
Operative Approach: Subtemporal Craniotomy (± Zygomatic Osteotomy / Anterior Petrosectomy)
Case / Approach Snapshot
- Anatomy at risk: corridor-defining nerves, arteries, veins/sinuses, cisterns, bone landmarks, muscle/fascial planes, and closure structures that determine exposure and morbidity.
- Operative steps: confirm position and trajectory, mark landmarks, protect soft tissue and named neurovascular structures, perform the bone/soft-tissue corridor, open/close dura or target compartment deliberately, and verify hemostasis/reconstruction; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: brain relaxation failure, venous or sinus bleeding, cranial nerve/perforator risk, exposure that is too narrow, CSF leak, cosmetic/temporalis/frontalis problems, and conversion to a wider or alternate corridor.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas — Subtemporal · Radiopaedia — petroclival · PubMed Central — subtemporal / Kawase
High-Yield Literature
- Anterior Petrosectomy vs. Retrosigmoid Approach-Surgical Anatomy and Navigation-Augmented Morphometric Analysis: A Comparative Study in Cadaveric Laboratory Setting — Signoretti S. Brain sciences 2025. PubMed
- Cranio-Orbito-Zygomatic Approach: Core Techniques for Tailoring Target Exposure and Surgical Freedom — Luzzi S. Brain sciences 2022. PubMed
- The posterior subtemporal keyhole approach combined with the transchoroidal approach to the ambient cistern: microsurgical anatomy and image-guided quantitative analysis — Wang H. Acta neurochirurgica 2010. PubMed
- Tentorial dural arteriovenous fistulas — Zhou LF. Surgical neurology 2007. PubMed
- Combined transsylvian-subtemporal exposure of cerebral aneurysms involving the basilar apex — Kopitnik TA. Microsurgery 1994. PubMed
- Subtemporal approach to posterior cerebral artery aneurysms — Goehre F. World neurosurgery 2015. PubMed
- Surgical approaches for the lateral mesencephalic sulcus — Cavalcanti DD. Journal of neurosurgery 2020. PubMed
- Microsurgical Management of Blister-Type Basilar Artery Apex Region Aneurysms: Companion Cases Demonstrate Technical Nuances of the Subtemporal Approach: 2-Dimensional Operative Video — Howard BM. Operative neurosurgery (Hagerstown, Md.) 2021. PubMed
- Comparison of lateral microsurgical preauricular and anterior endoscopic approaches to the jugular foramen — Komune N. The Journal of laryngology and otology 2015. PubMed
- The oculomotor-tentorial triangle. Part 1: microsurgical anatomy and techniques to enhance exposure — Tayebi Meybodi A. Journal of neurosurgery 2019. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
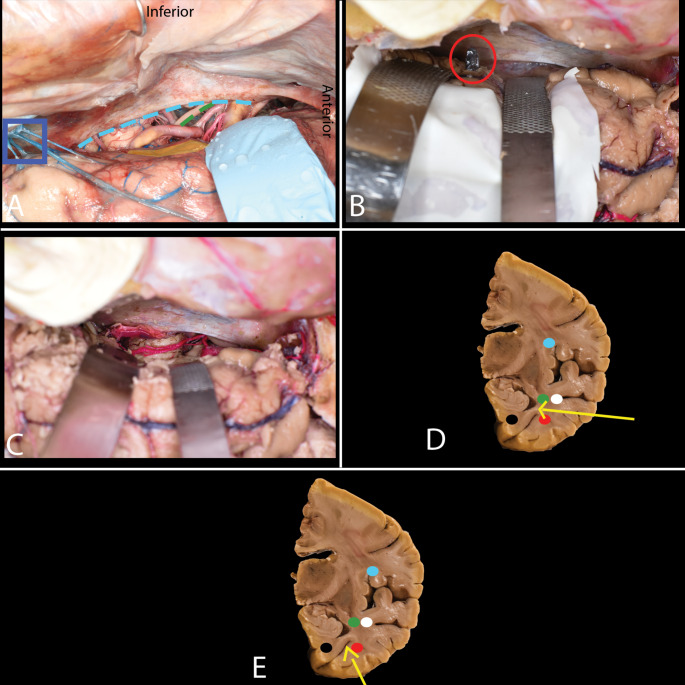 Fig. 4. Subtemporal approach. A-E. A A retractor is placed under the brain, identifying the collateral sulcus. A cortical incision is made near the uncus (yellow), and care is taken to preserve… Source: Anatomical considerations in selective amygdalohippocampectomy techniques for refractory temporal lobe epilepsy: a cadaveric study with emphasis on white matter tract anatomy — Surgical and Radiologic Anatomy 2024; CC BY.
Fig. 4. Subtemporal approach. A-E. A A retractor is placed under the brain, identifying the collateral sulcus. A cortical incision is made near the uncus (yellow), and care is taken to preserve… Source: Anatomical considerations in selective amygdalohippocampectomy techniques for refractory temporal lobe epilepsy: a cadaveric study with emphasis on white matter tract anatomy — Surgical and Radiologic Anatomy 2024; CC BY.
