
Case Prep: Microvascular Decompression (MVD) for Trigeminal Neuralgia
Case / Approach Snapshot
- Anatomy at risk: target nuclei or cortical regions, trajectories, vessels, ventricles, cranial nerves, white-matter tracts, and stimulation/lesion side-effect pathways.
- Operative steps: confirm diagnosis and target, plan trajectory or exposure, use mapping/monitoring/stereotaxy as appropriate, place/lesion/resect with physiologic confirmation, close hardware or wound, and plan programming/follow-up; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: hemorrhage, seizure, neurologic or mood/cognitive change, lead/device migration or infection, stimulation side effects, hardware failure, and revision or programming strategy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [left/right] trigeminal neuralgia ([V2/V3/V2-V3]) refractory to medical management planned for [left/right] retrosigmoid craniotomy for microvascular decompression.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Retrosigmoid craniotomy — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Trigeminal Neuralgia — Cruccu G. The New England journal of medicine 2020. PubMed
- [Microvascular Decompression for Trigeminal Neuralgia Due to Venous Compression] — Toda H. No shinkei geka. Neurological surgery 2024. PubMed
- [Microvascular decompression in trigeminal neuralgia following vertebrobasilar dolichoectasia] — Shulev YA. Zhurnal voprosy neirokhirurgii imeni N. N. Burdenko 2020. PubMed
- Microvascular decompression for trigeminal neuralgia due to vertebrobasilar artery compression: a systematic review and meta-analysis — Di Carlo DT. Neurosurgical review 2022. PubMed
- Surgical technique management of microvascular decompression for trigeminal neuralgia — Yang L. Ideggyogyaszati szemle 2022. PubMed
- Trigeminal Neuralgia — Cruccu G. Continuum (Minneapolis, Minn.) 2017. PubMed
- Trigeminal Neuralgia — Zakrzewska JM. American family physician 2016. PubMed
- Endoscopic microvascular decompression versus microscopic microvascular decompression for trigeminal neuralgia: A systematic review and meta-analysis — Chen L. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia 2023. PubMed
- Microvascular decompression for trigeminal neuralgia — Sade B. Neurosurgery clinics of North America 2014. PubMed
- Microvascular decompression for pediatric onset trigeminal neuralgia: patterns and variation — Dou NN. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2022. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
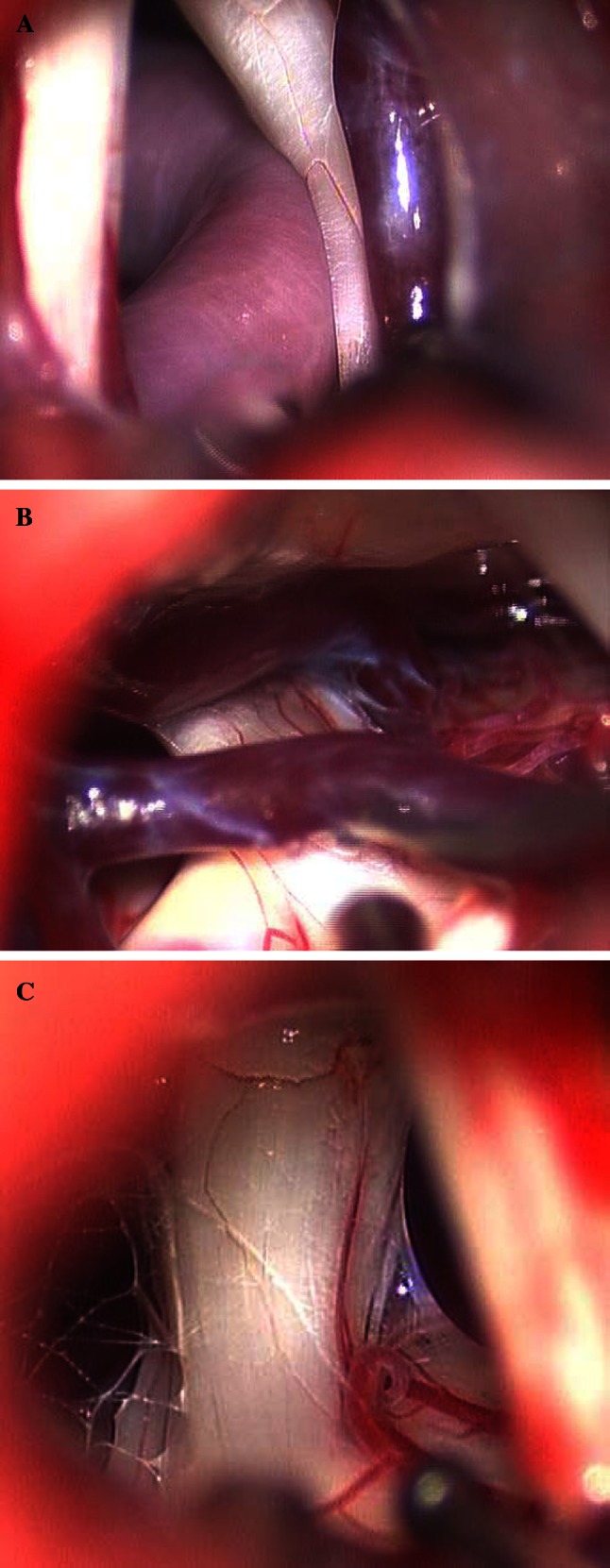 Fig. 1. Representative intraoperative images of a artery compression and vein close, b vein compression, and c arachnoid adhesions Source: Arterial compression of nerve is the primary cause of trigeminal neuralgia — Neurological Sciences 2013; CC BY.
