
Case Prep: Jugular Foramen Tumor (Glomus Jugulare / Schwannoma / Meningioma)
Case / Approach Snapshot
- Anatomy at risk: tumor compartment, arterial supply, venous drainage/sinuses, cranial nerves, white-matter tracts, pituitary/CSF pathways when relevant, and functional cortex.
- Operative steps: review imaging and goals, choose exposure, obtain brain relaxation, devascularize when possible, debulk internally, dissect capsule from critical structures, verify extent/safety, and reconstruct watertight closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: venous or arterial injury, swelling, seizure, cranial nerve or endocrine change, CSF leak, residual tumor left for safety, staged surgery, radiation, or adjuvant therapy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [left/right] jugular foramen tumor ([glomus jugulare/paraganglioma / schwannoma / meningioma]) presenting with [pulsatile tinnitus / hearing loss / lower cranial neuropathy] planned for [far lateral / combined transtemporal-transjugular (infratemporal fossa) ] resection [± preoperative embolization].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Far-lateral (transcondylar) craniotomy — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Transtemporal Suprajugular Approach with Neck Dissection for Jugular Foramen Tumor Resection: Operative Video — Sarris CE. Journal of neurological surgery. Part B, Skull base 2021. PubMed
- Jugular foramen tumor causing isolated hypoglossal nerve palsy: a case report — Wen Z. Frontiers in oncology 2026. PubMed
- Giant jugular foramen tumor — Lai WS. Ear, nose, & throat journal 2013. PubMed
- Peripheral primitive neuroectodermal tumor of the jugular foramen: case report — Yamazaki T. Neurosurgery 2002. PubMed
- Endoluminal Sigmoid Sinus Occlusion During Jugular Foramen Tumor Surgery: Novel Technique, Operative Nuances, and Clinical Experience With 33 Patients — Castillo AL. Operative neurosurgery (Hagerstown, Md.) 2024. PubMed
- Surgical Management of Jugular Foramen Schwannomas — Aftahy AK. Cancers 2021. PubMed
- Cochlear Implantation for Sensorineural Hearing Loss Related to Cochlear Aqueduct Obstruction by a Jugular Foramen Tumor — Ewer N. Laryngoscope investigative otolaryngology 2025. PubMed
- Plasmacytoma presenting as jugular foramen tumor in a young woman with multiple myeloma — How J. American journal of hematology 2019. PubMed
- Anaplastic Hemangiopericytoma of the Jugular Foramen: Case Report and Systematic Review — Li D. World neurosurgery 2021. PubMed
- [An anatomical and technical note for neurosurgery of the jugular foramen tumor [author’s transl)] — Hakuba A. No shinkei geka. Neurological surgery 1982. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
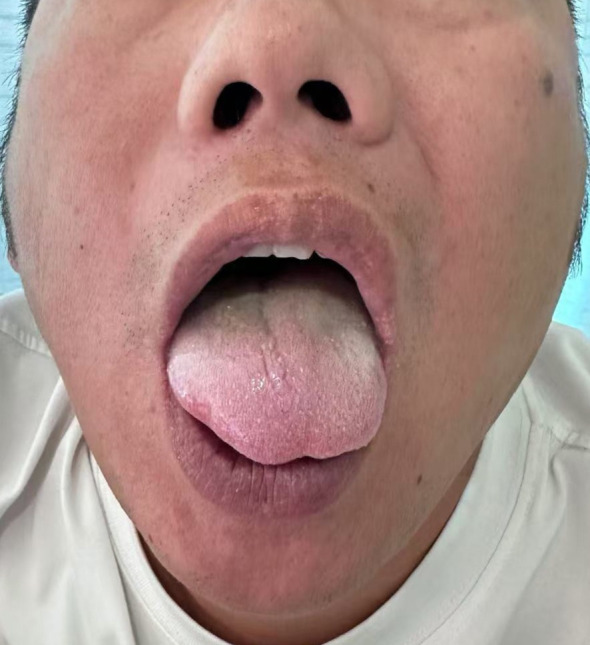 Figure 1. Clinical photograph of the tongue showing leftward deviation upon protrusion, presenting as asymmetry. Source: Jugular foramen tumor causing isolated hypoglossal nerve palsy: a case report — Frontiers in Oncology 2026; CC BY.
