
Case Prep: Petroclival Meningioma Resection
Case / Approach Snapshot
- Anatomy at risk: tumor compartment, arterial supply, venous drainage/sinuses, cranial nerves, white-matter tracts, pituitary/CSF pathways when relevant, and functional cortex.
- Operative steps: review imaging and goals, choose exposure, obtain brain relaxation, devascularize when possible, debulk internally, dissect capsule from critical structures, verify extent/safety, and reconstruct watertight closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: venous or arterial injury, swelling, seizure, cranial nerve or endocrine change, CSF leak, residual tumor left for safety, staged surgery, radiation, or adjuvant therapy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [size] cm [left/right] petroclival meningioma presenting with [gait ataxia / CN deficits (V, VII, VIII) / headache] planned for [retrosigmoid / anterior petrosectomy (Kawase) / posterior petrosectomy / combined] approach for resection.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Presigmoid / petrosal approaches — detailed corridor setup, step-by-step technique & figures
Operative figures/atlases are © (linked, not copied). See media-sources.md.
- Technique/approach: The Neurosurgical Atlas — search “petroclival meningioma”
- Imaging: Radiopaedia — petroclival meningioma
- Open-access figures: PubMed Central
High-Yield Literature
- [Petroclival meningioma] — Ohata K. No shinkei geka. Neurological surgery 2002. PubMed
- Endoscopic endonasal transclival petroclival meningioma resection — Magill ST. Neurosurgical focus: Video 2022. PubMed
- Spontaneous regression of a petroclival meningioma: illustrative case — Noda R. Journal of neurosurgery. Case lessons 2024. PubMed
- The role of stereotactic radiosurgery in the management of petroclival meningioma: a systematic review — Wijaya JH. Journal of neuro-oncology 2022. PubMed
- Staged Approach for Petroclival Meningioma Resection — Klironomos G. Journal of neurological surgery. Part B, Skull base 2019. PubMed
- Endoscopic Far-Lateral Supracerebellar Infratentorial Approach for Petroclival Region Meningioma: Surgical Technique and Clinical Experience — Xie T. Operative neurosurgery (Hagerstown, Md.) 2022. PubMed
- Approach selection for resection of petroclival meningioma — Jackson C. Neurosurgical focus: Video 2022. PubMed
- Intracranial necrotising sarcoid granulomatosis mimicking petroclival meningioma — Valappil A. BMJ case reports 2022. PubMed
- Anterior transpetrosal (Kawase) approach for petroclival meningioma with trigeminal neuralgia: case report and literature review — Dzhindzhikhadze RS. Zhurnal voprosy neirokhirurgii imeni N. N. Burdenko 2023. PubMed
- Retrosigmoid Intradural Suprameatal Approach for Petroclival Meningioma — Ishi Y. Journal of neurological surgery. Part B, Skull base 2019. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
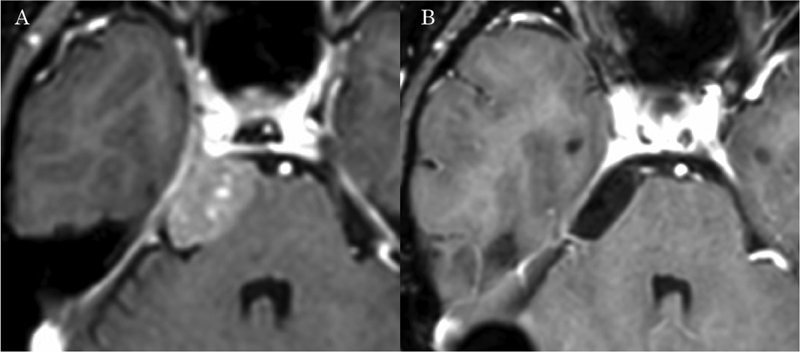 Fig. 1. Pre- and postoperative imaging. (A) Preoperative gadolinium-enhanced T1-weighted imaging (Gd-T1-WI) of magnetic resonance imaging (MRI) presenting with right petroclival meningioma. (B)… Source: Retrosigmoid Intradural Suprameatal Approach for Petroclival Meningioma — Journal of Neurological Surgery. Part B, Skull Base 2019; CC BY-NC-ND.
