
Case Prep: Traumatic Central Cord Syndrome
Case / Approach Snapshot
- Anatomy at risk: unstable columns, cord/roots, dura, vertebral artery or great-vessel/visceral structures by level, fracture lines, and fixation corridors.
- Operative steps: protect the spine during transfer/positioning, confirm levels and reduction goals, decompress when indicated, instrument/reconstruct stability, verify alignment and hardware, and plan ICU/brace/rehab needs; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: neurologic deterioration, reduction failure, vascular/visceral injury, durotomy, blood loss, hardware pullout, infection, and staged anterior/posterior stabilization.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with acute traumatic central cord syndrome following [hyperextension injury / fall / MVC] [on a background of cervical spondylosis] with [upper > lower extremity weakness] planned for [timing-dependent] cervical decompression [± fusion].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Posterior cervical approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Traumatic Central Cord Syndrome — Carr MT. Clinical spine surgery 2024. PubMed
- Traumatic central cord Syndrome: An integrated neurosurgical and neurocritical care perspective — Martínez-Palacios K. Brain & spine 2025. PubMed
- Traumatic central cord syndrome — Wyndaele JJ. Spinal cord 2010. PubMed
- Elderly traumatic central cord syndrome in the USA: a review of management and outcomes — Phelps RR. Journal of neurosurgical sciences 2021. PubMed
- Treatment of acute traumatic central cord syndrome: a score-based approach based on the literature — Kumar AA. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 2023. PubMed
- Acute traumatic central cord syndrome: a comprehensive review — Molliqaj G. Neuro-Chirurgie 2014. PubMed
- [Acute Traumatic Central Cord Syndrome: Etiology, Pathophysiology, Clinical Manifestation, and Treatment] — Tosic L. Praxis 2021. PubMed
- Early versus late surgical decompression for patients with acute traumatic central cord syndrome: a systematic review and meta-analysis — Sattari SA. The spine journal : official journal of the North American Spine Society 2024. PubMed
- Management of Acute Traumatic Central Cord Syndrome: A Narrative Review — Divi SN. Global spine journal 2019. PubMed
- Surgical intervention ≤ 24 hours versus > 24 hours after injury for the management of acute traumatic central cord syndrome: a systematic review and meta-analysis — Bin-Alamer O. Journal of neurosurgery. Spine 2024. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
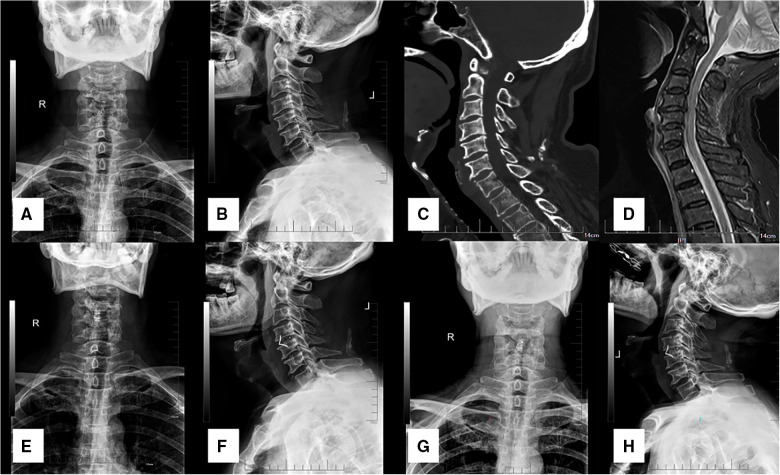 Figure 1. A 60-year-old male patient diagnosed with TCCS. (A,B) preoperative A-P and lateral x-ray showing the slight degenerative change of cervical spine with relative normal curvature, and… Source: The clinical efficacy of anterior cervical discectomy and fusion with ROI-C device vs. plate-cage in managing traumatic central cord syndrome — Frontiers in Surgery 2023; CC BY.
