
Operative Approach: Orbitozygomatic (Frontotemporal-Orbitozygomatic, FTOZ) Craniotomy
Case / Approach Snapshot
- Anatomy at risk: corridor-defining nerves, arteries, veins/sinuses, cisterns, bone landmarks, muscle/fascial planes, and closure structures that determine exposure and morbidity.
- Operative steps: confirm position and trajectory, mark landmarks, protect soft tissue and named neurovascular structures, perform the bone/soft-tissue corridor, open/close dura or target compartment deliberately, and verify hemostasis/reconstruction; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: brain relaxation failure, venous or sinus bleeding, cranial nerve/perforator risk, exposure that is too narrow, CSF leak, cosmetic/temporalis/frontalis problems, and conversion to a wider or alternate corridor.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas — Orbitozygomatic · Radiopaedia — skull base · PubMed Central — orbitozygomatic
High-Yield Literature
- 360° around the orbit: key surgical anatomy of the microsurgical and endoscopic cranio-orbital and orbitocranial approaches — Agosti E. Neurosurgical focus 2024. PubMed
- Frontotemporal orbitozygomatic craniotomy to exposure the cavernous sinus and its surrounding regions. Microsurgical anatomy — Jian FZ. Journal of neurosurgical sciences 2001. PubMed
- Cranio-Orbito-Zygomatic Approach: Core Techniques for Tailoring Target Exposure and Surgical Freedom — Luzzi S. Brain sciences 2022. PubMed
- Comparison of the Orbitozygomatic and Transmandibular Approaches to the Infratemporal Fossa — Aydin L. World neurosurgery 2025. PubMed
- Lipotranferences in post neurosurgical esthetic defects — Demichelis MDRE. Surgical neurology international 2023. PubMed
- Critically located cavernous malformations — Batay F. Minimally invasive neurosurgery : MIN 2007. PubMed
- The pretemporal transcavernous approach to the interpeduncular and prepontine cisterns: microsurgical anatomy and technique application — Seoane E. Neurosurgery 2000. PubMed
- The one-piece orbitozygomatic approach: the MacCarty burr hole and the inferior orbital fissure as keys to technique and application — Aziz KM. Acta neurochirurgica 2002. PubMed
- Orbitozygomatic Transsylvian Resection of a Craniopharyngioma: A Step-by-Step Guide — Rodríguez RG. World neurosurgery 2023. PubMed
- Minimally invasive approaches to aneurysms of the anterior circulation: selection criteria and clinical outcomes — Gandhi S. Journal of neurosurgical sciences 2018. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
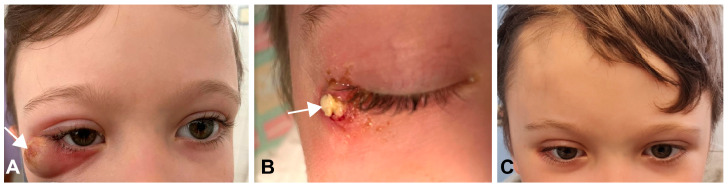 Figure 1. After the first (transconjunctival) surgery, a fistula and intermittent inflammatory symptoms developed in the orbital area and skin around the right outer canthus ((A,B); white arrow)…. Source: Modified Orbitozygomatic Craniotomy Approach for a Recurrent Orbital Tumor in a Pediatric Patient — Medicina 2024; CC BY.
Figure 1. After the first (transconjunctival) surgery, a fistula and intermittent inflammatory symptoms developed in the orbital area and skin around the right outer canthus ((A,B); white arrow)…. Source: Modified Orbitozygomatic Craniotomy Approach for a Recurrent Orbital Tumor in a Pediatric Patient — Medicina 2024; CC BY.