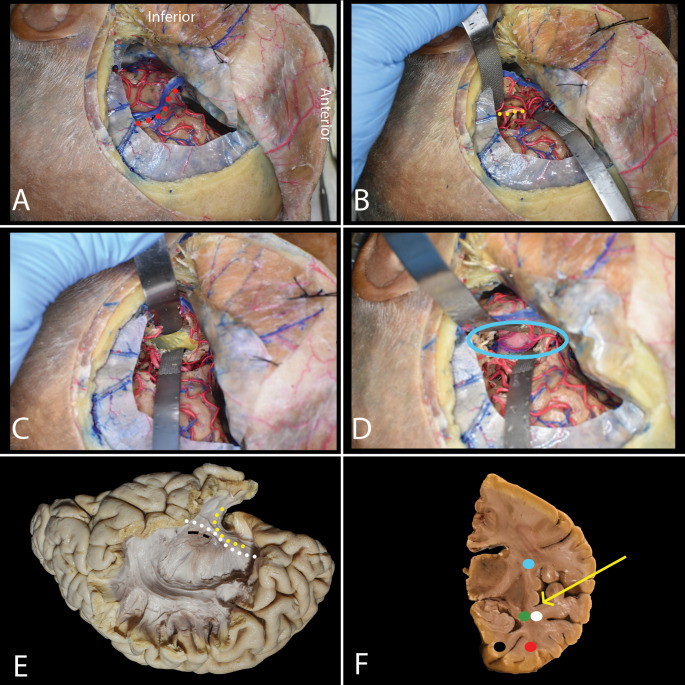 Fig. 5. Transsylvian approach. A-E. A A pterional craniotomy is performed. The sylvian fissure (red dots) is opened from the internal carotid artery bifurcation to 2 cm beyond the MCA… Source: Anatomical considerations in selective amygdalohippocampectomy techniques for refractory temporal lobe epilepsy: a cadaveric study with emphasis on white matter tract anatomy — Surgical and Radiologic Anatomy 2024; CC BY.
Fig. 5. Transsylvian approach. A-E. A A pterional craniotomy is performed. The sylvian fissure (red dots) is opened from the internal carotid artery bifurcation to 2 cm beyond the MCA… Source: Anatomical considerations in selective amygdalohippocampectomy techniques for refractory temporal lobe epilepsy: a cadaveric study with emphasis on white matter tract anatomy — Surgical and Radiologic Anatomy 2024; CC BY.
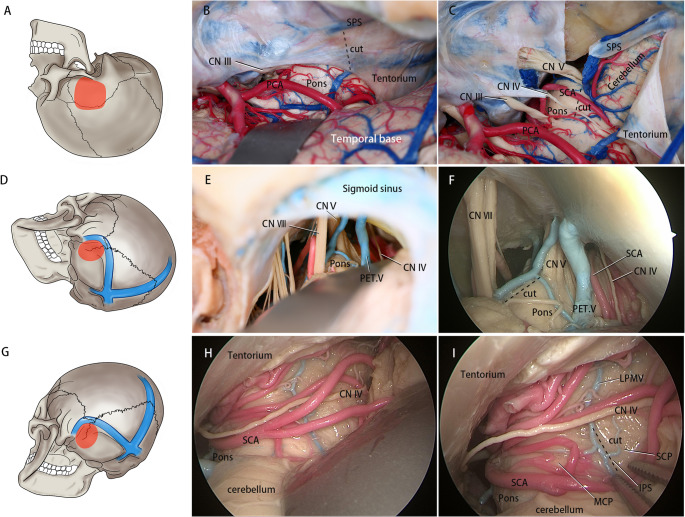 Fig. 1. A-C Subtemporal Transtentorial Approach (A): Schematic of the Subtemporal Transtentorial Approach craniotomy bone flap. (B): Following elevation of the temporal base, the tentorium is… Source: Analysis of Pontine cavernous malformation resection based on 3D microanatomical study — Neurosurgical Review 2025; CC BY-NC-ND.
Fig. 1. A-C Subtemporal Transtentorial Approach (A): Schematic of the Subtemporal Transtentorial Approach craniotomy bone flap. (B): Following elevation of the temporal base, the tentorium is… Source: Analysis of Pontine cavernous malformation resection based on 3D microanatomical study — Neurosurgical Review 2025; CC BY-NC-ND.
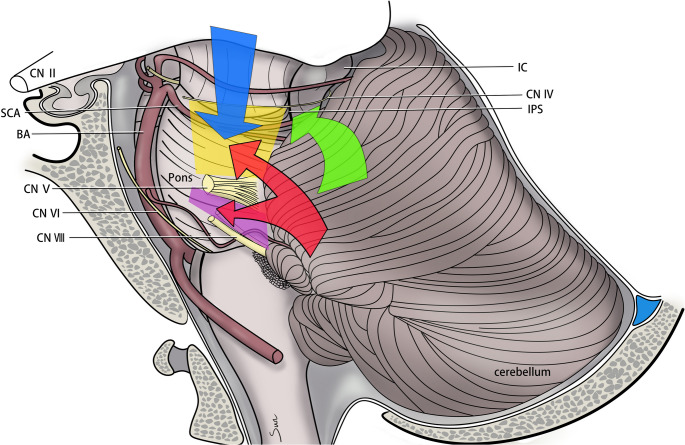 Fig. 4. Exposure ranges of surgical approaches and safety entry zones (Yellow quadrilateral: Superior trigeminal quadrangular space. Purple quadrilateral: Inferior trigeminal quadrangular space…. Source: Analysis of Pontine cavernous malformation resection based on 3D microanatomical study — Neurosurgical Review 2025; CC BY-NC-ND.
Fig. 4. Exposure ranges of surgical approaches and safety entry zones (Yellow quadrilateral: Superior trigeminal quadrangular space. Purple quadrilateral: Inferior trigeminal quadrangular space…. Source: Analysis of Pontine cavernous malformation resection based on 3D microanatomical study — Neurosurgical Review 2025; CC BY-NC-ND.