Figure 1. A 60-year-old male patient diagnosed with TCCS. (A,B) preoperative A-P and lateral x-ray showing the slight degenerative change of cervical spine with relative normal curvature, and… Source: The clinical efficacy of anterior cervical discectomy and fusion with ROI-C device vs. plate-cage in managing traumatic central cord syndrome — Frontiers in Surgery 2023; CC BY.
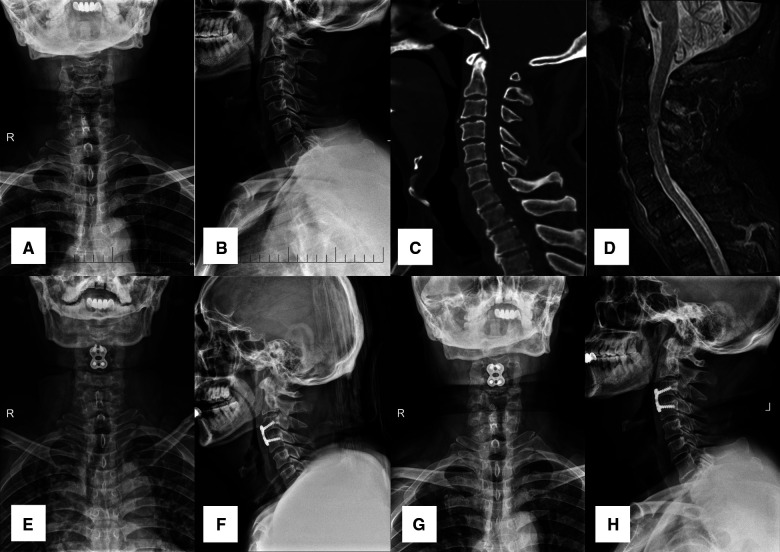 Figure 2. A 56-year-old male patient diagnosed with TCCS. (A,B) preoperative A-P and lateral X-ray images showing the slight degenerative change of cervical spine with relative normal curvature,… Source: The clinical efficacy of anterior cervical discectomy and fusion with ROI-C device vs. plate-cage in managing traumatic central cord syndrome — Frontiers in Surgery 2023; CC BY.
Figure 2. A 56-year-old male patient diagnosed with TCCS. (A,B) preoperative A-P and lateral X-ray images showing the slight degenerative change of cervical spine with relative normal curvature,… Source: The clinical efficacy of anterior cervical discectomy and fusion with ROI-C device vs. plate-cage in managing traumatic central cord syndrome — Frontiers in Surgery 2023; CC BY.
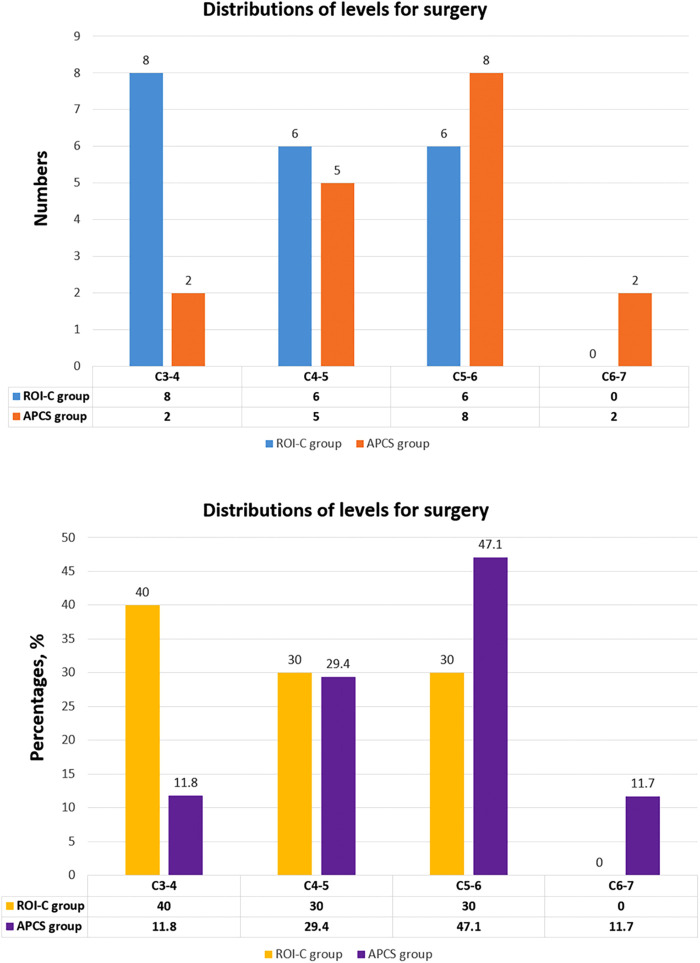 Figure 3. The distributions of levels for surgery in the ROI-C group and APCS group, exhibited as numbers and percentages. Source: The clinical efficacy of anterior cervical discectomy and fusion with ROI-C device vs. plate-cage in managing traumatic central cord syndrome — Frontiers in Surgery 2023; CC BY.
