
Operative Approach: Far-Lateral (Transcondylar) Craniotomy
Case / Approach Snapshot
- Anatomy at risk: corridor-defining nerves, arteries, veins/sinuses, cisterns, bone landmarks, muscle/fascial planes, and closure structures that determine exposure and morbidity.
- Operative steps: confirm position and trajectory, mark landmarks, protect soft tissue and named neurovascular structures, perform the bone/soft-tissue corridor, open/close dura or target compartment deliberately, and verify hemostasis/reconstruction; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: brain relaxation failure, venous or sinus bleeding, cranial nerve/perforator risk, exposure that is too narrow, CSF leak, cosmetic/temporalis/frontalis problems, and conversion to a wider or alternate corridor.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas — Transcondylar · Rhoton CCJ anatomy (PMC) · Radiopaedia — foramen magnum · PubMed Central — far lateral
High-Yield Literature
- Endoscopic Far-Lateral Supracerebellar Infratentorial Approach for Petroclival Region Meningioma: Surgical Technique and Clinical Experience — Xie T. Operative neurosurgery (Hagerstown, Md.) 2022. PubMed
- Gridding Microsurgical Anatomy of Far Lateral Approach in the Three-Dimensional Model — Tang K. The Journal of craniofacial surgery 2019. PubMed
- The far-lateral approach for foramen magnum meningiomas — Flores BC. Neurosurgical focus 2013. PubMed
- Microsurgical anatomy of the transcondylar, supracondylar, and paracondylar extensions of the far-lateral approach — Wen HT. Journal of neurosurgery 1997. PubMed
- Step-by-Step Dissection of the Extreme Lateral Transodontoid Approach to the Anterior Craniovertebral Junction: Surgical Anatomy and Technical Nuances — Abramov I. World neurosurgery 2024. PubMed
- Far lateral craniotomy for disconnection of vertebral dural arteriovenous fistula: how I do it — Rawanduzy C. Acta neurochirurgica 2023. PubMed
- A Microanatomical Study of the Far Lateral Approach — Di G. World neurosurgery 2019. PubMed
- Far-lateral transcondylar approach for microsurgical trapping of an anterior inferior cerebellar artery aneurysm — Caplan JM. Neurosurgical focus 2015. PubMed
- A taxonomy for brainstem cavernous malformations: subtypes of medullary lesions — Catapano JS. Journal of neurosurgery 2023. PubMed
- A modified far-lateral approach for large or giant meningiomas of the posterior fossa — Sanai N. Journal of neurosurgery 2010. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
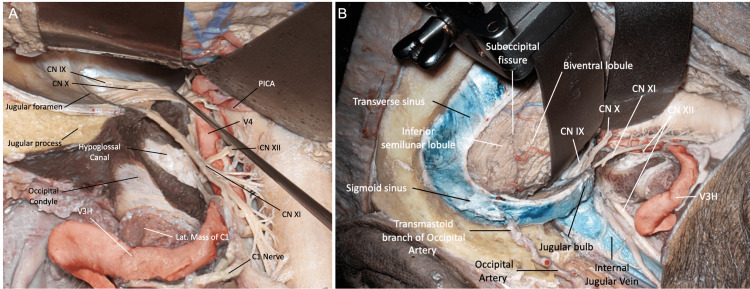 Figure 11. FL modifications. (A) Supracondylar modification. After removal of the jugular tubercle, the anterior medullary cistern and lower clivus can be reached. (B) Paracondylar modification…. Source: Immersive Surgical Anatomy of the Far-Lateral Approach — Cureus 2022; CC BY.
Figure 11. FL modifications. (A) Supracondylar modification. After removal of the jugular tubercle, the anterior medullary cistern and lower clivus can be reached. (B) Paracondylar modification…. Source: Immersive Surgical Anatomy of the Far-Lateral Approach — Cureus 2022; CC BY.
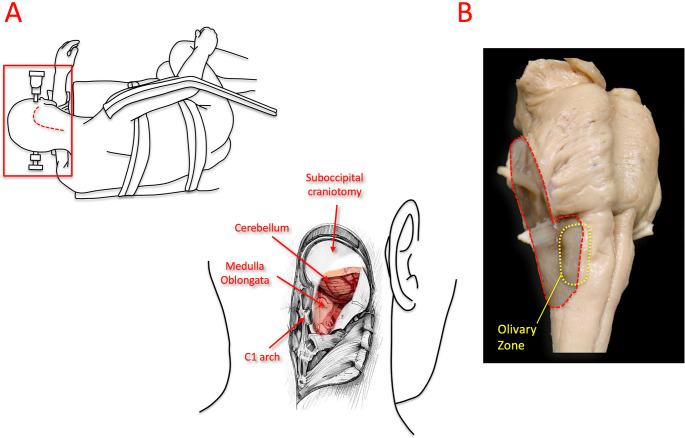 Fig. 1. Positioning and surgical exposure for the far-lateral suboccipital approach. (On Left) Simulated park-bench positioning for the far-lateral suboccipital approach, illustrating the… Source: Anatomical and quantitative analysis of safe entry zones to the lower brainstem through the far-lateral approach — Neurosurgical Review 2026; CC BY.
Fig. 1. Positioning and surgical exposure for the far-lateral suboccipital approach. (On Left) Simulated park-bench positioning for the far-lateral suboccipital approach, illustrating the… Source: Anatomical and quantitative analysis of safe entry zones to the lower brainstem through the far-lateral approach — Neurosurgical Review 2026; CC BY.