Figure 1. Clinical photograph of the tongue showing leftward deviation upon protrusion, presenting as asymmetry. Source: Jugular foramen tumor causing isolated hypoglossal nerve palsy: a case report — Frontiers in Oncology 2026; CC BY.
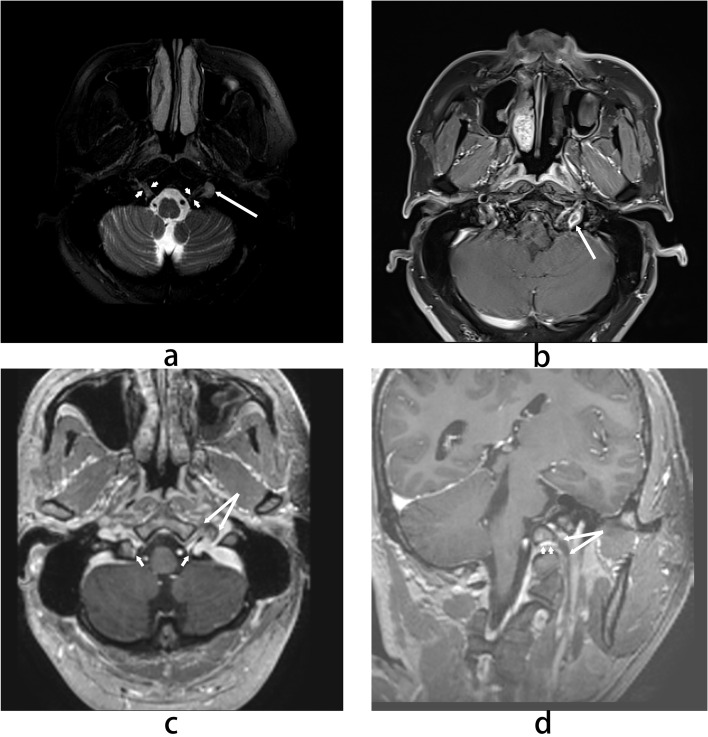 Figure 2. MRI findings. (a) Axial T2-weighted image shows a hyperintense nodule (long arrow) adjacent to the hypoglossal nerve (short arrow). (b) Axial contrast-enhanced T1-weighted image… Source: Jugular foramen tumor causing isolated hypoglossal nerve palsy: a case report — Frontiers in Oncology 2026; CC BY.
Figure 2. MRI findings. (a) Axial T2-weighted image shows a hyperintense nodule (long arrow) adjacent to the hypoglossal nerve (short arrow). (b) Axial contrast-enhanced T1-weighted image… Source: Jugular foramen tumor causing isolated hypoglossal nerve palsy: a case report — Frontiers in Oncology 2026; CC BY.
 Figure 3. Clinical timeline summarizing key events and interventions. Source: Jugular foramen tumor causing isolated hypoglossal nerve palsy: a case report — Frontiers in Oncology 2026; CC BY.
Figure 3. Clinical timeline summarizing key events and interventions. Source: Jugular foramen tumor causing isolated hypoglossal nerve palsy: a case report — Frontiers in Oncology 2026; CC BY.
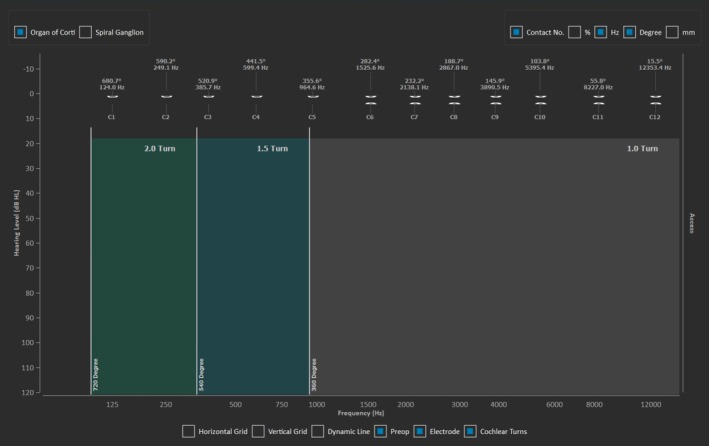 FIGURE 3. Electrode location by frequency place for anatomy based fitting. Source: Cochlear Implantation for Sensorineural Hearing Loss Related to Cochlear Aqueduct Obstruction by a Jugular Foramen Tumor — Laryngoscope Investigative Otolaryngology 2025; CC BY-NC-ND.
