
Operative Approach: Retrosigmoid (Retromastoid) Craniotomy
Case / Approach Snapshot
- Anatomy at risk: corridor-defining nerves, arteries, veins/sinuses, cisterns, bone landmarks, muscle/fascial planes, and closure structures that determine exposure and morbidity.
- Operative steps: confirm position and trajectory, mark landmarks, protect soft tissue and named neurovascular structures, perform the bone/soft-tissue corridor, open/close dura or target compartment deliberately, and verify hemostasis/reconstruction; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: brain relaxation failure, venous or sinus bleeding, cranial nerve/perforator risk, exposure that is too narrow, CSF leak, cosmetic/temporalis/frontalis problems, and conversion to a wider or alternate corridor.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas — Retromastoid · Rhoton CPA anatomy (PMC) · Radiopaedia — CPA · PubMed Central — retrosigmoid
High-Yield Literature
- Microsurgical Anatomy of the Endoscopy-Assisted Retrosigmoid Intradural Suprameatal Approach to the Meckel’s Cave — Xu Y. Operative neurosurgery (Hagerstown, Md.) 2021. PubMed
- Anterior Petrosectomy vs. Retrosigmoid Approach-Surgical Anatomy and Navigation-Augmented Morphometric Analysis: A Comparative Study in Cadaveric Laboratory Setting — Signoretti S. Brain sciences 2025. PubMed
- Microsurgical anatomy of acoustic neuroma — Rhoton AL Jr. Otolaryngologic clinics of North America 1992. PubMed
- Suprameatal extension of the retrosigmoid approach: microsurgical anatomy — Seoane E. Neurosurgery 1999. PubMed
- Microsurgical treatment of intracanalicular vestibular schwannomas — Noudel R. Progress in neurological surgery 2008. PubMed
- Critically located cavernous malformations — Batay F. Minimally invasive neurosurgery : MIN 2007. PubMed
- Microsurgical anatomy of the inner surface of the petrous bone: neuroradiological and morphometric analysis as an adjunct to the retrosigmoid transmeatal approach — Day JD. Neurosurgery 1994. PubMed
- Endoscopic retrosigmoid trans-petrosal fissure approach for vestibular schwannomas: case series — Feng S. Neurosurgical review 2024. PubMed
- Supracerebellar-supratrochlear and supracerebellar-infratrochlear triangles as gateways to the posterolateral midbrain and ambient cistern: descriptive and quantitative analysis of microsurgical anatomy — Hanalioglu S. Neurosurgical review 2025. PubMed
- Retrosigmoid suprafloccular transhorizontal fissure approach for resection of brainstem cavernous malformation — Ohue S. Neurosurgery 2010. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
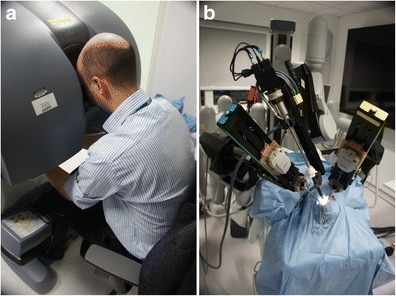 Fig. 1. Arrangement of the da Vinci master-slave system. a The surgeon is seated comfortably at the console and remotely controls the robots’ actions. b The surgical cart includes an endoscope… Source: da Vinci robot-assisted keyhole neurosurgery: a cadaver study on feasibility and safety — Neurosurgical Review 2014; CC BY.
Fig. 1. Arrangement of the da Vinci master-slave system. a The surgeon is seated comfortably at the console and remotely controls the robots’ actions. b The surgical cart includes an endoscope… Source: da Vinci robot-assisted keyhole neurosurgery: a cadaver study on feasibility and safety — Neurosurgical Review 2014; CC BY.
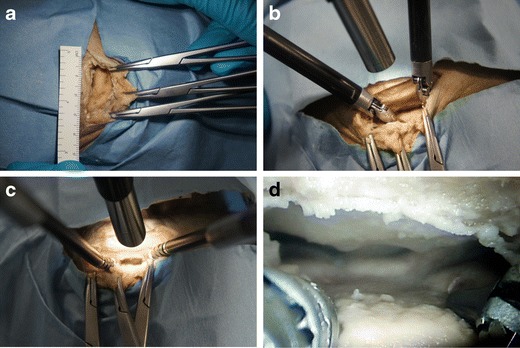 Fig. 2. Left supraorbital subfrontal approach through an eyebrow incision demonstrating the following: a keyhole craniotomy approximately 25 × 15 mm in size, b a 12-mm endoscope and two standard… Source: da Vinci robot-assisted keyhole neurosurgery: a cadaver study on feasibility and safety — Neurosurgical Review 2014; CC BY.
Fig. 2. Left supraorbital subfrontal approach through an eyebrow incision demonstrating the following: a keyhole craniotomy approximately 25 × 15 mm in size, b a 12-mm endoscope and two standard… Source: da Vinci robot-assisted keyhole neurosurgery: a cadaver study on feasibility and safety — Neurosurgical Review 2014; CC BY.
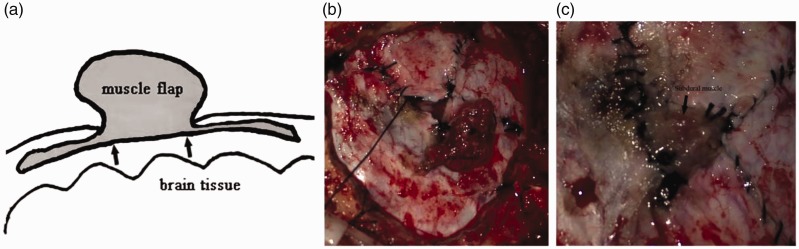 Figure 1.. Illustration of muscle flap repair. (a) Diagram of muscle flap repair. The black bar shows cerebrospinal fluid flow. (b) Free muscle flap before subdural packing. (c) Subdural muscle… Source: Effect of subdural muscle packing in repairing dura mater after retrosigmoid craniotomy — The Journal of International Medical Research 2020; CC BY-NC.
Figure 1.. Illustration of muscle flap repair. (a) Diagram of muscle flap repair. The black bar shows cerebrospinal fluid flow. (b) Free muscle flap before subdural packing. (c) Subdural muscle… Source: Effect of subdural muscle packing in repairing dura mater after retrosigmoid craniotomy — The Journal of International Medical Research 2020; CC BY-NC.