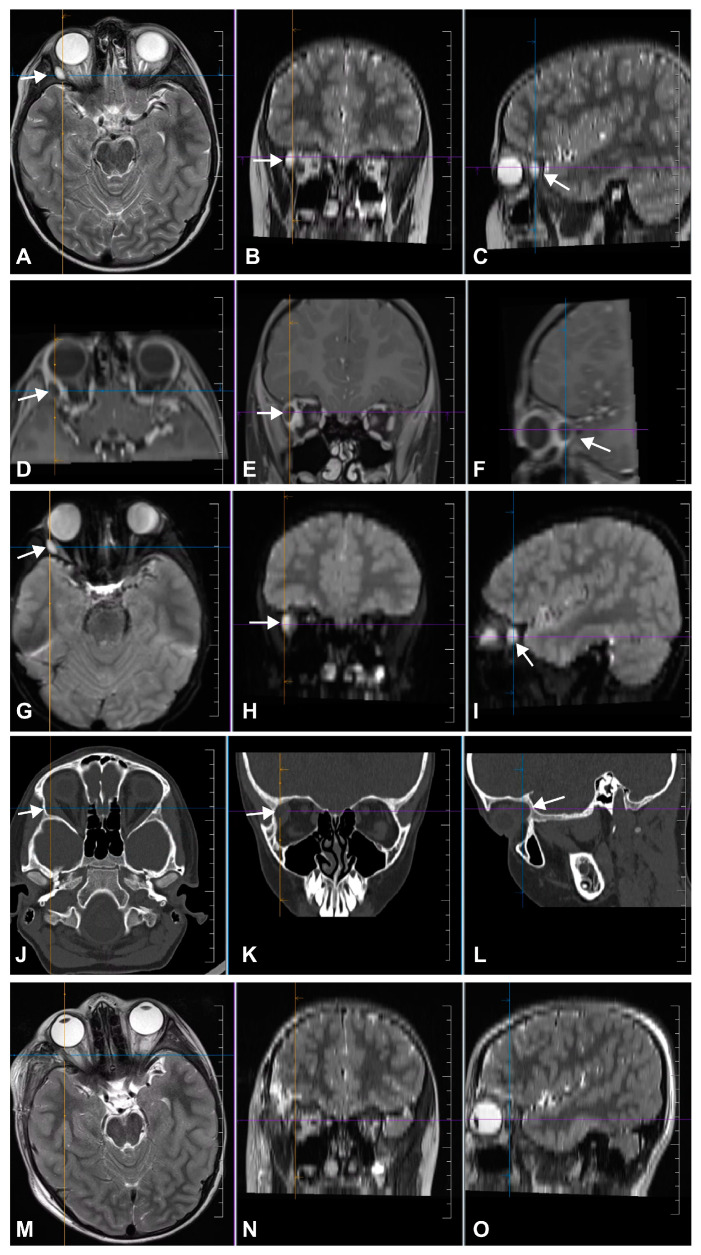 Figure 2. Radiographic work up. T2-(A–C) and T1-weighted MR images with contrast material (D–F) show a hyperintense lesion and an isointense lesion with postcontrast peripheral enhancement in the… Source: Modified Orbitozygomatic Craniotomy Approach for a Recurrent Orbital Tumor in a Pediatric Patient — Medicina 2024; CC BY.
Figure 2. Radiographic work up. T2-(A–C) and T1-weighted MR images with contrast material (D–F) show a hyperintense lesion and an isointense lesion with postcontrast peripheral enhancement in the… Source: Modified Orbitozygomatic Craniotomy Approach for a Recurrent Orbital Tumor in a Pediatric Patient — Medicina 2024; CC BY.
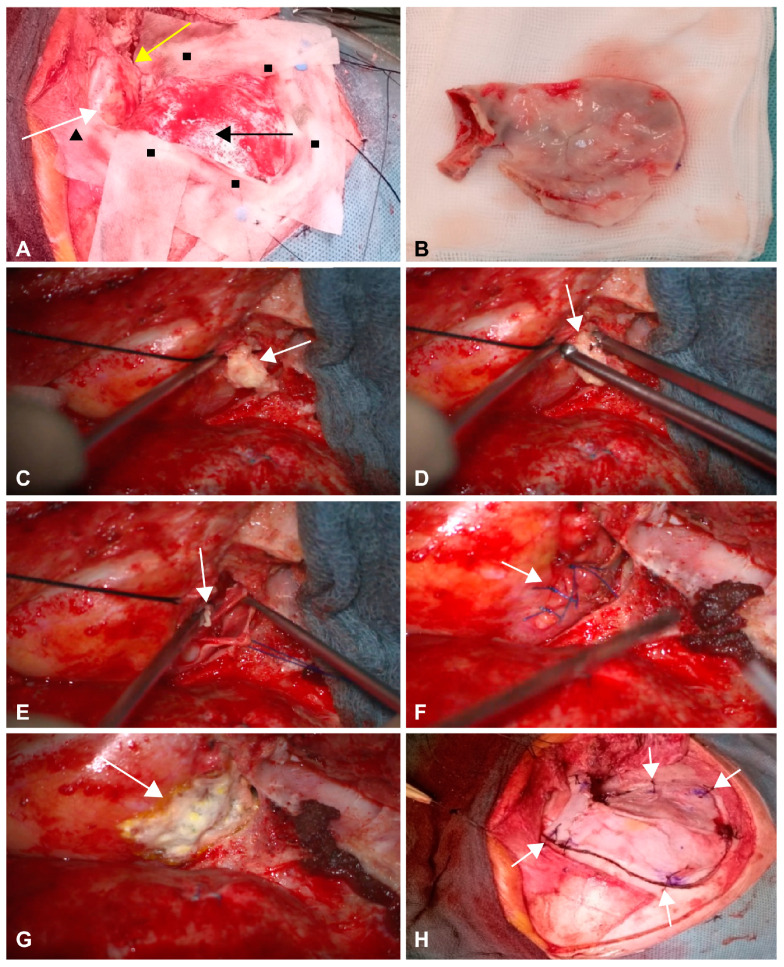 Figure 3. Intraoperative photographs from the reoperation using mOZ one-piece craniotomy. The patient is in supine position. The skull is rotated 45° to the left (A). After right-sided one-piece… Source: Modified Orbitozygomatic Craniotomy Approach for a Recurrent Orbital Tumor in a Pediatric Patient — Medicina 2024; CC BY.
Figure 3. Intraoperative photographs from the reoperation using mOZ one-piece craniotomy. The patient is in supine position. The skull is rotated 45° to the left (A). After right-sided one-piece… Source: Modified Orbitozygomatic Craniotomy Approach for a Recurrent Orbital Tumor in a Pediatric Patient — Medicina 2024; CC BY.