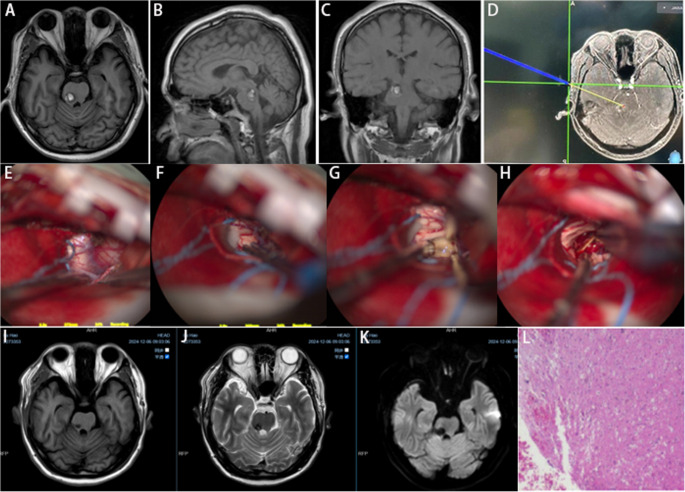 Fig. 5. A-C Preoperative magnetic resonance imaging (MRI) demonstrates hemorrhagic stroke within the right PCMs. D Stereotactic guidance was employed to define the surgical trajectory. E-H A… Source: Analysis of Pontine cavernous malformation resection based on 3D microanatomical study — Neurosurgical Review 2025; CC BY-NC-ND.
Fig. 5. A-C Preoperative magnetic resonance imaging (MRI) demonstrates hemorrhagic stroke within the right PCMs. D Stereotactic guidance was employed to define the surgical trajectory. E-H A… Source: Analysis of Pontine cavernous malformation resection based on 3D microanatomical study — Neurosurgical Review 2025; CC BY-NC-ND.
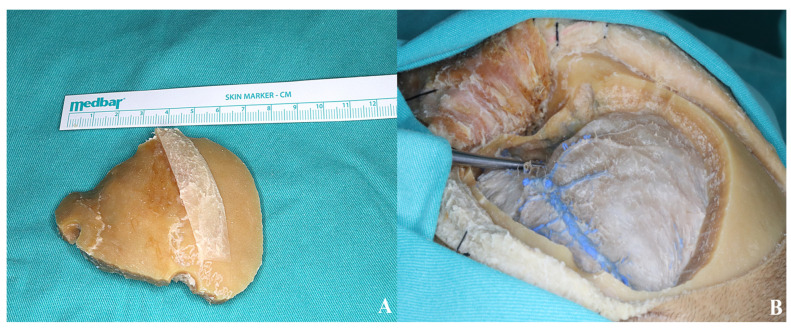 Figure 6. (A) Bone flap. (B) The thinned sphenoid ridge is demonstrated following basal drilling with the aid of a dissector. Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
Figure 6. (A) Bone flap. (B) The thinned sphenoid ridge is demonstrated following basal drilling with the aid of a dissector. Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
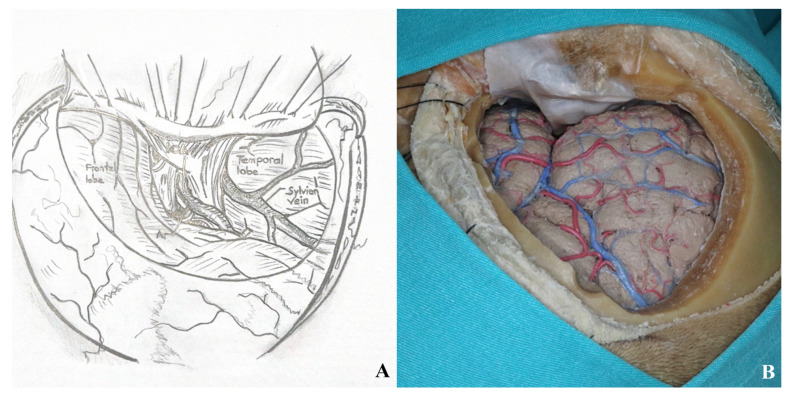 Figure 7. After the dural incision was made, the dura was elevated and suspended. (A). Illustration, (B). Cadaver footage. Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
Figure 7. After the dural incision was made, the dura was elevated and suspended. (A). Illustration, (B). Cadaver footage. Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
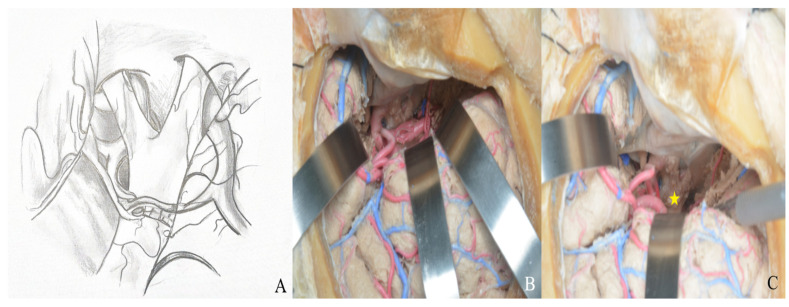 Figure 8. (A) Exposure of the lamina terminalis. (B) After Sylvian fissure dissection, retractors provided access to the anterior and middle skull base. (C) The lamina terminalis cistern was… Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
Figure 8. (A) Exposure of the lamina terminalis. (B) After Sylvian fissure dissection, retractors provided access to the anterior and middle skull base. (C) The lamina terminalis cistern was… Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
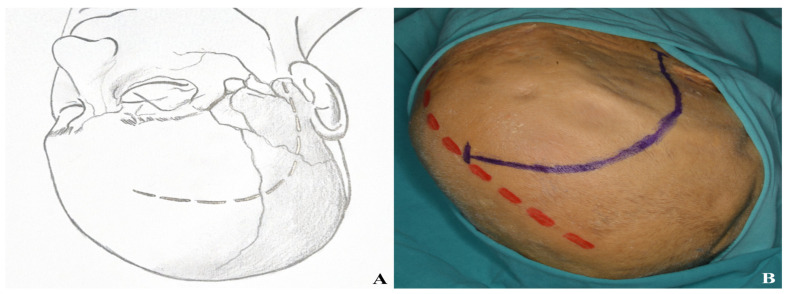 Figure 9. Incision plan for the one-piece orbitozygomatic approach [(A) incision sketch, (B) cadaver view: red line indicating midline; blue line indicating incision]. Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
Figure 9. Incision plan for the one-piece orbitozygomatic approach [(A) incision sketch, (B) cadaver view: red line indicating midline; blue line indicating incision]. Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
