
Case Prep: Vestibular Schwannoma (Acoustic Neuroma) Resection
Case / Approach Snapshot
- Anatomy at risk: tumor compartment, arterial supply, venous drainage/sinuses, cranial nerves, white-matter tracts, pituitary/CSF pathways when relevant, and functional cortex.
- Operative steps: review imaging and goals, choose exposure, obtain brain relaxation, devascularize when possible, debulk internally, dissect capsule from critical structures, verify extent/safety, and reconstruct watertight closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: venous or arterial injury, swelling, seizure, cranial nerve or endocrine change, CSF leak, residual tumor left for safety, staged surgery, radiation, or adjuvant therapy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [size] cm [left/right] vestibular schwannoma (Koos grade [I-IV]) presenting with [hearing loss/tinnitus/facial numbness/imbalance] planned for [retrosigmoid/translabyrinthine/middle fossa] craniotomy for [gross total/near total/subtotal] resection.
Figures, Imaging & Video
🎥 Operative video — Extended Retrosigmoid Craniotomy for Vestibular Schwannoma · Barrow Neurological Institute
More operative video: YouTube ▸ · Neurosurgical Atlas ▸
🧭 Operative approach: Retrosigmoid craniotomy — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
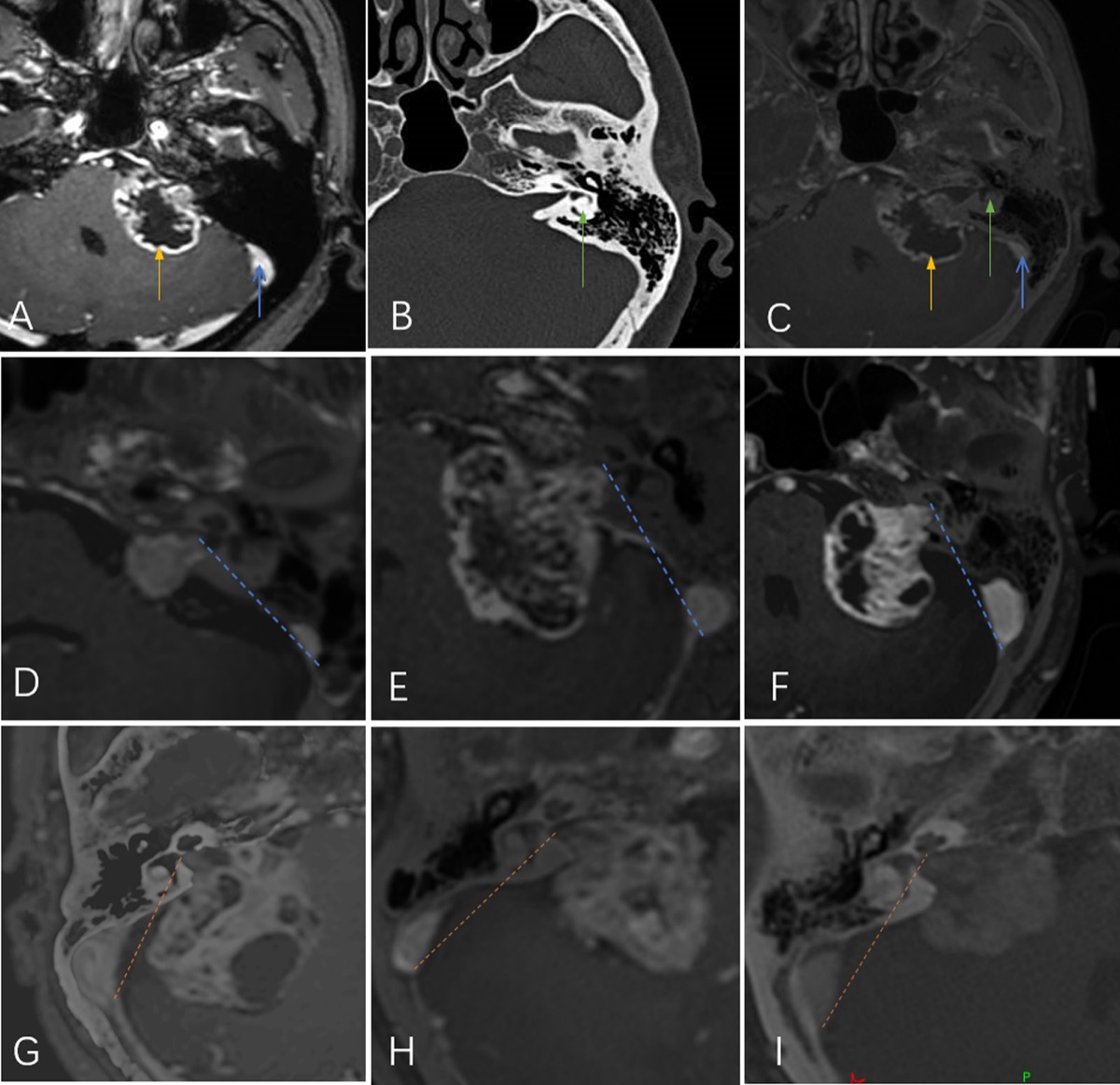
MRI/CT fusion: tumor (yellow), sigmoid sinus (blue), labyrinth (green); lateral vs medial type relative to the lateral safe line. Source: Jia et al., Front Surg 2022;9:889402, Fig 1. CC BY 4.0.