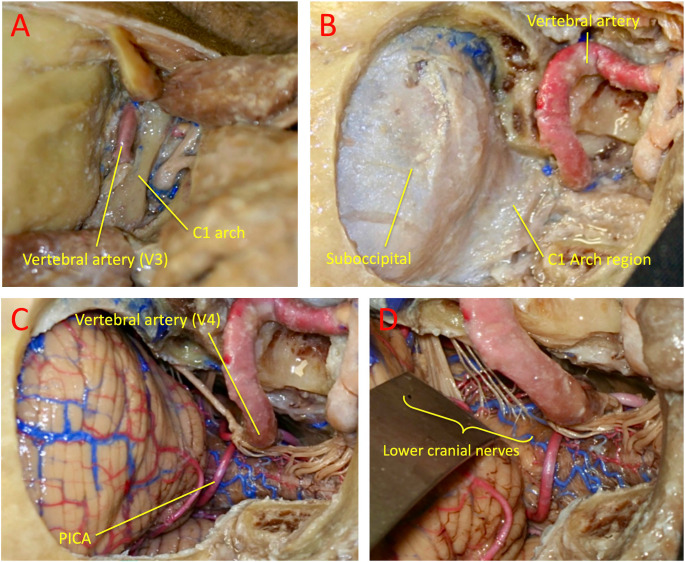 Fig. 2. Stepwise dissection and exposure in the far-lateral suboccipital approach. This approach enables assessment of the horizontal and vertical working angles to the olivary region of the… Source: Anatomical and quantitative analysis of safe entry zones to the lower brainstem through the far-lateral approach — Neurosurgical Review 2026; CC BY.
Fig. 2. Stepwise dissection and exposure in the far-lateral suboccipital approach. This approach enables assessment of the horizontal and vertical working angles to the olivary region of the… Source: Anatomical and quantitative analysis of safe entry zones to the lower brainstem through the far-lateral approach — Neurosurgical Review 2026; CC BY.
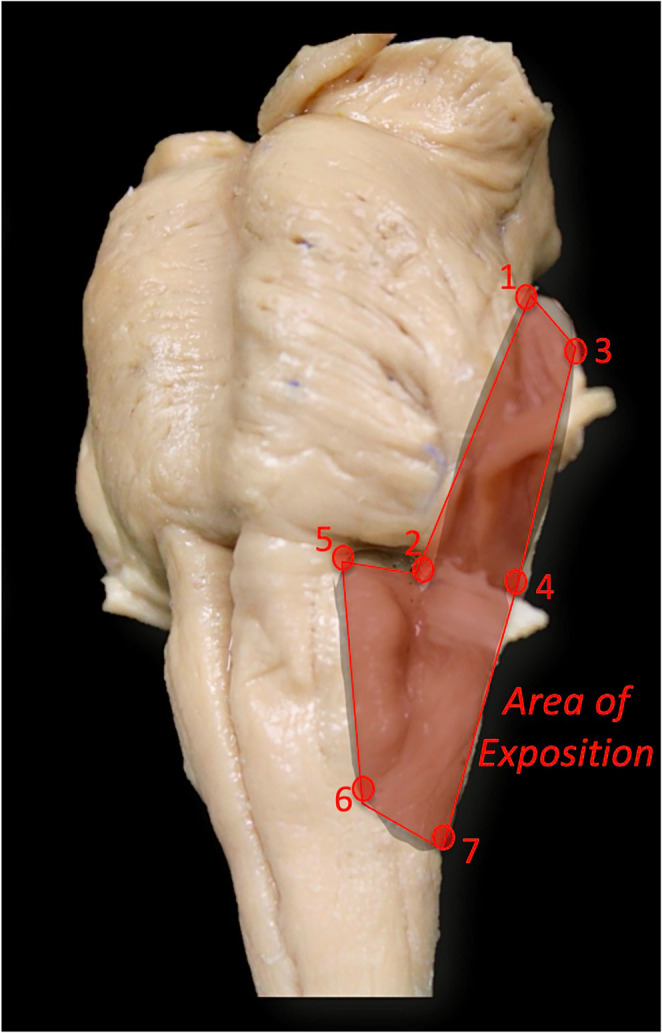 Fig. 3. Definition of the exposure area of the lower brainstem, including the pons and ventrolateral medulla. The following landmarks delimit the outlined region: (1) the most posterior point… Source: Anatomical and quantitative analysis of safe entry zones to the lower brainstem through the far-lateral approach — Neurosurgical Review 2026; CC BY.
Fig. 3. Definition of the exposure area of the lower brainstem, including the pons and ventrolateral medulla. The following landmarks delimit the outlined region: (1) the most posterior point… Source: Anatomical and quantitative analysis of safe entry zones to the lower brainstem through the far-lateral approach — Neurosurgical Review 2026; CC BY.
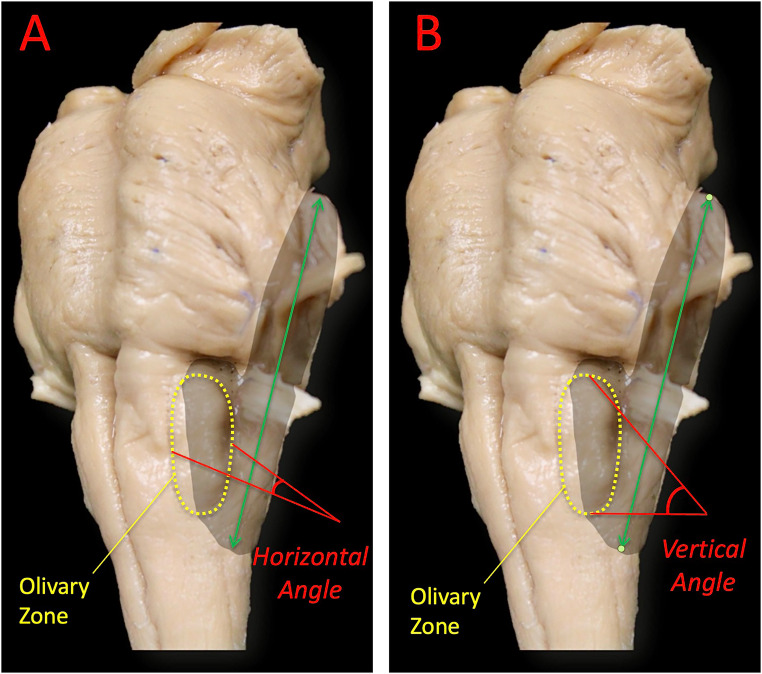 Fig. 4. Microsurgical working angles to the safe entry zone on the medullary olive. A: Horizontal working angle defined by the anterior-most and posterior-most limiting points on the olive,… Source: Anatomical and quantitative analysis of safe entry zones to the lower brainstem through the far-lateral approach — Neurosurgical Review 2026; CC BY.
