
Operative Approach: Presigmoid / Petrosal Approaches (Retrolabyrinthine · Translabyrinthine · Transcochlear · Combined Petrosal)
Case / Approach Snapshot
- Anatomy at risk: sigmoid/transverse sinuses, superior petrosal sinus, vein of Labbe, mastoid air cells, labyrinth/cochlea, facial nerve canal/geniculate, endolymphatic sac, jugular bulb, tentorium/CN IV, CN V-VIII and lower cranial nerves, basilar/AICA/SCA perforators, and eustachian tube-facing air cells.
- Operative steps: select the least morbid petrosal rung, plan hearing/facial/venous tradeoffs, expose mastoid-temporal bone, skeletonize sinuses/labyrinth/facial nerve, drill retrolabyrinthine/translabyrinthine/transcochlear/anterior petrosectomy corridors as needed, open presigmoid and temporal dura, manage SPS/tentorium, work the petroclival target, then obliterate air cells and reconstruct against CSF leak.
- Rescue plans: sigmoid/SPS bleeding, dominant venous drainage or Labbe compromise, facial nerve stimulation/injury, unintended labyrinth breach, high jugular bulb, petrous carotid/cochlear risk, brainstem/perforator adherence, CSF leak through mastoid/eustachian route, and need to downshift or stage rather than escalate exposure.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas — petrosectomy · Radiopaedia — petroclival meningioma · PubMed Central — combined petrosal
High-Yield Literature
- Petrosal Approach With Preservation of the Superior Petrosal Sinus (the Graceful Petrosal) for Resection of Giant Trigeminal Schwannoma: 2-Dimensional Operative Video — Almefty KK. Operative neurosurgery (Hagerstown, Md.) 2021. PubMed
- Microsurgical Resection of Giant Petroclival Meningioma via the Posterior Petrosal Approach: 2-Dimensional Operative Video — Ceccato GHW. World neurosurgery 2022. PubMed
- Partial labyrinthectomy petrous apicectomy approach to the petroclival region: an anatomic and technical study — Chanda A. Neurosurgery 2002. PubMed
- Combined petrosal approach — Polster SP. Current opinion in otolaryngology & head and neck surgery 2018. PubMed
- Presigmoid approach preserving the superior petrosal sinus in a pontine cavernous malformation associated to abnormal venous drainage of the brainstem: how I do it — Butrón-Díaz C. Acta neurochirurgica 2023. PubMed
- Combined presigmoid approach: A literature review — Albairmani SS. Surgical neurology international 2024. PubMed
- Dissection of the Petrosal Presigmoid-Retrolabyrinthine Approach for the Petroclival Region on a Cadaver: 2-Dimensional Operative Video — Borba Moreira L. Operative neurosurgery (Hagerstown, Md.) 2020. PubMed
- Combined petrosal approach: a systematic review and meta-analysis of surgical complications — Giammattei L. Neurosurgical review 2023. PubMed
- Development of a virtual dissection environment integrated into cadaveric dissection for skull base anatomy education — Uchida T. Journal of neurosurgery 2025. PubMed
- Pediatric Pontine Cavernous Malformations: The Presigmoid, Posterior Petrosal Approach — Kulwin CG. Operative neurosurgery (Hagerstown, Md.) 2018. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
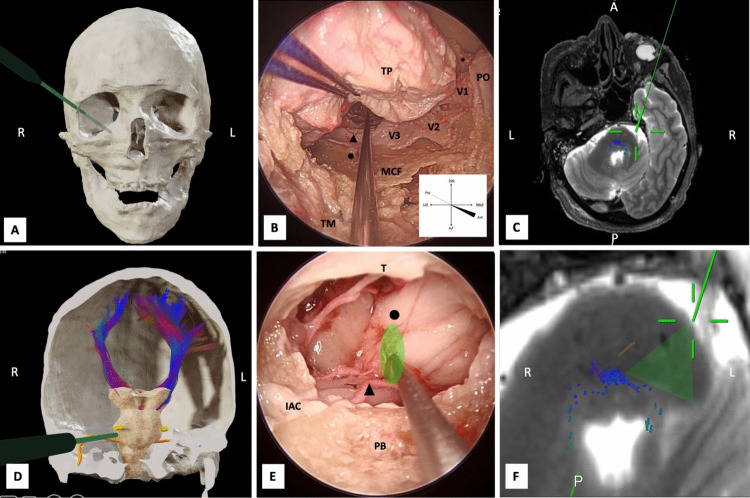 Fig. 4. Transorbital approach. A 3D reconstruction of the skull prior to dissection. A neuronavigation probe (green) indicates the trajectory of the right transorbital approach. The lateral… Source: Anatomical insights into the peri-trigeminal zone via transorbital, transclival, and retrosigmoid routes: a comparative cadaveric study with surgical implications — Acta Neurochirurgica 2026; CC BY.
Fig. 4. Transorbital approach. A 3D reconstruction of the skull prior to dissection. A neuronavigation probe (green) indicates the trajectory of the right transorbital approach. The lateral… Source: Anatomical insights into the peri-trigeminal zone via transorbital, transclival, and retrosigmoid routes: a comparative cadaveric study with surgical implications — Acta Neurochirurgica 2026; CC BY.