FIGURE 3. Electrode location by frequency place for anatomy based fitting. Source: Cochlear Implantation for Sensorineural Hearing Loss Related to Cochlear Aqueduct Obstruction by a Jugular Foramen Tumor — Laryngoscope Investigative Otolaryngology 2025; CC BY-NC-ND.
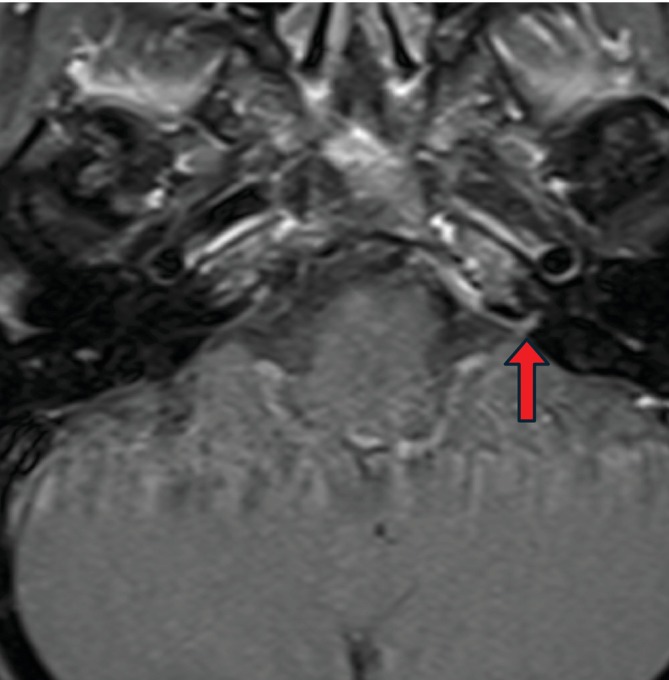 FIGURE 2. Axial contrast‐enhanced T1 MRI. Red arrow: Presence of enhancement of left cochlear aqueduct and adjacent dura consistent with tumor involvement. Source: Cochlear Implantation for Sensorineural Hearing Loss Related to Cochlear Aqueduct Obstruction by a Jugular Foramen Tumor — Laryngoscope Investigative Otolaryngology 2025; CC BY-NC-ND.
FIGURE 2. Axial contrast‐enhanced T1 MRI. Red arrow: Presence of enhancement of left cochlear aqueduct and adjacent dura consistent with tumor involvement. Source: Cochlear Implantation for Sensorineural Hearing Loss Related to Cochlear Aqueduct Obstruction by a Jugular Foramen Tumor — Laryngoscope Investigative Otolaryngology 2025; CC BY-NC-ND.
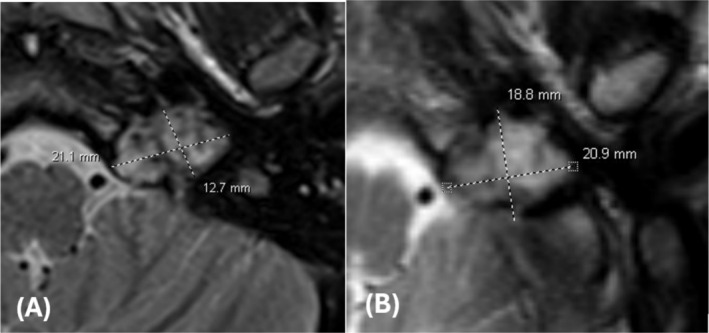 FIGURE 4. T2 axial MRI images of jugular foramen tumor (A) pre‐SRS (3.0 mm slice thickness) and (B) 3 months post‐SRS (5.0 mm slice thickness) revealing changes in tumor size. Source: Cochlear Implantation for Sensorineural Hearing Loss Related to Cochlear Aqueduct Obstruction by a Jugular Foramen Tumor — Laryngoscope Investigative Otolaryngology 2025; CC BY-NC-ND.
FIGURE 4. T2 axial MRI images of jugular foramen tumor (A) pre‐SRS (3.0 mm slice thickness) and (B) 3 months post‐SRS (5.0 mm slice thickness) revealing changes in tumor size. Source: Cochlear Implantation for Sensorineural Hearing Loss Related to Cochlear Aqueduct Obstruction by a Jugular Foramen Tumor — Laryngoscope Investigative Otolaryngology 2025; CC BY-NC-ND.