Figure 3. The distributions of levels for surgery in the ROI-C group and APCS group, exhibited as numbers and percentages. Source: The clinical efficacy of anterior cervical discectomy and fusion with ROI-C device vs. plate-cage in managing traumatic central cord syndrome — Frontiers in Surgery 2023; CC BY.
 Figure 4. Source: Management of Acute Traumatic Central Cord Syndrome: A Narrative Review — Global Spine J. 2019 May 8;9(1 Suppl):89S–97S. doi: 10.1177/2192568219830943; CC BY-NC-ND.
Figure 4. Source: Management of Acute Traumatic Central Cord Syndrome: A Narrative Review — Global Spine J. 2019 May 8;9(1 Suppl):89S–97S. doi: 10.1177/2192568219830943; CC BY-NC-ND.
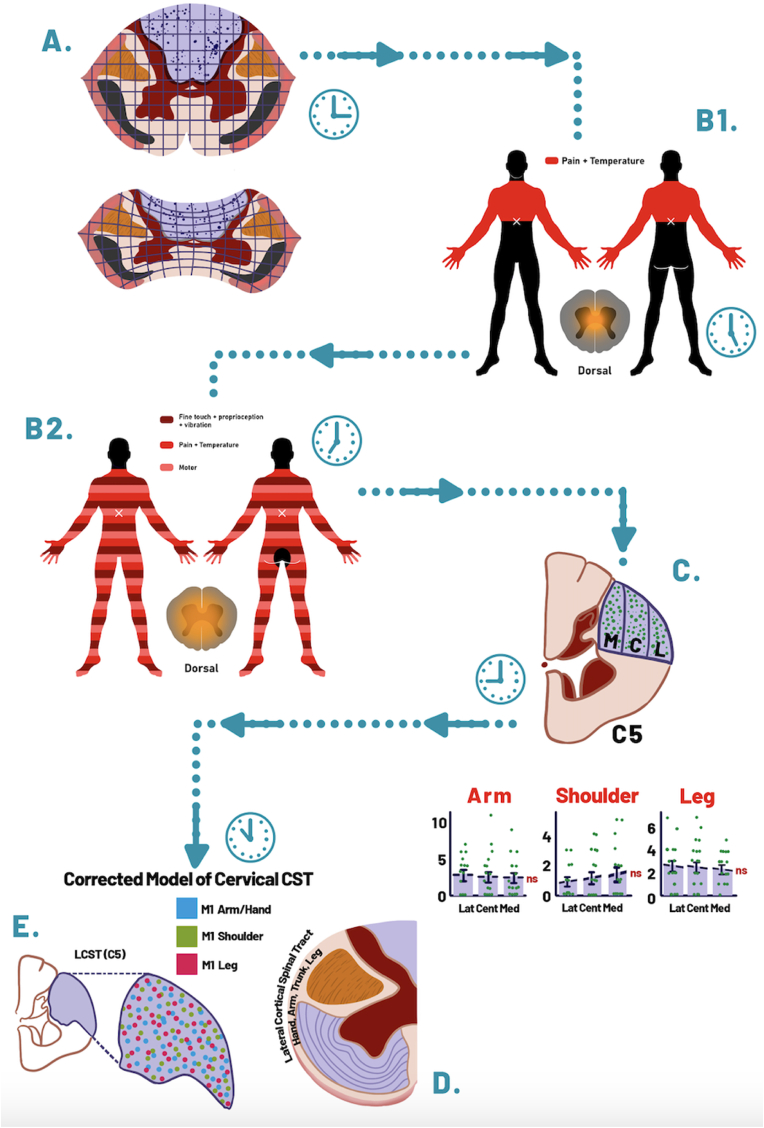 Fig. 1. TCCS pathophysiology concept evolution. The “clocks” sketches were added to illustrate symbolically different time points in history. (A) Based on initial Sir William Thorburn theories,… Source: Traumatic central cord Syndrome: An integrated neurosurgical and neurocritical care perspective — Brain & Spine 2025; CC BY-NC-ND.