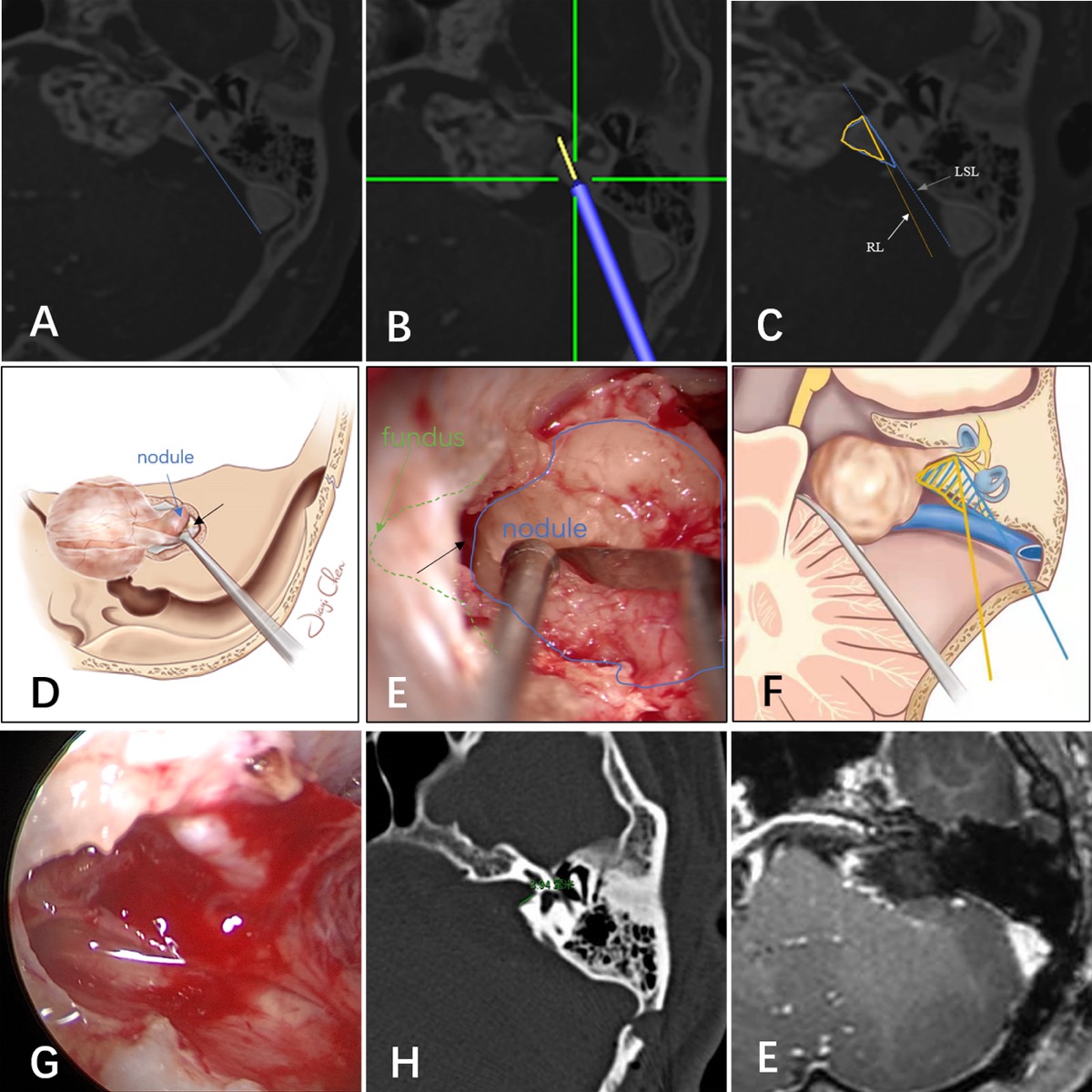
Microscopic view of the intrameatal tumor (blue) / IAC fundus (green) interface, with postop imaging confirming complete resection and intact labyrinth. Source: Jia et al., Front Surg 2022;9:889402, Fig 3. CC BY 4.0.