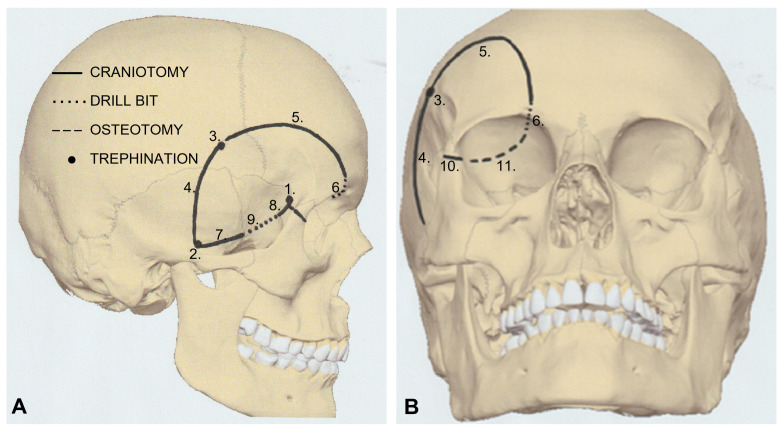 Figure 4. Bone work, which is a crucial part of the modified orbitozygomatic one-piece craniotomy, is demonstrated in the lateral (A) and anteroposterior (B) views. The trephinations corresponding… Source: Modified Orbitozygomatic Craniotomy Approach for a Recurrent Orbital Tumor in a Pediatric Patient — Medicina 2024; CC BY.
Figure 4. Bone work, which is a crucial part of the modified orbitozygomatic one-piece craniotomy, is demonstrated in the lateral (A) and anteroposterior (B) views. The trephinations corresponding… Source: Modified Orbitozygomatic Craniotomy Approach for a Recurrent Orbital Tumor in a Pediatric Patient — Medicina 2024; CC BY.
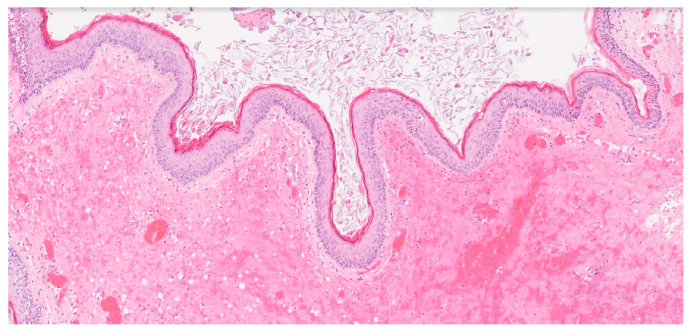 Figure 5. Histopathological examination shows a fibrous capsule lined with squamous epithelium, keratin, and inflammatory cells. No dysplastic transformation is detected. The patient was diagnosed… Source: Modified Orbitozygomatic Craniotomy Approach for a Recurrent Orbital Tumor in a Pediatric Patient — Medicina 2024; CC BY.
