm pain intensity on visual analogue scale (VAS- Arm) before and after surgery. Minimal clinically important differences (MCID) = 26 mm. Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
Figure 8. Arm pain intensity on visual analogue scale (VAS- Arm) before and after surgery. Minimal clinically important differences (MCID) = 26 mm. Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
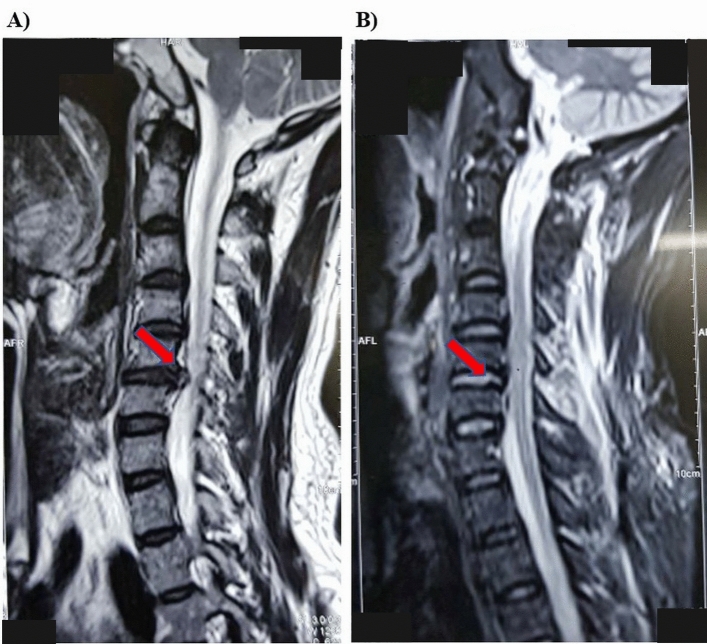 Figure 9. Herniation of C5-6 right. Before (A) and after (B) operation (male, 32 years old). Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
Figure 9. Herniation of C5-6 right. Before (A) and after (B) operation (male, 32 years old). Source: The first experience with fully endoscopic posterior cervical foraminotomy and discectomy for radiculopathy performed in Viet Duc University Hospital — Scientific Reports 2022; CC BY.
 Figure 10. Source: Minimally invasive tubular access for posterior cervical foraminotomy — Surg Neurol Int. 2015 May 19;6:81. doi: 10.4103/2152-7806.157308; CC BY-NC-SA.
Figure 10. Source: Minimally invasive tubular access for posterior cervical foraminotomy — Surg Neurol Int. 2015 May 19;6:81. doi: 10.4103/2152-7806.157308; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Unilateral radicular arm pain in [C_] distribution, dermatomal
- Failed conservative management
- Ideal: posterolateral/foraminal soft disc or foraminal stenosis causing single-level unilateral radiculopathy — posterior decompression preserves motion, avoids fusion and anterior approach risks
- Not ideal: central disc, myelopathy, kyphosis, axial-dominant pain, instability
Past Medical History
- Standard PMH, prior cervical surgery, smoking
Imaging Review
MRI
- Foraminal/posterolateral compression at [C_-C_], lateralized to symptomatic side, exclude central compression/myelopathy
CT
- Foraminal bony stenosis, uncovertebral/facet osteophytes
X-ray (flexion/extension)
- Alignment, no instability
Labs
- CBC, BMP, Coags, Type and screen
Neurological Examination
- Focused [C_] myotome/dermatome/reflex, Spurling test, rule out myelopathy
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: Wilson frame, Andrews/knee-chest frame, or Jackson/open-frame table by surgeon preference; flexion opens the interlaminar window and the abdomen must hang free.
- OR setup: radiolucent/Jackson table, fluoroscopy or O-arm/navigation, microscope/loupes for decompression, implant trays/graft ready for fusion, neuromonitoring for myelopathy/cord-risk cases, and postop brace plan confirmed.
- Special needs: arterial line/Foley/type-screen for long fusion/corpectomy, no long paralytic when MEPs are used, MAP/normotension for myelopathy or cord-risk cases, antibiotic redosing, and anticoagulation/DVT plan.
- Immediate postop orders: neuro checks by myotome/sensory level, airway/dysphagia watch for anterior cervical cases, CT/X-rays per construct, drain care, brace/activity orders, DVT prophylaxis timing, bowel regimen, and PT/OT mobilization.
Position
- OR table/bed: Wilson frame, Andrews/knee-chest frame, or Jackson/open-frame table by surgeon preference; flexion opens the interlaminar window and the abdomen must hang free.