Fig. 1. Representative intraoperative images of a artery compression and vein close, b vein compression, and c arachnoid adhesions Source: Arterial compression of nerve is the primary cause of trigeminal neuralgia — Neurological Sciences 2013; CC BY.
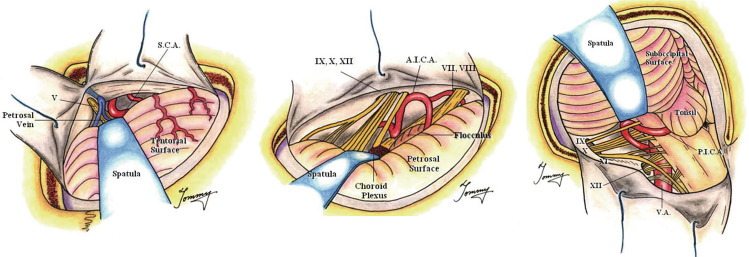 Fig. 3. “Rule of Three” framework for tailored MVD approaches to major neurovascular compression syndromes. Source: Historical evolution of microvascular decompression after Jannetta’s establishment: Anatomical maps and physiological compasses-a narrative review — Acta Neurochirurgica 2026; CC BY-NC-ND.
Fig. 3. “Rule of Three” framework for tailored MVD approaches to major neurovascular compression syndromes. Source: Historical evolution of microvascular decompression after Jannetta’s establishment: Anatomical maps and physiological compasses-a narrative review — Acta Neurochirurgica 2026; CC BY-NC-ND.
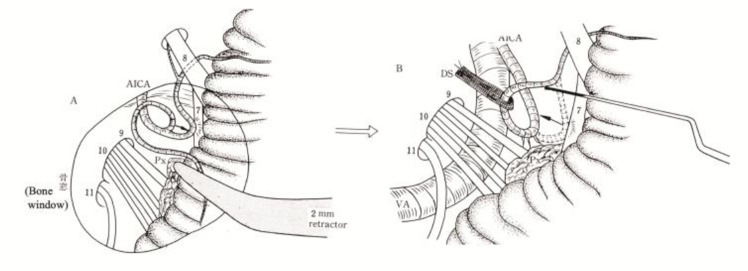 Fig. 5. Noncompressive transposition technique after MVD, illustrating transposition rather than simple interposition. Source: Historical evolution of microvascular decompression after Jannetta’s establishment: Anatomical maps and physiological compasses-a narrative review — Acta Neurochirurgica 2026; CC BY-NC-ND.
Fig. 5. Noncompressive transposition technique after MVD, illustrating transposition rather than simple interposition. Source: Historical evolution of microvascular decompression after Jannetta’s establishment: Anatomical maps and physiological compasses-a narrative review — Acta Neurochirurgica 2026; CC BY-NC-ND.