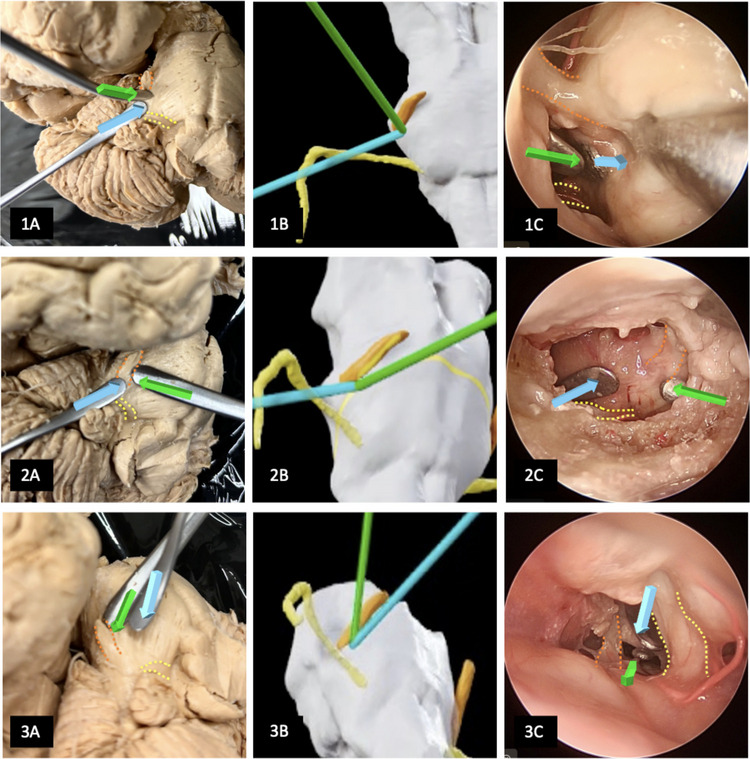 Fig. 5. Comparative image of the three surgical approaches. The peritrigeminal zone (PTZ) is bounded laterally by the root entry zone of the trigeminal nerve (highlighted with an orange dotted… Source: Anatomical insights into the peri-trigeminal zone via transorbital, transclival, and retrosigmoid routes: a comparative cadaveric study with surgical implications — Acta Neurochirurgica 2026; CC BY.
Fig. 5. Comparative image of the three surgical approaches. The peritrigeminal zone (PTZ) is bounded laterally by the root entry zone of the trigeminal nerve (highlighted with an orange dotted… Source: Anatomical insights into the peri-trigeminal zone via transorbital, transclival, and retrosigmoid routes: a comparative cadaveric study with surgical implications — Acta Neurochirurgica 2026; CC BY.
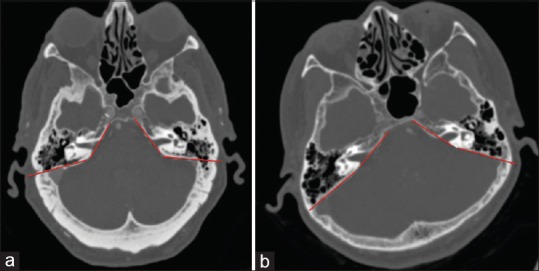 Figure 1. Example of petrous slope angle. (a) Example of a small petrous slope angle of approximately 116 degrees. (b) Example of a large petrous slope of approximately 155 degrees Source: Radiographic Assessment of the presigmoid retrolabyrinthine approach — Surgical Neurology International 2017; CC BY-NC-SA.
Figure 1. Example of petrous slope angle. (a) Example of a small petrous slope angle of approximately 116 degrees. (b) Example of a large petrous slope of approximately 155 degrees Source: Radiographic Assessment of the presigmoid retrolabyrinthine approach — Surgical Neurology International 2017; CC BY-NC-SA.
 Figure 4. Source: Radiographic Assessment of the presigmoid retrolabyrinthine approach — Surg Neurol Int. 2017 Jun 27;8:129. doi: 10.4103/sni.sni_243_16; CC BY-NC-SA.
Figure 4. Source: Radiographic Assessment of the presigmoid retrolabyrinthine approach — Surg Neurol Int. 2017 Jun 27;8:129. doi: 10.4103/sni.sni_243_16; CC BY-NC-SA.
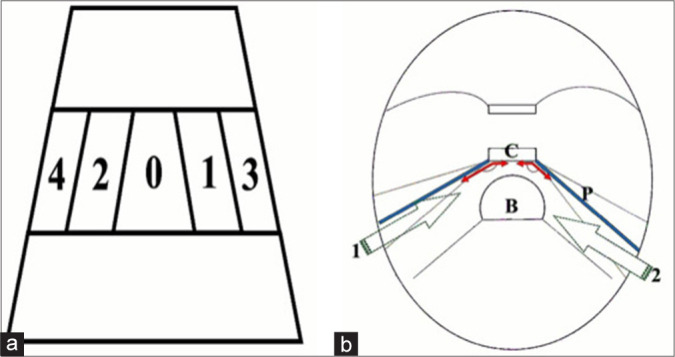 Figure 1:. (a) Depiction of the clival zone II with longitudinal classification of the basilar artery position in relation to the midline: grade-0, midline; grade-1, right paramedian; grade-2; left… Source: A standalone minimally invasive presigmoid retrolabyrinthine suprameatal approach: A cadaveric morphometric study — Surgical Neurology International 2025; CC BY-NC-SA.
Figure 1:. (a) Depiction of the clival zone II with longitudinal classification of the basilar artery position in relation to the midline: grade-0, midline; grade-1, right paramedian; grade-2; left… Source: A standalone minimally invasive presigmoid retrolabyrinthine suprameatal approach: A cadaveric morphometric study — Surgical Neurology International 2025; CC BY-NC-SA.