Fig. 1. Pre- and postoperative imaging. (A) Preoperative gadolinium-enhanced T1-weighted imaging (Gd-T1-WI) of magnetic resonance imaging (MRI) presenting with right petroclival meningioma. (B)… Source: Retrosigmoid Intradural Suprameatal Approach for Petroclival Meningioma — Journal of Neurological Surgery. Part B, Skull Base 2019; CC BY-NC-ND.
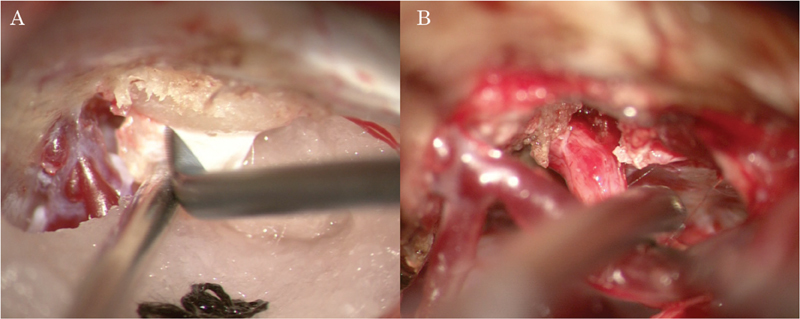 Fig. 2. Intraoperative view. (A) Exposure of the suprameatal tubercle after lateral suboccipital craniotomy. (B) The operative field after tumor removal, presenting a favorable view around the… Source: Retrosigmoid Intradural Suprameatal Approach for Petroclival Meningioma — Journal of Neurological Surgery. Part B, Skull Base 2019; CC BY-NC-ND.
Fig. 2. Intraoperative view. (A) Exposure of the suprameatal tubercle after lateral suboccipital craniotomy. (B) The operative field after tumor removal, presenting a favorable view around the… Source: Retrosigmoid Intradural Suprameatal Approach for Petroclival Meningioma — Journal of Neurological Surgery. Part B, Skull Base 2019; CC BY-NC-ND.
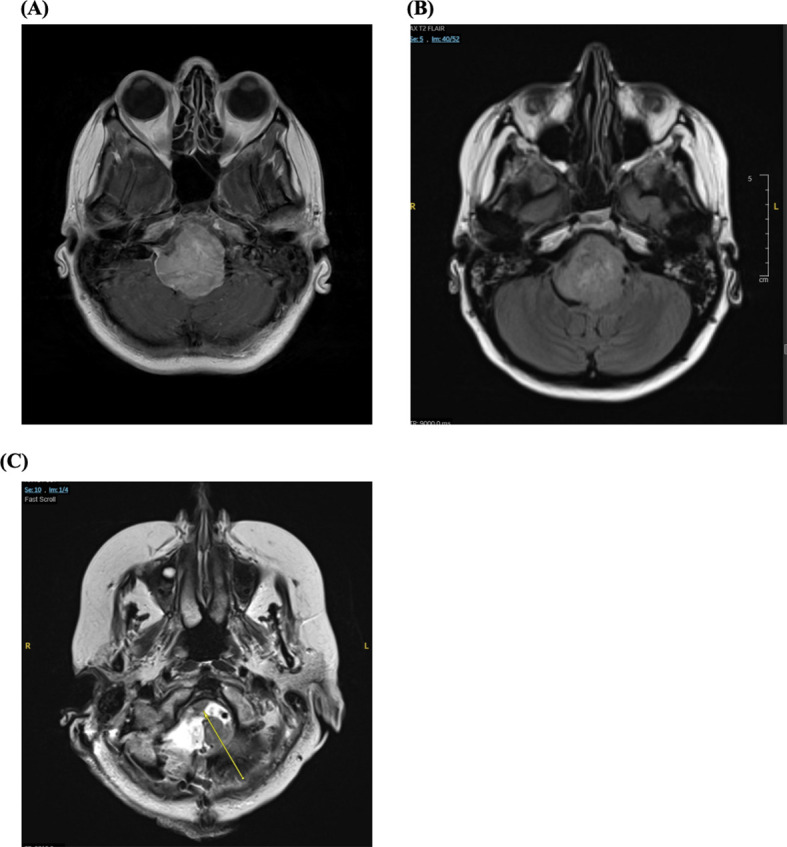 Figure 1. Axial magnetic resonance images (MRI) demonstrating a large right petroclival meningioma obstructing cerebrospinal fluid (CSF) flow through the fourth ventricle. (A) T1-weighted… Source: Case Report: Neuro-ophthalmic manifestations of petroclival meningioma — Frontiers in Ophthalmology 2026; CC BY.