High-Yield Literature
- EANO guideline on the diagnosis and treatment of vestibular schwannoma — Goldbrunner R. Neuro-oncology 2020. PubMed
- Vestibular schwannoma microsurgical technique — Rutherford SA. Handbook of clinical neurology 2025. PubMed
- Hearing Rehabilitation in Vestibular Schwannoma — Mankekar G. Audiology research 2023. PubMed
- Genomics of vestibular schwannoma — Smith MJ. Handbook of clinical neurology 2025. PubMed
- The inflammatory microenvironment in vestibular schwannoma — Hannan CJ. Neuro-oncology advances 2020. PubMed
- Retrosigmoid approach to vestibular schwannoma — Shapey J. Handbook of clinical neurology 2025. PubMed
- Hearing Aid in Vestibular-Schwannoma-Related Hearing Loss: A Review — Di Pasquale Fiasca VM. Audiology research 2023. PubMed
- History of vestibular schwannoma management — Ramsden R. Handbook of clinical neurology 2025. PubMed
- Management of Complications in Vestibular Schwannoma Surgery — Kutz JW Jr. Otolaryngologic clinics of North America 2023. PubMed
- Vestibular schwannoma unveiled by pregnancy: A case report and literature review — Kadir V. European journal of obstetrics, gynecology, and reproductive biology 2024. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
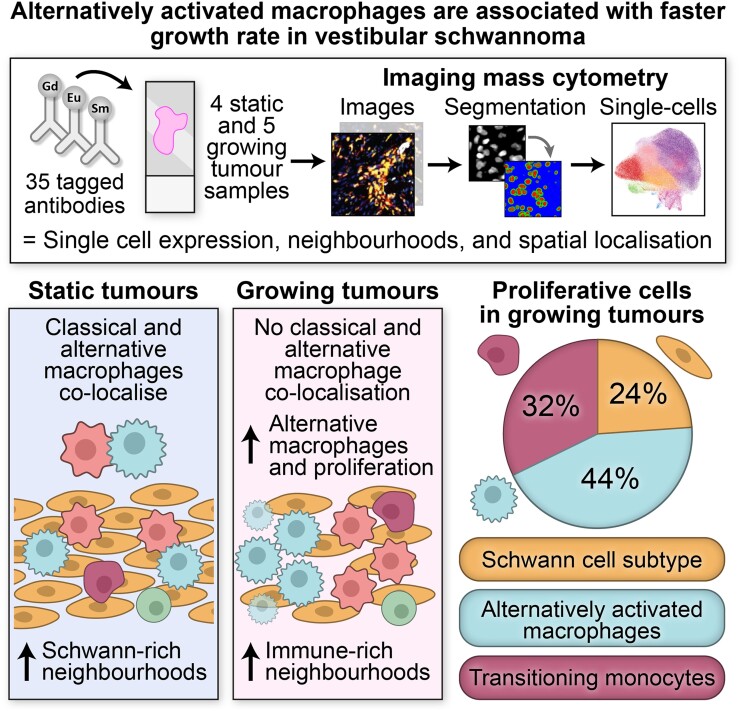 Graphical Abstract. Source: Alternatively activated macrophages are associated with faster growth rate in vestibular schwannoma — Brain Communications 2024; CC BY.
Graphical Abstract. Source: Alternatively activated macrophages are associated with faster growth rate in vestibular schwannoma — Brain Communications 2024; CC BY.
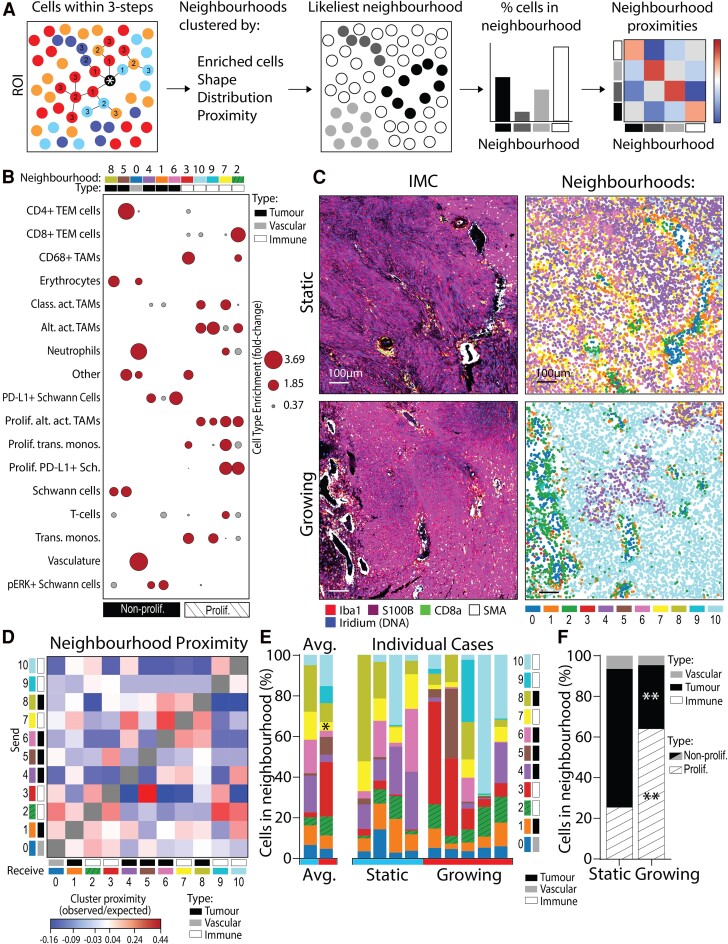 Figure 3. Growing VS have more cells residing in proliferative, immune-enriched neighbourhoods. (A) Schematic detailing how the cells within a three-step connection from the target cell define a… Source: Alternatively activated macrophages are associated with faster growth rate in vestibular schwannoma — Brain Communications 2024; CC BY.
