
Case Prep: Clival Chordoma Resection
Case / Approach Snapshot
- Anatomy at risk: tumor compartment, arterial supply, venous drainage/sinuses, cranial nerves, white-matter tracts, pituitary/CSF pathways when relevant, and functional cortex.
- Operative steps: review imaging and goals, choose exposure, obtain brain relaxation, devascularize when possible, debulk internally, dissect capsule from critical structures, verify extent/safety, and reconstruct watertight closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: venous or arterial injury, swelling, seizure, cranial nerve or endocrine change, CSF leak, residual tumor left for safety, staged surgery, radiation, or adjuvant therapy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a clival chordoma presenting with [diplopia (CN VI) / headache / lower cranial neuropathy] planned for endoscopic endonasal [transclival] resection [± staged/combined approach].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
CNS Video Library
🧭 Operative approach: Endoscopic endonasal approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Clival Chordoma: Case Report and Review of Recent Developments in Surgical and Adjuvant Treatments — Khawaja AM. Polish journal of radiology 2017. PubMed
- Proton beam therapy for clival chordoma: Optimising rare cancer treatments in Australia — Mathew A. Journal of medical radiation sciences 2024. PubMed
- Clival Chordoma: Endoscopic Bilateral Transmaxillary Approach — Youssef AS. Journal of neurological surgery. Part B, Skull base 2019. PubMed
- Cytodiagnosis of Clival Chordoma — Giri R. Journal of cytology 2023. PubMed
- Clival chordoma — Tarshis LM. The Journal of otolaryngology 1976. PubMed
- Clival chordoma: a single-centre outcome analysis — Jägersberg M. Acta neurochirurgica 2017. PubMed
- Clival chordoma with drop metastases — Nor FEM. Journal of radiology case reports 2018. PubMed
- Surgical Outcomes of Clival Chordoma Through Endoscopic Endonasal Approach: A Single-Center Experience — Chen G. Frontiers in endocrinology 2022. PubMed
- Fractionated Radiotherapy After Gross Total Resection of Clival Chordoma: A Systematic Review of Survival Outcomes — Gendreau JL. Neurosurgery 2023. PubMed
- An unusual presentation of clival chordoma: a case report and review of the literature — Andijani M. British journal of neurosurgery 2020. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
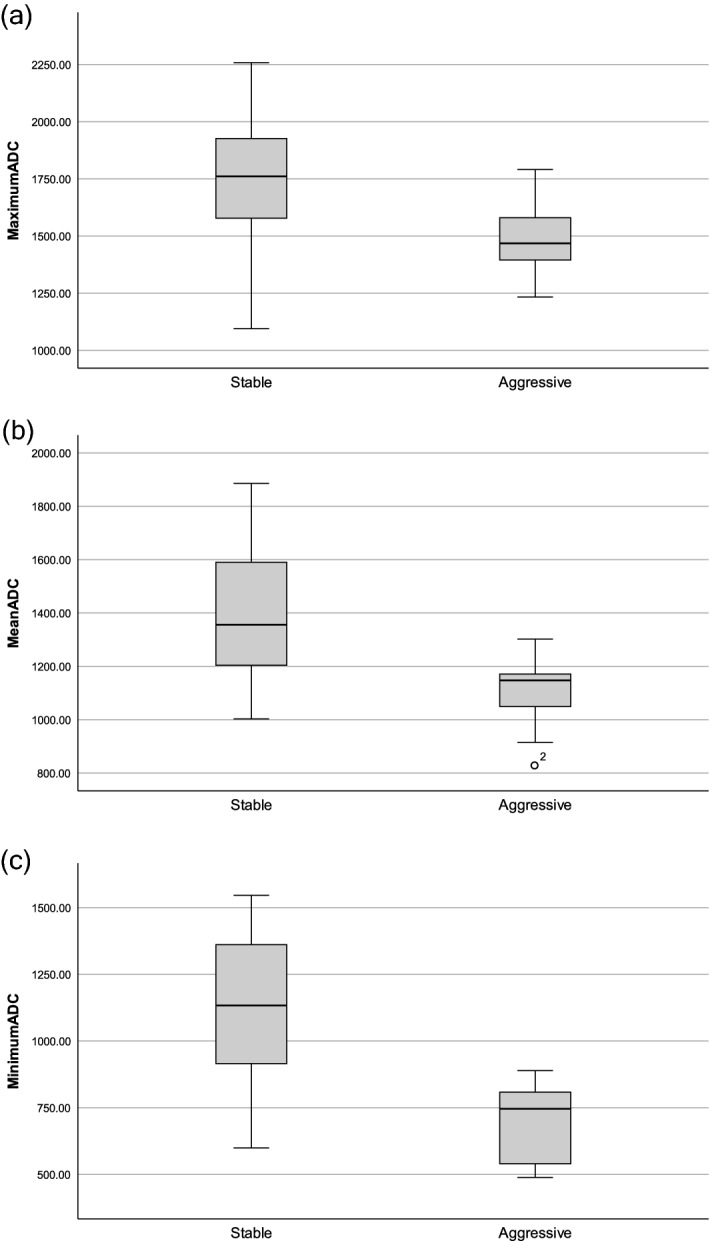 Figure 1. Comparison of ADC values between stable and aggressive chordoma (10–6 mm2/s). There were significant differences between groups in (a) maximum ADC (P = 0.012), (b) mean ADC (P < 0.001),… Source: Apparent diffusion coefficient as a prognostic factor in clival chordoma — Scientific Reports 2021; CC BY.