Figure 1. Axial magnetic resonance images (MRI) demonstrating a large right petroclival meningioma obstructing cerebrospinal fluid (CSF) flow through the fourth ventricle. (A) T1-weighted… Source: Case Report: Neuro-ophthalmic manifestations of petroclival meningioma — Frontiers in Ophthalmology 2026; CC BY.
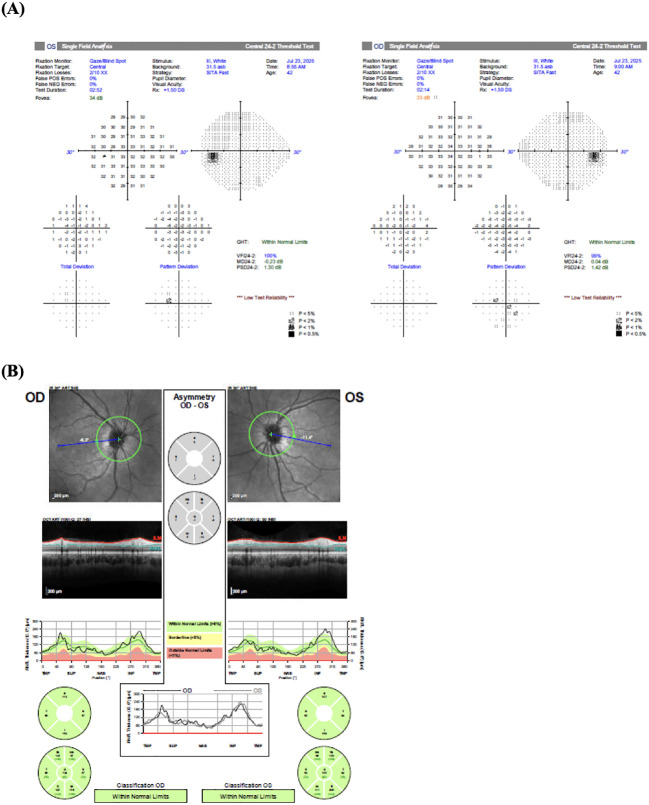 Figure 2. (A) Humphrey visual field testing demonstrated minimal deviations. (B) Optical coherence tomography showed no evidence of papilledema. Source: Case Report: Neuro-ophthalmic manifestations of petroclival meningioma — Frontiers in Ophthalmology 2026; CC BY.
Figure 2. (A) Humphrey visual field testing demonstrated minimal deviations. (B) Optical coherence tomography showed no evidence of papilledema. Source: Case Report: Neuro-ophthalmic manifestations of petroclival meningioma — Frontiers in Ophthalmology 2026; CC BY.