Fig. 1. TCCS pathophysiology concept evolution. The “clocks” sketches were added to illustrate symbolically different time points in history. (A) Based on initial Sir William Thorburn theories,… Source: Traumatic central cord Syndrome: An integrated neurosurgical and neurocritical care perspective — Brain & Spine 2025; CC BY-NC-ND.
 Fig. 2. (From left to right and bottom): (A) Sagittal T2 weighted image of a 65 year old gentleman who suffered a neck hyperextension injury, and presented with central cord syndrome. He… Source: Traumatic central cord Syndrome: An integrated neurosurgical and neurocritical care perspective — Brain & Spine 2025; CC BY-NC-ND.
Fig. 2. (From left to right and bottom): (A) Sagittal T2 weighted image of a 65 year old gentleman who suffered a neck hyperextension injury, and presented with central cord syndrome. He… Source: Traumatic central cord Syndrome: An integrated neurosurgical and neurocritical care perspective — Brain & Spine 2025; CC BY-NC-ND.
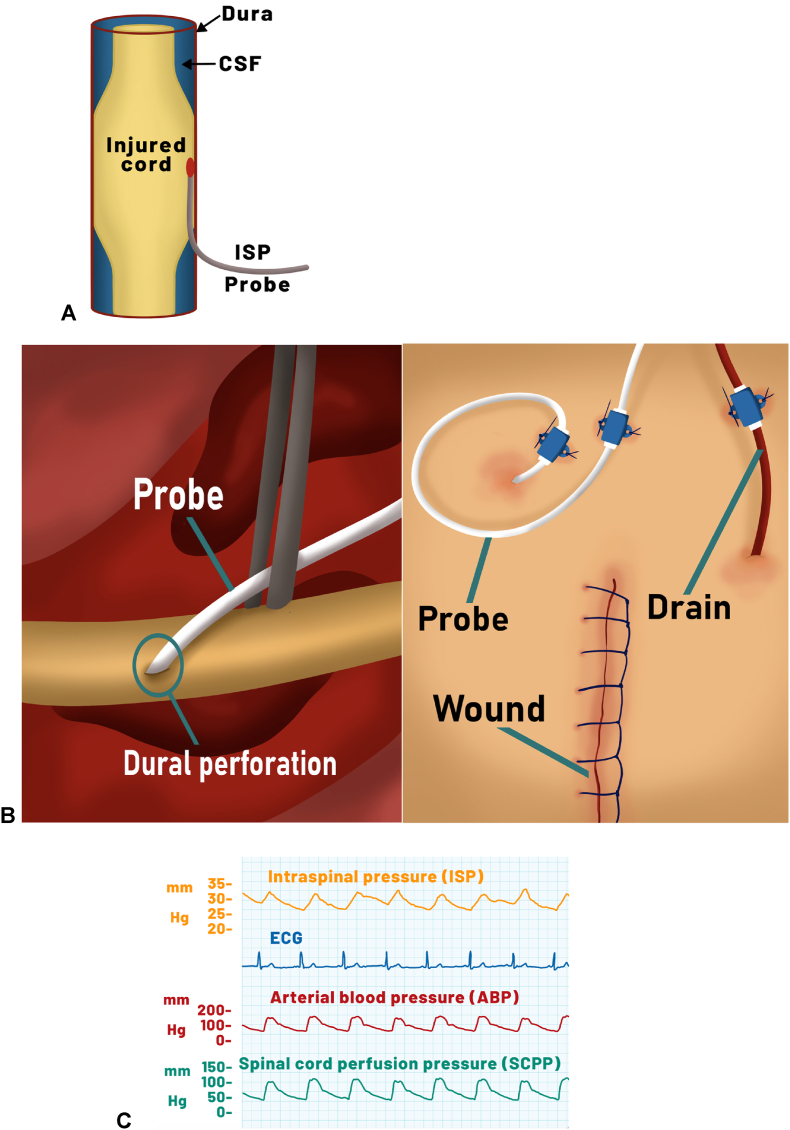 Fig. 3. Important steps in intraspinal pressure (ISP) monitoring technique and physiological variables assessment. (A) Probe proper location is in the subdural space (Phang and Papadopoulos,… Source: Traumatic central cord Syndrome: An integrated neurosurgical and neurocritical care perspective — Brain & Spine 2025; CC BY-NC-ND.