Figure 1. Comparison of ADC values between stable and aggressive chordoma (10–6 mm2/s). There were significant differences between groups in (a) maximum ADC (P = 0.012), (b) mean ADC (P < 0.001),… Source: Apparent diffusion coefficient as a prognostic factor in clival chordoma — Scientific Reports 2021; CC BY.
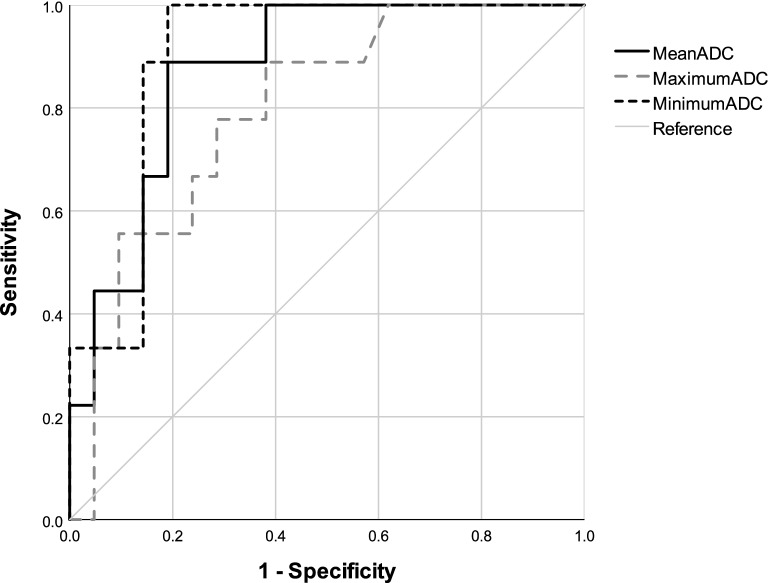 Figure 2. ROC curves for ADC values differentiating aggressive chordoma from stable chordoma. Source: Apparent diffusion coefficient as a prognostic factor in clival chordoma — Scientific Reports 2021; CC BY.
Figure 2. ROC curves for ADC values differentiating aggressive chordoma from stable chordoma. Source: Apparent diffusion coefficient as a prognostic factor in clival chordoma — Scientific Reports 2021; CC BY.