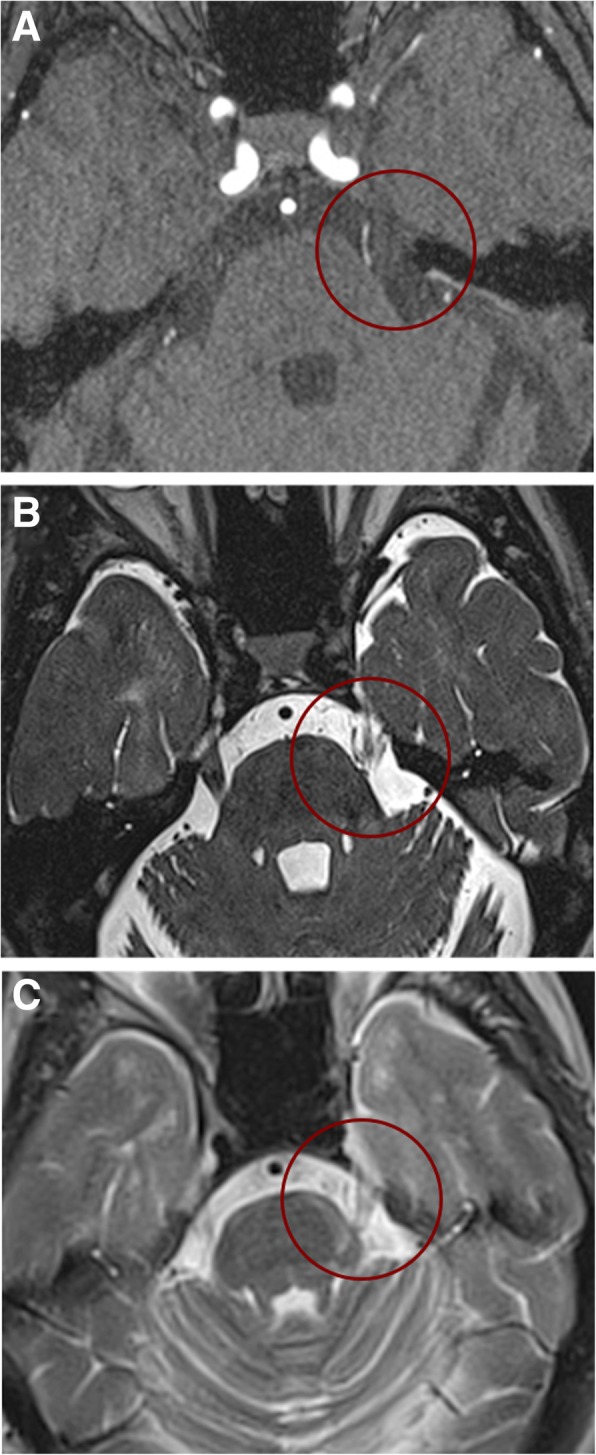 Fig. 1. Neuroimaging findings in a representative patient with TN secondary to MS possibly due to a double crush mechanism. 3D time-of-flight (TOF) magnetic resonance angiography scans (a) and… Source: Trigeminal neuralgia secondary to multiple sclerosis: from the clinical picture to the treatment options — The Journal of Headache and Pain 2019; CC BY.
Fig. 1. Neuroimaging findings in a representative patient with TN secondary to MS possibly due to a double crush mechanism. 3D time-of-flight (TOF) magnetic resonance angiography scans (a) and… Source: Trigeminal neuralgia secondary to multiple sclerosis: from the clinical picture to the treatment options — The Journal of Headache and Pain 2019; CC BY.
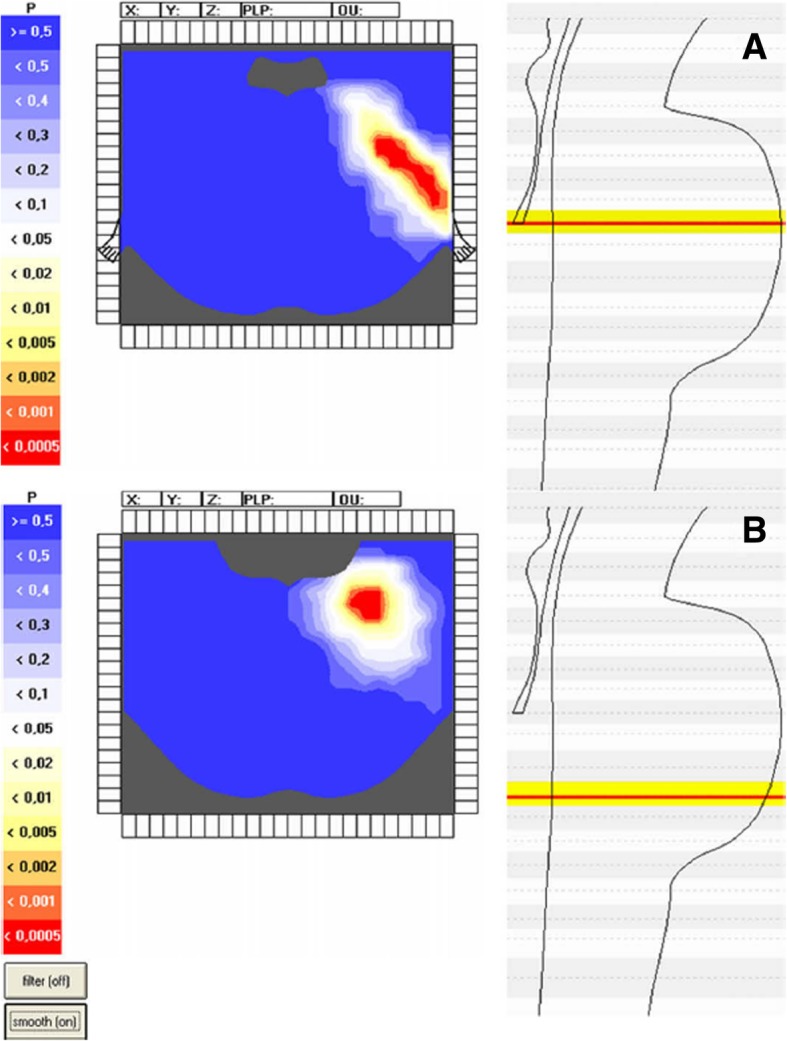 Fig. 2. Voxel-based analysis in patients with TN secondary to MS. Voxel-based brainstem model in patients with TN secondary to MS (TN group, n = 42) and in patients with trigeminal sensory… Source: Trigeminal neuralgia secondary to multiple sclerosis: from the clinical picture to the treatment options — The Journal of Headache and Pain 2019; CC BY.