Fig. 3. Important steps in intraspinal pressure (ISP) monitoring technique and physiological variables assessment. (A) Probe proper location is in the subdural space (Phang and Papadopoulos,… Source: Traumatic central cord Syndrome: An integrated neurosurgical and neurocritical care perspective — Brain & Spine 2025; CC BY-NC-ND.
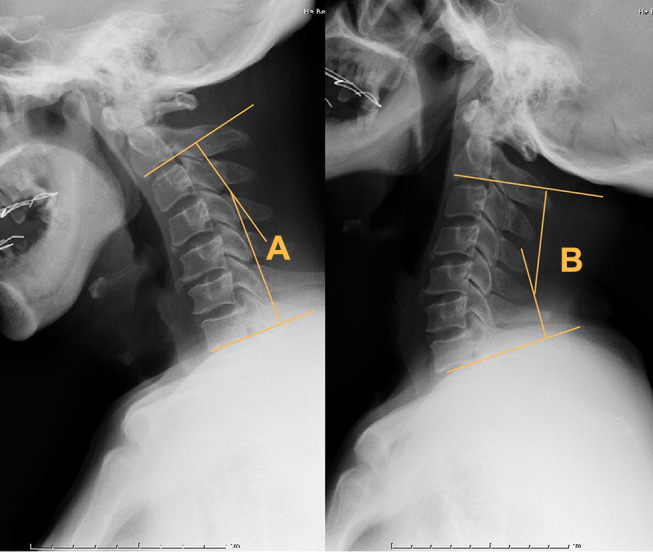 Figure 1. Angles created by a line parallel to the inferior aspect of the C2 vertebrae and a line parallel to that of the C7 vertebrae were measured at the flexion (A) and extension (B) lateral… Source: The Assessment of Dynamic Spinal Cord Impingement by Kinematic Magnetic Resonance Imaging in Patients with Traumatic Central Cord Syndrome — Therapeutics and Clinical Risk Management 2021; CC BY-NC.
Figure 1. Angles created by a line parallel to the inferior aspect of the C2 vertebrae and a line parallel to that of the C7 vertebrae were measured at the flexion (A) and extension (B) lateral… Source: The Assessment of Dynamic Spinal Cord Impingement by Kinematic Magnetic Resonance Imaging in Patients with Traumatic Central Cord Syndrome — Therapeutics and Clinical Risk Management 2021; CC BY-NC.