Fig. 4. Microsurgical working angles to the safe entry zone on the medullary olive. A: Horizontal working angle defined by the anterior-most and posterior-most limiting points on the olive,… Source: Anatomical and quantitative analysis of safe entry zones to the lower brainstem through the far-lateral approach — Neurosurgical Review 2026; CC BY.
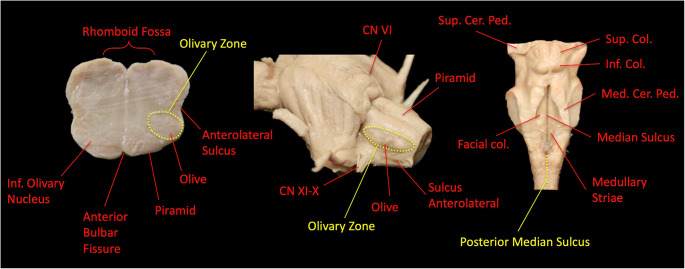 Fig. 5. Anatomical landmarks of the medulla oblongata and identification of safe entry zones. The posterior median sulcus and the olivary zone serve as safe entry pathways to the dorsal and… Source: Anatomical and quantitative analysis of safe entry zones to the lower brainstem through the far-lateral approach — Neurosurgical Review 2026; CC BY.
Fig. 5. Anatomical landmarks of the medulla oblongata and identification of safe entry zones. The posterior median sulcus and the olivary zone serve as safe entry pathways to the dorsal and… Source: Anatomical and quantitative analysis of safe entry zones to the lower brainstem through the far-lateral approach — Neurosurgical Review 2026; CC BY.
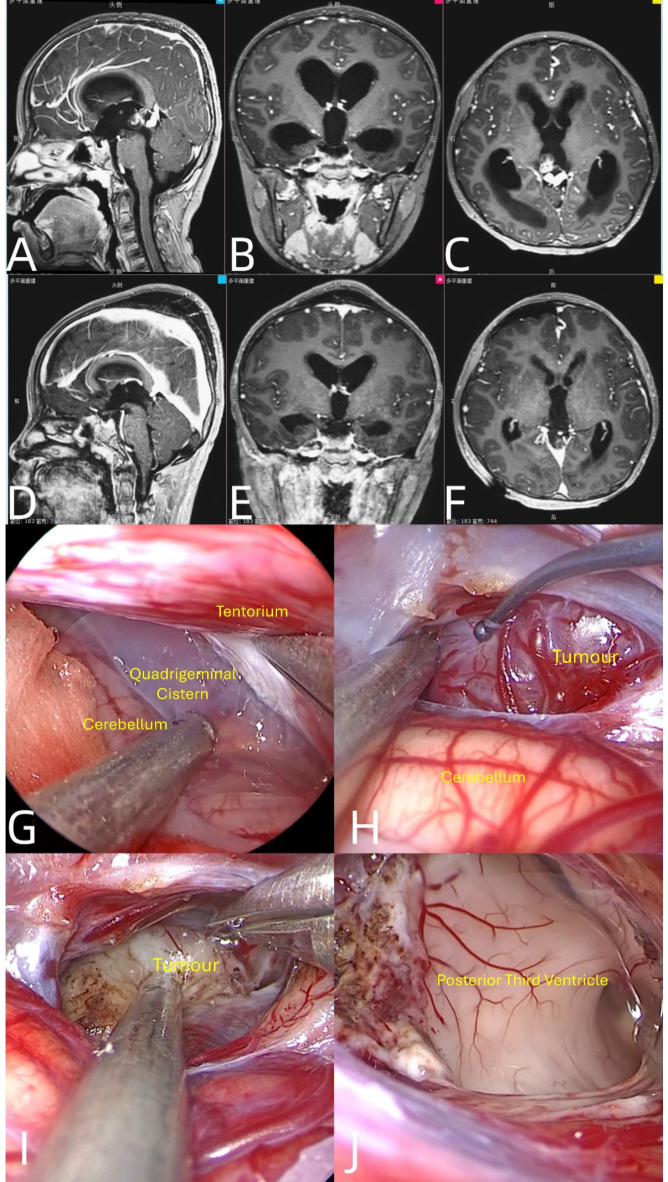 Fig. 1. Magnetic resonance imaging (MRI) and intraoperative images of pineal region tumours. (A-C) Preoperative MR image. (D-E) Postoperative MR image. (G) Opening of the quadruple pool. (H) Red… Source: Clinical outcomes of the neuroendoscopic far lateral supracerebellar infratentorial approach for resection of deep brain lesions — Scientific Reports 2025; CC BY-NC-ND.
Fig. 1. Magnetic resonance imaging (MRI) and intraoperative images of pineal region tumours. (A-C) Preoperative MR image. (D-E) Postoperative MR image. (G) Opening of the quadruple pool. (H) Red… Source: Clinical outcomes of the neuroendoscopic far lateral supracerebellar infratentorial approach for resection of deep brain lesions — Scientific Reports 2025; CC BY-NC-ND.