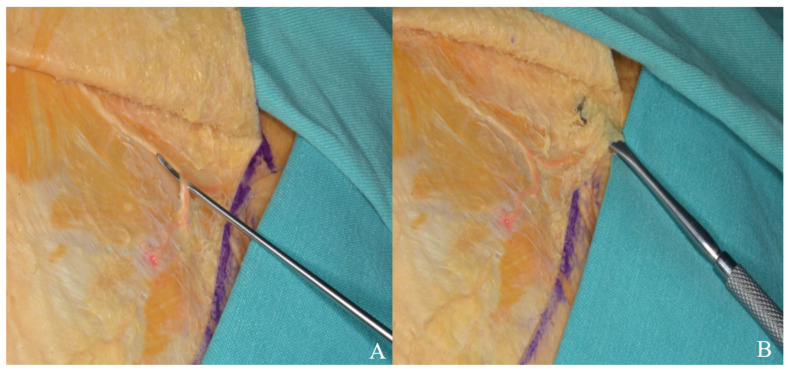 Figure 10. The skin flap was retracted anteriorly, and the superficial temporal artery (A) and facial nerve branches (B) were carefully dissected and mobilized with a dissector. Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
Figure 10. The skin flap was retracted anteriorly, and the superficial temporal artery (A) and facial nerve branches (B) were carefully dissected and mobilized with a dissector. Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
The subtemporal craniotomy is the inferolateral middle-fossa corridor to the tentorial incisura, lateral midbrain, and upper posterior fossa. By elevating the temporal lobe off the middle-fossa floor, the surgeon looks medially across the incisura to the crural/ambient/interpeduncular cisterns — reaching the basilar trunk and apex, SCA/PCA, P1–P2, CN III and IV, the posterior cavernous sinus, and Meckel’s cave. Adding a zygomatic osteotomy drops the temporalis and reduces temporal-lobe retraction; adding an anterior petrosectomy (Kawase) extends the reach to the petroclival junction, upper clivus, and ventral pons.
General Considerations
- What it accesses: the tentorial incisura and its three cisternal compartments (crural, ambient, interpeduncular) and the lateral midbrain; the upper basilar complex; Meckel’s cave and the posterior cavernous sinus. With petrous apex drilling it crosses into the petroclival region.
- The defining trade-off is temporal-lobe retraction. Everything in this approach is organized around minimizing it: a craniotomy flush to the floor, gravity (lateral position), CSF drainage (lumbar drain), and — when needed — a zygomatic osteotomy. The vein of Labbé is the anatomic limit; its preservation governs how far posteriorly the temporal lobe may be elevated.
- Extensions (know the ladder):
- + Zygomatic osteotomy → temporalis drops inferiorly; less retraction, wider upward angle (useful for higher basilar apex).
- + Anterior petrosectomy (Kawase/Glasscock-Kawase rhomboid) → extradural drilling of the petrous apex medial to the IAC opens the petroclival junction and the ventral pons / upper basilar trunk with tentorial division.
- Combined petrosal / presigmoid when the lesion spans the whole clivus (see presigmoid-petrosal-approach.md).