Figure 3. Growing VS have more cells residing in proliferative, immune-enriched neighbourhoods. (A) Schematic detailing how the cells within a three-step connection from the target cell define a… Source: Alternatively activated macrophages are associated with faster growth rate in vestibular schwannoma — Brain Communications 2024; CC BY.
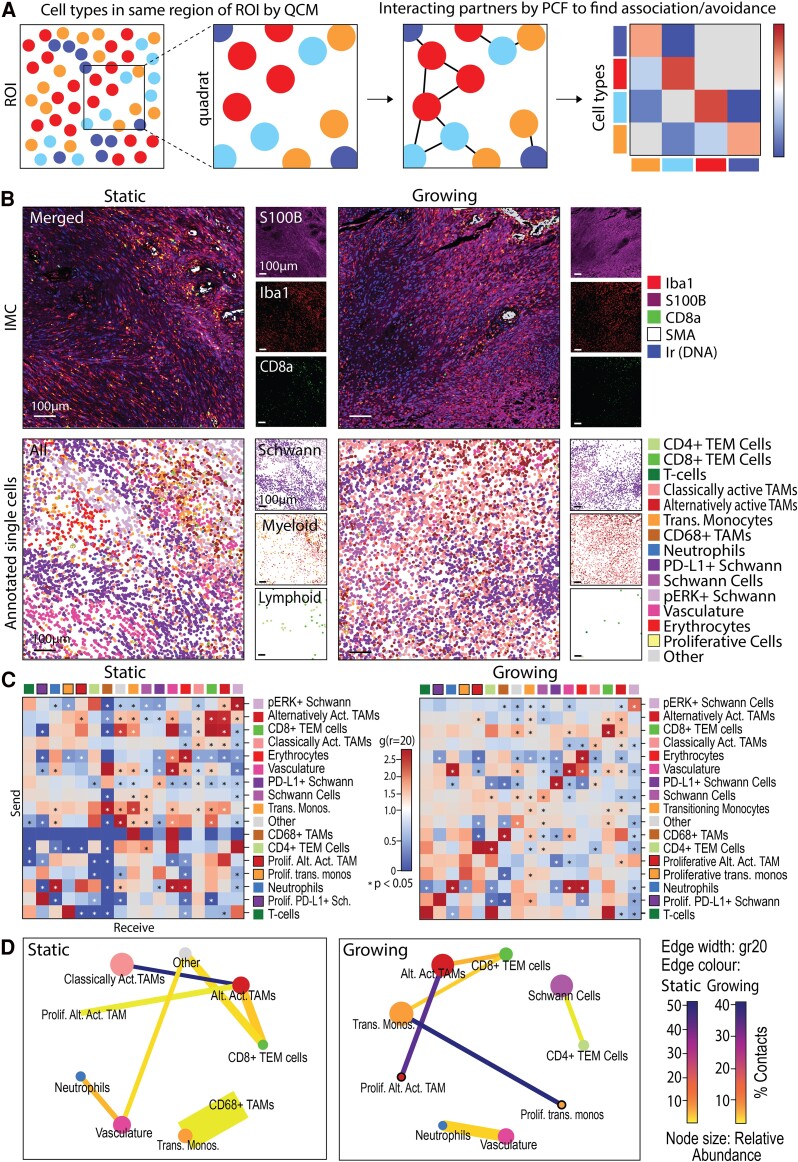 Figure 4. Classically activated TAMs associate with alternatively activated TAMs in static but not growing VS. (A) Schematic detailing how significant positive and negative cell–cell spatial… Source: Alternatively activated macrophages are associated with faster growth rate in vestibular schwannoma — Brain Communications 2024; CC BY.