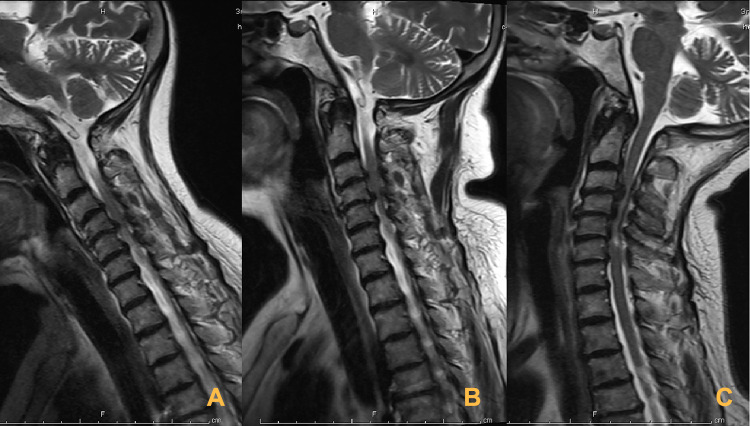 Figure 2. A 50-year-old patient with TCCS. T2-weighted MR images depict disk protrusion and hypertrophy of the ligamentum flavum at the C3-6 level. (A) In flexion, decompression of the cord… Source: The Assessment of Dynamic Spinal Cord Impingement by Kinematic Magnetic Resonance Imaging in Patients with Traumatic Central Cord Syndrome — Therapeutics and Clinical Risk Management 2021; CC BY-NC.
Figure 2. A 50-year-old patient with TCCS. T2-weighted MR images depict disk protrusion and hypertrophy of the ligamentum flavum at the C3-6 level. (A) In flexion, decompression of the cord… Source: The Assessment of Dynamic Spinal Cord Impingement by Kinematic Magnetic Resonance Imaging in Patients with Traumatic Central Cord Syndrome — Therapeutics and Clinical Risk Management 2021; CC BY-NC.
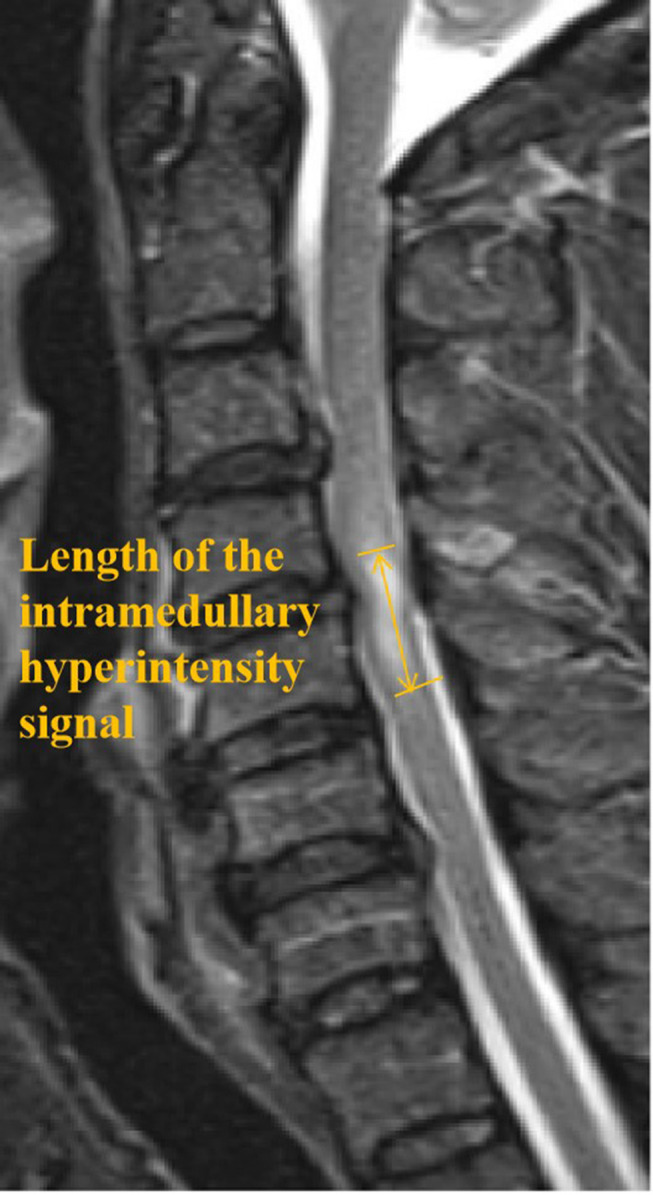 Figure 3. Length of the intramedullary hyperintensity signal (LIHS) – yellow arrow. This distance was measured as the proximal-distal range of the intramedullary hyperintensity signal. The LIHS… Source: The Assessment of Dynamic Spinal Cord Impingement by Kinematic Magnetic Resonance Imaging in Patients with Traumatic Central Cord Syndrome — Therapeutics and Clinical Risk Management 2021; CC BY-NC.