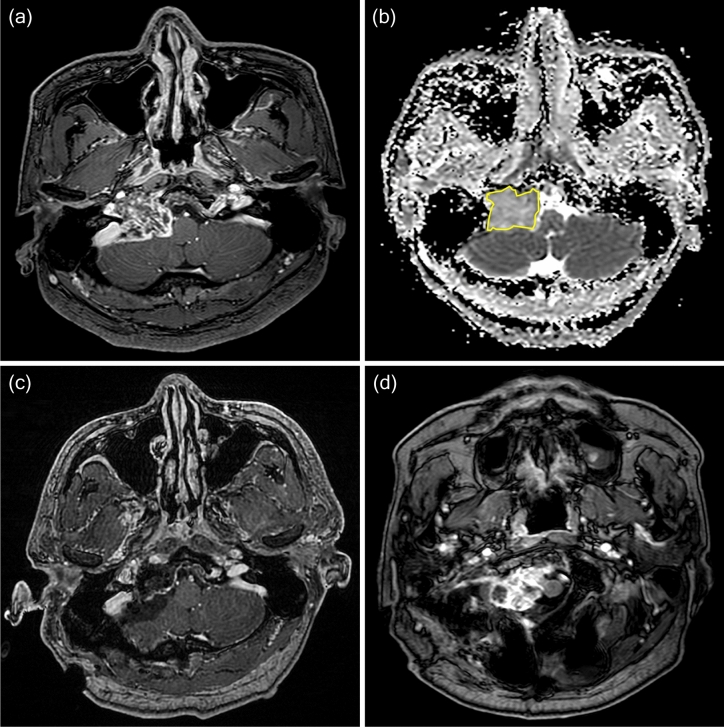 Figure 4. A 37-year-old man was diagnosed with classic chordoma and placed in the aggressive group. (a) Preoperative contrast enhanced T1-weighted imaging showed a tumor compressing the brainstem…. Source: Apparent diffusion coefficient as a prognostic factor in clival chordoma — Scientific Reports 2021; CC BY.
Figure 4. A 37-year-old man was diagnosed with classic chordoma and placed in the aggressive group. (a) Preoperative contrast enhanced T1-weighted imaging showed a tumor compressing the brainstem…. Source: Apparent diffusion coefficient as a prognostic factor in clival chordoma — Scientific Reports 2021; CC BY.
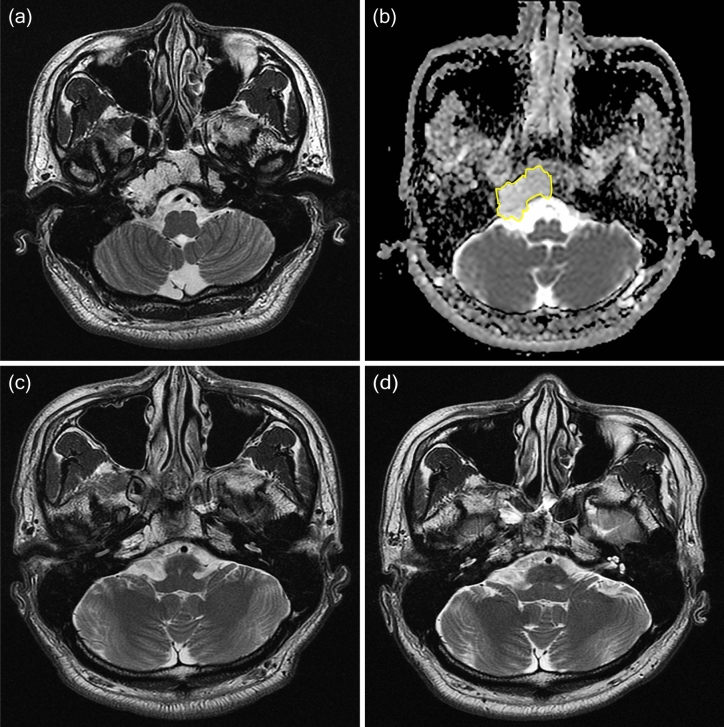 Figure 5. A 36-year-old man diagnosed with classic chordoma and placed in the stable group. (a) Preoperative T2-weighted imaging showed a T2 high signal mass arising from the clivus. (b) The ROI… Source: Apparent diffusion coefficient as a prognostic factor in clival chordoma — Scientific Reports 2021; CC BY.
Figure 5. A 36-year-old man diagnosed with classic chordoma and placed in the stable group. (a) Preoperative T2-weighted imaging showed a T2 high signal mass arising from the clivus. (b) The ROI… Source: Apparent diffusion coefficient as a prognostic factor in clival chordoma — Scientific Reports 2021; CC BY.
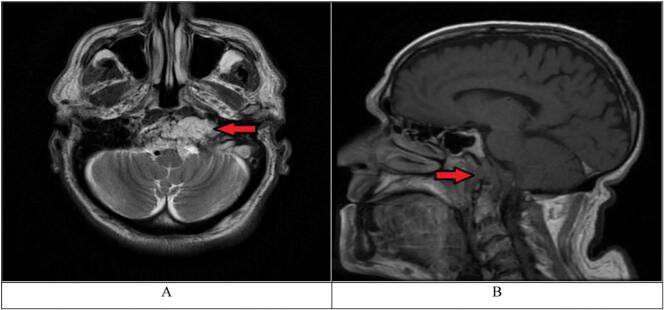 Fig. 1. A. T2-weighted MRI, axial view. The arrow shows hyperintense Clival lesion located 3 mm from the anterior end of the clivus, the mass can be seen compressing the left internal carotid… Source: Clival chordoma presenting with isolated unilateral cranial nerve XII palsy: A case report — International Journal of Surgery Case Reports 2024; CC BY.