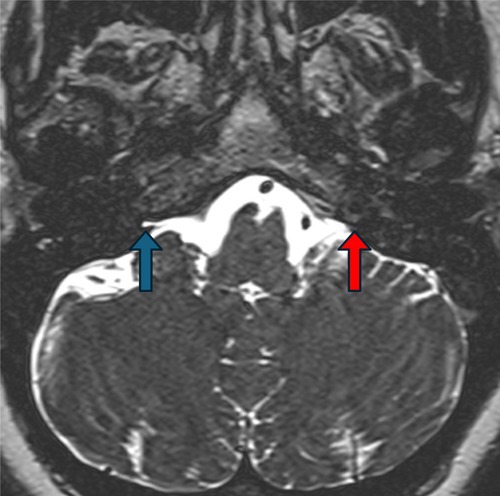 Figure 7. Source: Cochlear Implantation for Sensorineural Hearing Loss Related to Cochlear Aqueduct Obstruction by a Jugular Foramen Tumor — Laryngoscope Investig Otolaryngol. 2025 Aug 27;10(4):e70171. doi: 10.1002/lio2.70171; CC BY-NC-ND.
Figure 7. Source: Cochlear Implantation for Sensorineural Hearing Loss Related to Cochlear Aqueduct Obstruction by a Jugular Foramen Tumor — Laryngoscope Investig Otolaryngol. 2025 Aug 27;10(4):e70171. doi: 10.1002/lio2.70171; CC BY-NC-ND.
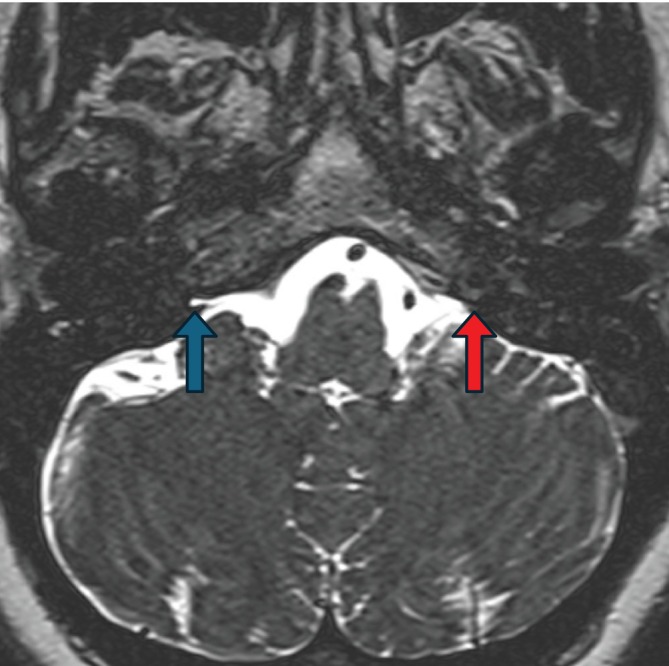 FIGURE 1. Axial heavily T2 weighted MRI. Blue arrow: Presence of fluid signal in cochlear aqueduct on non‐tumor size, indicating no occlusion. Red arrow: Absence of fluid signal in cochlear… Source: Cochlear Implantation for Sensorineural Hearing Loss Related to Cochlear Aqueduct Obstruction by a Jugular Foramen Tumor — Laryngoscope Investigative Otolaryngology 2025; CC BY-NC-ND.
FIGURE 1. Axial heavily T2 weighted MRI. Blue arrow: Presence of fluid signal in cochlear aqueduct on non‐tumor size, indicating no occlusion. Red arrow: Absence of fluid signal in cochlear… Source: Cochlear Implantation for Sensorineural Hearing Loss Related to Cochlear Aqueduct Obstruction by a Jugular Foramen Tumor — Laryngoscope Investigative Otolaryngology 2025; CC BY-NC-ND.