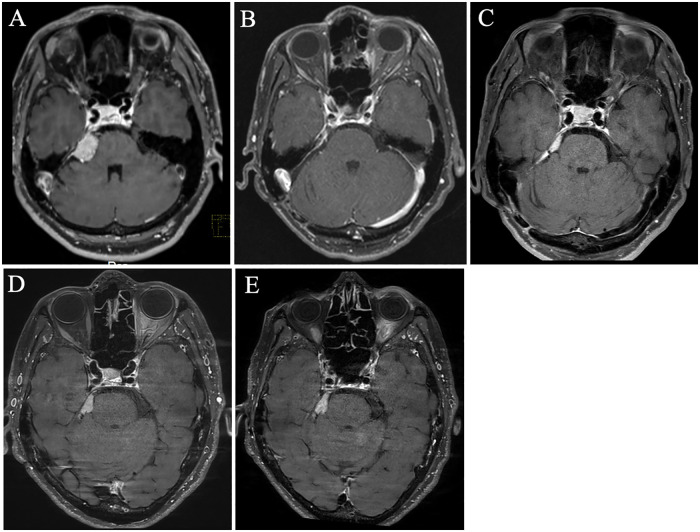 Figure 1. (A) Gadolinum-enhanced T1-weighted magnetic resonance imaging (MRI) at initial presentation shows a right petroclival meningioma. (B) Postoperative MRI demonstrates no residual tumor in… Source: Case Report: Intravenous fosphenytoin successfully treated acute exacerbation of secondary trigeminal neuralgia due to petroclival meningioma — Frontiers in Pain Research 2026; CC BY.
Figure 1. (A) Gadolinum-enhanced T1-weighted magnetic resonance imaging (MRI) at initial presentation shows a right petroclival meningioma. (B) Postoperative MRI demonstrates no residual tumor in… Source: Case Report: Intravenous fosphenytoin successfully treated acute exacerbation of secondary trigeminal neuralgia due to petroclival meningioma — Frontiers in Pain Research 2026; CC BY.
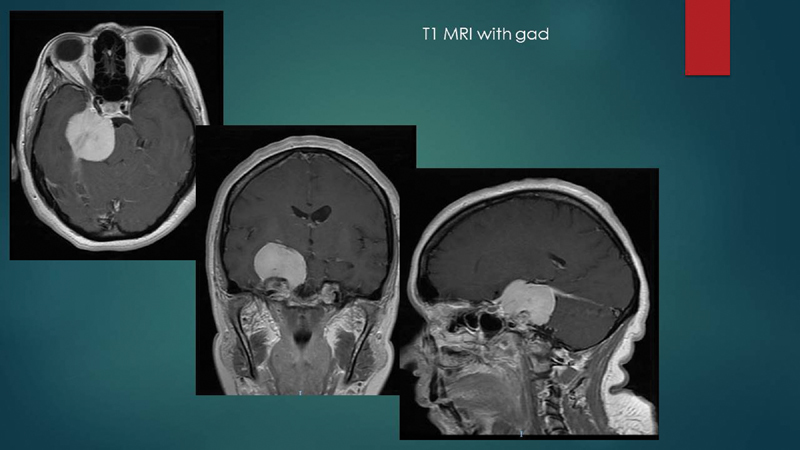 Fig. 1. MRI T1 + gad demonstrates a sizable petroclival meningioma. MRI, magnetic resonance imaging. Source: Staged Approach for Petroclival Meningioma Resection — Journal of Neurological Surgery. Part B, Skull Base 2019; CC BY-NC-ND.
Fig. 1. MRI T1 + gad demonstrates a sizable petroclival meningioma. MRI, magnetic resonance imaging. Source: Staged Approach for Petroclival Meningioma Resection — Journal of Neurological Surgery. Part B, Skull Base 2019; CC BY-NC-ND.
 Figure 7. Source: Drainage patterns of the superficial middle cerebral vein: Effects on perioperative managements of petroclival meningioma — Surg Neurol Int. 2015 Aug 7;6:130. doi: 10.4103/2152-7806.162483; CC BY-NC-SA.
Figure 7. Source: Drainage patterns of the superficial middle cerebral vein: Effects on perioperative managements of petroclival meningioma — Surg Neurol Int. 2015 Aug 7;6:130. doi: 10.4103/2152-7806.162483; CC BY-NC-SA.