Fig. 2. Voxel-based analysis in patients with TN secondary to MS. Voxel-based brainstem model in patients with TN secondary to MS (TN group, n = 42) and in patients with trigeminal sensory… Source: Trigeminal neuralgia secondary to multiple sclerosis: from the clinical picture to the treatment options — The Journal of Headache and Pain 2019; CC BY.
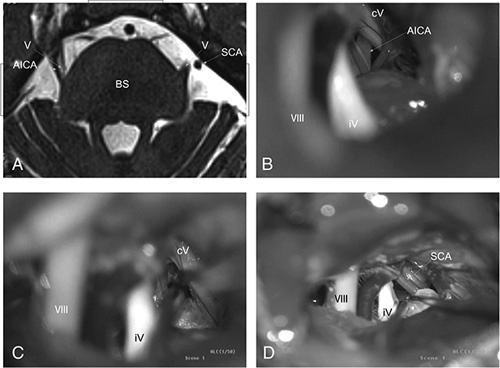 Figure 1. Patient 1: (A) Three-dimensional time-of-flight magnetic resonance angiography findings. Anterior inferior cerebellar artery compresses the right trigeminal nerve, left side was… Source: Unilateral Approach to Primary Bilateral Trigeminal Neuralgia Via Bilateral Microvascular Decompression — The Journal of Craniofacial Surgery 2022; CC BY-NC-ND.
Figure 1. Patient 1: (A) Three-dimensional time-of-flight magnetic resonance angiography findings. Anterior inferior cerebellar artery compresses the right trigeminal nerve, left side was… Source: Unilateral Approach to Primary Bilateral Trigeminal Neuralgia Via Bilateral Microvascular Decompression — The Journal of Craniofacial Surgery 2022; CC BY-NC-ND.
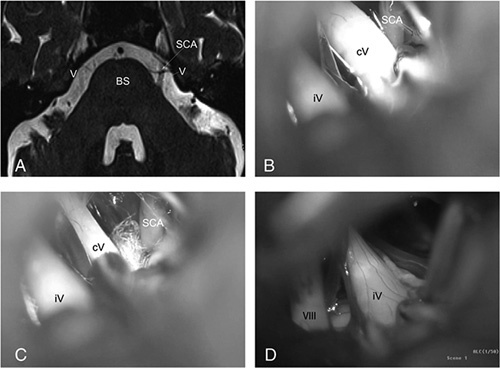 Figure 2. Patient 2: (A) Three-dimensional time-of-flight magnetic resonance angiography findings. Superior cerebellar artery compressed the left trigeminal nerve. (b) Contralateral trigeminal… Source: Unilateral Approach to Primary Bilateral Trigeminal Neuralgia Via Bilateral Microvascular Decompression — The Journal of Craniofacial Surgery 2022; CC BY-NC-ND.
Figure 2. Patient 2: (A) Three-dimensional time-of-flight magnetic resonance angiography findings. Superior cerebellar artery compressed the left trigeminal nerve. (b) Contralateral trigeminal… Source: Unilateral Approach to Primary Bilateral Trigeminal Neuralgia Via Bilateral Microvascular Decompression — The Journal of Craniofacial Surgery 2022; CC BY-NC-ND.