Figure 4. Classically activated TAMs associate with alternatively activated TAMs in static but not growing VS. (A) Schematic detailing how significant positive and negative cell–cell spatial… Source: Alternatively activated macrophages are associated with faster growth rate in vestibular schwannoma — Brain Communications 2024; CC BY.
 Figure 4. Source: Sudden Sensorineural Hearing Loss and Facial Palsy in Patients with Vestibular Schwannoma Based on the Population Data of Korea — J Int Adv Otol. 2023 Nov 1;19(6):468–71. doi: 10.5152/iao.2023.231121; CC BY-NC.
Figure 4. Source: Sudden Sensorineural Hearing Loss and Facial Palsy in Patients with Vestibular Schwannoma Based on the Population Data of Korea — J Int Adv Otol. 2023 Nov 1;19(6):468–71. doi: 10.5152/iao.2023.231121; CC BY-NC.
 Figure 5. Source: Immunological Analysis of Vestibular Schwannoma Patients — J Int Adv Otol. 2023 Jan 1;19(1):1–4. doi: 10.5152/iao.2023.22581; CC BY-NC.
Figure 5. Source: Immunological Analysis of Vestibular Schwannoma Patients — J Int Adv Otol. 2023 Jan 1;19(1):1–4. doi: 10.5152/iao.2023.22581; CC BY-NC.
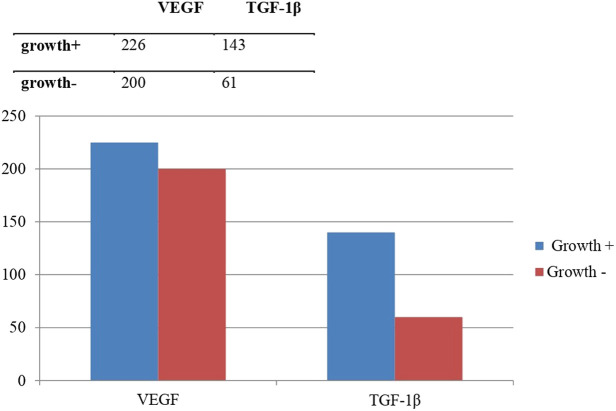 Figure 1.. Level of growth factors in the tumor growth group vs. the no tumor growth group. Source: Immunological Analysis of Vestibular Schwannoma Patients — The Journal of International Advanced Otology 2023; CC BY-NC.
Figure 1.. Level of growth factors in the tumor growth group vs. the no tumor growth group. Source: Immunological Analysis of Vestibular Schwannoma Patients — The Journal of International Advanced Otology 2023; CC BY-NC.
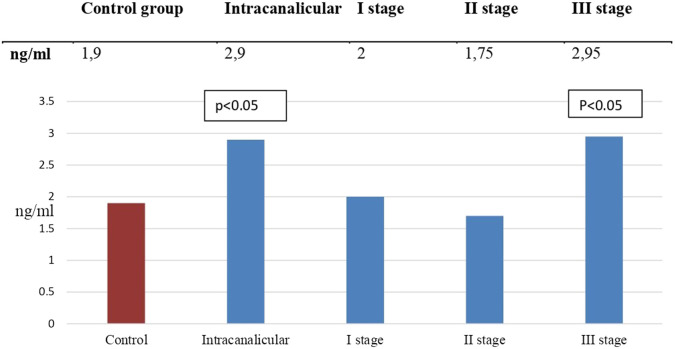 Figure 2.. Concentration of carcinoembryonic antigen in patients with different stages of vestibular schwannoma in comparison to the control group. Source: Immunological Analysis of Vestibular Schwannoma Patients — The Journal of International Advanced Otology 2023; CC BY-NC.
Figure 2.. Concentration of carcinoembryonic antigen in patients with different stages of vestibular schwannoma in comparison to the control group. Source: Immunological Analysis of Vestibular Schwannoma Patients — The Journal of International Advanced Otology 2023; CC BY-NC.