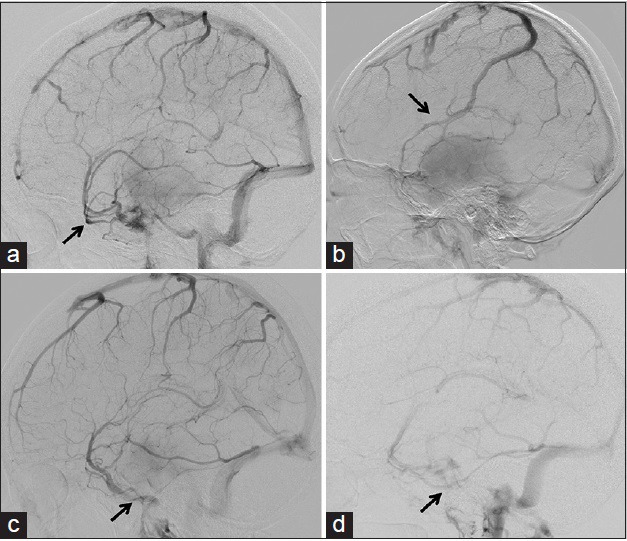 Figure 1. Examples of the four types of superficial middle cerebral vein drainage patterns. (a) Carotid angiogram in venous phase showing the superficial middle cerebral vein draining into the… Source: Drainage patterns of the superficial middle cerebral vein: Effects on perioperative managements of petroclival meningioma — Surgical Neurology International 2015; CC BY-NC-SA.
Figure 1. Examples of the four types of superficial middle cerebral vein drainage patterns. (a) Carotid angiogram in venous phase showing the superficial middle cerebral vein draining into the… Source: Drainage patterns of the superficial middle cerebral vein: Effects on perioperative managements of petroclival meningioma — Surgical Neurology International 2015; CC BY-NC-SA.
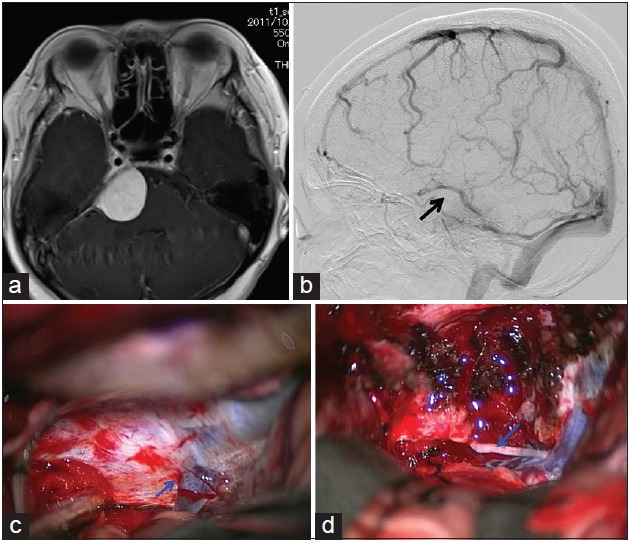 Figure 2. Example of a case in which the superficial middle cerebral vein was absent. (a) T1-weighted magnetic resonance imaging with contrast medium showing a right petroclival meningioma… Source: Drainage patterns of the superficial middle cerebral vein: Effects on perioperative managements of petroclival meningioma — Surgical Neurology International 2015; CC BY-NC-SA.
Figure 2. Example of a case in which the superficial middle cerebral vein was absent. (a) T1-weighted magnetic resonance imaging with contrast medium showing a right petroclival meningioma… Source: Drainage patterns of the superficial middle cerebral vein: Effects on perioperative managements of petroclival meningioma — Surgical Neurology International 2015; CC BY-NC-SA.
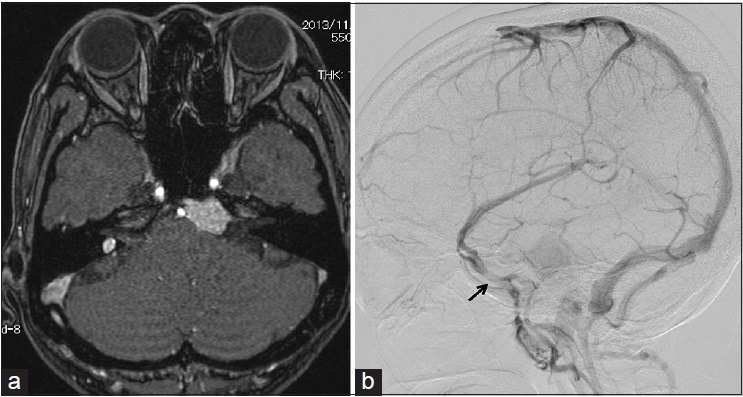 Figure 3. Example of a superficial middle cerebral vein connecting to the sphenobasal vein. (a) T1-weighted magnetic resonance imaging with contrast medium showing a left petrocalival meningioma… Source: Drainage patterns of the superficial middle cerebral vein: Effects on perioperative managements of petroclival meningioma — Surgical Neurology International 2015; CC BY-NC-SA.