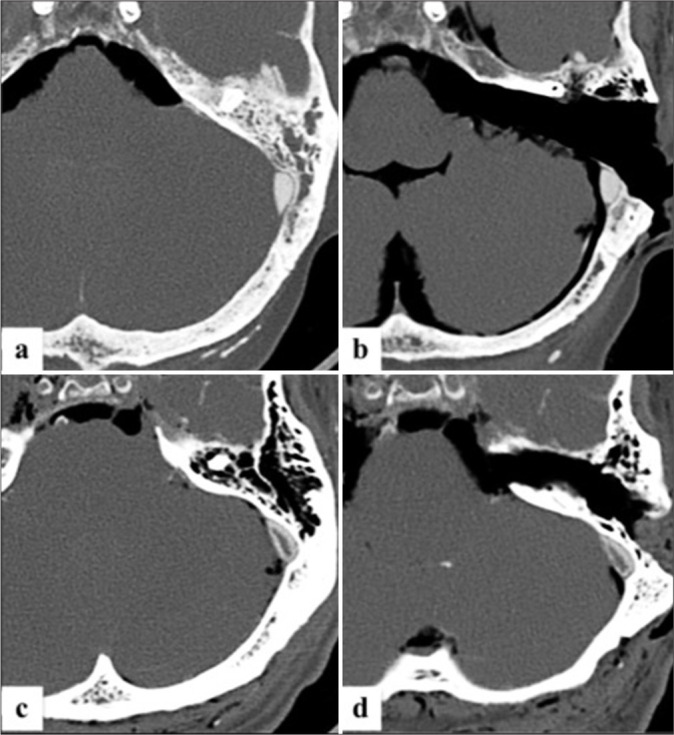 Figure 2:. Pre- and post-procedural cranial computed tomography scans showing the variation of the presigmoid retrolabyrinthine suprameatal approach (PRSA) corridor and the exposure of prepontine… Source: A standalone minimally invasive presigmoid retrolabyrinthine suprameatal approach: A cadaveric morphometric study — Surgical Neurology International 2025; CC BY-NC-SA.
Figure 2:. Pre- and post-procedural cranial computed tomography scans showing the variation of the presigmoid retrolabyrinthine suprameatal approach (PRSA) corridor and the exposure of prepontine… Source: A standalone minimally invasive presigmoid retrolabyrinthine suprameatal approach: A cadaveric morphometric study — Surgical Neurology International 2025; CC BY-NC-SA.
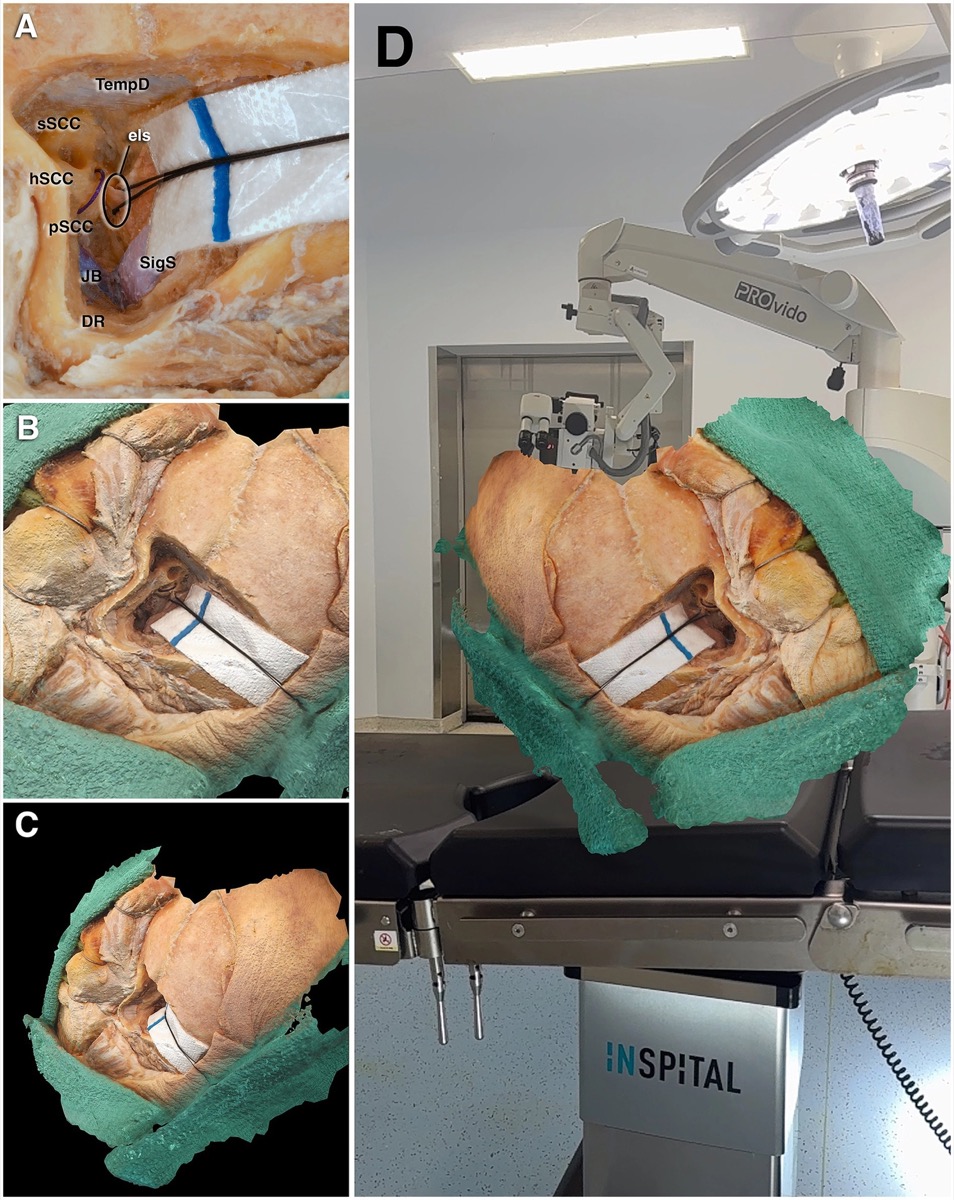
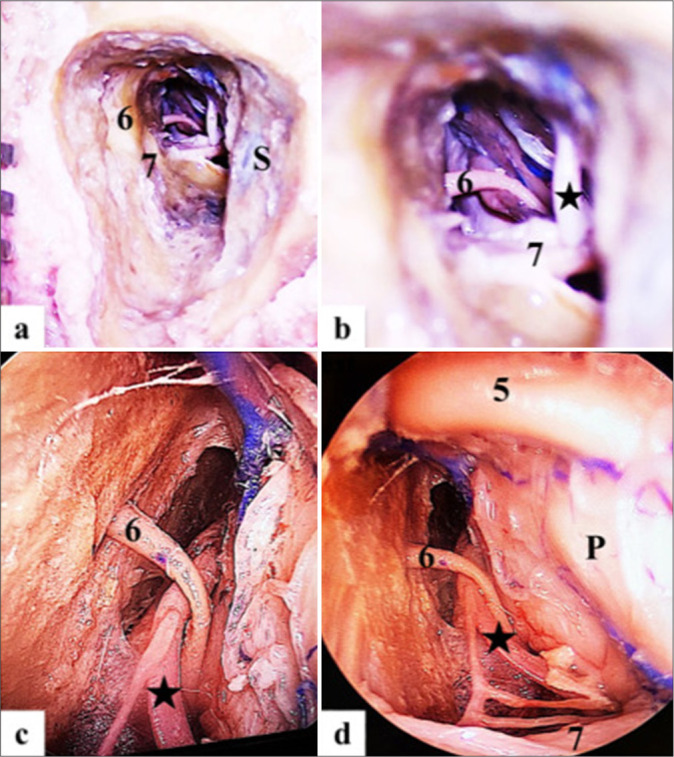 Figure 3:. Operative steps on injected cadaver head showing the extent of the minimally invasive bone cavity of left side Presigmoid retrolabyrinthine suprameatal approach: (a and b) microscopic… Source: A standalone minimally invasive presigmoid retrolabyrinthine suprameatal approach: A cadaveric morphometric study — Surgical Neurology International 2025; CC BY-NC-SA.