Indications
- Low-lying basilar apex / basilar trunk and SCA aneurysms (an alternative/complement to orbitozygomatic) → see basilar-tip-aneurysm.md
- Petroclival meningioma (anterior petrosectomy variant) → see petroclival-meningioma.md
- Trigeminal schwannoma / Meckel’s cave and posterior cavernous sinus lesions
- Lateral mesencephalic / tentorial-incisural lesions (e.g., midbrain cavernoma via the lateral mesencephalic sulcus), tentorial meningioma
- Selected P2 PCA aneurysms, tentorial dural fistulas
Relevant Surgical Anatomy
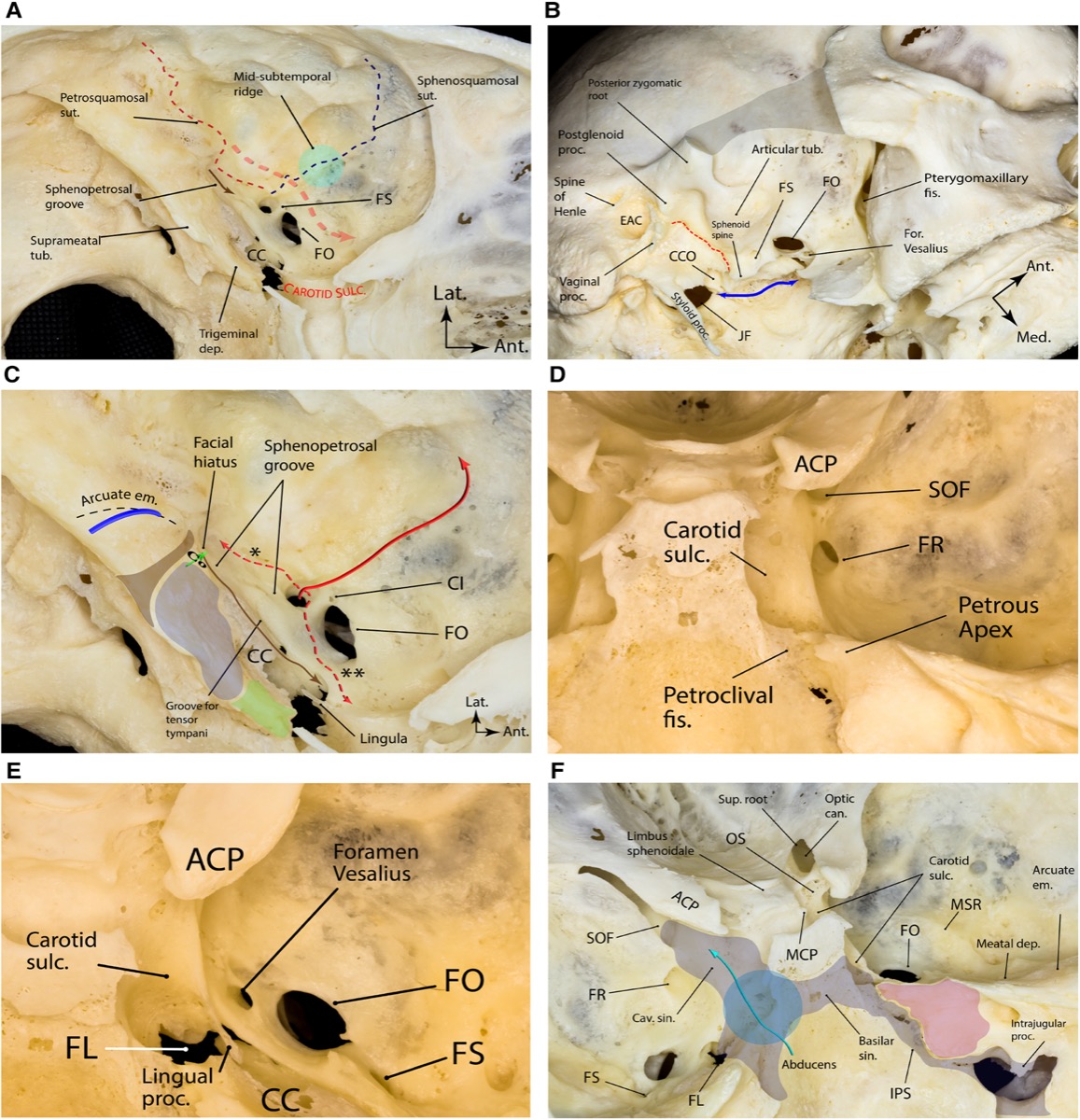
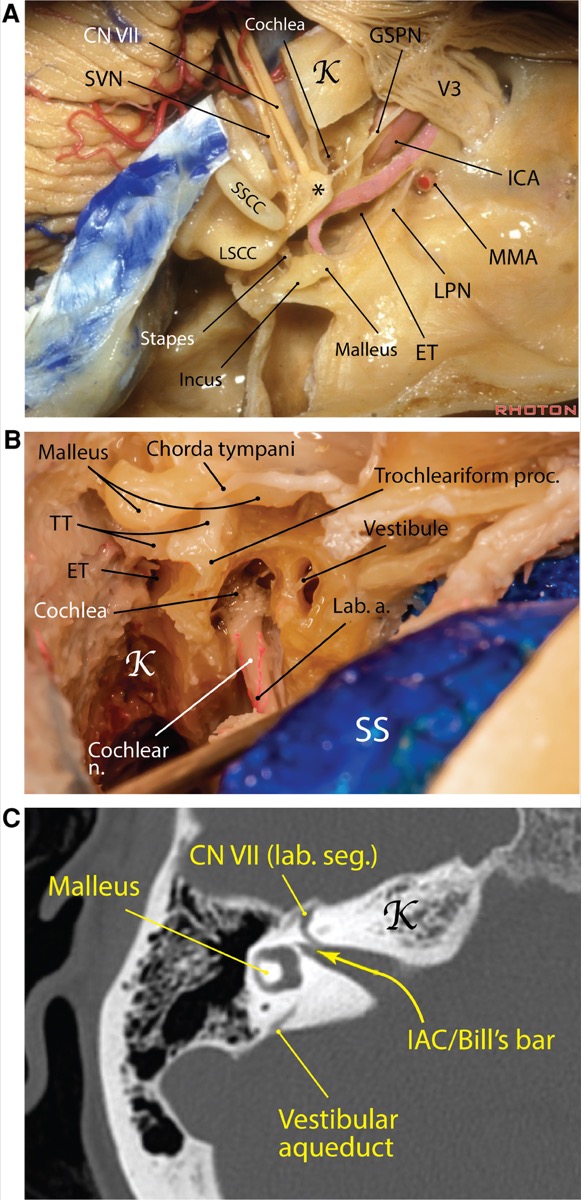
- Middle-fossa floor: from lateral to medial — foramen spinosum (MMA), foramen ovale (V3), arcuate eminence (superior semicircular canal), greater superficial petrosal nerve (GSPN) running to the facial hiatus, and the petrous ridge.