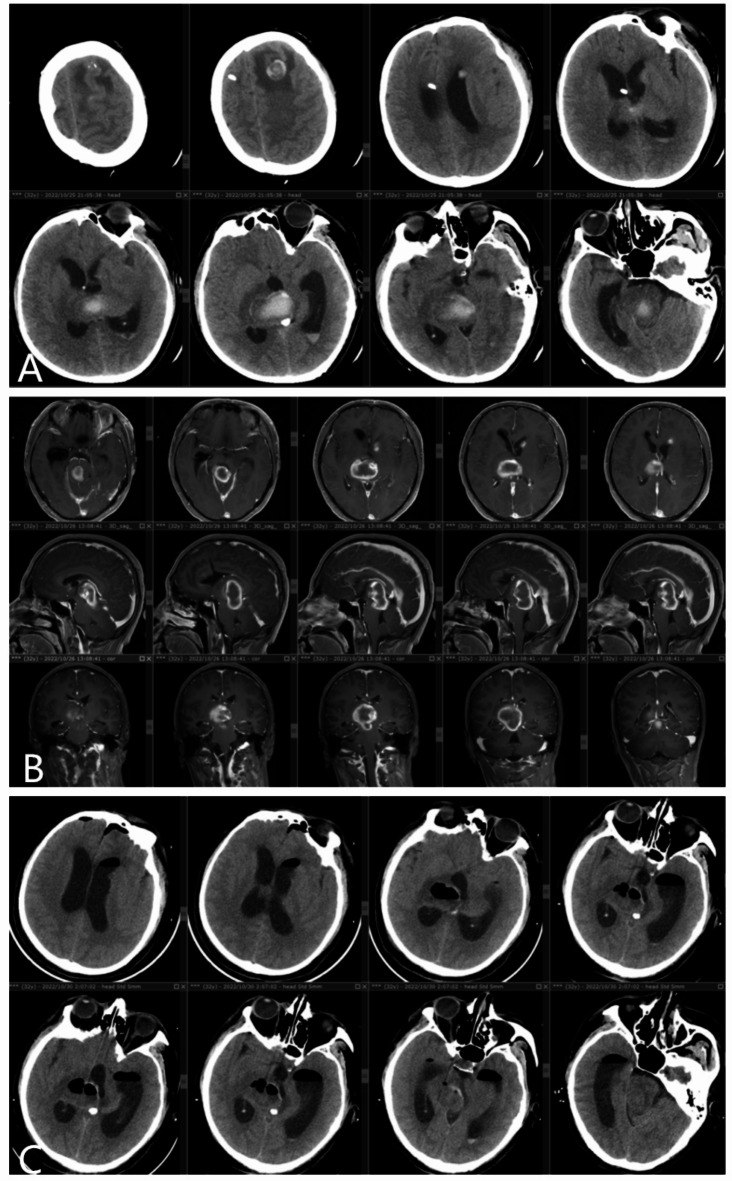 Fig. 2. Imaging data of patients with thalamic haematoma. (A) Preoperative cranial CT revealed a right thalamic haematoma and left frontal lobe haematoma. (B) Preoperative MR image. (C)… Source: Clinical outcomes of the neuroendoscopic far lateral supracerebellar infratentorial approach for resection of deep brain lesions — Scientific Reports 2025; CC BY-NC-ND.
Fig. 2. Imaging data of patients with thalamic haematoma. (A) Preoperative cranial CT revealed a right thalamic haematoma and left frontal lobe haematoma. (B) Preoperative MR image. (C)… Source: Clinical outcomes of the neuroendoscopic far lateral supracerebellar infratentorial approach for resection of deep brain lesions — Scientific Reports 2025; CC BY-NC-ND.
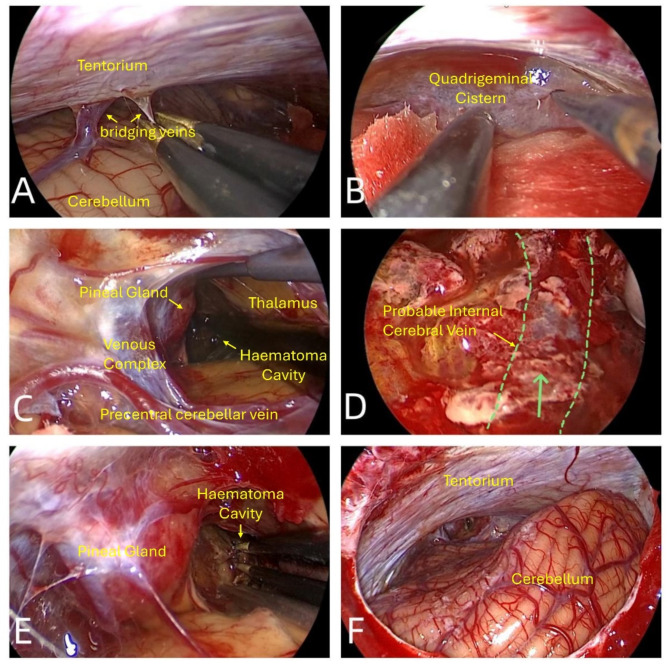 Fig. 3. Intraoperative images of patients with thalamic haematoma. (A) Electrocoagulation and devascularization of the bridging vein. (B) Opening of the arachnoid. (C) Thalamic haematoma. (D)… Source: Clinical outcomes of the neuroendoscopic far lateral supracerebellar infratentorial approach for resection of deep brain lesions — Scientific Reports 2025; CC BY-NC-ND.
Fig. 3. Intraoperative images of patients with thalamic haematoma. (A) Electrocoagulation and devascularization of the bridging vein. (B) Opening of the arachnoid. (C) Thalamic haematoma. (D)… Source: Clinical outcomes of the neuroendoscopic far lateral supracerebellar infratentorial approach for resection of deep brain lesions — Scientific Reports 2025; CC BY-NC-ND.
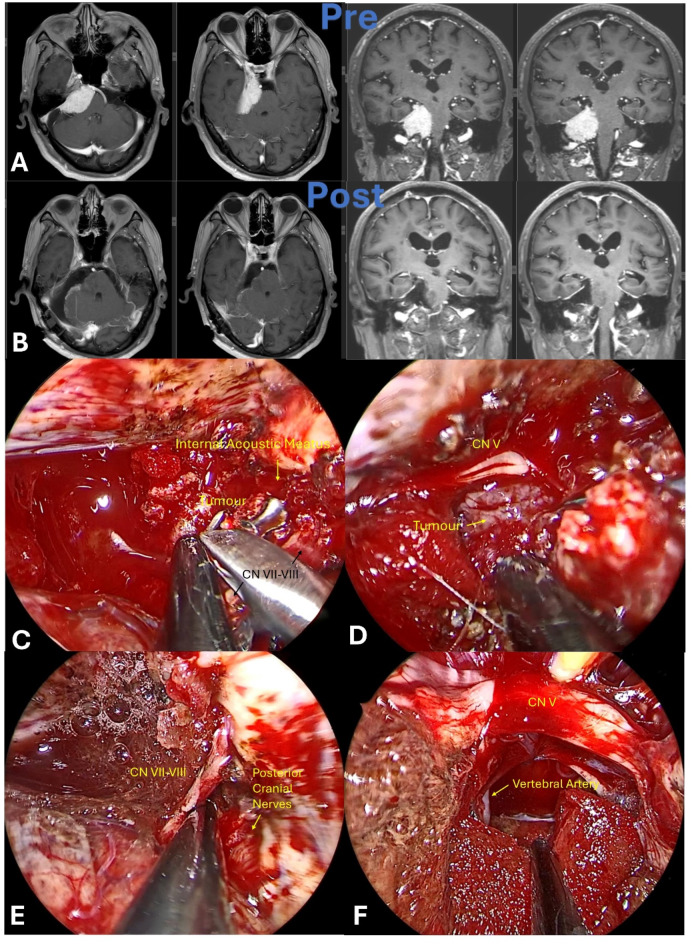 Fig. 4. Magnetic resonance imaging (MRI) and intraoperative images of petroclival meningioma. (A) Preoperative MR image. (B) Postoperative MR image. (C) The tumor encircles the acoustic-facial… Source: Clinical outcomes of the neuroendoscopic far lateral supracerebellar infratentorial approach for resection of deep brain lesions — Scientific Reports 2025; CC BY-NC-ND.