Figure 5. Histopathological examination shows a fibrous capsule lined with squamous epithelium, keratin, and inflammatory cells. No dysplastic transformation is detected. The patient was diagnosed… Source: Modified Orbitozygomatic Craniotomy Approach for a Recurrent Orbital Tumor in a Pediatric Patient — Medicina 2024; CC BY.
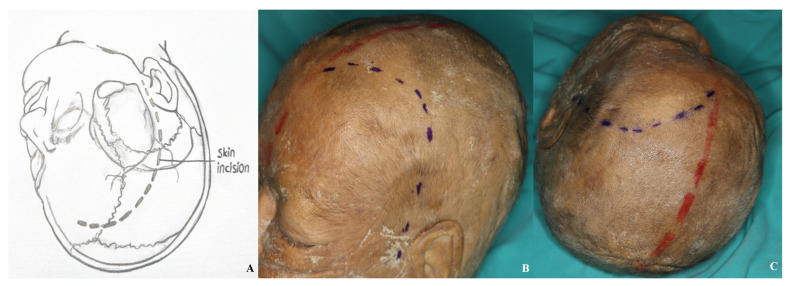 Figure 1. Incision line for pterional craniotomy with all anatomical landmarks visible [(A) demonstration, (B,C) incision view; red line: midline; blue line: incision]. Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
Figure 1. Incision line for pterional craniotomy with all anatomical landmarks visible [(A) demonstration, (B,C) incision view; red line: midline; blue line: incision]. Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
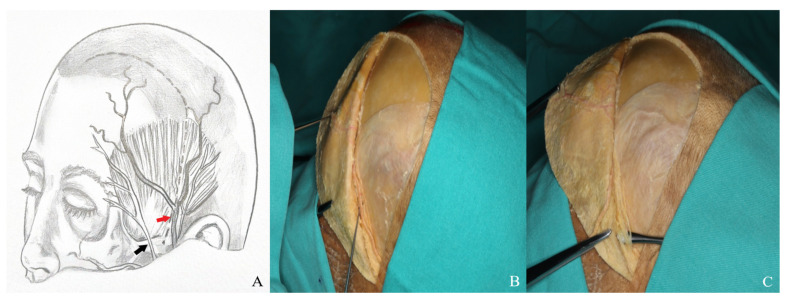 Figure 2. (A) Course of the superficial temporal artery [red arrow] and facial nerve [black arrow]. (B) The superficial temporal artery was visualized on the skin flap and elevated using a hook…. Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
Figure 2. (A) Course of the superficial temporal artery [red arrow] and facial nerve [black arrow]. (B) The superficial temporal artery was visualized on the skin flap and elevated using a hook…. Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
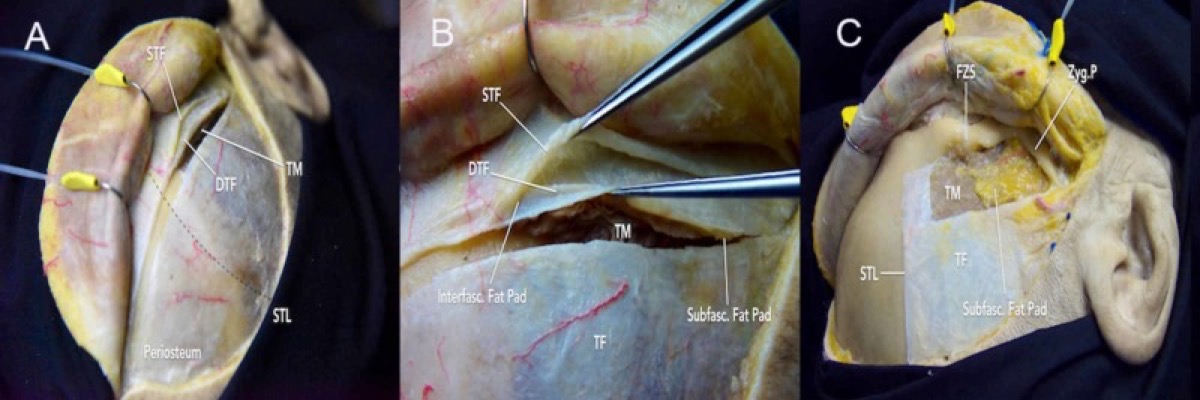
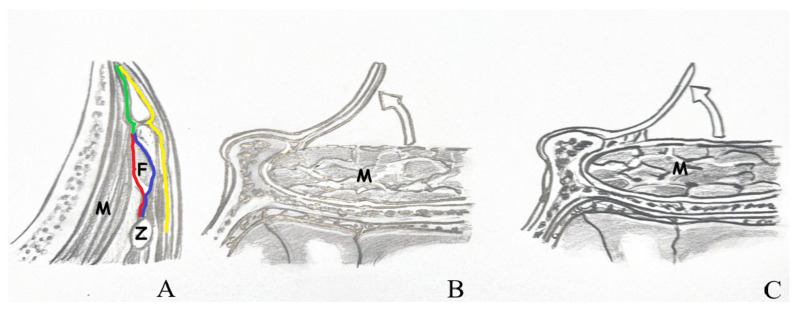 Figure 3. (A) View of the temporal muscle fascia. (B) Subfascial dissection. (C) Interfacial dissection [Z: zygomatic arch; F: fat pad; M: temporal muscle; red line: deep layer of deep temporal… Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