- Kawase’s (Glasscock-Kawase) rhomboid / anterior petrosectomy triangle: bounded by the GSPN (anterolateral), the petrous ridge/superior petrosal sinus (posterior), the arcuate eminence (posterolateral), and V3 / the trigeminal porus (anteromedial). Drilling this bone — medial to the IAC and cochlea, above the petrous ICA, anterior to the labyrinth — opens the petroclival window.
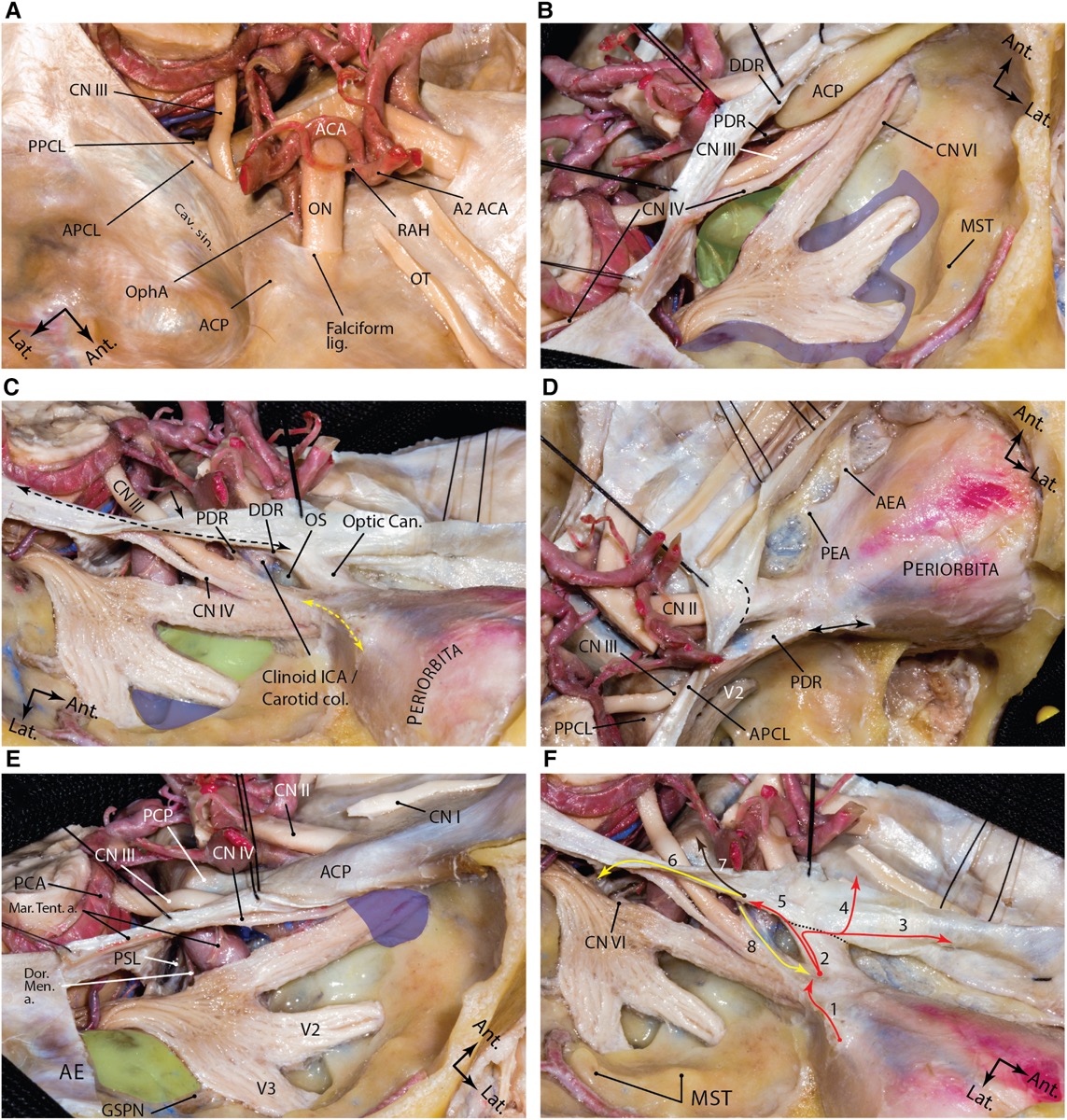
- Tentorial incisura: the free edge carries CN IV (enters the tentorium near the incisural apex — protect it during tentorial division), with CN III anteriorly at the interpeduncular cistern.
- Vein of Labbé: the dominant inferior anastomotic vein from the temporal lobe to the transverse sinus — sacrifice risks temporal venous infarction and (dominant side) aphasia.