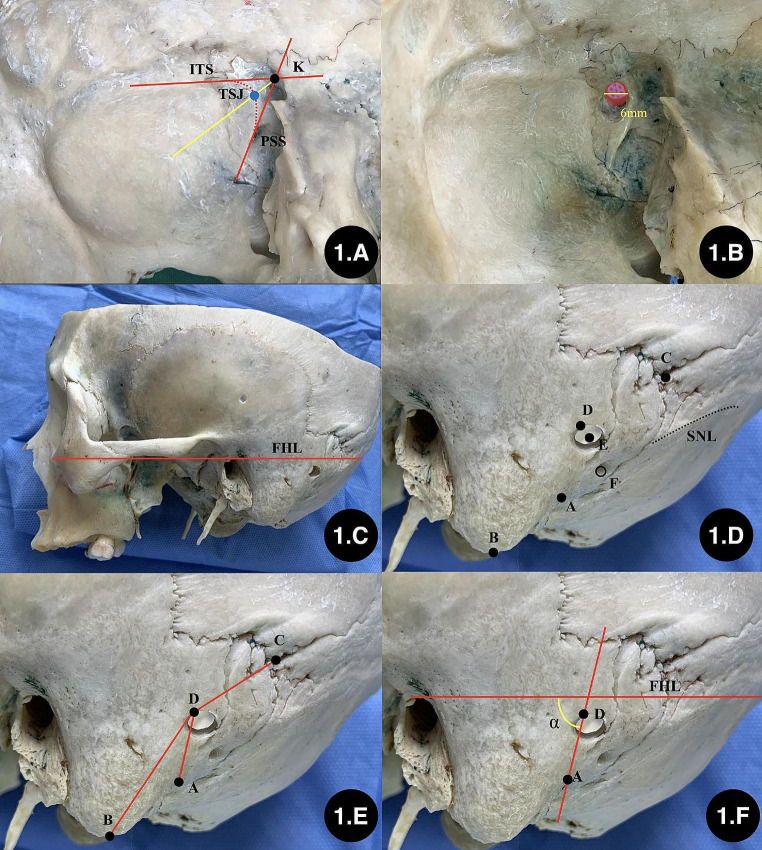 Fig. 1. The method of locating the keypoint and “keyhole”. A: location of the TSJ; B: drilling the “keyhole” (6 mm in diameter); C: confirming the baseline; D: marking the extracranial… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
Fig. 1. The method of locating the keypoint and “keyhole”. A: location of the TSJ; B: drilling the “keyhole” (6 mm in diameter); C: confirming the baseline; D: marking the extracranial… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
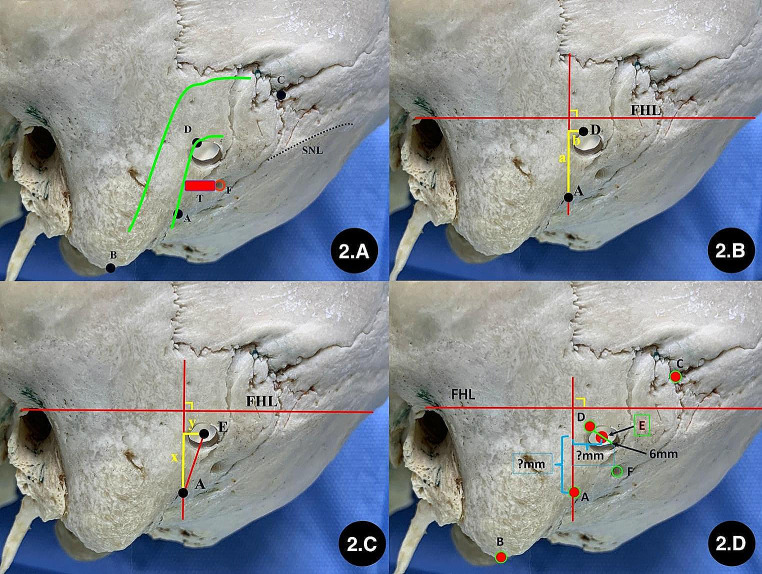 Fig. 2. Establishing the coordinate system for locating “keypoint” and “keyhole”. A: observing the relationship between burr hole and TSJ from skull surface; B: measuring the position between… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
Fig. 2. Establishing the coordinate system for locating “keypoint” and “keyhole”. A: observing the relationship between burr hole and TSJ from skull surface; B: measuring the position between… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
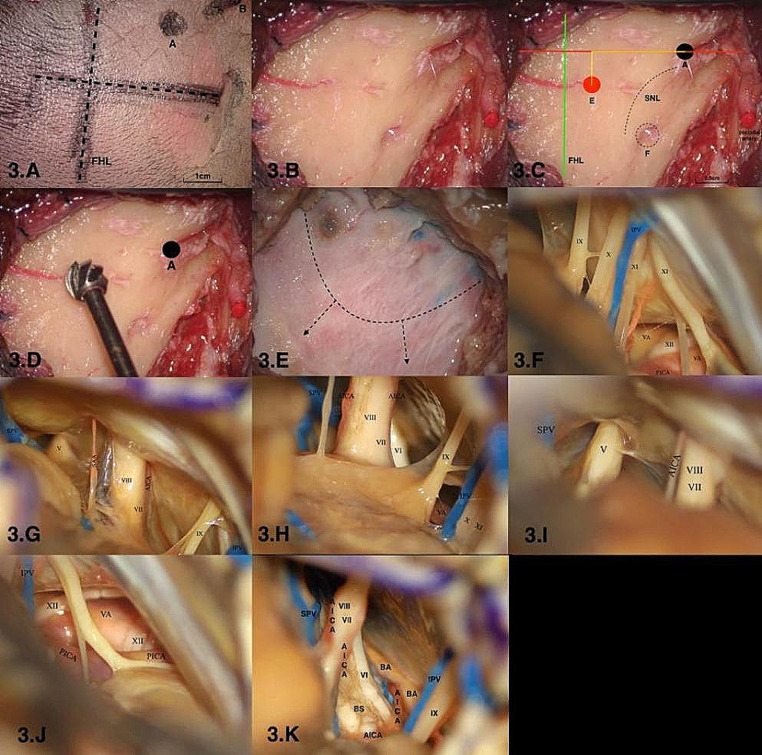 Fig. 3. Imitating and evaluating the new craniotomic method of the retrosigmoid keyhole approach on cadaveric specimens. A: Incision of the scalp; B: recognize the bone landmarks; C:… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
Fig. 3. Imitating and evaluating the new craniotomic method of the retrosigmoid keyhole approach on cadaveric specimens. A: Incision of the scalp; B: recognize the bone landmarks; C:… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
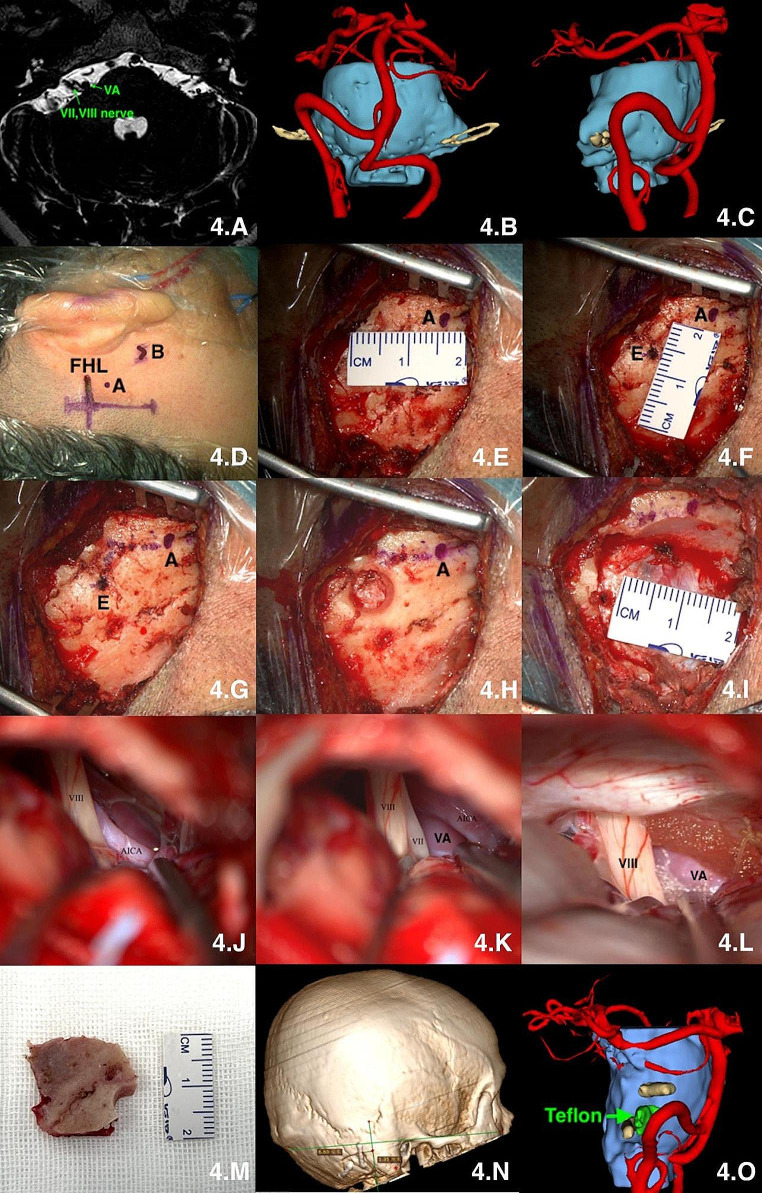 Fig. 4. microsurgical treatment of Hemifacial spasm via suboccipital retrosigmoid keyhole approach based on “one point, two lines and two distances” theory. A: MR scan; B and C: multimodal… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