- Prone (Mayfield) or sitting (some surgeons — less bleeding, but VAE risk); neck flexed; reverse Trendelenburg
- IONM optional
Approach: Posterior, Tubular (MIS) or Open Midline/Paramedian
Key Surgical Steps
- Fluoroscopic level localization
- MIS: paramedian stab, sequential tubular dilators docked on the lamina-facet junction of the symptomatic side; Open: small midline/paramedian incision, unilateral subperiosteal dissection
- Identify the “V-point” — junction of superior and inferior laminae at the medial facet
- Laminoforaminotomy: high-speed drill + Kerrison to remove medial edge of the lamina and medial ~1/3 of the facet (preserve > 50% of facet to avoid instability) over the exiting nerve root
- Identify and decompress the exiting nerve root; follow it into the foramen, remove osteophyte/foraminal stenosis
- Soft disc: gently retract the root superiorly, remove the disc fragment from the axilla/under the root (minimal root retraction — root is taut)
- Confirm root is decompressed and mobile
- Hemostasis (epidural veins — bipolar/Gelfoam), closure (tube removed; minimal closure for MIS)
Critical Anatomy & Structures at Risk
- Exiting nerve root — gentle handling, taut root
- Vertebral artery (anterior to foramen — do not drill too far ventral/lateral)
- Spinal cord/dura (medial — avoid)
- Facet joint — preserve > 50% (instability if over-resected)
- Epidural venous plexus (bleeding)
Equipment
- Tubular retractor system (MIS) or standard retractors
- High-speed drill, fine Kerrison rongeurs, nerve hooks, micro-instruments
- Fluoroscopy, bipolar, hemostatic agents, microscope/loupes/endoscope
Monitoring
- Optional EMG/SSEP; precordial Doppler if sitting
Anesthesia
- General; if sitting → VAE precautions; standard
Potential Complications
- Nerve root injury (retraction)
- Vertebral artery injury (over-ventral drilling)
- CSF leak (dural injury), epidural hematoma
- Instability (excess facet removal), inadequate decompression/recurrence
- VAE (sitting)
Operative Note Template
Preoperative Diagnosis: [Left/Right] [C_] cervical radiculopathy from foraminal [soft disc/spondylosis] at [C_-C_]
Postoperative Diagnosis: Same
Procedure: [Left/Right] [minimally invasive] posterior cervical laminoforaminotomy at [C_-C_] [with discectomy]
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Tubular retractor (if MIS), high-speed drill, fluoroscopy, microscope; [EMG] Implants: None Complications: None
Indications: [Age]yo [M/F] with unilateral [C_] radiculopathy from foraminal/posterolateral compression at [C_-C_], refractory to conservative care — ideal for motion-preserving posterior foraminotomy. Risks (root/VA injury, instability if over-resection) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and the patient positioned prone in Mayfield. The level was localized fluoroscopically. [MIS: sequential tubular dilators were docked on the lamina-facet junction; / Open: a small paramedian exposure was performed.] The V-point (junction of superior/inferior laminae at the medial facet) was identified, and a facet-preserving laminoforaminotomy (removing the medial ~1/3 of the facet, preserving >50%) was performed over the exiting [C_] root with the drill and fine Kerrisons.
The exiting nerve root was decompressed into the foramen and any foraminal osteophyte addressed; [a disc fragment was removed from the axilla with minimal root retraction]. The root was confirmed free and mobile. Hemostasis of the epidural plexus was obtained.
The tube was removed [/ minimal closure performed]. The patient was awakened with [improved] arm symptoms and discharged [same day/overnight].
Postoperative Plan
- Same-day or overnight; neuro checks (arm function)
- No collar/fusion; early mobilization
- Pain control, activity as tolerated
- Follow-up 2-4 weeks; expect good radicular pain relief, motion preserved
Chief-Level Case Review
Use these as the senior-level mental model for Posterior Cervical Foraminotomy (Laminoforaminotomy):
- Decision point: Localize twice and instrument once: numbering, transitional anatomy, prior hardware, rib count, navigation dataset, and fluoroscopic level confirmation are mandatory.
- Technical lever: Positioning is treatment: table choice, abdomen-free prone setup, alignment goals, shoulders/hips, eyes/plexus pressure, neuromonitoring baselines, and fluoroscopic access all change the case.
- Bailout: Protect neural elements by sequence: decompression before correction when needed, MAP support for cord risk, no long paralytic with MEPs, and immediate response to signal change.
- Postop watch: Finish with construct logic: decompression adequacy, screw purchase, alignment, fusion bed/graft, drain plan, brace/activity orders, postop CT/X-rays, and DVT timing.
Common Pimp Questions
Use these to pressure-test preparation for Posterior Cervical Foraminotomy (Laminoforaminotomy):
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]