Fig. 1. A. T2-weighted MRI, axial view. The arrow shows hyperintense Clival lesion located 3 mm from the anterior end of the clivus, the mass can be seen compressing the left internal carotid… Source: Clival chordoma presenting with isolated unilateral cranial nerve XII palsy: A case report — International Journal of Surgery Case Reports 2024; CC BY.
 Fig. 2. T2-weighted MRI, axial view. Signs of surgical intervention on the clivus are noted. The arrow shows residual tumor. (post-operative MRI). Source: Clival chordoma presenting with isolated unilateral cranial nerve XII palsy: A case report — International Journal of Surgery Case Reports 2024; CC BY.
Fig. 2. T2-weighted MRI, axial view. Signs of surgical intervention on the clivus are noted. The arrow shows residual tumor. (post-operative MRI). Source: Clival chordoma presenting with isolated unilateral cranial nerve XII palsy: A case report — International Journal of Surgery Case Reports 2024; CC BY.
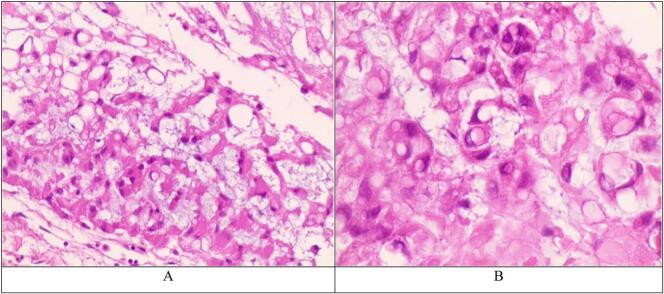 Fig. 3. A. Chordoma (H&E 100×). Prominent myxoid background containing small columns or clusters of bubbly physalipharous cells. B. Chordoma (H&E 400×). Occasional cells with irregular or… Source: Clival chordoma presenting with isolated unilateral cranial nerve XII palsy: A case report — International Journal of Surgery Case Reports 2024; CC BY.
Fig. 3. A. Chordoma (H&E 100×). Prominent myxoid background containing small columns or clusters of bubbly physalipharous cells. B. Chordoma (H&E 400×). Occasional cells with irregular or… Source: Clival chordoma presenting with isolated unilateral cranial nerve XII palsy: A case report — International Journal of Surgery Case Reports 2024; CC BY.
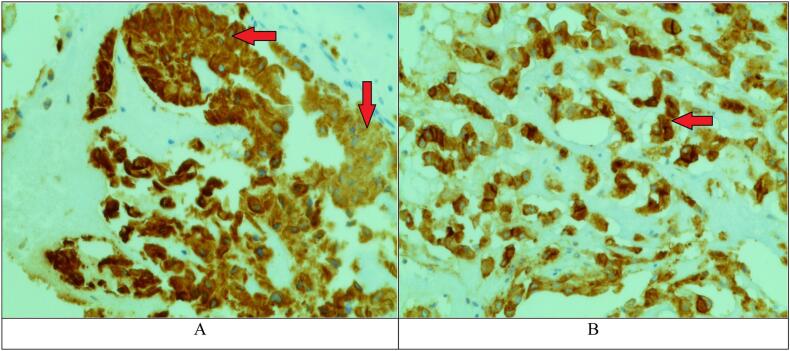 Fig. 4. A. Chordoma, Immunohistochemical staining. Arrows show positivity for cytokeratin (CK). B. Chordoma, Immunohistochemical staining. The arrow shows positivity for epithelial membrane… Source: Clival chordoma presenting with isolated unilateral cranial nerve XII palsy: A case report — International Journal of Surgery Case Reports 2024; CC BY.
Fig. 4. A. Chordoma, Immunohistochemical staining. Arrows show positivity for cytokeratin (CK). B. Chordoma, Immunohistochemical staining. The arrow shows positivity for epithelial membrane… Source: Clival chordoma presenting with isolated unilateral cranial nerve XII palsy: A case report — International Journal of Surgery Case Reports 2024; CC BY.