Fig. 4. Magnetic resonance imaging (MRI) and intraoperative images of petroclival meningioma. (A) Preoperative MR image. (B) Postoperative MR image. (C) The tumor encircles the acoustic-facial… Source: Clinical outcomes of the neuroendoscopic far lateral supracerebellar infratentorial approach for resection of deep brain lesions — Scientific Reports 2025; CC BY-NC-ND.
The far-lateral craniotomy is the posterolateral corridor to the ventral and ventrolateral craniocervical junction — the anterior foramen magnum, lower clivus, ventral medulla, and the lower cranial nerves (IX–XII), the distal vertebral artery (VA), the vertebrobasilar junction, and PICA. By removing the lateral rim of the foramen magnum, the posterior arch of C1, and (when needed) the posterior third of the occipital condyle, the surgeon looks along the ventral surface of the medulla — reaching lesions in front of the brainstem without any brainstem retraction.
General Considerations
- What it accesses: ventral/ventrolateral foramen magnum and lower clivus, the ventral medulla and cervicomedullary junction, CN IX–XII, the V3 (extradural horizontal) and V4 (intradural) vertebral artery, PICA origin, and the vertebrobasilar junction.
- Core principle: the obstacle to seeing the front of the medulla is bone (condyle/foramen magnum rim), not brain. Removing lateral bone — rather than retracting the neuraxis — converts a deep ventral target into a tangential, retractor-free exposure.
- The graded “condylar” ladder (Salas/Rhoton):
- Far-lateral (retrocondylar): lateral suboccipital craniectomy + lateral foramen-magnum rim + C1 hemilaminectomy, without condyle removal — adequate for many dorsolateral lesions.
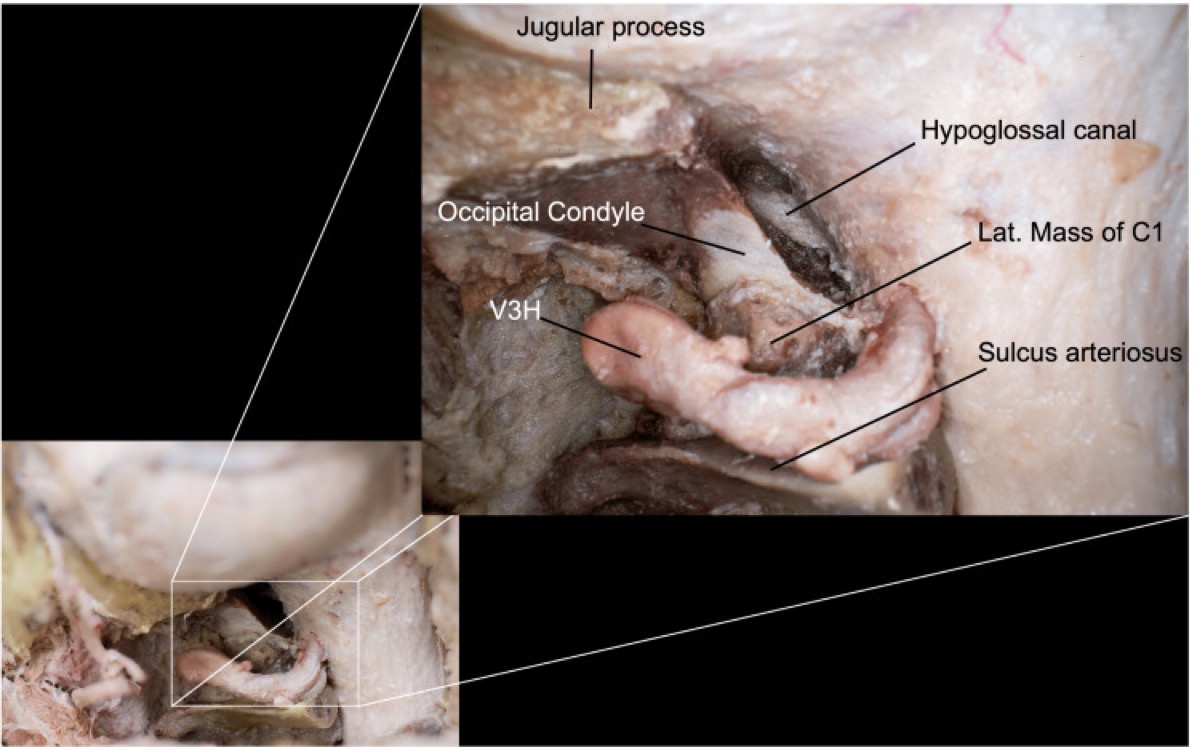
- Transcondylar: add resection of the posterior third of the occipital condyle (and the lateral C1 mass as needed) to flatten the ventral trajectory — the workhorse extension; the hypoglossal canal is the anteromedial limit.
- Supracondylar: drill the jugular tubercle (above the condyle) for ventral clival/CN access.
- Paracondylar: remove bone lateral to the condyle toward the jugular process for jugular-foramen/glomus lesions.