Fig. 4. microsurgical treatment of Hemifacial spasm via suboccipital retrosigmoid keyhole approach based on “one point, two lines and two distances” theory. A: MR scan; B and C: multimodal… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
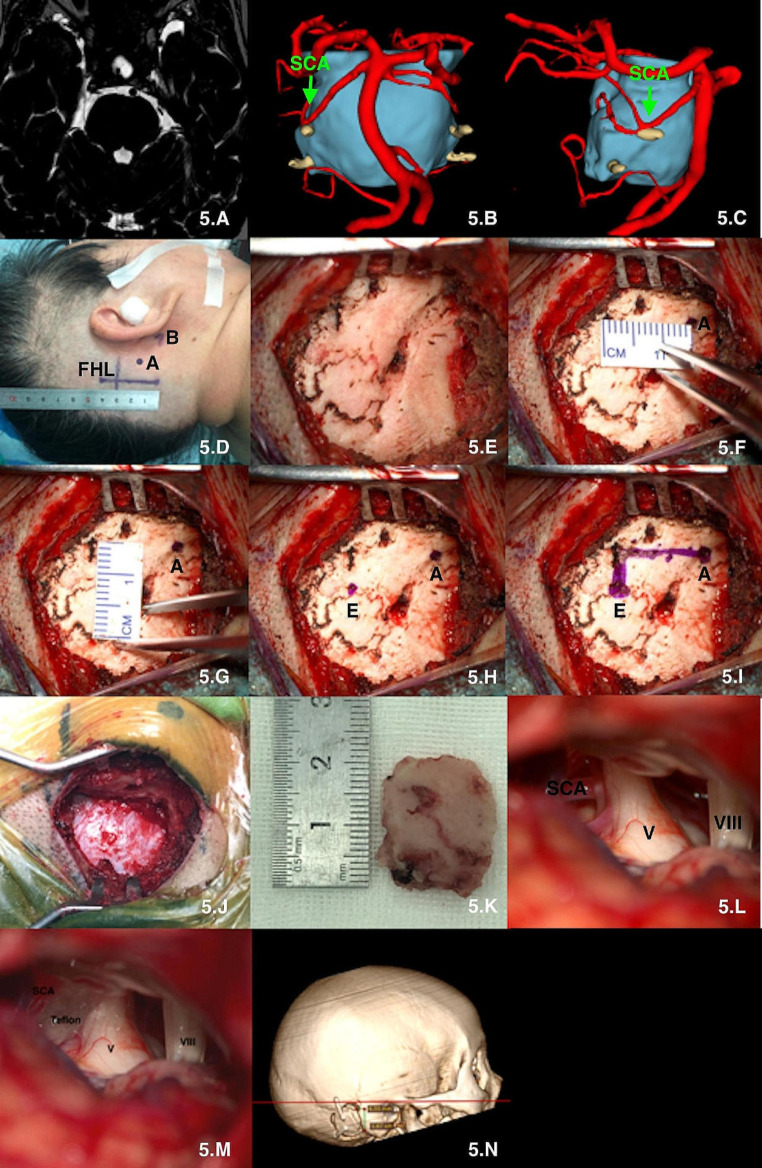 Fig. 5. microsurgical treatment of Trigminal neuralgia via suboccipital retrosigmoid keyhole approach based on “one point, two lines and two distances” theory. A: MR scan; B and C: multimodal… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
Fig. 5. microsurgical treatment of Trigminal neuralgia via suboccipital retrosigmoid keyhole approach based on “one point, two lines and two distances” theory. A: MR scan; B and C: multimodal… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
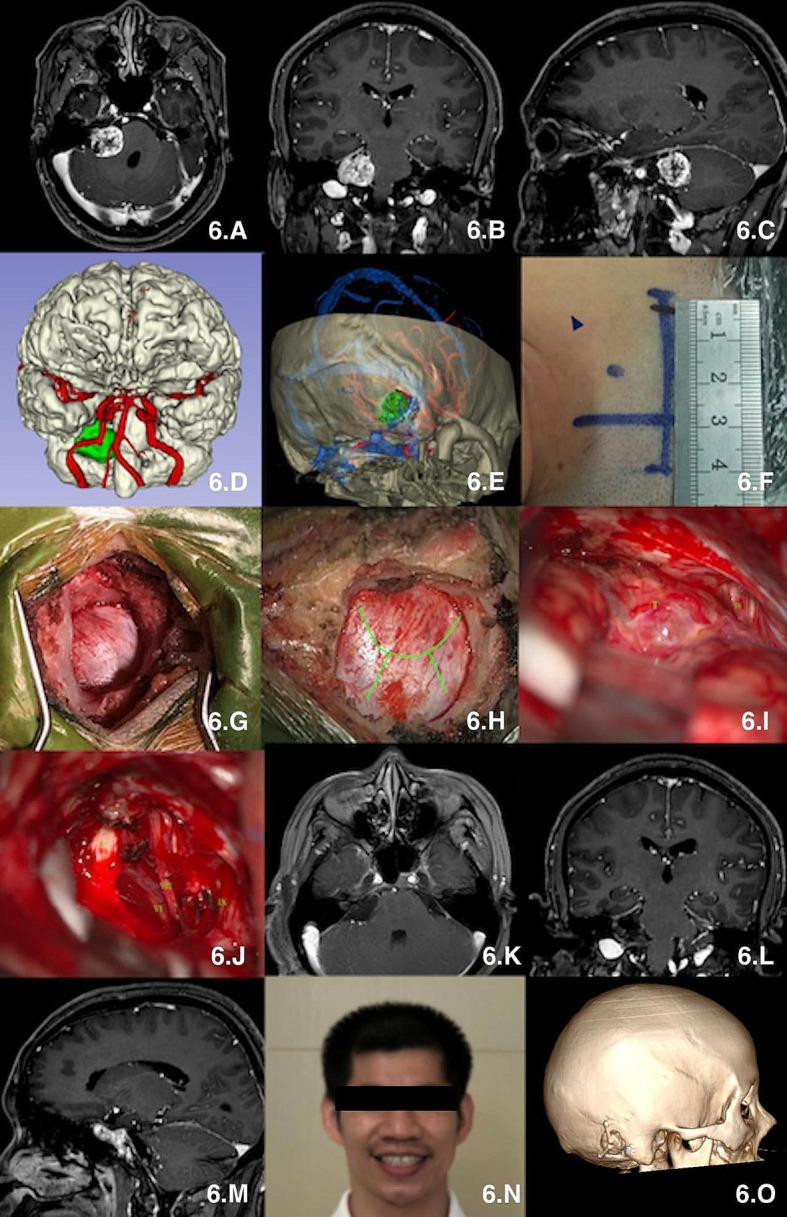 Fig. 6. microsurgical treatment of vestibular neuroma via suboccipital retrosigmoid keyhole approach based on “one point, two lines and two distances” theory. A-C: MR scan; D : multimodal… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
Fig. 6. microsurgical treatment of vestibular neuroma via suboccipital retrosigmoid keyhole approach based on “one point, two lines and two distances” theory. A-C: MR scan; D : multimodal… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
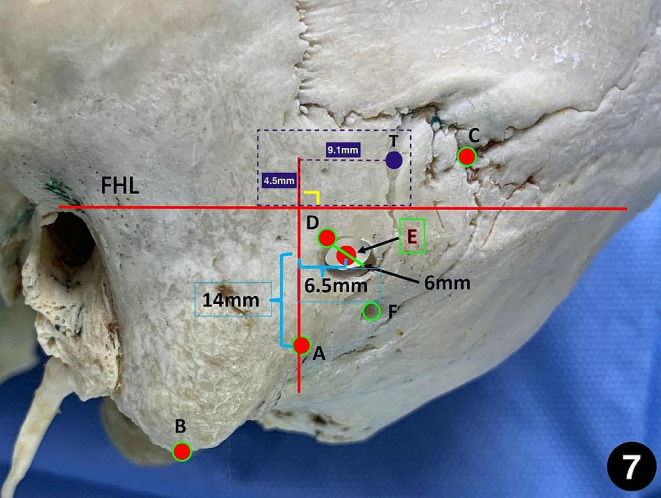 Fig. 7. the method of precisely locating the central point of keyhole via suboccipital retrosigmoid keyhole approach based on “one point, two lines and two distances” theory. A: the top point of… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