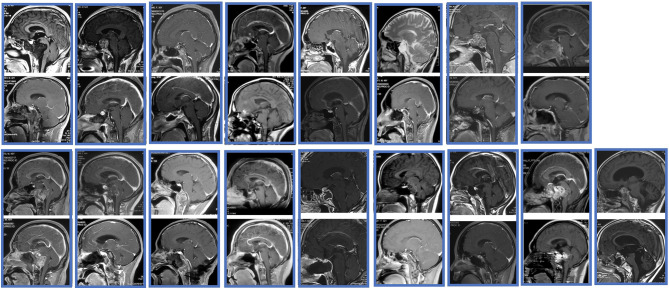 Figure 1. The pre- and post- MRIs of all the patients. Source: Surgical Outcomes of Clival Chordoma Through Endoscopic Endonasal Approach: A Single-Center Experience — Frontiers in Endocrinology 2022; CC BY.
Figure 1. The pre- and post- MRIs of all the patients. Source: Surgical Outcomes of Clival Chordoma Through Endoscopic Endonasal Approach: A Single-Center Experience — Frontiers in Endocrinology 2022; CC BY.
History of Present Illness
- Chief complaint: Diplopia (CN VI palsy — abducens along clivus, classic), headache, lower CN dysfunction, brainstem compression
- Locally aggressive, midline, bone-destructive; arises from notochordal remnants
- Prior treatment/surgery/radiation (often recurrent/multiply-operated)
Imaging Review
MRI (T1±Gad, T2)
- Midline clival mass, T2 hyperintense, heterogeneous enhancement
- Brainstem compression, extent (upper/mid/lower clivus), lateral extension (petrous, cavernous, jugular foramen)
- ICA (paraclival/cavernous) and basilar artery relationship/encasement
- Dural breach, intradural extension
CT / CTA
- Bony destruction, calcification, sequestered bone; ICA bony canal; craniocervical junction stability (lower clival/C1-2 → may need fusion)
Labs
- CBC, BMP, Coags, Type and crossmatch
Neurological Examination
- Full CN (VI especially, lower CNs), brainstem/long tracts, swallowing
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: navigation, endoscope/microscope as approach requires, ENT co-surgeon for endonasal cases, Doppler, lumbar drain only when indicated, reconstruction materials, and visual/endocrine baseline available.
- Special needs: steroid strategy individualized (Cushing workup may require avoiding preop steroids), DI/sodium protocol, AM cortisol/endocrine labs, visual-check plan, arterial line for large/vascular cases, and CSF-leak/nasal precautions.
- Immediate postop orders: neuro and visual checks, strict I/O with sodium/urine specific gravity schedule when pituitary stalk risk exists, cortisol/endocrine replacement plan, nasal precautions, MRI/CT timing, steroid taper, and DVT prophylaxis timing.
Diagnosis & Indication
- Indication: Maximal safe resection (extent of resection is the strongest prognostic factor) followed by high-dose proton/photon radiation
- Endoscopic endonasal transclival is workhorse for midline; lateral extension may need combined/transcranial or far-lateral
- Goals: Gross total/maximal resection while preserving neurovascular structures; en bloc when feasible (usually piecemeal due to location)
Position
- Supine, slight extension, navigation (CT/MR + CTA fusion), possible lumbar drain
- ENT co-surgeon (endonasal)
Key Surgical Steps (Endoscopic Endonasal Transclival)
- Nasal phase, nasoseptal flap(s) harvested (reconstruction — may need bilateral/extended)
- Wide sphenoidotomy, posterior septectomy
- Identify and skeletonize both paraclival/cavernous ICAs (navigation + micro-Doppler) — define safe lateral corridor between carotids
- Drill clival bone, remove tumor + involved bone (chordoma invades bone — must remove affected bone)
- Work between the carotids; for intradural extension, open dura, debulk off brainstem/basilar
- Preserve CN VI (Dorello canal), basilar perforators, brainstem
- Maximal resection; accept residual on encased ICA/basilar/brainstem
- Robust multilayer skull base reconstruction (fascia lata, fat, nasoseptal flap, sealant ± lumbar drain) — high CSF leak risk (clival/posterior fossa)
Critical Anatomy & Structures at Risk
- Internal carotid arteries (paraclival/cavernous) — define lateral limits; injury catastrophic
- Basilar artery and perforators, brainstem (pons/medulla)
- CN VI (Dorello canal), lower cranial nerves (lateral/lower extension), CN III/IV
- Craniocervical junction stability (lower clival/condylar resection)
Equipment
- Endoscope + endonasal skull base set, navigation (CTA fusion), high-speed drill, micro-Doppler, ICG