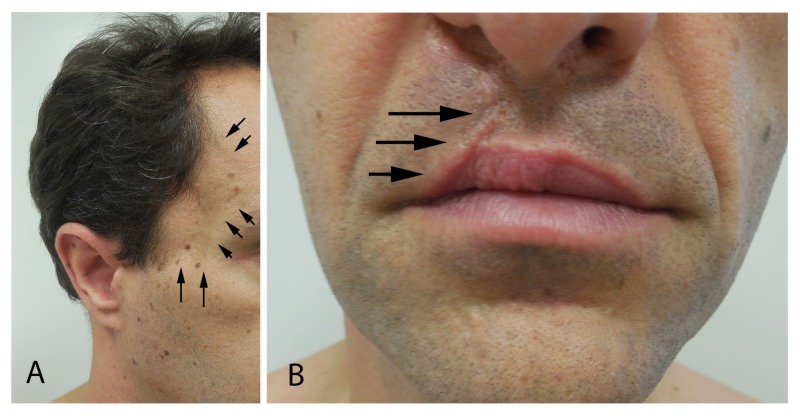 Figure 1. Juvenile nasopharyngeal angiofibroma and cleft lip and cleft palate.A 38-year-old man has atrophy of the right temporal area (arrows) resulting from the surgical treatment of his… Source: A Man with Juvenile Nasopharyngeal Angiofibroma, Vestibular Schwannoma, Cleft Lip and Cleft Palate, and Various Nevi: Case Report and Review — Cureus 2018; CC BY.
Figure 1. Juvenile nasopharyngeal angiofibroma and cleft lip and cleft palate.A 38-year-old man has atrophy of the right temporal area (arrows) resulting from the surgical treatment of his… Source: A Man with Juvenile Nasopharyngeal Angiofibroma, Vestibular Schwannoma, Cleft Lip and Cleft Palate, and Various Nevi: Case Report and Review — Cureus 2018; CC BY.
 Figure 2. Compound dysplastic nevus with mild atypia on the right mid-back.Distant (A) and closer (B) views of an oval dark brown patch (arrow) on the right mid-back. Microscopic examination of… Source: A Man with Juvenile Nasopharyngeal Angiofibroma, Vestibular Schwannoma, Cleft Lip and Cleft Palate, and Various Nevi: Case Report and Review — Cureus 2018; CC BY.
Figure 2. Compound dysplastic nevus with mild atypia on the right mid-back.Distant (A) and closer (B) views of an oval dark brown patch (arrow) on the right mid-back. Microscopic examination of… Source: A Man with Juvenile Nasopharyngeal Angiofibroma, Vestibular Schwannoma, Cleft Lip and Cleft Palate, and Various Nevi: Case Report and Review — Cureus 2018; CC BY.
 Figure 3. Combined (blue and intradermal) nevus of the right mid-chest.Distant (A) and closer (B) views of a small black macule (arrow) on the right mid-chest. Microscopic examination of the shave… Source: A Man with Juvenile Nasopharyngeal Angiofibroma, Vestibular Schwannoma, Cleft Lip and Cleft Palate, and Various Nevi: Case Report and Review — Cureus 2018; CC BY.
Figure 3. Combined (blue and intradermal) nevus of the right mid-chest.Distant (A) and closer (B) views of a small black macule (arrow) on the right mid-chest. Microscopic examination of the shave… Source: A Man with Juvenile Nasopharyngeal Angiofibroma, Vestibular Schwannoma, Cleft Lip and Cleft Palate, and Various Nevi: Case Report and Review — Cureus 2018; CC BY.
History of Present Illness
- Chief complaint: Unilateral sensorineural hearing loss / tinnitus / imbalance / facial numbness
- Duration and progression:
- Hearing: Unilateral progressive sensorineural hearing loss; sudden hearing loss in some
- Tinnitus: Unilateral
- Vestibular: Imbalance (rarely vertigo — slow-growing tumor allows compensation)
- Facial sensation: Numbness (CN V compression — large tumors)
- Facial weakness: Rare at presentation unless very large
- Headache: Suggests hydrocephalus (large tumors with brainstem compression)
- NF2: Bilateral vestibular schwannomas = NF2 (different management)
Past Medical History
- NF2 (neurofibromatosis type 2) — bilateral VS; hearing preservation paramount
- Prior hearing loss (baseline hearing status critical for approach selection)
- Prior radiation (gamma knife, proton beam)
- Prior surgery
- Allergies:
- Medications:
Imaging Review
MRI Brain/IAC (Thin-cut T1+Gad, T2, CISS/FIESTA)
- Size: __ x __ x ___ cm (largest CPA component)
- Koos classification:
- Grade I: Intracanalicular only
- Grade II: Extends into CPA, < 2 cm
- Grade III: Fills CPA but no brainstem contact, 2-3 cm
- Grade IV: Brainstem compression, > 3 cm
- IAC involvement: Fundus extension, canal widening
- Brainstem compression: Degree of displacement, 4th ventricle compression
- Hydrocephalus: Present/absent
- Cerebellopontine angle: Tumor filling, cistern obliteration
- Cranial nerves:
- CN VII (facial nerve): Often displaced anteroinferiorly by tumor
- CN V: Contact or compression (large tumors)
- CN VIII: Origin nerve (superior vs inferior vestibular)
- Cystic component: Cystic tumors can be more adherent to facial nerve
- Enhancement: Homogeneous (typical) vs heterogeneous
CT Temporal Bone
- IAC widening
- Posterior fossa bony anatomy
- Vestibular aqueduct
- Cochlear apparatus (hearing preservation planning)
Audiometry
- Pure tone audiogram: SRT, speech discrimination score (SDS)
- Serviceable hearing: AAO-HNS Class A or B (SDS >= 50%, PTA <= 50 dB)
- Non-serviceable hearing: Class C or D
- ABR (auditory brainstem response): Wave V latency
- Word recognition score (WRS): Critical for approach selection
Labs
- CBC, BMP, Coags
- Type and crossmatch
- Genetic testing for NF2 if bilateral or young
Neurological Examination
Cranial Nerves (Detailed)
- CN V: Facial sensation (V1, V2, V3), corneal reflex, masseter
- CN VII: House-Brackmann grade at baseline (I = normal, VI = total paralysis)
- CN VIII:
- Hearing: Weber (lateralizes to GOOD ear), Rinne (positive both sides if sensorineural)
- Vestibular: Romberg, head thrust test, nystagmus
- CN IX-XII: Lower cranial nerves (large tumors)
Cerebellar
- Gait, tandem walking, coordination
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: Mayfield, navigation, microscope/endoscope, cranial nerve monitoring/BAER when relevant, EVD/CSF diversion plan, watertight closure and fat/fascia graft materials, and blood available for vascular tumors.