Figure 3:. Operative steps on injected cadaver head showing the extent of the minimally invasive bone cavity of left side Presigmoid retrolabyrinthine suprameatal approach: (a and b) microscopic… Source: A standalone minimally invasive presigmoid retrolabyrinthine suprameatal approach: A cadaveric morphometric study — Surgical Neurology International 2025; CC BY-NC-SA.
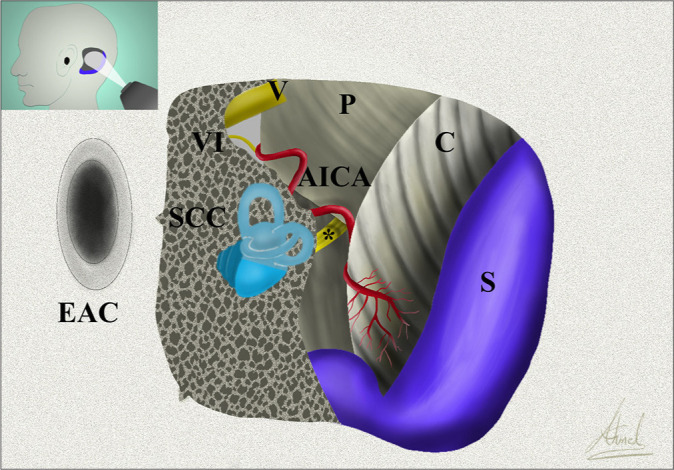 Figure 4:. Artistic depiction of the Presigmoid retrolabyrinthine suprameatal approach with related operative anatomy. AICA: Anterior inferior cerebellar artery; C: Cerebellum; EAC: External… Source: A standalone minimally invasive presigmoid retrolabyrinthine suprameatal approach: A cadaveric morphometric study — Surgical Neurology International 2025; CC BY-NC-SA.
Figure 4:. Artistic depiction of the Presigmoid retrolabyrinthine suprameatal approach with related operative anatomy. AICA: Anterior inferior cerebellar artery; C: Cerebellum; EAC: External… Source: A standalone minimally invasive presigmoid retrolabyrinthine suprameatal approach: A cadaveric morphometric study — Surgical Neurology International 2025; CC BY-NC-SA.
 Figure 9. Source: A standalone minimally invasive presigmoid retrolabyrinthine suprameatal approach: A cadaveric morphometric study — Surg Neurol Int. 2025 Feb 28;16:68. doi: 10.25259/SNI_1110_2024; CC BY-NC-SA.