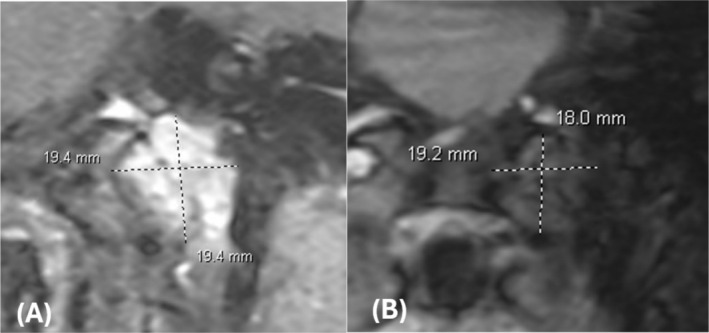 FIGURE 5. T1 post‐contrast FLASH coronal MRI images of jugular foramen tumor (A) pre‐SRS (3.0 mm slice thickness) and (B) 3 months post‐SRS (5.0 mm slice thickness) revealing changes in tumor size. Source: Cochlear Implantation for Sensorineural Hearing Loss Related to Cochlear Aqueduct Obstruction by a Jugular Foramen Tumor — Laryngoscope Investigative Otolaryngology 2025; CC BY-NC-ND.
FIGURE 5. T1 post‐contrast FLASH coronal MRI images of jugular foramen tumor (A) pre‐SRS (3.0 mm slice thickness) and (B) 3 months post‐SRS (5.0 mm slice thickness) revealing changes in tumor size. Source: Cochlear Implantation for Sensorineural Hearing Loss Related to Cochlear Aqueduct Obstruction by a Jugular Foramen Tumor — Laryngoscope Investigative Otolaryngology 2025; CC BY-NC-ND.
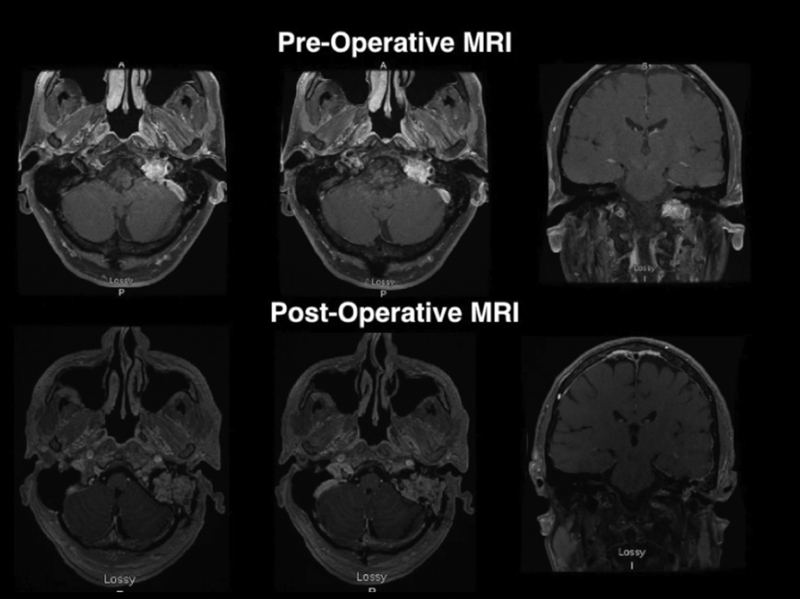 Fig. 1. Pre and postoperative images. Source: Gross Total Resection of a Jugular Foramen Thyroid Medullary Metastasis via a Transjugular Transsigmoid Approach — Journal of Neurological Surgery. Part B, Skull Base 2018; CC BY-NC-ND.
Fig. 1. Pre and postoperative images. Source: Gross Total Resection of a Jugular Foramen Thyroid Medullary Metastasis via a Transjugular Transsigmoid Approach — Journal of Neurological Surgery. Part B, Skull Base 2018; CC BY-NC-ND.