Figure 3. (A) View of the temporal muscle fascia. (B) Subfascial dissection. (C) Interfacial dissection [Z: zygomatic arch; F: fat pad; M: temporal muscle; red line: deep layer of deep temporal… Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
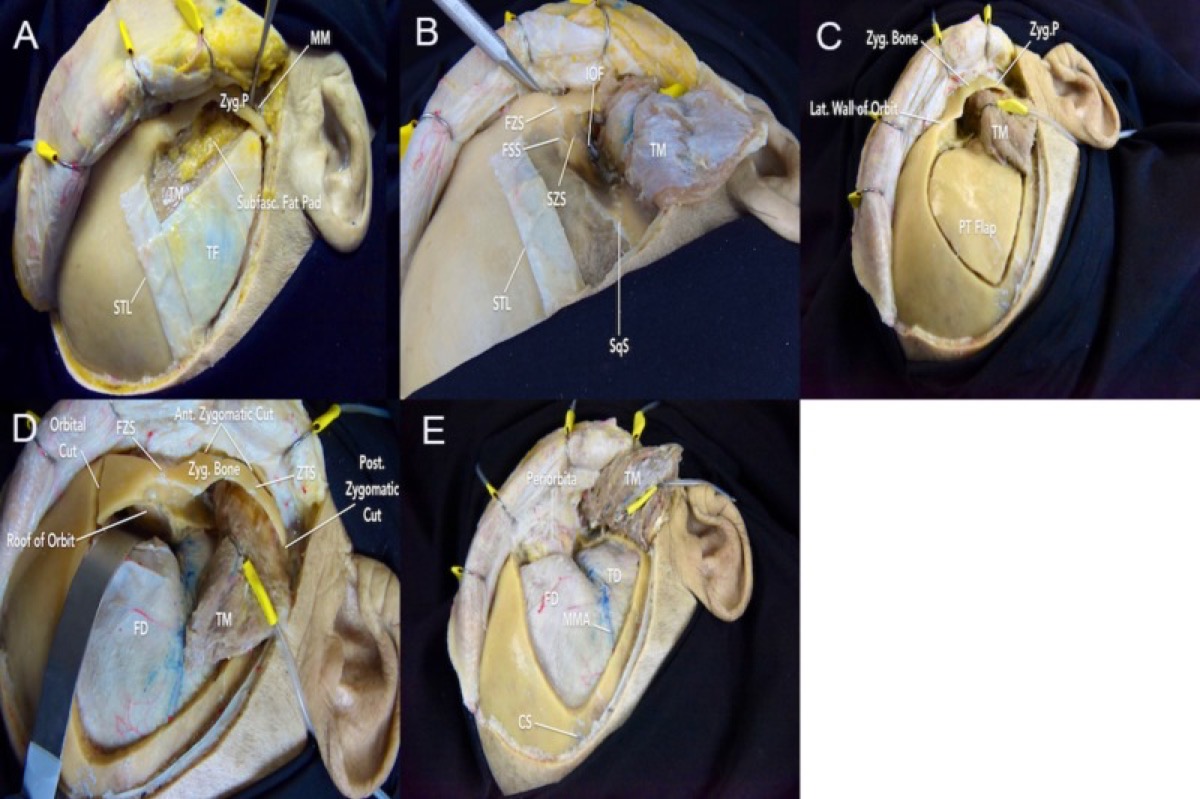
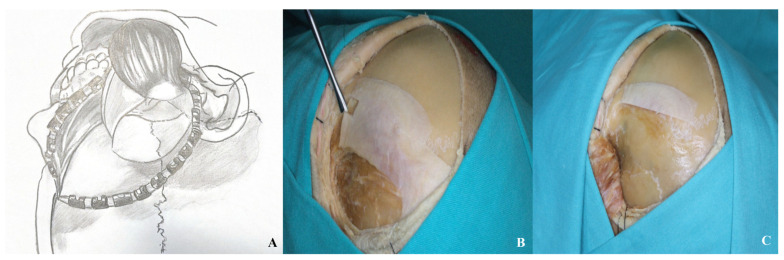 Figure 4. After initial dissection from the keyhole with a dissector, the temporalis muscle was elevated in a subperiosteal plane and retracted inferiorly [(A) demonstration, (B,C) cadaver… Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
Figure 4. After initial dissection from the keyhole with a dissector, the temporalis muscle was elevated in a subperiosteal plane and retracted inferiorly [(A) demonstration, (B,C) cadaver… Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
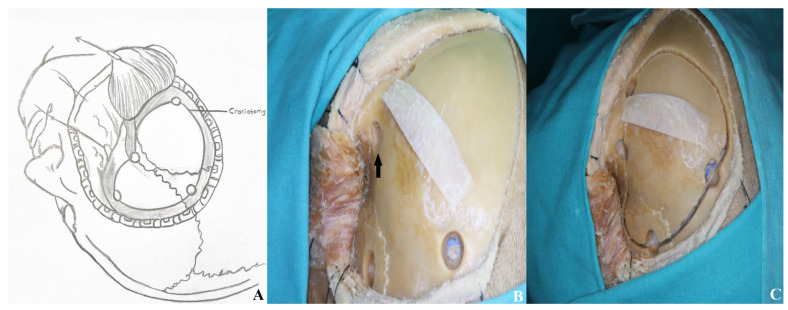 Figure 5. The initial burr hole was made at the McCarty point [black arrow], known as the “keyhole,” followed by three additional burr holes. A pterional craniotomy was then completed to elevate… Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
Figure 5. The initial burr hole was made at the McCarty point [black arrow], known as the “keyhole,” followed by three additional burr holes. A pterional craniotomy was then completed to elevate… Source: Exploring the Lamina Terminalis: A Stepwise Anatomical Comparison of Pterional and Orbitozygomatic Craniotomy Approaches — Life 2025; CC BY.