Fig. 7. the method of precisely locating the central point of keyhole via suboccipital retrosigmoid keyhole approach based on “one point, two lines and two distances” theory. A: the top point of… Source: A novel theory for rapid localization of the transverse-sigmoid sinus junction and “keyhole” in the retrosigmoid keyhole approach: micro-anatomical study, technique nuances, and clinical application — Neurosurgical Review 2024; CC BY.
The retrosigmoid craniotomy is the workhorse posterolateral corridor to the cerebellopontine angle (CPA), petroclival region, and lateral posterior fossa. It is the approach for vestibular schwannoma, CPA meningioma and epidermoid, microvascular decompression (trigeminal neuralgia, hemifacial spasm, glossopharyngeal neuralgia), and selected petroclival and foramen magnum lesions. Its power lies in a small, low-morbidity bony window placed precisely at the transverse–sigmoid sinus junction, combined with early CSF drainage that lets the cerebellum fall away from the petrous face — giving a wide, retractor-light view of cranial nerves III–XII.
General Considerations
- What it accesses: the CPA and lateral posterior fossa from the foramen magnum (CN XII) below to the trigeminal nerve and tentorial incisura above; with intradural suprameatal drilling (RISA) and petrous apex work it reaches the upper clivus and Meckel’s cave.
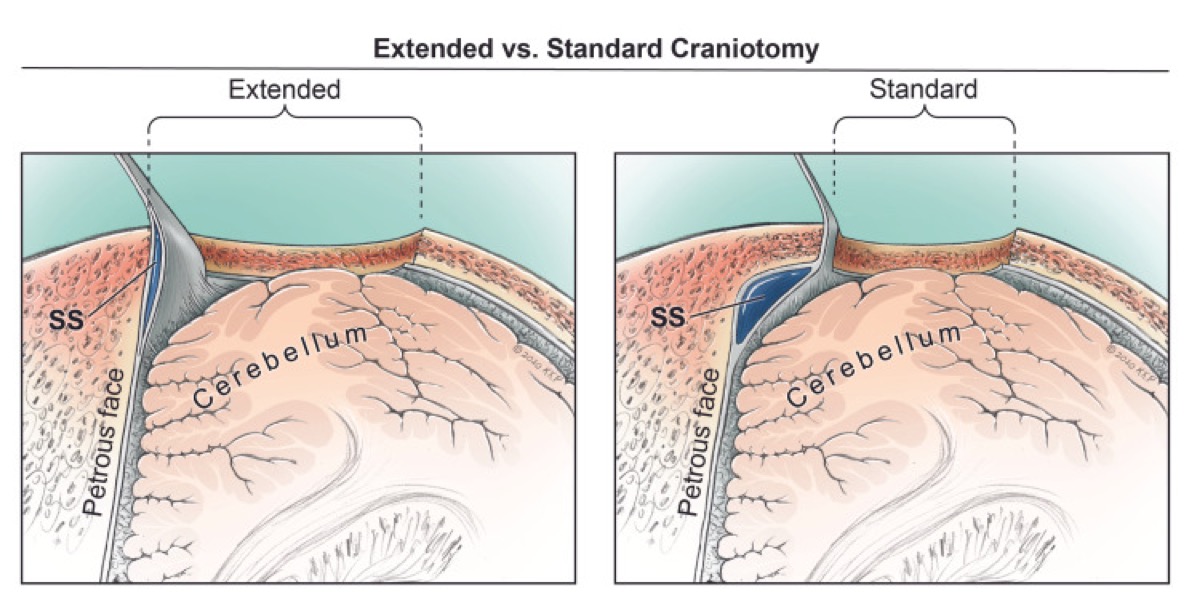
- Core principle: expose the medial edge of the sigmoid sinus and the inferior edge of the transverse sinus so the surgeon can look along the petrous face rather than across the cerebellum. The single most important determinant of a good CPA view is how far laterally (to the sigmoid) and superiorly (to the transverse) the bone is removed — not the diameter of the craniotomy.