Figure 9. Source: A standalone minimally invasive presigmoid retrolabyrinthine suprameatal approach: A cadaveric morphometric study — Surg Neurol Int. 2025 Feb 28;16:68. doi: 10.25259/SNI_1110_2024; CC BY-NC-SA.
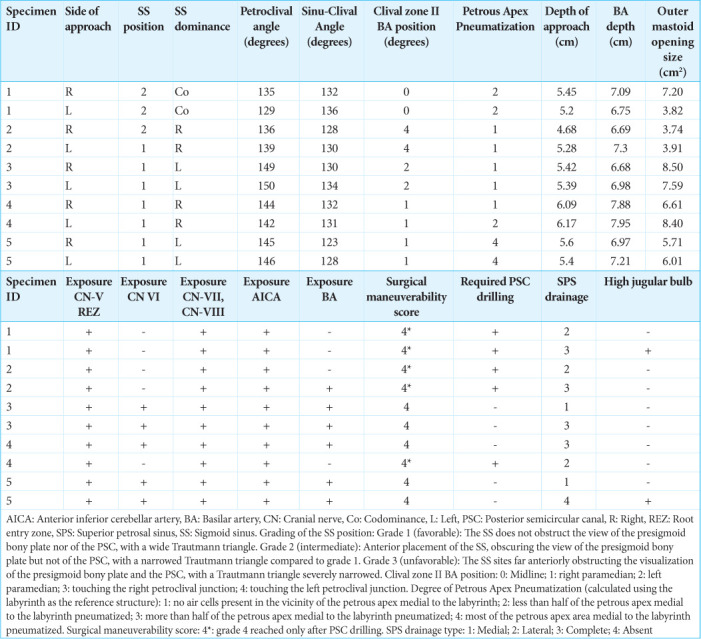 Figure 10. Source: A standalone minimally invasive presigmoid retrolabyrinthine suprameatal approach: A cadaveric morphometric study — Surg Neurol Int. 2025 Feb 28;16:68. doi: 10.25259/SNI_1110_2024; CC BY-NC-SA.
Figure 10. Source: A standalone minimally invasive presigmoid retrolabyrinthine suprameatal approach: A cadaveric morphometric study — Surg Neurol Int. 2025 Feb 28;16:68. doi: 10.25259/SNI_1110_2024; CC BY-NC-SA.
The petrosal (presigmoid) approaches drill through the petrous temporal bone to reach the petroclival region, mid-clivus, Meckel’s cave, and the ventral pons along the shortest, most anterior trajectory — opening the dura in front of the sigmoid sinus (presigmoid) and dividing the tentorium to combine supra- and infratentorial exposure. They form a graded ladder trading hearing/facial function for ventral reach: retrolabyrinthine (hearing-preserving) → translabyrinthine (sacrifices hearing) → transcochlear (sacrifices hearing + reroutes the facial nerve); the combined petrosal adds an anterior petrosectomy (Kawase) for maximal petroclival exposure. These are the big-gun skull-base approaches for large petroclival meningiomas and chordomas.
General Considerations
- What it accesses: the petroclival junction, middle/upper clivus, Meckel’s cave, prepontine cistern, and ventral pons, with control of CN III–XI and the basilar trunk/AICA/SCA.
- The presigmoid principle: drilling the mastoid/petrous bone lets the dura be opened anterior to the sigmoid sinus, bringing the surgeon’s line of sight directly onto the petroclival dura — far more anterior than the retrosigmoid route — and dividing the tentorium unites the middle and posterior fossa corridors.
- The graded ladder (hearing/facial trade-off):
- Retrolabyrinthine — bone removed behind the labyrinth; hearing and facial function preserved; narrowest presigmoid window.
- Translabyrinthine — labyrinth removed; hearing sacrificed, facial nerve preserved; wider.
- Transcochlear — cochlea removed and facial nerve rerouted; widest ventral access; hearing lost, facial-palsy risk.
- Combined petrosal — posterior petrosectomy + anterior petrosectomy (Kawase) + tentorial division for the largest petroclival lesions.
- Reserve for the right lesion. These approaches are long and morbid; many petroclival lesions are now managed with retrosigmoid ± subtemporal/Kawase, staged routes, or radiosurgery. Choose petrosal when a large, firm, ventral petroclival tumor demands the exposure.
Indications
- Large petroclival meningioma (the prototypical indication) → petroclival-meningioma.md
- Clival / petroclival chordoma, chondrosarcoma → clival-chordoma.md
- Trigeminal schwannoma (Meckel’s/posterior fossa dumbbell), epidermoid
- Mid-basilar/ventral pontine vascular lesions, brainstem cavernoma (anterolateral)
Petrosal Ladder: What You Gain and Spend
| Variant | Exposure gained | Function spent | Best fit |
|---|---|---|---|
| Retrolabyrinthine | Presigmoid window with hearing preservation | Narrower corridor, more limited anterior reach | Serviceable hearing, smaller petroclival/ventral pontine target |
| Translabyrinthine | Wider presigmoid/CPA exposure | Sacrifices hearing | Nonserviceable hearing, large CPA/petroclival lesion |
| Transcochlear | Most anterior posterior-petrosal reach | Hearing lost, facial rerouting morbidity | Extreme ventral clival/petroclival disease when facial/hearing tradeoff justified |
| Combined petrosal | Adds Kawase/anterior petrosectomy and supratentorial control | Longer, more venous/CSF-leak morbidity | Large petroclival meningioma/chordoma crossing middle and posterior fossae |
| Retrosigmoid or Kawase alone | Less drilling and morbidity | Less ventral/combined exposure | Softer, smaller, lateralized, or staged lesions |
The right answer is often not “maximum petrosectomy.” Escalate only when the lesion’s anterior/ventral extension, consistency, and neurovascular encasement demand the extra bone removal.