The orbitozygomatic craniotomy is the maximal anterolateral skull-base exposure — a pterional craniotomy extended by removal of the superolateral orbital rim/roof and the zygoma. By taking down the bony bar that the brain otherwise forces you to retract around, it widens the working angle and shortens the working distance to the parasellar region, anterior/posterior cavernous sinus, basilar apex, interpeduncular fossa, and upper clivus — while reducing brain retraction. It is the surgeon’s answer to deep midline and high lesions that a standard pterional reaches only with frontal/temporal lobe retraction.
General Considerations
The OZ builds on the pterional — review pterional-craniotomy.md for the shared scalp, facial-nerve-protecting fascial dissection, temporalis handling, and pterional bone flap; this chapter focuses on what the orbitozygomatic adds.
- Why remove the orbital rim/roof? It lifts the line of sight off the anterior fossa floor, eliminating the “ski-slope” of frontal-lobe retraction and adding ~20–30° of upward/subfrontal working angle toward the suprasellar and interpeduncular region.
- Why remove the zygoma? It lets the temporalis drop inferiorly, opening a flat subtemporal/transcavernous trajectory to the petroclival region and basilar apex without temporal-lobe retraction.
- Variants (know all four):
- One-piece FTOZ — pterional flap and orbitozygomatic bar removed as a single unit (fewer cuts, faster, robust reconstruction).
- Two-piece FTOZ — pterional flap first, then the orbitozygomatic bar as a separate piece (classic Zabramski/Spetzler; maximal control of the orbital cuts).
- Three-piece — adds a separate zygomatic arch segment.
- Mini-orbitozygomatic (MOz) / supraorbital-OZ keyhole — a MacCarty-keyhole craniotomy plus a limited orbital bar for selected parasellar lesions.