- Retraction philosophy: modern practice is retractor-light or retractor-free. CSF egress from the cerebellomedullary (cisterna magna) and CPA cisterns relaxes the cerebellum; gravity (lateral/park-bench positioning) does the rest. Fixed blade retraction on the cerebellum is a leading cause of avoidable ataxia and should be transient if used at all.
- Craniotomy vs craniectomy: a replaced bone flap (cranioplasty) reduces postoperative headache and pseudomeningocele compared with craniectomy and is preferred when feasible; craniectomy remains acceptable, especially in revision or when the bone is thin/pneumatized.
Indications
- Vestibular schwannoma (hearing-preservation candidate, any size with brainstem reach) → see vestibular-schwannoma.md
- CPA meningioma, epidermoid → see epidermoid.md
- Microvascular decompression: trigeminal neuralgia, hemifacial spasm, glossopharyngeal neuralgia → see mvd-trigeminal-neuralgia.md, mvd-hemifacial-spasm.md
- Petroclival meningioma (smaller, or combined/staged) → see petroclival-meningioma.md
- Foramen magnum / lower CN lesions (with far-lateral extension) → see foramen-magnum-meningioma-far-lateral.md, jugular-foramen-tumor.md
Relative limitations
- Ventral brainstem and mid/lower clivus are seen only obliquely (consider far-lateral, endoscopic endonasal transclival, or petrosal approaches).
- A high-riding jugular bulb or anteriorly placed sigmoid narrows the inferolateral corridor.
- Hearing-destructive alternatives (translabyrinthine) trade hearing for a shorter, more lateral route to the IAC.
Relevant Surgical Anatomy
Venous sinuses (the frame of the approach).
- Transverse sinus (TS) runs in the attachment of the tentorium, roughly along the superior nuchal line.
- Sigmoid sinus (SS) curves down in the sigmoid groove behind the mastoid, anterior/deep to the digastric groove, to the jugular bulb.
- Transverse–sigmoid junction (TSJ) is the superolateral corner of the bony window and the key landmark.
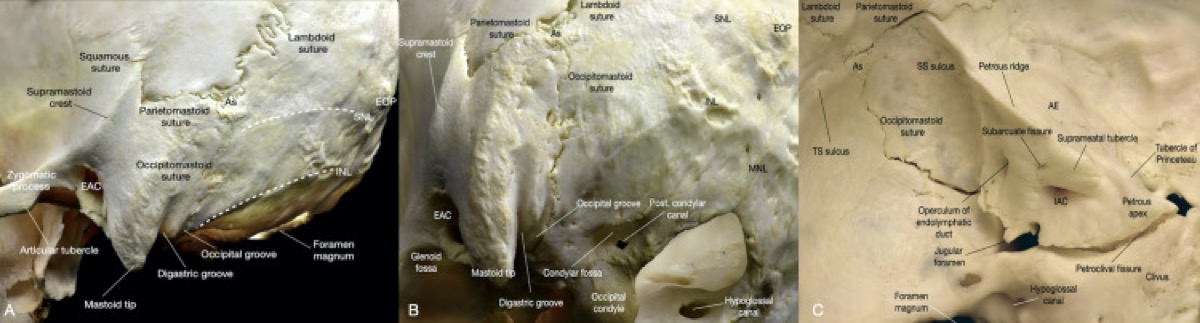
- Asterion (meeting of lambdoid, parietomastoid, occipitomastoid sutures) overlies the TSJ or the inferior transverse sinus in most heads — but its position is variable, so it guides, and navigation/anatomy confirms.
- Mastoid emissary vein pierces bone near the SS and reliably bleeds — anticipate and wax it.
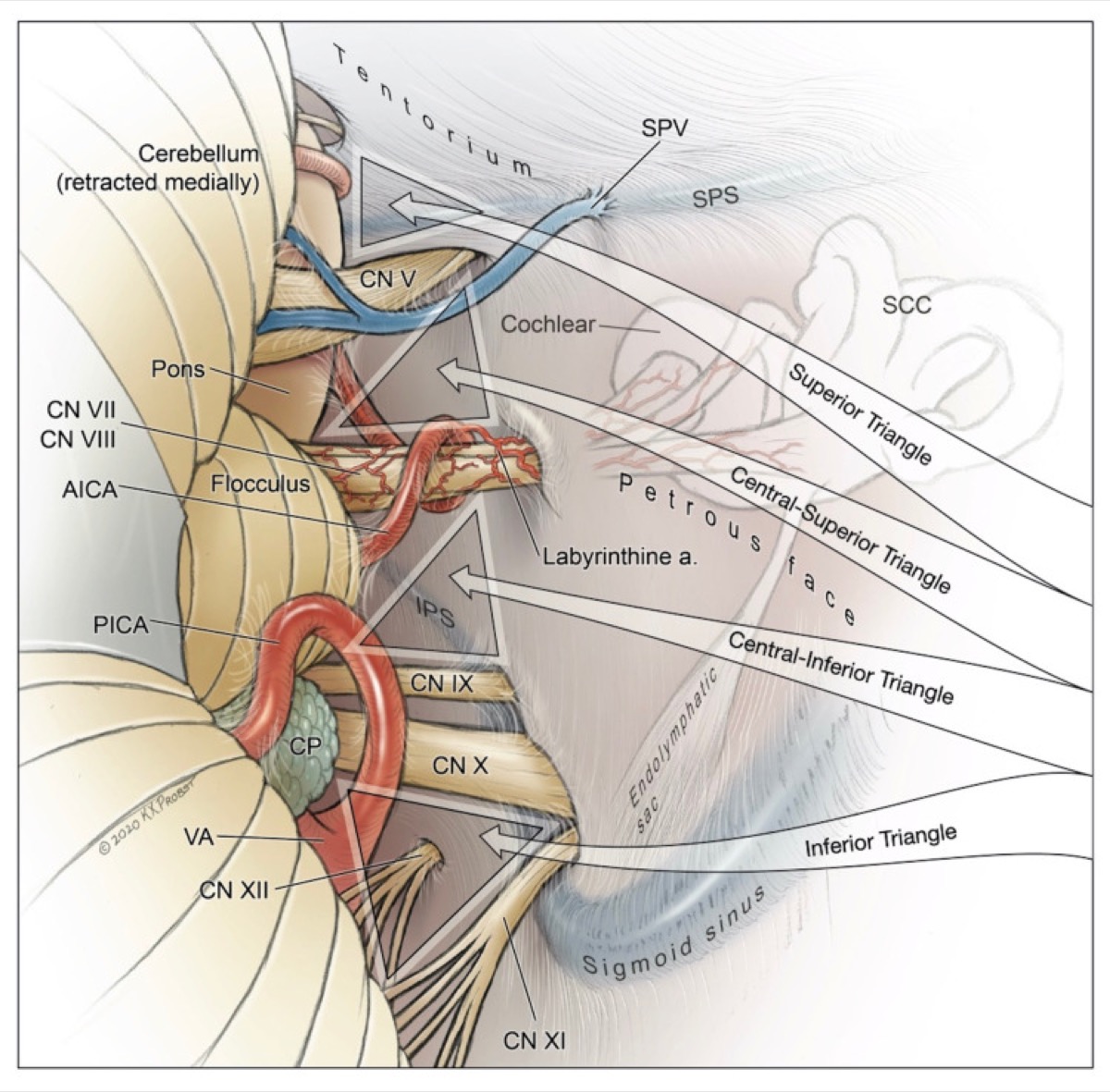
Cranial nerve relationships at the CPA (superior → inferior on the petrous face): CN V (trigeminal porus, superomedial); CN VII/VIII complex entering the internal acoustic meatus (VII anterosuperior, cochlear inferior, vestibular posterior); flocculus and choroid plexus marking the foramen of Luschka just dorsal to the VII/VIII root exit; CN IX–X–XI to the jugular foramen; CN XII to the hypoglossal canal below. AICA loops near the VII/VIII complex and into the IAC (subarcuate/labyrinthine branches) — its preservation is mandatory.