Relevant Surgical Anatomy
- Temporal bone: mastoid air cells, the labyrinth (semicircular canals) and cochlea, the facial nerve (mastoid/tympanic segments, geniculate), the endolymphatic sac, and the sinodural (Citelli) angle.
- Venous framework: sigmoid and transverse sinuses, superior petrosal sinus (SPS), jugular bulb, and the vein of Labbé — the petrosal corridor lives between the sigmoid (behind) and the labyrinth/cochlea (in front), under the SPS/tentorium.
- Tentorium and incisura: divided (behind CN IV’s entry) to connect fossae; CN IV, V at the incisura.
- Petroclival contents: CN VI (Dorello’s canal), the basilar artery, AICA/SCA, and the pons.
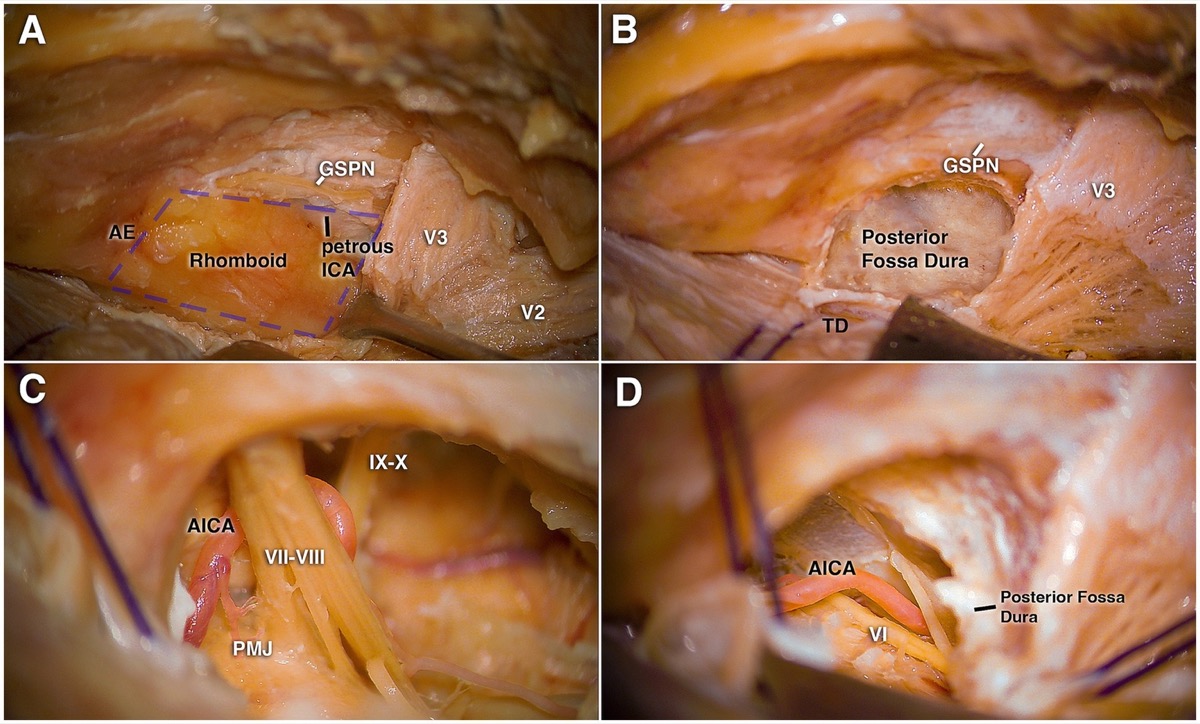
Front Neurol 2026;17:1736101 — CC BY 4.0. The anterior petrosectomy (Kawase) component of the combined petrosal approach.
Preoperative Evaluation
- High-resolution CT temporal bone: labyrinth, cochlea, facial nerve canal, jugular bulb height, degree of pneumatization, and tumor bony involvement — decides which rung of the ladder is feasible.
- MRI / MRV: tumor extent and consistency, brainstem/CN/vessel relations, venous dominance (sigmoid), and the vein of Labbé (its drainage governs temporal-lobe safety).
- Audiometry and facial-nerve baseline — central to choosing retro- vs trans-labyrinthine vs transcochlear and to counseling.
Preoperative No-Go / Modify Flags
- Serviceable hearing with a lesion manageable by retrosigmoid/Kawase should push away from translabyrinthine/transcochlear escalation.
- Dominant ipsilateral sigmoid sinus, high-riding jugular bulb, large emissary veins, or critical vein of Labbe drainage may force a different position, smaller corridor, or staged plan.
- Highly pneumatized temporal bone increases CSF leak risk; plan wax/fat/fascial/vascularized flap reconstruction before the drill starts.
- Facial nerve weakness, prior mastoid surgery, radiation, or cholesteatoma/infection changes drilling risk and may require neurotology leadership.
- A soft tumor with safe retrosigmoid debulking may not need the morbidity of a full petrosal route.
Logistics, OR Setup & Orders
- OR setup: Mayfield, microscope/endoscope as needed, navigation, cranial nerve monitoring/BAER when relevant, Doppler/air-embolism readiness for sitting or semisitting positions, and watertight closure materials.