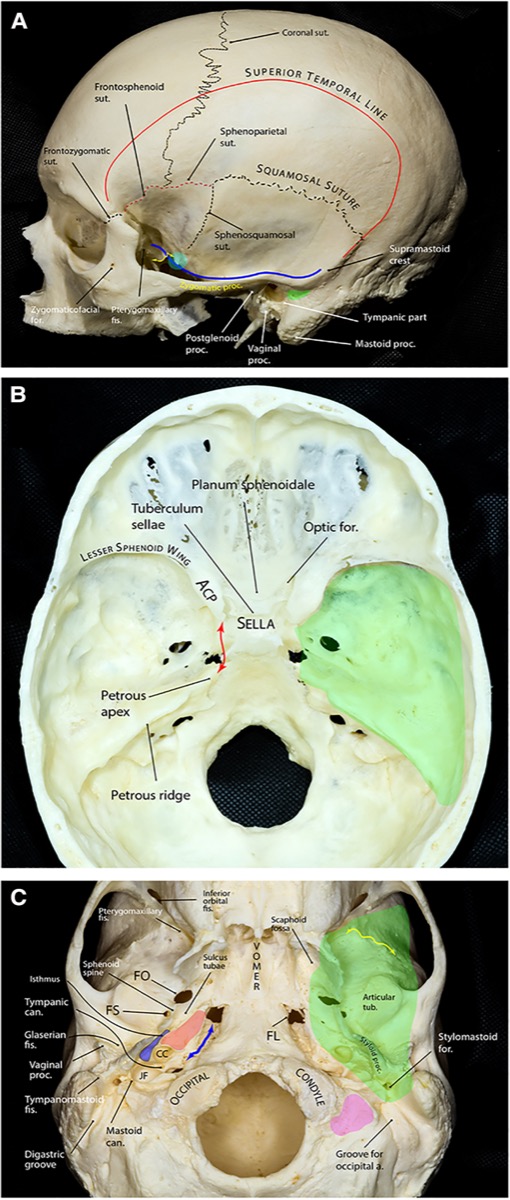
Comprehensive microsurgical anatomy of the middle cranial fossa, Part I. Front Surg 2023;10:1132774 — CC BY 4.0.
Preoperative Evaluation
- MRI/CISS for the lesion and the incisural cisterns; CTA/MRA for vascular targets and basilar apex height relative to the posterior clinoid.
- Thin-cut CT of the petrous bone before any petrosectomy: position of the cochlea, IAC, petrous ICA, and labyrinth; degree of air-cell pneumatization (CSF-leak risk).
- Vein of Labbé / venous anatomy (MRV) — dominant drainage influences retraction strategy and side.
- Audiometry/facial baseline if petrous drilling is planned. Dominant-hemisphere considerations for retraction.
Logistics, OR Setup & Orders
- OR setup: Mayfield/head holder plan, microscope/endoscope, navigation, vascular instruments/ICG when applicable, skull base reconstruction supplies, and approach-specific retractors/drills ready before opening.
- Special needs: arterial line for major intracranial or vascular cases, Foley for long cases, neuromonitoring by corridor, dexamethasone/antiepileptic/BP plan by pathology, and blood products for vascular or skull base exposure.
- Immediate postop orders: disposition and neuro-check frequency, HOB/activity, postop CT/MRI/CTA timing, BP goals, steroid/antiepileptic plan, DVT prophylaxis timing, drain management, and focused cranial nerve/visual/language/motor exams.
Anesthesia & Neuromonitoring
- GA/TIVA; lumbar drain is commonly placed to relax the temporal lobe (drain after dura is opened to avoid herniation). SSEP/MEP, BAER and facial EMG for petrous work, CN III/IV/VI EMG as indicated; EEG/burst-suppression for temporary clipping. Normotension.
Positioning
- Lateral or supine with a large ipsilateral shoulder roll, head in Mayfield, turned ~90° so the middle-fossa floor is roughly horizontal (vertex slightly down) — the temporal lobe then falls away from the floor by gravity, the single most effective way to limit retraction.
- The lateral position is favored for extensive work (gravity does more of the retraction); ensure the dependent shoulder/brachial plexus is protected and venous outflow is unobstructed.
- Slight neck extension brings the floor into view; confirm the zygoma is accessible if an osteotomy is planned.
Incision & Soft Tissue
- A question-mark or vertical/linear temporal incision centered over the ear root and zygoma (a “T”-bar or reverse-question-mark for larger exposures). Stay above the arch anteriorly to protect the facial nerve frontal branch (interfascial dissection if the flap extends anteriorly — see pterional).
- Reflect temporalis inferiorly; for a zygomatic osteotomy, expose the arch subperiosteally and cut it (anterior and posterior) so the temporalis drops, opening a flat trajectory to the floor.
Craniotomy
- A temporal craniotomy centered low over the middle fossa; rongeur/drill the inferior bone edge flush with the middle-fossa floor — any residual bony lip forces additional temporal-lobe retraction and must be removed.
- Wax exposed air cells. If a zygomatic osteotomy was done, the inferior trajectory is now flat.
- For the anterior petrosectomy variant, elevate the middle-fossa dura extradurally from posterior to anterior (to avoid avulsing the GSPN and a dehiscent geniculate facial nerve), identify the landmarks, and drill Kawase’s rhomboid.
Comprehensive microsurgical anatomy of the middle cranial fossa, Part I. Front Surg 2023;10:1132774 — CC BY 4.0. The anterior petrosectomy is drilled within this rhomboid, medial to the IAC/cochlea and above the petrous ICA.
Dural Opening & Intradural Work
- Open the temporal dura based inferiorly; elevate the temporal lobe gently (after CSF egress via the lumbar drain) to reach the tentorial edge. Identify and protect the vein of Labbé — do not tether or sacrifice it.
- Follow the free edge medially; identify CN IV entering the tentorium and CN III anteriorly. To open the posterior fossa, place a tentorial-edge stitch and divide the tentorium behind the entry point of CN IV, reflecting it to expose the petroclival/upper-basilar region.
- Open the incisural cisterns sharply: the crural and ambient cisterns (P2/PCA, SCA, basal vein), and the interpeduncular cistern (basilar apex, P1, perforators, CN III). Proceed to lesion-specific steps (basilar apex clipping, petroclival tumor via the petrosectomy window, Meckel’s cave/trigeminal schwannoma).