Indications
- Ventral/ventrolateral foramen magnum meningioma (the prototypical indication) → see foramen-magnum-meningioma-far-lateral.md
- VA, VA–PICA, and vertebrobasilar junction aneurysms
- Lower clivus / CCJ chordoma and chondrosarcoma → see clival-chordoma.md
- Jugular foramen tumors (paracondylar extension), hypoglossal schwannoma → see jugular-foramen-tumor.md
- Cervicomedullary intramedullary lesions, PICA territory exposure
Relevant Surgical Anatomy
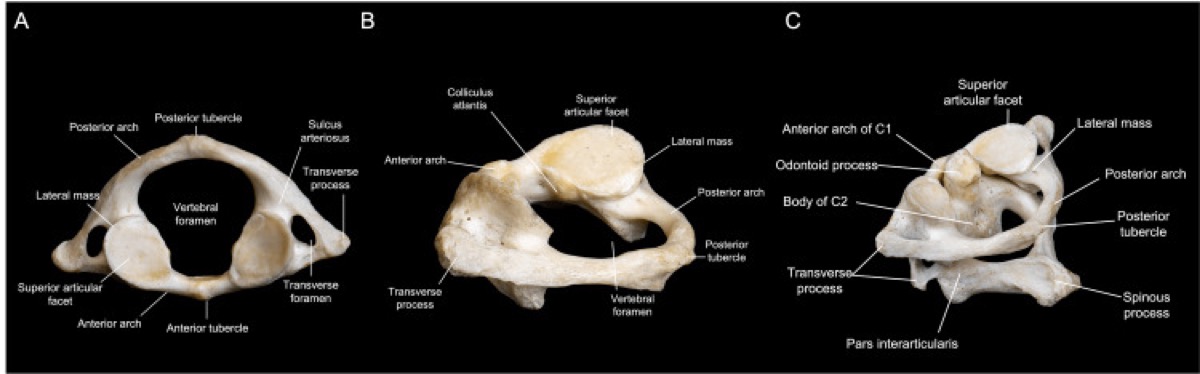
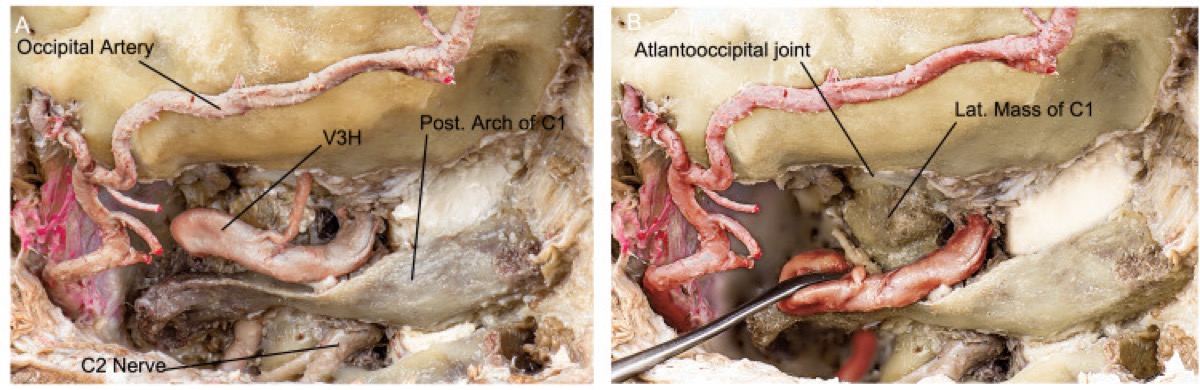
- Suboccipital triangle: bounded by rectus capitis posterior major (medial), superior oblique (superolateral), and inferior oblique (inferolateral); its floor contains the horizontal V3 segment of the VA lying in the sulcus arteriosus on the superior surface of the C1 posterior arch, surrounded by a dense suboccipital venous plexus. This triangle is the key to safe VA control.
- Vertebral artery course: ascends through the C2→C1 transverse foramina (V3), turns medially and posteriorly along the C1 sulcus, then pierces the dura at the foramen magnum to become V4 intradurally. Anomalies matter: an extradural PICA origin or a fenestrated/duplicated VA can be injured during muscle/bone work.
- Occipital condyle & hypoglossal canal: the condyle sits at the anterolateral foramen magnum; the hypoglossal canal (CN XII) runs anteromedially through its base — the medial-anterior limit of safe condyle drilling. Resecting >~50% of a condyle risks craniocervical instability (consider occipitocervical fusion).
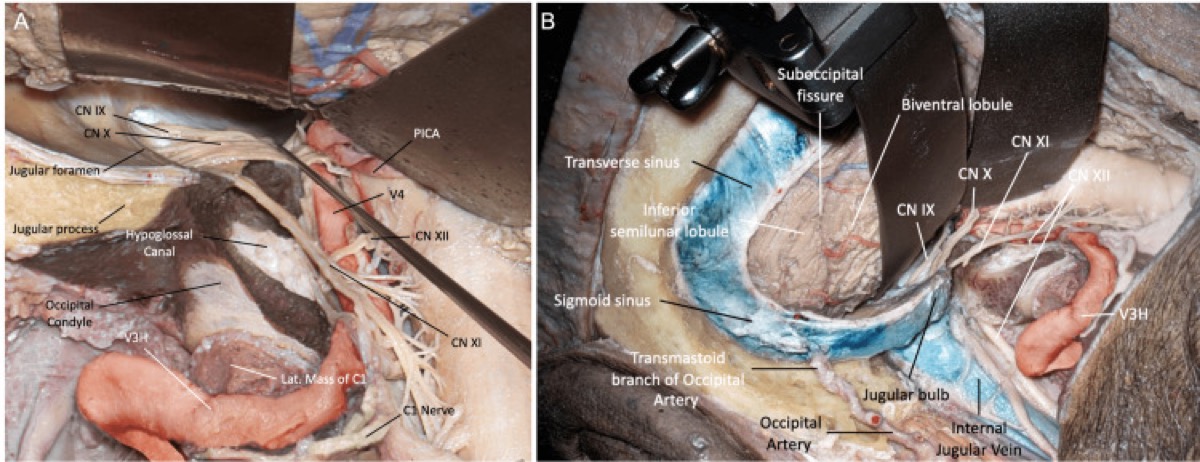
- Intradural lower CNs: CN XI spinal rootlets ascend along the lateral cord; CN IX–X–XI converge to the jugular foramen; CN XII rootlets run between the VA and the medulla to the hypoglossal canal. The dentate ligament is a landmark (and can be divided to rotate the cord for ventral access).