- Special needs: arterial line, Foley, antiemetic plan, dexamethasone when tumor/edema risk warrants it, EVD/CSF diversion plan, VAE monitoring when sitting, and lower-CN airway/swallow contingency.
- Immediate postop orders: posterior fossa neuro checks, CN V-XII and swallow/voice screen, HOB elevation, CT for hemorrhage/hydrocephalus when indicated, MRI for tumor EOR, CSF leak/pseudomeningocele watch, and nausea control.
Anesthesia & Neuromonitoring
- GA/TIVA; continuous facial EMG, BAER (if hearing preservation), SSEP/MEP, lower-CN and CN III–VI EMG. Lumbar drain often placed. Neurotologist/skull-base team commonly co-operate. VAE precautions if semi-sitting.
Positioning
- Supine with the head turned to the contralateral side (or lateral/park-bench), mastoid uppermost, Mayfield fixation; the ipsilateral shoulder is supported/tucked. The vein-of-Labbé–bearing temporal lobe must not be compromised by positioning or retraction.
Exposure — Craniotomy + Petrosectomy Drilling
- Large C-shaped retroauricular + temporal incision; a temporo-occipital craniotomy spanning the transverse sinus (presigmoid + subtemporal exposure), preserving a vascularized pericranial/temporalis flap for reconstruction.
- Mastoidectomy: skeletonize the sigmoid sinus, SPS, and sinodural angle; identify the labyrinth and facial nerve canal.
- Select the rung: retrolabyrinthine (preserve labyrinth, hearing) vs translabyrinthine (drill the canals — hearing lost) vs transcochlear (remove cochlea, reroute the facial nerve). Drill anteriorly toward the petrous apex; an anterior petrosectomy (Kawase rhomboid) is added for the combined petrosal.
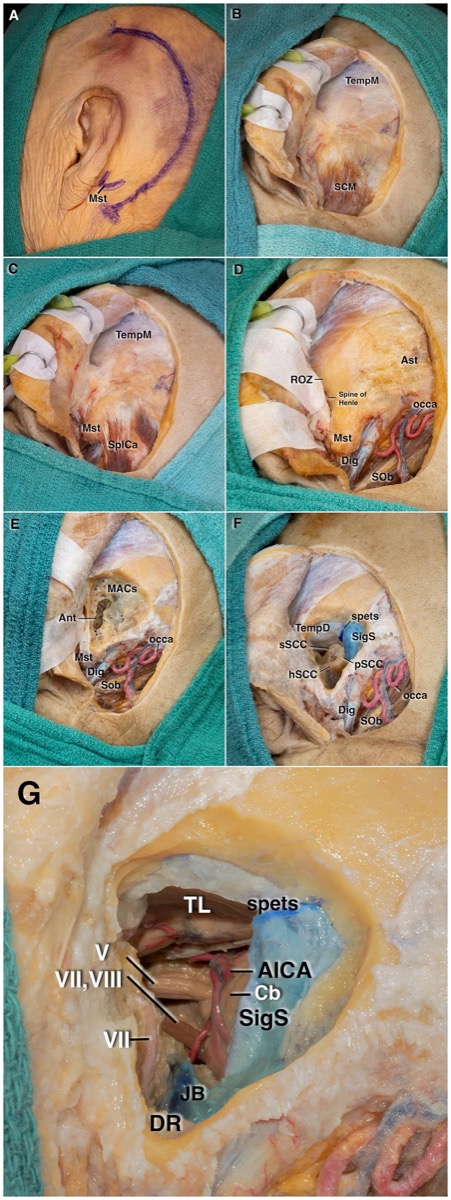
Front Neurol 2026;17:1736101 — CC BY 4.0. Stepwise temporal-bone drilling exposing the presigmoid corridor and CPA.
Dural Opening, Tentorial Division & Intradural Work
- Open the dura presigmoid (anterior to the sigmoid sinus) and along the temporal base; ligate/divide the superior petrosal sinus and divide the tentorium behind the entry of CN IV, uniting the supra- and infratentorial fields.
- Protect the vein of Labbé (do not tether/sacrifice), the sigmoid sinus, and CN IV. Work the petroclival lesion: devascularize the clival/petrous dural base, debulk, and dissect the capsule off the brainstem, basilar/AICA/SCA, and CN III–XI; preserve perforators.
Drilling and Dural-Opening Pearls
- Skeletonize before sacrificing: know sigmoid, jugular bulb, facial canal, labyrinth, and dura before deepening the petrosectomy.
- Use diamond burrs and copious irrigation near labyrinth, facial nerve, sigmoid sinus, and petrous carotid; heat injury is still injury.
- Open air cells deliberately and seal them immediately enough that they are not forgotten at closure.
- Divide tentorium under direct visualization and behind CN IV; the trochlear nerve is small, unforgiving, and easy to injure during tentorial division.
- If preserving SPS, work around it intentionally; if dividing it, confirm venous collateral tolerance and control both ends.
Intraoperative Rescue
- Sigmoid/SPS bleeding: pack, lower venous pressure, expose both ends, repair/clip/suture when possible, and avoid sinus sacrifice without dominance/collateral confidence.
- Vein of Labbe tension: release temporal retraction, alter the working angle, or stage; sacrificing Labbe can create a dominant temporal venous infarct.
- Facial nerve irritation: stop drilling/traction, irrigate cool, verify stimulation threshold, and change trajectory; do not drill blind around a dehiscent canal.