Preoperative Evaluation
- MRI with thin-cut (CISS/FIESTA) sequences through the CPA/IAC: lesion size, brainstem contact, IAC fundus extension, and for MVD the offending vessel and conflict point.
- CT / CT venogram (or MRV): pneumatization of the mastoid/petrous (air-cell risk for CSF leak), jugular bulb height/dominance, sigmoid position, and patency of the contralateral transverse sinus before any sinus sacrifice is contemplated.
- Audiometry (pure-tone average, speech discrimination) for hearing-preservation decision-making in VS.
- Baseline facial function (House-Brackmann), lower cranial nerve and swallowing assessment for larger or inferiorly placed lesions.
Logistics, OR Setup & Orders
- OR setup: Mayfield, microscope/endoscope as needed, navigation, cranial nerve monitoring/BAER when relevant, Doppler/air-embolism readiness for sitting or semisitting positions, and watertight closure materials.
- Special needs: arterial line, Foley, antiemetic plan, dexamethasone when tumor/edema risk warrants it, EVD/CSF diversion plan, VAE monitoring when sitting, and lower-CN airway/swallow contingency.
- Immediate postop orders: posterior fossa neuro checks, CN V-XII and swallow/voice screen, HOB elevation, CT for hemorrhage/hydrocephalus when indicated, MRI for tumor EOR, CSF leak/pseudomeningocele watch, and nausea control.
Anesthesia & Neuromonitoring
- GA, total intravenous anesthesia favored when MEPs/facial EMG are used; no long-acting paralytic after intubation so facial/lower-CN EMG is interpretable.
- Monitoring: continuous facial nerve EMG (and stimulation) for VS/MVD; BAERs for hearing preservation; SSEP/MEP and lower-CN (IX/X, XI, XII) EMG as dictated by lesion location; lateral spread response for hemifacial spasm.
- If a sitting/semi-sitting position is used: precordial Doppler, end-tidal CO₂, and a right-atrial catheter for venous air embolism (VAE) detection/aspiration; pre-op echocardiogram to exclude a PFO (relative contraindication to sitting).
- Lumbar drain is generally unnecessary (CSF is released intradurally) but can be considered case-by-case.
Positioning
Several positions achieve the same goal — the mastoid eminence as the highest point, the petrous face perpendicular to the floor, and gravity assisting cerebellar relaxation:
- Lateral / park-bench (most common): patient lateral, operative side up; head in Mayfield 3-pin fixation, flexed (≈2 fingerbreadths chin-to-sternum), rotated so the nose turns ~10–15° toward the floor, and laterally flexed toward the contralateral shoulder to open the cervicomastoid angle. The ipsilateral shoulder is taped down caudally to keep it out of the surgeon’s hands. An axillary roll protects the dependent brachial plexus.
- Supine with ipsilateral shoulder roll, head turned ~90°: simple and stable for thinner patients; can strain the neck if rotation is excessive.
- Semi-sitting / sitting (selected centers, esp. for venous drainage and a bloodless field): excellent gravity drainage and clean field, at the cost of VAE risk and the need for PFO screening and air-embolism monitoring.
Pin placement keeps the single pin on the operative side low and posterior so it does not encroach on the incision; the contralateral two pins sit above the ear and at the forehead. Confirm the venous outflow (no kinking of the dependent jugular) after final positioning. All pressure points padded; eyes protected.
Incision & Soft-Tissue Dissection
- Incision options: a vertical/slightly curved linear incision ~1 fingerbreadth behind the mastoid groove, centered on the asterion and extending from just above the pinna to the level of the mastoid tip (workhorse for MVD and most VS); or a C-/inverted-U myocutaneous flap for larger tumors needing wider exposure. Mark the asterion, mastoid tip, digastric groove, and superior nuchal line; navigation or Doppler can mark the sinuses on the skin.
- Incise scalp and the suboccipital muscles in line with the skin and elevate as a cuff, preserving a muscular/fascial cuff superiorly and at the superior nuchal line for a secure, watertight closure later (key to preventing CSF leak/pseudomeningocele).
- Subperiosteal dissection exposes the asterion, the mastoid behind the spine of Henle, and enough occipital bone medial to the sigmoid. Protect and wax the mastoid emissary vein when encountered. Avoid straying anterior over the mastoid (facial nerve in its vertical segment is at risk in extensive drilling).