Preoperative Evaluation
- MRI for the lesion and its relation to the medulla, lower CNs, and VA; CTA/CT angiogram for the VA course, dominance, PICA origin, and any anomaly, and for condyle/jugular-tubercle bony anatomy and the hypoglossal canal.
- Assess baseline lower cranial nerve function and swallowing (aspiration risk); flexion-extension imaging if CCJ instability is a question.
- Plan condyle-resection extent preoperatively; counsel about possible occipitocervical fusion and lower-CN deficits.
Logistics, OR Setup & Orders
- OR setup: Mayfield, microscope/endoscope as needed, navigation, cranial nerve monitoring/BAER when relevant, Doppler/air-embolism readiness for sitting or semisitting positions, and watertight closure materials.
- Special needs: arterial line, Foley, antiemetic plan, dexamethasone when tumor/edema risk warrants it, EVD/CSF diversion plan, VAE monitoring when sitting, and lower-CN airway/swallow contingency.
- Immediate postop orders: posterior fossa neuro checks, CN V-XII and swallow/voice screen, HOB elevation, CT for hemorrhage/hydrocephalus when indicated, MRI for tumor EOR, CSF leak/pseudomeningocele watch, and nausea control.
Anesthesia & Neuromonitoring
- GA/TIVA; no long-acting paralytic (CN EMG). SSEP/MEP, lower-CN EMG (IX/X via vocalis, XI trapezius/SCM, XII tongue), and brainstem monitoring.
- If a sitting/semi-sitting position is chosen: VAE precautions (precordial Doppler, end-tidal CO₂, right-atrial line) and PFO screening. Most surgeons use park-bench/lateral to avoid this.
Positioning
- Park-bench (lateral) is the workhorse: patient lateral, operative side up, in Mayfield fixation; the dependent arm is supported off the table edge in a sling, axillary roll in place.
- Head maneuver (three moves) to bring the ventral foramen magnum into view: (1) flexion (chin toward sternum), (2) rotation ~30–45° toward the floor/contralateral side, and (3) lateral flexion of the head toward the contralateral shoulder. The mastoid becomes the highest point and the surgeon looks up the ventral medulla.
- Ipsilateral shoulder taped down caudally to open the cervico-mastoid angle; verify venous outflow and recheck IONM after positioning.
Incision & Soft-Tissue Dissection
- Hockey-stick (inverted-J) incision: down the midline from the inion to ~C3–C4, then curving laterally along the superior nuchal line toward the mastoid — or a C-shaped/“lazy-S” flap. The midline limb uses the avascular nuchal raphe.
- Reflect a myocutaneous flap inferolaterally, taking the suboccipital muscles off the occiput and C1; leave a muscular/nuchal cuff superiorly for watertight closure.
- Identify the VA early in the suboccipital triangle: dissect subperiosteally on the superior surface of the C1 posterior arch from medial to lateral, staying on bone, to expose V3 in its sulcus within the venous plexus. Control plexus bleeding with flowable hemostatic/gentle packing; skeletonize and protect (and, if transposition is needed, mobilize) the VA.
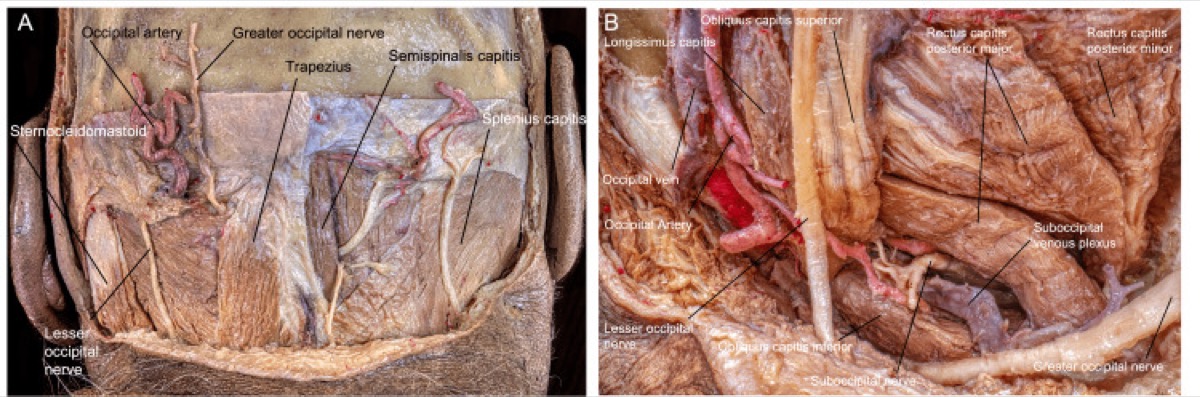
Payman A, et al. “Immersive Surgical Anatomy of the Far-Lateral Approach,” Cureus 2022;14(11):e31257 — CC BY. Muscular, vascular (VA), and nervous anatomy of the corridor.
Bone Work — Craniotomy, C1, and the Condyle
Craniotomy / craniectomy + C1
- Lateral suboccipital craniotomy/craniectomy carried laterally to the sigmoid sinus and inferiorly to the foramen magnum; remove the lateral rim of the foramen magnum (the key maneuver of the basic far-lateral).
- C1 hemilaminectomy out to the VA sulcus / transverse foramen (protect V3). Wax the abundant venous bleeding.
Condyle / jugular tubercle (extensions as needed)
- Transcondylar: drill the posterior third of the occipital condyle to flatten the ventral trajectory; the hypoglossal canal is the anteromedial stop (identify it; the emissary/condylar veins herald it). Tailor the extent to the lesion — only remove what the trajectory requires.
- Supracondylar (jugular tubercle) / paracondylar drilling added for ventral clival or jugular-foramen reach.
- If condyle resection approaches/exceeds ~50% (or with pre-existing laxity), plan occipitocervical fusion — see occipitocervical-fusion.md.
Payman A, et al. Cureus 2022;14(11):e31257 — CC BY.
Dural Opening & Intradural Work
- Open the dura in a curvilinear/C- or T-shaped flap based on the sigmoid sinus, carrying the limb across the VA dural entry (a dural cuff around V4 is preserved/repaired); tack toward the sinus. Beware the posterior spinal artery and the dural VA ring.