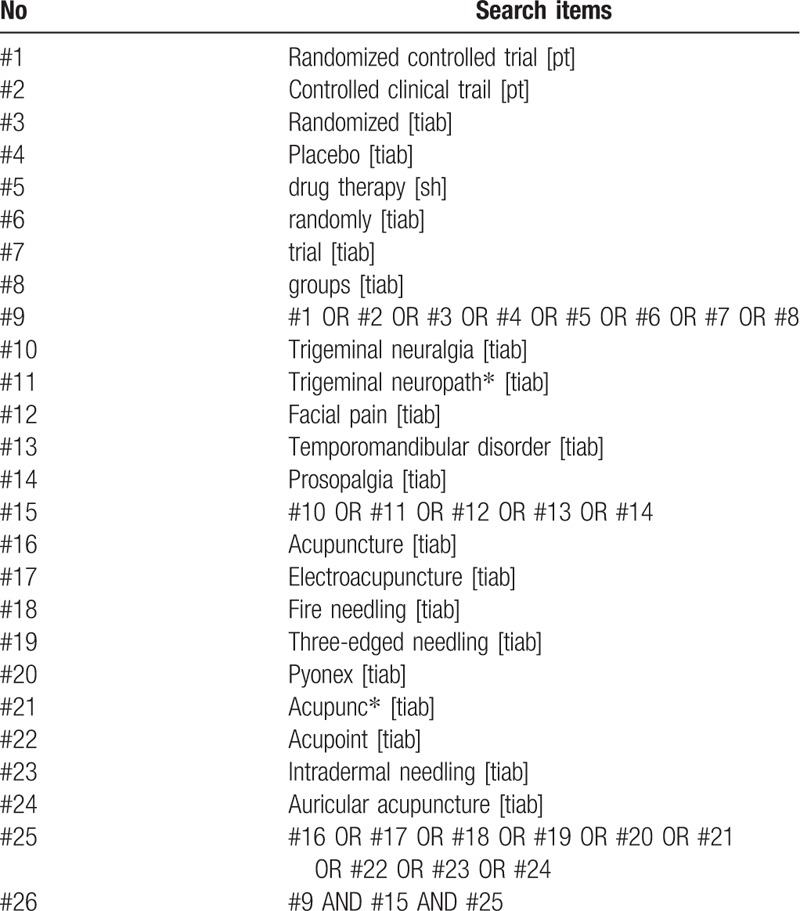 Figure 6. Source: Acupuncture treatment on idiopathic trigeminal neuralgia: A systematic review protocol — Medicine (Baltimore). 2019 Jan 25;98(4):e14239. doi: 10.1097/MD.0000000000014239; CC BY.
Figure 6. Source: Acupuncture treatment on idiopathic trigeminal neuralgia: A systematic review protocol — Medicine (Baltimore). 2019 Jan 25;98(4):e14239. doi: 10.1097/MD.0000000000014239; CC BY.
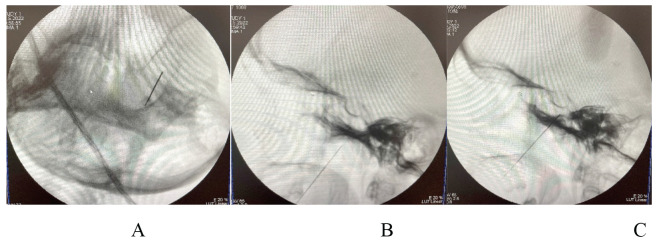 Figure 1. A Passage of the needle through the lateral part of the foramen ovale, B advancement of the needle towards the Gasseri ganglia, C position of the needle for radiofrequency ablation of… Source: TREATMENT OPTIONS FOR TRIGEMINAL NEURALGIA — Acta Clinica Croatica 2022; CC BY-NC-ND.
Figure 1. A Passage of the needle through the lateral part of the foramen ovale, B advancement of the needle towards the Gasseri ganglia, C position of the needle for radiofrequency ablation of… Source: TREATMENT OPTIONS FOR TRIGEMINAL NEURALGIA — Acta Clinica Croatica 2022; CC BY-NC-ND.
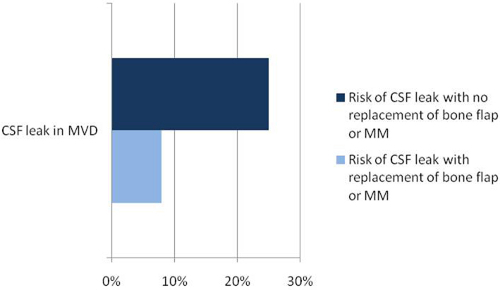 Figure 9. Source: Microvascular Decompression: Salient Surgical Principles and Technical Nuances — J Vis Exp. 2011 Jul 5;(53):2590. doi: 10.3791/2590; CC BY-NC-ND.
Figure 9. Source: Microvascular Decompression: Salient Surgical Principles and Technical Nuances — J Vis Exp. 2011 Jul 5;(53):2590. doi: 10.3791/2590; CC BY-NC-ND.