- Unintended labyrinth opening in a hearing-preservation case: stop and reassess hearing goal, seal appropriately, counsel postoperatively, and avoid compounding with cochlear/facial injury.
- Brainstem/perforator adherence: leave adherent capsule rather than avulsing AICA/SCA/basilar perforators; radiosurgery/staged reoperation is better than a perforator stroke.
- CSF leak risk at closure: add fat, fascia, muscle/pericranial flap, eustachian-tube/air-cell occlusion, lumbar drainage when appropriate, and low threshold for early repair if rhinorrhea/otorrhea occurs.
Closure & Reconstruction
- Meticulous closure is critical — CSF leak is the signature complication. Obliterate the mastoid/petrous defect and eustachian tube–facing air cells with autologous fat, achieve a watertight (grafted) dural closure, and buttress with a vascularized pericranial/temporalis flap. Replace bone; lumbar drain managed per leak risk.
Further operative anatomy & technique
Front Neurol 2026;17:1736101 — CC BY 4.0.
Nuances & Pitfalls (surgeon-level)
- Match the rung to the hearing/facial reality. Don’t sacrifice a hearing ear or risk the facial nerve for exposure you don’t need — retrolabyrinthine if hearing is serviceable; escalate only as the lesion demands.
- Vein of Labbé and the temporal lobe — positioning and tentorial work must protect Labbé; its loss causes temporal venous infarction/aphasia (dominant side).
- CSF leak is the dominant morbidity — fat obliteration + vascularized flap + watertight dura; under-treated air cells leak to the middle ear/eustachian tube.
- Facial nerve is at risk throughout drilling (and is deliberately rerouted in transcochlear) — continuous EMG, identify the canal early.
- Sinus/SPS handling — confirm sigmoid dominance before any sinus sacrifice; control the SPS deliberately.
- Reserve the approach — for many lesions a retrosigmoid or subtemporal/Kawase (or staged/combined) route is less morbid; the full petrosal is for large, firm, ventral petroclival disease.
Complications
CSF leak (most common); hearing loss (trans-labyrinthine/cochlear) and facial palsy; vein of Labbé / temporal venous infarction; CN IV/V/VI and lower-CN deficits; sigmoid-sinus thrombosis/venous infarct; brainstem/vascular injury; meningitis; long operative time/approach morbidity.
Cross-links
- Pathology: petroclival-meningioma.md · clival-chordoma.md · vestibular-schwannoma.md
- Related corridors: subtemporal-craniotomy.md (anterior petrosectomy/Kawase) · retrosigmoid-craniotomy.md · far-lateral-craniotomy.md
Figure Use & Attribution
About the figures. Copyrighted operative figures/videos are linked (Neurosurgical Atlas, Rhoton); embedded images are public-domain (Gray’s Anatomy) or CC‑BY (open-access), credited beneath each image. See media-sources.md and figures/CREDITS.md.
Atlas chapter: Extended Posterior Petrosectomy — Neurosurgical Atlas
Chief-Level Corridor Review
Use these as the senior-level mental model for Presigmoid / Petrosal Approaches (Retrolabyrinthine · Translabyrinthine · Transcochlear · Combined Petrosal):
- Decision point: Define the exposure goal before incision: target, working angles, proximal/distal control, and the structure that cannot tolerate retraction.
- Technical lever: Know the first irreversible step: bone removal, dural opening, vascular control, or muscle/fascial division that commits the corridor.
- Bailout: Verbalize the bailout: extend exposure, change trajectory, add CSF drainage, obtain proximal control, convert to a larger corridor, or stop for imaging.
- Postop watch: Protect closure from the start: vascularized tissue, watertight dural/reconstruction plan, dead-space control, and drain strategy should be chosen before the final intradural step.
Common Pimp Questions
Use these to pressure-test preparation for Presigmoid / Petrosal Approaches (Retrolabyrinthine · Translabyrinthine · Transcochlear · Combined Petrosal):
- What patient position and head rotation make gravity work for this corridor?
- What named nerve, vessel, sinus, or muscle/fascial plane is most commonly injured?
- What bone work or soft-tissue step creates the exposure rather than simply using more retraction?
- What is the bailout if exposure is inadequate, bleeding occurs, or the brain is tight?
- What closure maneuver prevents the signature complication of this approach?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Exact head rotation/flexion/extension and pin placement: [attending-specific]
- Skin incision length, flap type, and muscle/fascial preservation technique: [attending-specific]
- Drill, rongeur, endoscope, microscope, retractor, and navigation preferences: [attending-specific]
- Drain use, closure materials, watertightness threshold, and postop imaging routine: [attending-specific]
Case Guides Using This Approach
References
- Al-Mefty O, Fox JL, Smith RR. Petrosal approach for petroclival meningiomas. Neurosurgery. 1988;22(3):510–517.
- House WF, Hitselberger WE. The transcochlear approach to the skull base. Arch Otolaryngol. 1976.
- Kawase T, Shiobara R, Toya S. Anterior transpetrosal-transtentorial approach for sphenopetroclival meningiomas. Neurosurgery. 1991;28(6):869–876.
- Anterolateral, lateral, and posterior corridors to complex skull base lesions in sphenocavernous and petroclival regions: microsurgical anatomy with 3D reconstructions. Front Neurol. 2026;17:1736101. CC BY 4.0. (figures embedded above)
- Cohen-Gadol AA. Extended Posterior Petrosectomy. The Neurosurgical Atlas. link