- Nasoseptal flap, fascia lata/fat graft, sealant, lumbar drain
- CN stimulator
Monitoring
- SSEPs, MEPs, CN EMG (VI, lower CNs), BAER
Anesthesia
- Arterial line, crossmatched blood, ICA injury contingency (rapid transfusion, neuroIR on standby for sacrifice/embolization), long case
Potential Complications
- ICA injury — life-threatening; pack, balloon/embolize, angiography
- CSF leak (high) — robust reconstruction
- CN deficits (VI common), brainstem injury
- Craniocervical instability (may need occipitocervical fusion)
- Recurrence (high — adjuvant radiation essential), meningitis
Operative Note Template
Preoperative Diagnosis: Clival chordoma [with brainstem compression / CN VI palsy]
Postoperative Diagnosis: Same
Procedure: Endoscopic endonasal transclival resection of clival chordoma with multilayer skull base reconstruction [nasoseptal flap]
Surgeon / Assistant: Neurosurgery + ENT skull base co-surgeon Anesthesia: General endotracheal EBL / Fluids / Blood products: [crossmatched; ICA-injury contingency ready] Adjuncts: Neuronavigation with CTA fusion, micro-Doppler, ICG, high-speed drill, CN EMG (VI, lower CNs)/SSEP/MEP; lumbar drain Implants: Fascia lata/fat graft, nasoseptal flap, sealant Complications: None
Indications: [Age]yo [M/F] with a clival chordoma causing [diplopia (CN VI)/brainstem compression]. Maximal safe resection followed by proton/photon radiation was planned. Risks (ICA injury, CSF leak, CN deficits, CCJ instability) discussed; rapid-transfusion and neuro-IR contingency arranged.
Description of Procedure: After consent and time-out, general anesthesia was induced, navigation registered with CTA fusion, and a lumbar drain placed. With the ENT co-surgeon, a nasal phase with nasoseptal flap harvest, wide sphenoidotomy, and posterior septectomy was performed. Both paraclival ICAs were identified and skeletonized with navigation and micro-Doppler, defining the safe intercarotid corridor.
The clival bone and tumor were drilled and removed, including involved bone. Working between the carotids, [the dura was opened for the intradural component and tumor debulked off the brainstem and basilar artery], preserving CN VI (Dorello canal), basilar perforators, and the brainstem. Maximal resection was achieved; residual encasing the ICA/basilar/brainstem was left. A robust multilayer skull base reconstruction was performed with fascia lata, fat, the vascularized nasoseptal flap, and sealant.
The patient was transferred to the ICU with CSF-leak precautions and the lumbar drain in place.
Postoperative Plan
- ICU, neuro checks q1h
- CSF leak precautions, lumbar drain management, DI/Na if sellar involvement
- CN VI and lower CN assessment, swallow eval
- MRI/CT postop (EOR), watch rhinorrhea/meningitis/pneumocephalus
- Adjuvant proton/photon radiation (essential), tumor board
- CCJ stability assessment; long-term surveillance MRI
Chief-Level Case Review
Use these as the senior-level mental model for Clival Chordoma Resection:
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Clival Chordoma Resection:
- What is the surgical goal: gross-total, maximal safe, decompression, diagnosis, or cytoreduction?
- What eloquent cortex, tract, cranial nerve, vessel, or sinus defines the stopping point?
- What adjunct changes the case: navigation, mapping, 5-ALA, ultrasound, endoscope, ICG, or neuromonitoring?
- What is the edema, steroid, seizure, DVT, and postop imaging plan?
- What complication would you check for first in PACU based on this lesion location?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Extent-of-resection goal and functional stopping points: [attending-specific]
- Mapping/monitoring, 5-ALA, ultrasound, ICG, endoscope, or tractography preferences: [attending-specific]
- Steroid, antiepileptic, mannitol/hypertonic saline, and antibiotic plan: [attending-specific]
- Postop MRI timing, ICU/floor threshold, and adjuvant-referral workflow: [attending-specific]