- Anterior petrosectomy completed: with the rhomboid drilled and the superior petrosal sinus/tentorium divided, the ventral pons and mid-upper clivus come into view for petroclival lesions.
Closure
- Watertight dura with graft as needed (the temporal floor and any petrous defect are leak-prone); obliterate drilled petrous air cells with fat/wax and reinforce with a vascularized flap (temporalis/pericranium) for petrosectomy defects.
- Replace the bone flap and re-plate the zygomatic arch anatomically if osteotomized. Reattach temporalis to limit hollowing/trismus. Lumbar drain managed per leak risk.
Further operative anatomy & technique
Comprehensive microsurgical anatomy of the middle cranial fossa, Part I. Front Surg 2023;10:1132774 — CC BY 4.0.
Comprehensive microsurgical anatomy of the middle cranial fossa, Part I. Front Surg 2023;10:1132774 — CC BY 4.0.
Nuances & Pitfalls (surgeon-level)
- The vein of Labbé is sacrosanct. Plan the corridor anterior to it; if posterior reach is needed, mobilize rather than divide. Venous infarction is the signature catastrophic complication.
- Take the bone to the floor. The commonest technical error is leaving an inferior bony lip that converts a gravity approach into a retraction approach.
- Lumbar drain then elevate. Relax the temporal lobe with CSF before any retraction; intermittent (not fixed, prolonged) retraction limits contusion/aphasia.
- Protect CN IV during tentorial division — divide behind its tentorial entry and tag the edge.
- Petrosectomy hazards: the petrous ICA (below the GSPN — avulsing the GSPN can tear a dehiscent geniculate facial nerve or injure the ICA), the cochlea (at the GSPN–arcuate-eminence angle), and the IAC/labyrinth. Drill within the rhomboid under navigation and with facial/BAER monitoring.
- Air cells = CSF leak. Wax/fat-graft meticulously, especially after petrous drilling.
- Decide on the zygomatic osteotomy up front when the target is high (basilar apex above the posterior clinoid) — it buys upward angle without more brain retraction.
Complications
Temporal-lobe contusion / venous infarction (vein of Labbé) and aphasia; CN III/IV palsy (diplopia); hearing loss/facial palsy and petrous ICA injury (petrosectomy); CSF leak; seizures; vascular/perforator injury at the basilar apex; trismus/temporal hollowing; infection.
Cross-links
- Related corridors: orbitozygomatic-craniotomy.md · presigmoid-petrosal-approach.md · pterional-craniotomy.md
- Pathology: basilar-tip-aneurysm.md · petroclival-meningioma.md
Figure Use & Attribution
About the figures. Copyrighted operative figures/videos are linked (Neurosurgical Atlas); embedded images are public-domain (Gray’s Anatomy) or CC‑BY (open-access cadaveric anatomy), credited beneath each image. See media-sources.md and figures/CREDITS.md.
Atlas chapter: Temporal / Subtemporal Craniotomy — Neurosurgical Atlas
Chief-Level Corridor Review
Use these as the senior-level mental model for Subtemporal Craniotomy (± Zygomatic Osteotomy / Anterior Petrosectomy):
- Decision point: Define the exposure goal before incision: target, working angles, proximal/distal control, and the structure that cannot tolerate retraction.
- Technical lever: Know the first irreversible step: bone removal, dural opening, vascular control, or muscle/fascial division that commits the corridor.
- Bailout: Verbalize the bailout: extend exposure, change trajectory, add CSF drainage, obtain proximal control, convert to a larger corridor, or stop for imaging.
- Postop watch: Protect closure from the start: vascularized tissue, watertight dural/reconstruction plan, dead-space control, and drain strategy should be chosen before the final intradural step.
Common Pimp Questions
Use these to pressure-test preparation for Subtemporal Craniotomy (± Zygomatic Osteotomy / Anterior Petrosectomy):
- What patient position and head rotation make gravity work for this corridor?
- What named nerve, vessel, sinus, or muscle/fascial plane is most commonly injured?
- What bone work or soft-tissue step creates the exposure rather than simply using more retraction?
- What is the bailout if exposure is inadequate, bleeding occurs, or the brain is tight?
- What closure maneuver prevents the signature complication of this approach?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Exact head rotation/flexion/extension and pin placement: [attending-specific]
- Skin incision length, flap type, and muscle/fascial preservation technique: [attending-specific]
- Drill, rongeur, endoscope, microscope, retractor, and navigation preferences: [attending-specific]
- Drain use, closure materials, watertightness threshold, and postop imaging routine: [attending-specific]
Case Guides Using This Approach
- No case guide currently links directly to this approach.
References
- Kawase T, Toya S, Shiobara R, Mine T. Transpetrosal approach for aneurysms of the lower basilar artery. J Neurosurg. 1985;63(6):857–861.
- Kawase T, Shiobara R, Toya S. Anterior transpetrosal-transtentorial approach for sphenopetroclival meningiomas. Neurosurgery. 1991;28(6):869–876.
- Day JD, Fukushima T, Giannotta SL. Cranial base approaches to posterior circulation aneurysms. J Neurosurg. 1997.
- Comprehensive microsurgical anatomy of the middle cranial fossa: Part I — Osseous and meningeal anatomy. Front Surg. 2023;10:1132774. CC BY 4.0. (figures embedded above)
- Rhoton AL Jr. The tentorial incisura and The middle cranial fossa. Neurosurgery (Rhoton anatomy series).
- Cohen-Gadol AA. Temporal/Subtemporal Craniotomy. The Neurosurgical Atlas. link