Figure 3. Length of the intramedullary hyperintensity signal (LIHS) – yellow arrow. This distance was measured as the proximal-distal range of the intramedullary hyperintensity signal. The LIHS… Source: The Assessment of Dynamic Spinal Cord Impingement by Kinematic Magnetic Resonance Imaging in Patients with Traumatic Central Cord Syndrome — Therapeutics and Clinical Risk Management 2021; CC BY-NC.
History of Present Illness
- Chief complaint: After hyperextension injury — weakness greater in the upper extremities (especially hands) than lower extremities, variable sensory loss, ± bladder dysfunction
- Classic mechanism: hyperextension in an older patient with pre-existing cervical spondylosis/stenosis (cord pinched between osteophytes and infolded ligamentum flavum), often without fracture
- Younger patients: higher-energy, may have fracture/dislocation
- Burning hands, gait
Past Medical History
- Cervical spondylosis/stenosis, OPLL, prior cervical surgery, anticoagulation
- Ankylosing spondylitis/DISH (rigid spine — fracture risk with hyperextension)
- Standard PMH
Imaging Review
MRI Cervical
- Cord signal change (T2 hyperintensity) at the stenotic level(s), pre-existing spondylotic stenosis, disc-osteophyte, ligamentum infolding
- Exclude fracture/dislocation/ligamentous injury (STIR), epidural hematoma
- Extent/levels of compression
CT Cervical
- Bony stenosis, OPLL, fracture (often absent), canal diameter, alignment
CTA (if fracture through foramen transversarium)
Labs
- CBC, BMP, Coags, type and screen
Neurological Examination
- ASIA exam — characterize upper > lower weakness, hand intrinsics, sensory, sacral sparing, sphincter; serial exams (many improve early)
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- OR setup: spine table with log-roll precautions, fluoroscopy/O-arm/navigation, traction/Mayfield when cervical, posterior/anterior implant trays, decompression instruments, cell saver/blood for large constructs, and IONM before positioning when feasible.
- Special needs: arterial line, Foley, type/cross, MAP augmentation for acute SCI per local protocol, no long paralytic when MEPs are needed, anticoagulation/reversal plan, and airway strategy for unstable cervical injuries.
- Immediate postop orders: serial ASIA/neuro checks, MAP goal/duration if SCI, CT/X-rays for hardware/alignment, brace/collar orders, drain care, DVT prophylaxis timing, bowel/bladder/skin care, and early rehab/SCI consult.