- Special needs: arterial line, Foley, dexamethasone for edema, antiemetic plan, lower-CN airway/swallow contingency, EVD/ETV plan for hydrocephalus, and audiology/facial-nerve baseline when relevant.
- Immediate postop orders: ICU neuro checks, CN/eye movement/facial/swallow/voice exams, HOB 30, CT for hemorrhage/hydrocephalus, MRI for EOR, CSF-leak/pseudomeningocele watch, dex taper, and early swallow/ENT consult when lower CN risk exists.
Approach Selection — CRITICAL DECISION
| Approach | Hearing Preservation | Facial Nerve View | Best For |
|---|---|---|---|
| Retrosigmoid | Possible | Good (posterior view) | Medium tumors, hearing preservation attempt |
| Translabyrinthine | No (destroys labyrinth) | Excellent (early ID) | Large tumors, non-serviceable hearing |
| Middle Fossa | Best chance | Adequate | Small intracanalicular, serviceable hearing |
- Middle fossa: Koos I, serviceable hearing, tumor < 1.5 cm
- Retrosigmoid: Koos II-III, serviceable hearing, tumor with CPA component
- Translabyrinthine: Koos III-IV, non-serviceable hearing, large tumors (best facial nerve outcome for large tumors)
Position
Retrosigmoid:
- Lateral/park bench (ipsilateral side up) or supine with head turned
- Head flexed, vertex tilted down, mastoid highest point
- Mayfield skull clamp
Translabyrinthine:
- Supine, head turned contralateral, ipsilateral ear up
- Mayfield clamp
- Shoulder roll
Middle Fossa:
- Supine, head turned 90 degrees, ipsilateral ear up
- Mayfield clamp
Key Surgical Steps (Retrosigmoid Approach)
- Retrosigmoid craniotomy — expose sigmoid and transverse sinus junction
- Dural opening — based on sinuses
- CSF drainage — cerebellomedullary cistern for relaxation
- Cerebellar retraction — minimal, gravity-assisted
- Identify tumor in CPA — debulk the center (CUSA) to reduce tumor volume
- Identify CN VII — CRITICAL
- Typically displaced ANTEROINFERIORLY
- Use facial nerve EMG stimulator to locate nerve on tumor capsule
- CN VII course: brainstem → across CPA → tumor capsule (often splayed) → IAC → fundus
- Progressive tumor removal:
- Internal debulking first
- Then capsule dissection from medial to lateral
- Identify and preserve the arachnoid plane between tumor and brainstem/cerebellum
- Identify CN VII on tumor capsule — dissect tumor OFF the nerve, NOT nerve off tumor
- Drill posterior wall of IAC — to access intracanalicular component
- Identify transverse crest (Bill’s bar) — CN VII is ANTERIOR to Bill’s bar
- Leave a bone shell over the posterior semicircular canal (if hearing preservation)
- Remove intracanalicular tumor — work lateral to medial
- Final facial nerve confirmation — stimulate along entire course
- Hearing preservation: If attempting, monitor BAER continuously; preserve cochlear nerve
- Hemostasis: Pack IAC with fat graft + bone wax (prevent CSF leak)
- Dural closure: Watertight with graft if needed
Critical Anatomy & Structures at Risk
- Facial nerve (CN VII) — the priority structure; displaced by tumor but usually anatomically continuous. Stimulate frequently to map location
- Cochlear nerve (CN VIII cochlear division) — if hearing preservation attempted; runs with CN VII
- AICA — may be displaced or encased; gives off labyrinthine artery
- Labyrinthine artery — end artery to inner ear; injury → total hearing loss
- Trigeminal nerve (CN V) — compressed superiorly by large tumors
- Lower cranial nerves (IX, X, XI) — at risk with large tumors extending to jugular foramen
- Brainstem — medially; avoid any traction or thermal injury
- Petrosal vein — may need sacrifice for exposure; risk of venous infarction
- Cerebellum — avoid retraction injury
Equipment
- Operating microscope
- Facial nerve stimulator (monopolar and bipolar probes) — ESSENTIAL
- CUSA for tumor debulking
- High-speed drill (diamond burr for IAC drilling)
- Microsurgical instruments (micro scissors, dissectors, hooks)