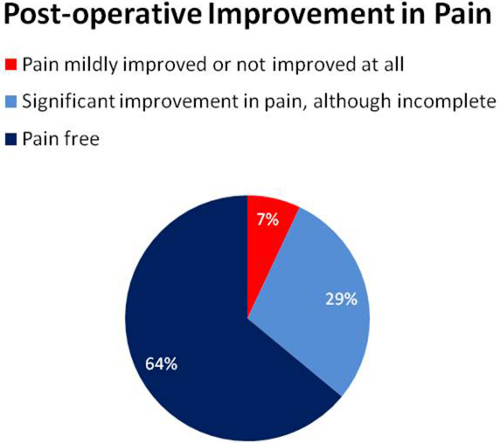 Figure 10. Source: Microvascular Decompression: Salient Surgical Principles and Technical Nuances — J Vis Exp. 2011 Jul 5;(53):2590. doi: 10.3791/2590; CC BY-NC-ND.
Figure 10. Source: Microvascular Decompression: Salient Surgical Principles and Technical Nuances — J Vis Exp. 2011 Jul 5;(53):2590. doi: 10.3791/2590; CC BY-NC-ND.
History of Present Illness
- Chief complaint: Lancinating/electric shock-like facial pain
- Duration:
- Distribution: V1 / V2 / V3 / combination
- V1 (ophthalmic): Forehead, upper eyelid
- V2 (maxillary): Cheek, upper lip, upper teeth, nasal ala
- V3 (mandibular): Lower jaw, lower lip, lower teeth, tongue
- Triggers: Chewing, talking, brushing teeth, wind on face, light touch
- Character: Lancinating/shooting/electric (classic Type 1) vs constant aching (Type 2/atypical)
- Frequency of attacks:
- Pain-free intervals between attacks:
- BNI pain scale:
- Medical management tried:
- Carbamazepine (first-line): Dose __, response __
- Oxcarbazepine: Dose __, response __
- Baclofen, gabapentin, lamotrigine:
- Side effects / intolerance:
- Prior procedures: Percutaneous rhizotomy, gamma knife, prior MVD
- Red flags for secondary TN: Age < 40, bilateral symptoms, sensory loss, constant pain → consider MS, tumor
Past Medical History
- Multiple sclerosis (secondary TN — MVD less effective)
- Prior TN procedures (percutaneous, gamma knife, prior MVD)
- Hearing loss (ipsilateral — affects approach risk)
- Other cranial nerve pathology
- Allergies:
- Medications:
Imaging Review
MRI Brain with Thin-Cut Posterior Fossa Sequences
- CISS/FIESTA sequence (high-resolution T2):
- Identify vascular loop at trigeminal root entry zone (REZ)
- Offending vessel:
- Superior cerebellar artery (SCA) — most common (~75%)
- Anterior inferior cerebellar artery (AICA) — second most common
- Vertebral artery / basilar artery — large vessel contact
- Vein (petrosal vein, bridging vein) — less favorable for MVD
- Combination
- Side of compression (dorsal, ventral, cranial, caudal)
- Nerve displacement / distortion / atrophy
- MRI brain: Rule out tumor (CPA epidermoid, meningioma, schwannoma causing secondary TN)
- Demyelinating plaques (if MS suspected)
MRA / CTA
- Course of offending vessel
- Relationship to brainstem and CN V
- Arterial anatomy of posterior circulation
Audiology
- Baseline audiogram — BAER monitoring requires serviceable hearing
- Document any pre-existing hearing loss
Labs
- CBC, BMP, Coags
- Type and screen
- Carbamazepine level (if still on it — important for perioperative management)
Neurological Examination
Trigeminal Nerve (CN V)
- Sensation: V1, V2, V3 (light touch, pinprick) — should be NORMAL in classic TN (deficit suggests secondary cause)
- Motor: Masseter, temporalis, pterygoids — should be normal
- Corneal reflex: Present/absent (V1)
- Trigger zones: Map carefully
Other Cranial Nerves (Posterior Fossa)
- CN VII: Facial symmetry/strength
- CN VIII: Hearing — Weber, Rinne, audiogram results
- CN IX, X: Palate, gag, voice
- CN XI: SCM, trapezius
- CN XII: Tongue
Cerebellar
- Finger-to-nose, heel-to-shin, gait — baseline for posterior fossa surgery
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: Mayfield, microscope, cranial nerve monitoring/BAER for MVD, Teflon/felt and microinstruments, dural graft/sealant for Chiari, and watertight closure materials.
- Special needs: arterial line optional by comorbidity/position, antiemetic plan, steroid plan by edema/aseptic meningitis risk, airway/OSA precautions, and CSF-leak/pseudomeningocele strategy.
- Immediate postop orders: posterior fossa neuro checks, facial/hearing/swallow exam as relevant, nausea/pain control, HOB 30, CT/MRI if concern or protocol, wound/CSF leak watch, and activity restrictions.