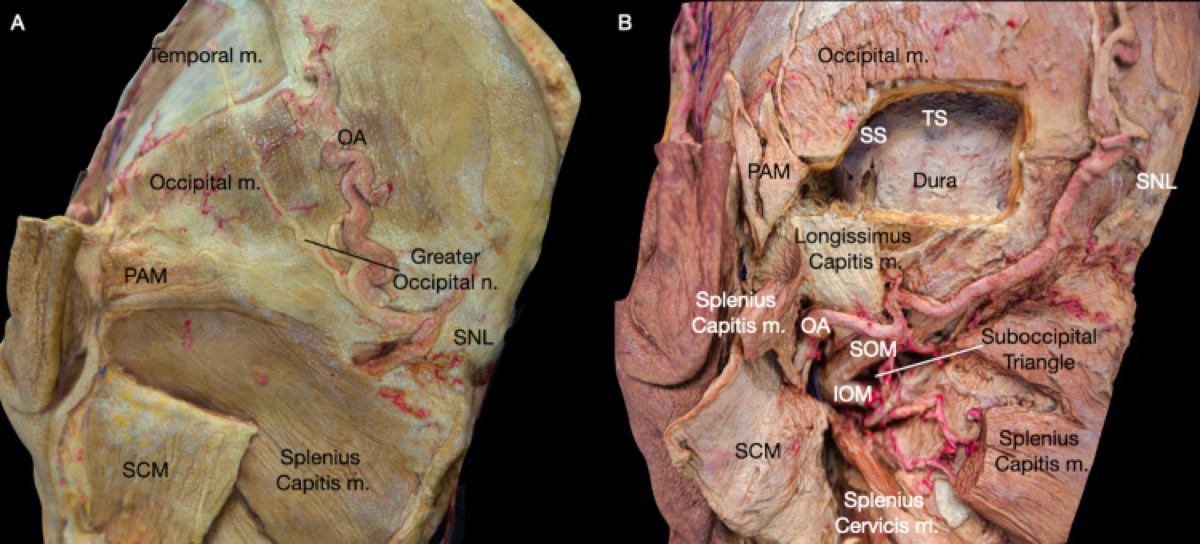
Belykh E, et al. “Immersive Surgical Anatomy of the Retrosigmoid Approach,” Cureus 2021;13(7):e16068 — CC BY 4.0. Superficial (A) and deep (B) postauricular muscle layers; the suboccipital muscle cuff is preserved for watertight closure.
Craniotomy / Craniectomy
- Burr hole placed just inferomedial to the asterion, over the inferior transverse sinus or the TSJ (navigation/anatomy-guided). Some surgeons use a single keyhole at the junction; care is taken to separate dura from bone over the sinus before turning the flap.
- Turn a craniotomy (preferred) or perform a craniectomy ~2.5–3 cm, deliberately carrying the superolateral margin to unroof the medial edge of the sigmoid sinus and the inferior edge of the transverse sinus. A diamond/cutting burr thins the bone over the sinuses, which are then exposed with a small curette/Kerrison — bony decompression of the sinuses (not their retraction) is what opens the trajectory.
- Meticulously wax all exposed mastoid/petrous air cells — this single step is the best defense against postoperative CSF rhinorrhea/otorrhea and pseudomeningocele.
- Tack-up sutures (or the bone edge) control epidural venous ooze; the dura is exposed flush with the sinus margins.
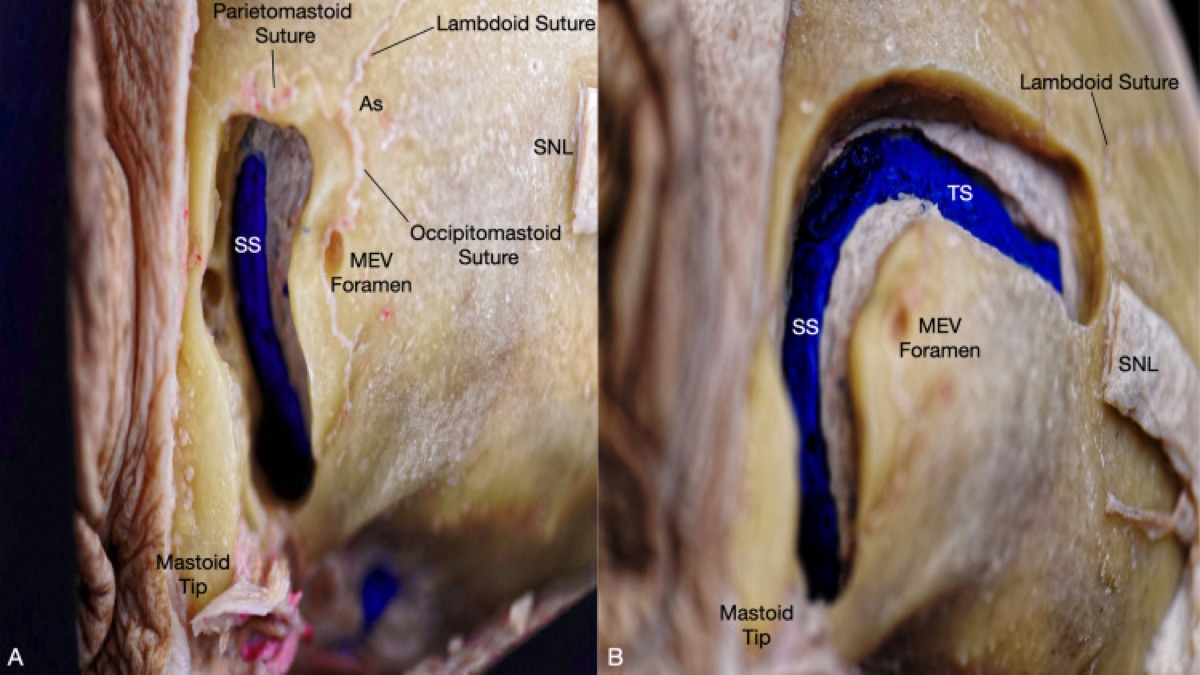
Belykh E, et al. Cureus 2021;13(7):e16068 — CC BY 4.0. The sigmoid sinus lies anterior/inferior to the asterion and connects to the mastoid emissary vein; the transverse sinus runs deep to the superior nuchal line.
Dural Opening
- Open the dura in a C-shaped (or cruciate/Y-shaped) flap based on the sigmoid sinus, hinged laterally, and tack the flap toward the sinuses with stay sutures to widen the corridor and protect the sinus.
- Before wide opening, gently elevate the inferolateral cerebellum and open the cisterna magna / cerebellomedullary cistern to release CSF; the cerebellum relaxes and falls medially, opening the CPA without fixed retraction.
- Take care that the dural opening edge does not tether bridging veins (e.g., the superior petrosal vein/Dandy’s vein complex), which are addressed deliberately under magnification.
Intradural Work
- Under the microscope, follow the petrous face medially. Sharp arachnoid dissection opens the CPA cistern; identify the CN VII/VIII complex at the porus acusticus, the flocculus and choroid plexus at Luschka marking the root exit zone, and AICA looping nearby.
- Define the lesion-specific targets:
- Vestibular schwannoma: facial-nerve mapping, internal debulking, then capsule dissection off the facial nerve; drill the IAC posterior wall (after waxing/identifying air cells) for fundal tumor; protect the labyrinth for hearing preservation.
- MVD (TN): expose the trigeminal root entry zone at the pons, sharply free arachnoid, identify the conflicting vessel (commonly SCA), and interpose Teflon felt (or transpose the vessel). For HFS, work at the CN VII root exit zone at the pontomedullary junction (commonly AICA/PICA/vertebral artery); the lateral spread response should resolve.