- Bipolar (fine tip, low setting near facial nerve)
- Hemostatic agents
- Abdominal fat graft (for IAC packing and dead space)
- Bone wax
- Dural substitute
Monitoring
- Continuous facial EMG (CN VII) — CRITICAL; detects mechanical irritation
- Facial nerve stimulator — direct stimulation to locate nerve on tumor
- BAER — hearing preservation monitoring
- SSEPs
- Optional: CN V, CN IX/X/XI EMG (large tumors)
Anesthesia Considerations
- Arterial line
- Foley
- NO long-acting paralytic after intubation — facial EMG monitoring requires no paralysis
- Short-acting paralytic for intubation only, then allow to wear off
- Cefazolin 2g IV
- Dexamethasone 10 mg IV
- Mannitol 0.5-1 g/kg
- Antiemetics (ondansetron — posterior fossa high nausea risk)
Potential Complications & Contingencies
- Facial nerve palsy — most feared; intraoperative stimulation guides preservation; if nerve anatomically intact, may still have temporary palsy (neuropraxia) → House-Brackmann grading post-op; eye care essential
- Hearing loss — labyrinthine artery injury, cochlear nerve stretch; BAER monitoring; accept loss if necessary for facial nerve preservation
- CSF leak — watertight closure, fat graft in IAC; if post-op leak → lumbar drain or wound revision
- Meningitis — from CSF leak pathway; monitor for fever/meningismus
- Cerebellar hematoma/edema — minimize retraction
- Residual/recurrent tumor — planned subtotal resection if facial nerve at risk → radiosurgery for residual
- Lower cranial nerve palsy — swallowing difficulty, voice hoarseness; speech/swallow eval
Operative Note Template
[Include: approach, tumor size, facial nerve location on tumor, stimulation thresholds throughout case, facial nerve anatomic preservation, extent of resection, IAC drilling, BAER monitoring results, fat graft placement, closure]
Postoperative Plan
- ICU x 24-48 hours (posterior fossa)
- Neuro checks q1h — posterior fossa precautions
- Facial nerve assessment: House-Brackmann grade hourly initially
- If HB > III: Ophthalmology consult for eye care (corneal exposure)
- Eye lubrication (artificial tears q1h, ointment at night)
- Moisture chamber at night
- Gold weight consideration if persistent palsy
- CT head 6 hours post-op
- Audiogram before discharge (if hearing preservation attempted)
- HOB 30 degrees
- Dexamethasone taper
- Anti-emetics PRN
- DVT prophylaxis
- CSF leak monitoring: Watch incision and nose (rhinorrhea if via IAC/mastoid)
- MRI with gadolinium at 3-6 months (extent of resection)
- If subtotal resection: Plan for surveillance MRI and possible Gamma Knife for residual
- Follow-up: 2-4 weeks clinic; serial MRI; audiometry annually
- NF2 patients: Genetics, screening for other tumors (meningiomas, spinal tumors)
Chief-Level Case Review
Use these as the senior-level mental model for Vestibular Schwannoma (Acoustic Neuroma) Resection:
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Vestibular Schwannoma (Acoustic Neuroma) Resection:
- What is the surgical goal: gross-total, maximal safe, decompression, diagnosis, or cytoreduction?
- What eloquent cortex, tract, cranial nerve, vessel, or sinus defines the stopping point?
- What adjunct changes the case: navigation, mapping, 5-ALA, ultrasound, endoscope, ICG, or neuromonitoring?
- What is the edema, steroid, seizure, DVT, and postop imaging plan?
- What complication would you check for first in PACU based on this lesion location?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Extent-of-resection goal and functional stopping points: [attending-specific]
- Mapping/monitoring, 5-ALA, ultrasound, ICG, endoscope, or tractography preferences: [attending-specific]
- Steroid, antiepileptic, mannitol/hypertonic saline, and antibiotic plan: [attending-specific]
- Postop MRI timing, ICU/floor threshold, and adjuvant-referral workflow: [attending-specific]