- Release CSF from the cisterna magna; the cerebellum and tonsil relax. Identify the lower CNs (XI rootlets along the cord first, then X and IX to the jugular foramen, XII rootlets between VA and medulla), PICA, and V4.
- Divide the dentate ligament (and, if needed, the highest dorsal rootlet) to rotate the cord and widen the ventral corridor. Work between the CN rootlets to reach a ventral meningioma (which displaces the neuraxis dorsally) or the VA/PICA/vertebrobasilar lesion. Preserve every perforator to the medulla.
Closure
- Watertight dura, almost always with a graft (the VA cuff and condyle defect make primary closure difficult) + sealant; fat graft the condylar/retromastoid defect; wax all air cells.
- If the bone flap was free, replace it (cranioplasty); perform occipitocervical fusion if condyle resection or instability warrants.
- Reapproximate the suboccipital muscles in layers to the superior cuff (second defense against CSF leak/pseudomeningocele). Layered closure.
Further operative anatomy & technique
Payman A et al., Cureus 2022;14(11):e31257 — CC BY 4.0.
Payman A et al., Cureus 2022;14(11):e31257 — CC BY 4.0.
Payman A et al., Cureus 2022;14(11):e31257 — CC BY 4.0.
Nuances & Pitfalls (surgeon-level)
- The vertebral artery is the case. Identify V3 early in the suboccipital triangle on the superior C1 arch, dissect on bone, and control the venous plexus deliberately. Know the VA dominance and PICA origin (including a rare extradural PICA) from the CTA before you start.
- Hypoglossal canal = stop sign. It is the anteromedial limit of condyle drilling; breaching it risks CN XII palsy (tongue deviation, dysarthria).
- Tailor the condyle. More condyle = more ventral angle but more instability; remove only what the trajectory needs, and fuse (occipitocervical) if >~50% is taken or the joint is incompetent.
- Lower-CN vigilance. Manipulating IX–XI risks dysphagia/aspiration and hoarseness; coordinate hemodynamics with anesthesia and assess swallowing before feeding postoperatively.
- Venous plexus bleeding around V3 and the condylar emissary veins is brisk — flowable hemostatics and patience, not blind bipolar near the VA.
- CSF leak is the commonest morbidity — meticulous air-cell waxing, fat graft, grafted watertight dura, and tight muscle closure.
Complications
VA injury / occlusion (medullary/cerebellar infarct); lower-CN palsies (IX–XII) with dysphagia/aspiration, hoarseness, tongue weakness; craniocervical instability (condyle resection); CSF leak / pseudomeningocele; cerebellar/medullary injury or perforator stroke; venous air embolism (if sitting); wound infection/meningitis.
Cross-links
- Related corridors: retrosigmoid-craniotomy.md · midline-suboccipital-craniotomy.md · presigmoid-petrosal-approach.md
- Pathology: foramen-magnum-meningioma-far-lateral.md · jugular-foramen-tumor.md · clival-chordoma.md · occipitocervical-fusion.md
Figure Use & Attribution
About the figures. Copyrighted operative figures/videos are linked (Neurosurgical Atlas, Rhoton); embedded images are public-domain (Gray’s Anatomy) or CC‑BY (open-access cadaveric anatomy), credited beneath each image. See media-sources.md and figures/CREDITS.md.
Atlas chapters & neuroanatomy: Far-Lateral Suboccipital (Transcondylar) Approach · Far-Lateral & Transcondylar Approaches (Neuroanatomy) · Far-Lateral Approach & Extensions
Chief-Level Corridor Review
Use these as the senior-level mental model for Far-Lateral (Transcondylar) Craniotomy:
- Decision point: Define the exposure goal before incision: target, working angles, proximal/distal control, and the structure that cannot tolerate retraction.
- Technical lever: Know the first irreversible step: bone removal, dural opening, vascular control, or muscle/fascial division that commits the corridor.
- Bailout: Verbalize the bailout: extend exposure, change trajectory, add CSF drainage, obtain proximal control, convert to a larger corridor, or stop for imaging.
- Postop watch: Protect closure from the start: vascularized tissue, watertight dural/reconstruction plan, dead-space control, and drain strategy should be chosen before the final intradural step.
Common Pimp Questions
Use these to pressure-test preparation for Far-Lateral (Transcondylar) Craniotomy:
- What patient position and head rotation make gravity work for this corridor?
- What named nerve, vessel, sinus, or muscle/fascial plane is most commonly injured?
- What bone work or soft-tissue step creates the exposure rather than simply using more retraction?
- What is the bailout if exposure is inadequate, bleeding occurs, or the brain is tight?
- What closure maneuver prevents the signature complication of this approach?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Exact head rotation/flexion/extension and pin placement: [attending-specific]
- Skin incision length, flap type, and muscle/fascial preservation technique: [attending-specific]
- Drill, rongeur, endoscope, microscope, retractor, and navigation preferences: [attending-specific]
- Drain use, closure materials, watertightness threshold, and postop imaging routine: [attending-specific]
Case Guides Using This Approach
- Foramen Magnum Meningioma — Far Lateral Approach
- Jugular Foramen Tumor (Glomus Jugulare / Schwannoma / Meningioma)
- Occipitocervical Fusion
References
- Heros RC. Lateral suboccipital approach for vertebral and vertebrobasilar artery lesions. J Neurosurg. 1986;64(4):559–562.
- Rhoton AL Jr. The far-lateral approach and its transcondylar, supracondylar, and paracondylar extensions. Neurosurgery. 2000;47(3 Suppl):S195–S209.
- Salas E, Sekhar LN, Ziyal IM, et al. Variations of the extreme-lateral craniocervical approach. J Neurosurg (Spine). 1999;90(2 Suppl):206–219.
- Wen HT, Rhoton AL Jr, et al. Microsurgical anatomy of the transcondylar, supracondylar, and paracondylar extensions of the far-lateral approach. J Neurosurg. 1997;87(4):555–585.
- Payman A, Rios Zermeno J, Hirpara A, El-Sayed IH, Abla A, Rodriguez Rubio R. Immersive Surgical Anatomy of the Far-Lateral Approach. Cureus. 2022;14(11):e31257. CC BY. PMC9733796
- Cohen-Gadol AA. Far-Lateral Suboccipital (Transcondylar) Approach. The Neurosurgical Atlas. link