Diagnosis & Indication
- Working diagnosis: Classic trigeminal neuralgia (Type 1), medically refractory
- Surgical indication: Failed adequate trial of at least two medications (carbamazepine + one other), intolerable side effects, or patient preference for definitive treatment
- Goals: Identify and decompress the offending vessel from the trigeminal nerve REZ
- MVD advantages: Highest long-term cure rate (~80% at 10 years), non-destructive (preserves CN V function)
- Alternatives discussed:
- Percutaneous procedures (balloon compression, glycerol rhizotomy, radiofrequency thermocoagulation)
- Gamma Knife radiosurgery
- Continued medical management
Position
- Patient position: Lateral decubitus (park bench) with ipsilateral side UP — OR supine with head turned contralateral
- Park bench preferred:
- Ipsilateral side up (affected side up)
- Axillary roll under dependent arm
- Lower leg flexed, upper leg straight, pillow between legs
- Head flexed (chin toward chest) — opens angle between cerebellum and petrous bone
- Head slightly rotated (face toward floor) — mastoid is highest point
- Vertex tilted slightly toward floor
- Skull clamp: Mayfield 3-pin
- Retrosigmoid exposure: Mastoid highest point of the field
- Table: Neutral or slight reverse Trendelenburg
Incision
- Type: Curvilinear or linear incision behind the ear
- Landmarks:
- 2 fingerbreadths behind the ear
- Centered at the level of the transverse-sigmoid sinus junction (estimated: asterion)
- ~5-6 cm length
Approach: Retrosigmoid Craniotomy
Key Surgical Steps
- Incision — retromastoid curvilinear, centered on asterion
- Suboccipital craniectomy/craniotomy — ~2.5 x 2.5 cm
- Expose the junction of the transverse and sigmoid sinuses
- Keyhole burr hole just inferior and medial to the asterion
- Bone removal to expose the edge of the sigmoid sinus laterally and transverse sinus superiorly
- Dural opening — curvilinear, based on sigmoid/transverse sinus junction
- CSF drainage — open cisterna magna or lateral cerebellomedullary cistern early for cerebellar relaxation
- Cerebellar retraction — MINIMAL, gravity-assisted; brain relaxes after CSF drainage
- Identify CN V — follows the trigeminal nerve from the pons to Meckel’s cave
- Identify the offending vessel:
- SCA: Most commonly compresses from superiorly or superomedially at the REZ
- AICA: Compresses from inferiorly or laterally
- Vertebral/basilar: Large vessel indentation
- Vein: May run along the nerve
- Look for nerve compression, distortion, or grooving at the REZ (proximal 5mm of nerve where central myelin transitions to peripheral myelin)
- Mobilize the offending vessel — gently dissect the vessel away from the nerve
- Place Teflon felt pledget — interpose between the vessel and the nerve to prevent re-contact
- Shape and size the Teflon to keep the vessel displaced
- Do NOT pack Teflon too tightly (can cause new compression)
- Inspect for additional compressive vessels — multiple vessels may be present
- If venous compression: Decision to coagulate and divide vs. transpose. Veins are harder to decompress; petrosal vein sacrifice is sometimes necessary but risks venous infarction
- If NO clear offending vessel found:
- Inspect thoroughly (360 degrees around nerve)
- Consider arachnoid bands causing tethering
- May still decompress (some occult compression)
- Consider partial sensory rhizotomy as adjunct (less preferred)
- Hemostasis and inspection — ensure no bleeding, cerebellar surface intact
- Dural closure — watertight (primary or with dural graft)
- Cranioplasty — replace bone or methylmethacrylate/titanium mesh over defect
- Standard closure
Critical Anatomy & Structures at Risk
- Trigeminal nerve (CN V) — the nerve being decompressed; avoid manipulation/traction
- CN VII/VIII complex — runs inferior to CN V in the CPA; at risk during approach
- AICA — gives off the labyrinthine artery (supplies inner ear); avoid compression or vasospasm
- Superior petrosal vein (Dandy vein) — drains lateral cerebellar surface; sacrifice may be needed for exposure but risks venous infarction
- Cerebellar surface — avoid excessive retraction
- Sigmoid and transverse sinuses — lateral and superior limits of craniotomy; injury causes hemorrhage
- Vertebral artery — deep in the CPA; at risk with large vessel decompression
- Brainstem — medial limit; avoid any instrument contact
Equipment
- Operating microscope (essential)
- High-speed drill (craniotomy)
- Microsurgical instruments
- Teflon felt (for decompression pledgets)
- Bipolar forceps (fine tip)
- Brain retractor (small, self-retaining — minimal use)
- Hemostatic agents (Surgicel, Gelfoam)
- Bone fixation or cranioplasty material
Monitoring
- BAER (Brainstem Auditory Evoked Responses) — monitors CN VIII; changes suggest AICA/labyrinthine artery compromise
- Facial nerve EMG (CN VII) — detects inadvertent facial nerve stimulation