Figure 3. Example of a superficial middle cerebral vein connecting to the sphenobasal vein. (a) T1-weighted magnetic resonance imaging with contrast medium showing a left petrocalival meningioma… Source: Drainage patterns of the superficial middle cerebral vein: Effects on perioperative managements of petroclival meningioma — Surgical Neurology International 2015; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Ataxia, trigeminal symptoms, hearing loss, diplopia, facial numbness, headache
- Insidious onset, large at presentation
- CN deficits map to tumor extent (V at petrous apex, VII/VIII at IAC, VI Dorello canal, lower CN at jugular foramen)
Imaging Review
MRI (T1+Gad, T2, CISS) + MRA/MRV
- Origin medial to CN V at petroclival junction (upper clivus, petrous apex)
- Brainstem compression/displacement, pial invasion, T2 cleft (arachnoid plane present?)
- Basilar artery and branches encasement
- CN involvement, cavernous sinus/Meckel cave extension
- Venous anatomy (petrosal vein, sinuses)
CT / CTA
- Petrous bone pneumatization, bony anatomy for petrosectomy, jugular bulb position, sigmoid/transverse sinus dominance
Audiology
- Baseline audiogram (approach selection, BAER)
Labs
- CBC, BMP, Coags, Type and crossmatch
Neurological Examination
- Full CN exam (II-XII), cerebellar, long tracts, gait
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: navigation, endoscope/microscope as approach requires, ENT co-surgeon for endonasal cases, Doppler, lumbar drain only when indicated, reconstruction materials, and visual/endocrine baseline available.
- Special needs: steroid strategy individualized (Cushing workup may require avoiding preop steroids), DI/sodium protocol, AM cortisol/endocrine labs, visual-check plan, arterial line for large/vascular cases, and CSF-leak/nasal precautions.
- Immediate postop orders: neuro and visual checks, strict I/O with sodium/urine specific gravity schedule when pituitary stalk risk exists, cortisol/endocrine replacement plan, nasal precautions, MRI/CT timing, steroid taper, and DVT prophylaxis timing.
Approach Selection (complex, often staged/combined)
- Retrosigmoid: Workhorse; good for tumors with significant posterior fossa/CPA component; familiar, lower morbidity
- Anterior petrosectomy (Kawase): Upper clivus/petrous apex tumors; drills Kawase triangle for petroclival access, preserves hearing
- Posterior petrosectomy (presigmoid: retrolabyrinthine/translabyrinthine/transcochlear): Wide petroclival exposure; hearing trade-offs
- Combined petrosal / staged: Giant tumors
- Realistic goal often subtotal resection + radiosurgery (function preservation prioritized over completeness)
Position
- Lateral/park bench or supine with head turned; Mayfield; mastoid up
Key Surgical Steps (Retrosigmoid example)
- Retrosigmoid craniotomy, expose transverse-sigmoid junction
- Open dura, drain CSF (cisterna magna), relax cerebellum
- Identify CN VII/VIII, V, lower CNs; tumor medial to CN V
- Internal debulking (CUSA/ultrasonic aspirator)
- Dissect capsule off brainstem in arachnoid plane (T2 cleft); preserve perforators to brainstem and basilar branches
- Dissect off CNs (stimulate VII)
- Drill petrous apex (Kawase) if anterior extension needs exposure
- Accept residual on brainstem/basilar/cavernous sinus if no plane → radiosurgery
- Watertight dural closure, fat graft for air cells, prevent CSF leak
Critical Anatomy & Structures at Risk
- Brainstem and perforators — pial invasion; perforator injury devastating
- Basilar artery and branches (AICA, SCA) — encasement
- Cranial nerves III-XII (especially V, VI/Dorello, VII, VIII, lower CNs)
- Venous sinuses, petrosal vein, jugular bulb