History of Present Illness
- Chief complaint: Pulsatile tinnitus, conductive hearing loss (glomus — vascular middle ear mass), lower cranial neuropathy (IX, X, XI — dysphagia, hoarseness, aspiration), CN XII, facial weakness, ataxia
- Glomus jugulare (paraganglioma): highly vascular, may be catecholamine-secreting (screen!), part of paraganglioma syndromes (SDH mutations — screen/genetics, multicentricity)
- Jugular foramen schwannoma (CN IX-XI), meningioma
- Symptom duration, prior treatment
Past Medical History
- Catecholamine screening (glomus) — plasma/urine metanephrines (rule out secretory tumor — anesthetic crisis risk), SDHx genetic testing/family history (paraganglioma syndromes, pheochromocytoma)
- Cardiac (if secretory), prior treatment/radiation
- Standard PMH
Imaging Review
MRI (T1±Gad, T2) + MRA/MRV
- Tumor extent (jugular foramen, into middle ear/neck/posterior fossa), “salt-and-pepper” flow voids (glomus), brainstem/cerebellar relationship
- Sigmoid/jugular venous system (dominant side? occlusion?), dural venous sinuses
CT temporal bone
- Bony erosion (glomus — “moth-eaten” jugular foramen; vs smooth enlargement in schwannoma), jugular bulb, carotid canal, ossicles, mastoid
Angiography + Embolization
- Preoperative embolization (glomus — highly vascular; reduces blood loss), feeders (ascending pharyngeal, etc.), ICA involvement, venous anatomy, balloon test occlusion if ICA sacrifice possible
Audiology
- Baseline audiogram
Labs
- CBC, BMP, Coags, type and crossmatch, metanephrines (glomus)
Neurological Examination
- Lower cranial nerves (IX-XII), VII, VIII, cerebellar, gait; baseline swallow/voice (critical for counseling/aspiration risk)
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: Mayfield, navigation, microscope/endoscope, cranial nerve monitoring/BAER when relevant, EVD/CSF diversion plan, watertight closure and fat/fascia graft materials, and blood available for vascular tumors.
- Special needs: arterial line, Foley, dexamethasone for edema, antiemetic plan, lower-CN airway/swallow contingency, EVD/ETV plan for hydrocephalus, and audiology/facial-nerve baseline when relevant.
- Immediate postop orders: ICU neuro checks, CN/eye movement/facial/swallow/voice exams, HOB 30, CT for hemorrhage/hydrocephalus, MRI for EOR, CSF-leak/pseudomeningocele watch, dex taper, and early swallow/ENT consult when lower CN risk exists.
Diagnosis & Indication / Strategy
- Indication: Symptomatic/growing tumor; management individualized — surgery (cure but CN morbidity), radiosurgery (growth control with lower CN morbidity — increasingly favored for glomus, esp. with intact CN function), or combined; observation for small/asymptomatic elderly
- Glomus: preoperative embolization + alpha-blockade if secretory
- Multidisciplinary (neurotology/skull base + neurosurgery ± head and neck/vascular)
Position
- Lateral/park bench or supine head-turned; Mayfield; neck prepped (proximal vascular control); IONM (lower CNs, VII, VIII)
Key Surgical Steps (Combined transtemporal-transjugular / infratemporal fossa)
- Postauricular incision, expose the neck for proximal ICA/IJV and lower CN control
- Mastoidectomy, skeletonize the sigmoid sinus, jugular bulb, facial nerve (± anterior transposition of CN VII for infratemporal fossa type A), fallopian canal
- Control the sigmoid sinus and internal jugular vein (ligate/pack the sigmoid-jugular system — only if contralateral venous drainage adequate)
- Expose and resect tumor from the jugular foramen; preserve lower cranial nerves (IX, X, XI) where possible — dissect off the pars nervosa
- Manage ICA (petrous/cervical — skeletonize/protect; embolization/BTO planning if involved)
- Far lateral/posterior fossa extension for intradural/brainstem component
- Resect dural attachment (meningioma); accept residual on CNs/ICA if adherent
- Watertight closure + fat/flap obliteration of the defect/eustachian tube (CSF leak prevention)
Critical Anatomy & Structures at Risk
- Lower cranial nerves (IX, X, XI, XII) — dysphagia/aspiration, hoarseness, shoulder; often the dominant morbidity
- Internal carotid artery (petrous/cervical), jugular bulb / sigmoid sinus / IJV (venous drainage — ensure contralateral patency before sacrifice)
- Facial nerve (VII) (transposition risk), CN VIII (hearing)
- Brainstem/cerebellum, dura (CSF leak)
Equipment
- Microscope, drill (mastoid/skull base), navigation, CUSA, ICG, micro-Doppler
- CN monitoring (VII, VIII, IX-XII), fat graft/flap, dural substitute, sealant