- CPA meningioma/epidermoid: devascularize the dural base, debulk, then dissect the capsule off the brainstem and cranial nerves; epidermoid pearls are teased out of every cistern with care to protect perforators and nerves.
- Preserve every perforator and the AICA; keep cranial-nerve manipulation minimal and watch EMG/BAER trends. Lower-CN handling can cause bradycardia/asystole — communicate with anesthesia.
Belykh E, et al. Cureus 2021;13(7):e16068 — CC BY 4.0. The four operative steps of the retrosigmoid exposure.
Closure
- Watertight dural closure is paramount; use a graft (pericranium, fascia, or a dural substitute) for any defect. A small piece of muscle/fat and dural sealant reinforce the suture line.
- Re-wax/obliterate opened air cells; pack the mastoid defect with autologous fat if pneumatized, to prevent CSF leak into the mastoid/middle ear.
- Replace the bone flap (cranioplasty) with plate/mesh, or perform titanium/methyl-methacrylate cranioplasty if craniectomy was done — restoring the bony contour reduces headache and pseudomeningocele.
- Reapproximate the suboccipital muscle and fascia in distinct, tight layers to the preserved cuff; this muscular closure is the second line of defense against CSF leak. Galea and skin closed meticulously.
Further operative anatomy & technique
Belykh E et al., Cureus 2021;13(7):e16068 — CC BY 4.0.
Belykh E et al., Cureus 2021;13(7):e16068 — CC BY 4.0.
Nuances & Pitfalls (surgeon-level)
- Don’t trust the asterion alone. Its overlap with the TSJ is variable; confirm sinus position with navigation, the suture pattern, and direct exposure before committing the superolateral bone cut.
- Expose the sinuses, don’t injure them. Decompressing the sigmoid/transverse edges buys trajectory; a sigmoid tear is controlled with Gelfoam/Surgicel and gentle pressure (not aggressive packing, which risks sinus thrombosis and venous infarction). Confirm a dominant contralateral outflow before any deliberate sinus sacrifice.
- Air cells are the enemy of a dry post-op. Wax them at the craniotomy and again at closure; fat-graft a pneumatized mastoid. CSF rhinorrhea after retrosigmoid surgery is almost always through unwaxed petromastoid cells into the middle ear and eustachian tube.
- CSF first, then work. Release the cisterna magna early; a relaxed cerebellum eliminates most need for retraction and dramatically reduces ataxia.
- Mind the AICA and the petrosal vein. Sacrificing a dominant superior petrosal (Dandy’s) vein can cause venous cerebellar/brainstem edema; coagulate sparingly and only when necessary.
- Sitting position is a deliberate trade-off. Superb drainage and a clean field versus VAE/PFO risk — screen and monitor accordingly, or default to lateral/park-bench.
- Lower-cranial-nerve vigilance in inferior exposures: anticipate hemodynamic responses and protect IX–XII to avoid aspiration and hoarseness.
Complications
- CSF leak / pseudomeningocele (incisional, rhinorrhea, otorrhea) — air-cell and dural/muscle closure dependent
- Facial weakness, hearing loss (VS), trigeminal/lower-CN dysfunction
- Cerebellar retraction injury / ataxia, venous infarction (petrosal vein/sinus)
- Vascular injury (AICA, perforators), brainstem injury
- Venous air embolism (sitting), tension pneumocephalus, postoperative headache
- Wound infection, meningitis
Cross-links
- Tumors: vestibular-schwannoma.md · epidermoid.md · petroclival-meningioma.md · jugular-foramen-tumor.md · foramen-magnum-meningioma-far-lateral.md
- Functional: mvd-trigeminal-neuralgia.md · mvd-hemifacial-spasm.md
- Related corridors: far-lateral-craniotomy.md · presigmoid-petrosal-approach.md · midline-suboccipital-craniotomy.md
Figure Use & Attribution
About the figures. Copyrighted operative figures and videos are linked (Neurosurgical Atlas, Rhoton collection); embedded images are public-domain (Gray’s Anatomy) or Creative Commons CC‑BY (open-access cadaveric anatomy), each credited beneath the image. See media-sources.md and figures/CREDITS.md.
Atlas chapters & video: Retromastoid Craniotomy — Neurosurgical Atlas · The Retrosigmoid Craniotomy (Neuroanatomy) · Retrosigmoid Approach — 3D Model · Cranial Approaches — General Principles
Chief-Level Corridor Review
Use these as the senior-level mental model for Retrosigmoid (Retromastoid) Craniotomy:
- Decision point: Define the exposure goal before incision: target, working angles, proximal/distal control, and the structure that cannot tolerate retraction.
- Technical lever: Know the first irreversible step: bone removal, dural opening, vascular control, or muscle/fascial division that commits the corridor.
- Bailout: Verbalize the bailout: extend exposure, change trajectory, add CSF drainage, obtain proximal control, convert to a larger corridor, or stop for imaging.
- Postop watch: Protect closure from the start: vascularized tissue, watertight dural/reconstruction plan, dead-space control, and drain strategy should be chosen before the final intradural step.
Common Pimp Questions
Use these to pressure-test preparation for Retrosigmoid (Retromastoid) Craniotomy:
- What patient position and head rotation make gravity work for this corridor?
- What named nerve, vessel, sinus, or muscle/fascial plane is most commonly injured?
- What bone work or soft-tissue step creates the exposure rather than simply using more retraction?
- What is the bailout if exposure is inadequate, bleeding occurs, or the brain is tight?
- What closure maneuver prevents the signature complication of this approach?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Exact head rotation/flexion/extension and pin placement: [attending-specific]
- Skin incision length, flap type, and muscle/fascial preservation technique: [attending-specific]
- Drill, rongeur, endoscope, microscope, retractor, and navigation preferences: [attending-specific]
- Drain use, closure materials, watertightness threshold, and postop imaging routine: [attending-specific]
Case Guides Using This Approach
- Epidermoid Tumor Resection
- Microvascular Decompression (MVD) for Trigeminal Neuralgia
- Microvascular Decompression for Hemifacial Spasm
- Vestibular Schwannoma (Acoustic Neuroma) Resection
References
- Rhoton AL Jr. The cerebellopontine angle and posterior fossa cranial nerves by the retrosigmoid approach. Neurosurgery. 2000;47(3 Suppl):S93–S129.
- Samii M, Gerganov VM. Surgery of Cerebellopontine Lesions. Springer, 2013.
- Jannetta PJ. Microvascular decompression of the trigeminal nerve root entry zone. In: Trigeminal Neuralgia.
- Belykh E, et al. Immersive Surgical Anatomy of the Retrosigmoid Approach. Cureus. 2021;13(7):e16068. CC BY 4.0. PMC8336623
- Cohen-Gadol AA. Retromastoid Craniotomy. The Neurosurgical Atlas. link
- Tanriover N, Rhoton AL, et al. Microsurgical anatomy of the cerebellopontine angle and internal acoustic meatus.