Diagnosis & Indication / Timing
- Working diagnosis: Traumatic central cord syndrome (incomplete SCI)
- Management debate: many improve with conservative care + MAP support; early surgical decompression increasingly favored for significant/persistent compression (esp. with continued deficit, instability, or fracture) — emerging evidence supports earlier decompression in incomplete SCI
- MAP goal 85-90 mmHg x ~5-7 days (cord perfusion) regardless of surgery
- Goals: decompress the stenotic cord, stabilize if unstable
Approach
- Anterior (ACDF/corpectomy) if focal anterior disc-osteophyte compression, kyphosis
- Posterior (laminectomy/laminoplasty ± fusion) if multilevel stenosis with lordosis, OPLL
- Combined for severe multilevel/instability
Position
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- Anterior: supine, awake fiberoptic intubation (myelopathic/unstable), in-line stabilization; Posterior: prone, Mayfield, careful log-roll; IONM baseline
Key Surgical Steps
- Per approach (see acdf, posterior-cervical-laminectomy-fusion, cervical-laminoplasty) — decompress the cord across the stenotic/injured levels, preserve perfusion, stabilize as indicated, IONM throughout
Critical Anatomy & Structures at Risk
- Spinal cord — already injured/edematous, exquisitely sensitive to perfusion/manipulation
- Vertebral arteries, nerve roots (C5 palsy after posterior decompression)
- Stability/alignment
Equipment
- Per approach (anterior cervical or posterior instrumentation sets), microscope, fluoroscopy/navigation, IONM
Monitoring
- SSEPs, MEPs, EMG; check around positioning
Anesthesia
- MAP 85-90 x 5-7 days, awake fiberoptic intubation (unstable/myelopathic), arterial line, no paralytic (IONM)
Potential Complications
- Neurological worsening (manipulation/perfusion), C5 palsy
- Approach-specific (dysphagia, VA injury, CSF leak, infection)
- Incomplete recovery (hand function often last/least to recover), instability
Operative Note Template
Preoperative Diagnosis: Traumatic central cord syndrome with cervical [spondylotic] stenosis [C_-C_] [± fracture]
Postoperative Diagnosis: Same
Procedure: [Anterior (ACDF/corpectomy) / Posterior (laminectomy/laminoplasty ± fusion)] cervical decompression for traumatic central cord syndrome
Surgeon / Assistant: Anesthesia: General endotracheal (awake fiberoptic intubation if unstable/myelopathic) EBL / Fluids: Adjuncts: Microscope, fluoroscopy/navigation; SSEP/MEP/EMG Implants: [Per approach — anterior plate/cage or posterior screws/rods, graft] Monitoring: SSEP/MEP — stable Complications: None
Indications: [Age]yo [M/F] with traumatic central cord syndrome after a hyperextension injury on a background of cervical stenosis, with [persistent/significant] cord compression and upper > lower extremity weakness. Early decompression was chosen [given persistent deficit/compression]; MAP 85–90 maintained. Risks discussed.
Description of Procedure: After consent and time-out, [awake fiberoptic intubation with in-line stabilization was performed], anesthesia induced maintaining MAP 85–90, and neuromonitoring established with stable baselines after positioning.
[Anterior: a Smith-Robinson approach with discectomy/corpectomy decompressed the cord at the focal compressive level(s), followed by interbody graft and plate.] [Posterior: prone positioning, and a laminectomy/laminoplasty (± lateral mass fusion) decompressed the cord across the multilevel stenosis.] Cord decompression was confirmed and perfusion preserved; neuromonitoring remained stable.
Closure was performed in layers. The patient was transferred to the ICU with MAP 85–90 and serial ASIA exams.
Postoperative Plan
- ICU, MAP 85-90 x 5-7 days, serial ASIA exams, airway monitoring (anterior)
- CT/X-ray postop, collar per construct
- DVT prophylaxis, bowel/bladder/skin care, SCI rehab consult early
- Counsel: recovery pattern (legs → bladder → proximal arms → hands; hands recover last/least); steroids controversial (institutional)
- Follow-up imaging, rehabilitation
Chief-Level Case Review
Use these as the senior-level mental model for Traumatic Central Cord Syndrome:
- Decision point: Treat physiology while preparing the room: airway, reversal, transfusion, ICP/CPP, sodium/osmolality, temperature, and repeat imaging drive timing as much as the scan finding.
- Technical lever: Know the operative priority: decompression, hemorrhage control, debridement, dural closure, reconstruction, stabilization, or contamination control.
- Bailout: Plan for swelling and coagulopathy: bone flap decision, duraplasty size, drain/EVD need, hemostatic adjuncts, and ICU handoff should be decided early.
- Postop watch: Postop failure modes are predictable: expanding hematoma, malignant edema, seizure, infection, CSF leak, venous sinus injury, and missed associated spine/vascular injury.
Common Pimp Questions
Use these to pressure-test preparation for Traumatic Central Cord Syndrome:
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]