- Preop embolization, vascular control/repair capability; neurotology collaboration
Monitoring
- Lower CN EMG (IX-XII), VII EMG, BAER, SSEP/MEP
Anesthesia
- Arterial line, crossmatched blood (vascular), alpha-blockade/avoid catecholamine surge if secretory glomus (pheo-like precautions), VAE precautions, airway/aspiration planning, long case
Potential Complications
- Lower cranial nerve palsies (dysphagia/aspiration — may need tracheostomy/PEG/vocal cord medialization), CN VII/VIII deficits
- Major hemorrhage (glomus — embolization helps), ICA injury, venous infarction (if dominant sinus sacrificed)
- CSF leak, hypertensive crisis (secretory), stroke
- Subtotal/recurrence (consider adjuvant radiosurgery)
Operative Note Template
Preoperative Diagnosis: [Left/Right] jugular foramen tumor ([glomus jugulare / schwannoma / meningioma]) with [pulsatile tinnitus / lower cranial neuropathy]
Postoperative Diagnosis: Same
Procedure: [Left/Right] [combined transtemporal-transjugular (infratemporal fossa) / far lateral] resection of jugular foramen tumor [following preoperative embolization]
Surgeon / Assistant: Neurosurgery + neurotology/skull base co-surgeon Anesthesia: General endotracheal [alpha-blockade if secretory glomus] EBL / Fluids / Blood products: [crossmatched] Adjuncts: Neuronavigation, high-speed drill, ICG, micro-Doppler; CN EMG (VII, IX-XII)/BAER/SSEP/MEP Implants: Fat graft/flap, dural substitute, sealant Complications: None
Indications: [Age]yo [M/F] with a jugular foramen [glomus jugulare] causing [pulsatile tinnitus/lower cranial neuropathy]; metanephrines were [negative]. Preoperative embolization was performed for this vascular tumor. Risks (lower CN palsies/aspiration, ICA injury, venous infarction, CSF leak) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced [with alpha-blockade precautions for the secretory tumor], and neuromonitoring established. With the neurotology co-surgeon, a postauricular incision was made and the neck dissected for proximal ICA/IJV and lower cranial nerve control. A mastoidectomy was performed, skeletonizing the sigmoid sinus, jugular bulb, and facial nerve [with anterior transposition of CN VII].
The sigmoid sinus and internal jugular vein were controlled and the venous system addressed (confirming adequate contralateral drainage before sacrifice). The tumor was resected from the jugular foramen, preserving the lower cranial nerves (IX-XII) off the pars nervosa where possible and protecting/skeletonizing the ICA; [the far-lateral extension addressed the intradural/brainstem component]. Residual adherent to the CNs/ICA was left. The defect was obliterated with fat/flap and a watertight closure performed with sealant to prevent CSF leak.
The patient was transferred to the ICU with lower-CN precautions and swallow assessment planned before PO intake.
Postoperative Plan
- ICU, neuro checks, lower CN assessment — swallow eval before PO, voice, aspiration precautions (often need speech/swallow therapy; consider early ENT for vocal cord)
- CT/MRI postop, audiogram, CSF leak watch
- Secretory glomus: hemodynamic monitoring, continue alpha-blockade taper
- Genetics referral (SDHx), screen for multicentric paraganglioma/pheochromocytoma
- Residual → radiosurgery/surveillance; rehab (swallow, shoulder); long-term follow-up
Chief-Level Case Review
Use these as the senior-level mental model for Jugular Foramen Tumor (Glomus Jugulare / Schwannoma / Meningioma):
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Jugular Foramen Tumor (Glomus Jugulare / Schwannoma / Meningioma):
- What is the surgical goal: gross-total, maximal safe, decompression, diagnosis, or cytoreduction?
- What eloquent cortex, tract, cranial nerve, vessel, or sinus defines the stopping point?
- What adjunct changes the case: navigation, mapping, 5-ALA, ultrasound, endoscope, ICG, or neuromonitoring?
- What is the edema, steroid, seizure, DVT, and postop imaging plan?
- What complication would you check for first in PACU based on this lesion location?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Extent-of-resection goal and functional stopping points: [attending-specific]
- Mapping/monitoring, 5-ALA, ultrasound, ICG, endoscope, or tractography preferences: [attending-specific]
- Steroid, antiepileptic, mannitol/hypertonic saline, and antibiotic plan: [attending-specific]
- Postop MRI timing, ICU/floor threshold, and adjuvant-referral workflow: [attending-specific]