- Lateral spread response (LSR) — for hemifacial spasm (not TN, but done in same approach)
- SSEPs
Anesthesia Considerations
- Arterial line
- Foley
- Cefazolin 2g IV
- Dexamethasone 10 mg IV
- No paralytic after intubation (EMG monitoring)
- Mannitol 0.5-1 g/kg (for cerebellar relaxation)
- Antiemetic prophylaxis (posterior fossa surgery → high nausea risk)
Potential Complications & Contingencies
- Hearing loss — AICA/labyrinthine artery compromise; monitor BAER; if changes, release retraction, check vessel
- Facial nerve palsy — traction injury during approach; gentle technique, monitor EMG
- CSF leak — watertight dural closure; if leak post-op, may need lumbar drain or wound revision
- Cerebellar hematoma/edema — minimize retraction; if post-op deficit, emergent CT
- Aseptic meningitis — chemical irritation from Teflon; steroids, supportive care
- Incomplete relief — ~70-80% pain-free at 5 years; recurrence may need reoperation or radiosurgery
- Facial numbness — usually from nerve manipulation; typically mild and improves
- Venous infarction — from petrosal vein sacrifice; minimize vein sacrifice
Operative Note Template
Preoperative Diagnosis: [Left/Right] trigeminal neuralgia (Type 1), medically refractory
Postoperative Diagnosis: Same; [SCA/AICA/vertebral artery/vein] compression of [left/right] trigeminal nerve at the root entry zone identified and decompressed
Procedure: [Left/Right] retrosigmoid craniotomy for microvascular decompression of the trigeminal nerve
[Include: positioning details (park bench), craniotomy size, CSF drainage, CN V identification, offending vessel identification and characterization (SCA/AICA, direction of compression, groove/distortion on nerve), Teflon pledget placement, BAER monitoring stability, watertight closure]
Postoperative Plan
- ICU or step-down x 24 hours (posterior fossa surgery)
- Neuro checks q1h x 24h (posterior fossa-specific: CN function, mental status, breathing pattern)
- Posterior fossa danger signs: Decreasing consciousness, irregular breathing, new CN deficit, cerebellar signs → EMERGENT CT → possible return to OR
- HOB 30 degrees
- CT head within 6 hours (rule out posterior fossa hematoma)
- Audiogram before discharge (compare to baseline)
- Trigeminal function assessment: Sensation V1/V2/V3, corneal reflex
- Facial nerve function: Symmetry, House-Brackmann grade
- Pain assessment: Expect immediate relief if decompression successful; may take days-weeks for full effect
- Taper TN medications SLOWLY (not immediately) — carbamazepine taper over 2-4 weeks
- Anti-emetics PRN (high nausea rate after posterior fossa surgery)
- DVT prophylaxis: SCDs, heparin SQ POD1
- Dexamethasone taper
- Wound care: Keep dry x 48h
- Activity: No heavy lifting x 4-6 weeks
- Follow-up: Clinic 2-4 weeks; long-term follow-up for recurrence monitoring
- Long-term success: ~70-80% pain-free at 5 years; ~90% initial success
Chief-Level Case Review
Use these as the senior-level mental model for Microvascular Decompression (MVD) for Trigeminal Neuralgia:
- Decision point: Define the symptom physiology: target circuit or offending vessel/nerve must match the history, exam, imaging, and intraoperative monitoring plan.
- Technical lever: Small errors matter: trajectory, lead/contact position, arachnoid dissection, cranial-nerve handling, or mapping threshold can be the difference between success and morbidity.
- Bailout: Have a stop rule: unacceptable mapping response, BAER/MEP/SSEP change, hemorrhage, CSF loss, poor target confidence, or patient intolerance should trigger a defined pivot.
- Postop watch: Postop success requires programming/follow-up details: neurologic exam, imaging, medication adjustment, device restrictions, wound care, and symptom-specific outcome tracking.
Common Pimp Questions
Use these to pressure-test preparation for Microvascular Decompression (MVD) for Trigeminal Neuralgia:
- What is the proximal-control plan before the lesion is manipulated?
- Which branch, perforator, or venous structure is most likely to be injured in this exposure?
- What are the intraoperative rupture steps, including temporary clip, suction, BP, and backup clip strategy?
- What confirms treatment success: ICG, Doppler, puncture/deflation, DSA, or postoperative CTA?
- What postoperative BP, vasospasm, antiplatelet, or anticoagulation issue changes the orders tonight?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Preferred approach side, sylvian split style, and cisternal-opening sequence: [attending-specific]
- Temporary clip threshold, burst-suppression preference, and BP during occlusion: [attending-specific]
- Clip manufacturer/shape sequence and whether Doppler, ICG, puncture, or intraop DSA is routine: [attending-specific]
- Antiplatelet/anticoagulation reversal and restart timing: [attending-specific]