- Labyrinth/cochlea (hearing, during petrosectomy)
Equipment
- Microscope, navigation, high-speed drill (petrosectomy), CUSA, ICG
- CN stimulator, fat graft, dural substitute, sealant
Monitoring
- SSEPs, MEPs, BAER, CN EMG (V, VII, VI, lower CNs)
Anesthesia
- Arterial line, crossmatched blood, long case, VAE precautions (if semi-sitting), antiemetics
Potential Complications
- CN deficits (often multiple) — facial, hearing, swallowing, diplopia
- Brainstem injury, perforator stroke
- CSF leak, venous infarction
- Subtotal resection/recurrence (accept for function)
Operative Note Template
Preoperative Diagnosis: [Left/Right] petroclival meningioma with [brainstem compression / CN deficits]
Postoperative Diagnosis: Same
Procedure: [Left/Right] [retrosigmoid / anterior petrosectomy (Kawase)] approach for resection of petroclival meningioma
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids / Blood products: [crossmatched] Adjuncts: Neuronavigation, high-speed drill, CUSA, ICG, CN stimulator; SSEP/MEP/BAER/CN EMG Implants: Dural substitute, fat graft, sealant Complications: None
Indications: [Age]yo [M/F] with a petroclival meningioma causing [ataxia/trigeminal symptoms/hearing loss]. Maximal safe resection was planned with function prioritized over completeness; residual to be followed/radiosurgery. Risks (multiple CN deficits, brainstem/perforator injury, CSF leak) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and neuromonitoring established. The head was fixed and the patient positioned [lateral/park-bench]. A [retrosigmoid craniotomy / anterior petrosectomy with Kawase triangle drilling] was performed and the dura opened with CSF egress to relax the cerebellum.
The cranial nerves (V, VII/VIII, lower CNs) were identified; the tumor lay medial to CN V. The tumor was internally debulked (CUSA) and the capsule dissected off the brainstem in the arachnoid plane (T2 cleft), preserving brainstem perforators and the basilar/AICA/SCA branches and dissecting off the cranial nerves with stimulation. Residual densely adherent to the brainstem, basilar, or cavernous sinus was deliberately left for radiosurgery. A watertight dural closure was performed with a fat graft for the drilled air cells and sealant to prevent CSF leak.
The patient was transferred to the ICU with posterior-fossa/CN precautions.
Postoperative Plan
- ICU, neuro checks q1h, posterior fossa & CN precautions
- CN assessment (facial HB grade, swallow eval before PO, eye care if VII palsy)
- CT 6h, MRI postop; audiogram
- Antiemetics, steroid taper, DVT prophylaxis
- Residual → radiosurgery, surveillance MRI
Chief-Level Case Review
Use these as the senior-level mental model for Petroclival Meningioma Resection:
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Petroclival Meningioma Resection:
- What is the surgical goal: gross-total, maximal safe, decompression, diagnosis, or cytoreduction?
- What eloquent cortex, tract, cranial nerve, vessel, or sinus defines the stopping point?
- What adjunct changes the case: navigation, mapping, 5-ALA, ultrasound, endoscope, ICG, or neuromonitoring?
- What is the edema, steroid, seizure, DVT, and postop imaging plan?
- What complication would you check for first in PACU based on this lesion location?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Extent-of-resection goal and functional stopping points: [attending-specific]
- Mapping/monitoring, 5-ALA, ultrasound, ICG, endoscope, or tractography preferences: [attending-specific]
- Steroid, antiepileptic, mannitol/hypertonic saline, and antibiotic plan: [attending-specific]
- Postop MRI timing, ICU/floor threshold, and adjuvant-referral workflow: [attending-specific]