- When pterional suffices: an extended pterional (orbital-roof flattening + sphenoid drilling, no formal osteotomy) captures much of the benefit for many lesions with less cosmetic cost — reserve the full OZ for high/deep midline targets, large or vascular tumors invading the orbit/cavernous sinus, and low basilar apex aneurysms.
Indications
- Basilar apex / upper basilar and high-riding aneurysms; giant ICA/ophthalmic aneurysms → see basilar-tip-aneurysm.md
- Cavernous sinus, parasellar, and clinoidal meningiomas; tumors crossing orbit ↔ cranium → see sphenoid-wing-meningioma.md, tuberculum-sellae-meningioma.md
- Craniopharyngioma and large suprasellar lesions with superior/retrochiasmatic extension → see craniopharyngioma.md
- Petroclival meningioma (with subtemporal/transcavernous trajectory) → see petroclival-meningioma.md
- Orbital apex / spheno-orbital lesions requiring orbital decompression
Relevant Surgical Anatomy (OZ-specific)
- MacCarty keyhole: a single burr hole at the frontosphenoid/frontozygomatic region (junction of the frontal process of the zygoma, superior temporal line, and frontozygomatic suture) that exposes frontal dura above and periorbita below the orbital roof — the pivot point of the osteotomy.
- Superior orbital rim & roof; lateral orbital wall (greater wing of sphenoid) between the superior orbital fissure (SOF) and inferior orbital fissure (IOF). The IOF is the inferior limit of the lateral orbital wall cut and connects the orbit to the infratemporal/pterygopalatine fossa.
- Zygoma: body and arch; the frontozygomatic suture (superior) and the zygomaticomaxillary/zygomaticotemporal junctions are the osteotomy points; the masseter attaches to the arch inferiorly.
- Periorbita (periosteal sheath of orbital contents) — kept intact to avoid orbital fat herniation/enophthalmos.
- Frontotemporal (frontalis) branch of CN VII over the zygoma (protect with interfascial/subfascial dissection — see pterional chapter); supraorbital nerve/vessels at the supraorbital notch/foramen (preserve); infraorbital nerve in the floor.
Preoperative Evaluation
- Thin-cut CT (bone windows) for orbital roof/rim, frontal sinus pneumatization, and zygomatic anatomy; CTA/MRA for vascular targets; navigation dataset.
- Ophthalmology baseline (vision, fields, motility) for orbital/parasellar lesions.
- Counsel re: transient periorbital edema, ecchymosis, trismus, and temporal hollowing; rare enophthalmos/pulsatile exophthalmos if periorbita/roof reconstruction is inadequate.
Logistics, OR Setup & Orders
- OR setup: Mayfield/head holder plan, microscope/endoscope, navigation, vascular instruments/ICG when applicable, skull base reconstruction supplies, and approach-specific retractors/drills ready before opening.
- Special needs: arterial line for major intracranial or vascular cases, Foley for long cases, neuromonitoring by corridor, dexamethasone/antiepileptic/BP plan by pathology, and blood products for vascular or skull base exposure.
- Immediate postop orders: disposition and neuro-check frequency, HOB/activity, postop CT/MRI/CTA timing, BP goals, steroid/antiepileptic plan, DVT prophylaxis timing, drain management, and focused cranial nerve/visual/language/motor exams.
Anesthesia & Neuromonitoring
- GA, TIVA when MEPs used; lumbar drain for large basal lesions to aid relaxation (see pterional chapter). SSEP/MEP; EEG/burst-suppression capability for temporary clipping; cranial-nerve EMG (III/IV/VI, facial) per target. Normotension (AVM is the BP exception).
Positioning
As for the pterional, supine with the head in Mayfield fixation, but tuned for a basal trajectory:
- Rotation ~20–30° to the contralateral side (less for more midline/superior targets such as basilar apex; more for ipsilateral parasellar lesions).
- Extension until the malar eminence is the highest point so the frontal lobe and orbital contents fall away by gravity — this matters more for the OZ than the pterional because the payoff is the basal subfrontal view.
- Vertex down slightly; ipsilateral shoulder roll if needed; reconfirm IONM after positioning.
Incision & Soft-Tissue Dissection
- Curvilinear (reverse question-mark) incision behind the hairline, from the zygomatic root (~1 cm anterior to the tragus, never below the arch — facial-nerve trunk) to the contralateral mid-pupillary line.
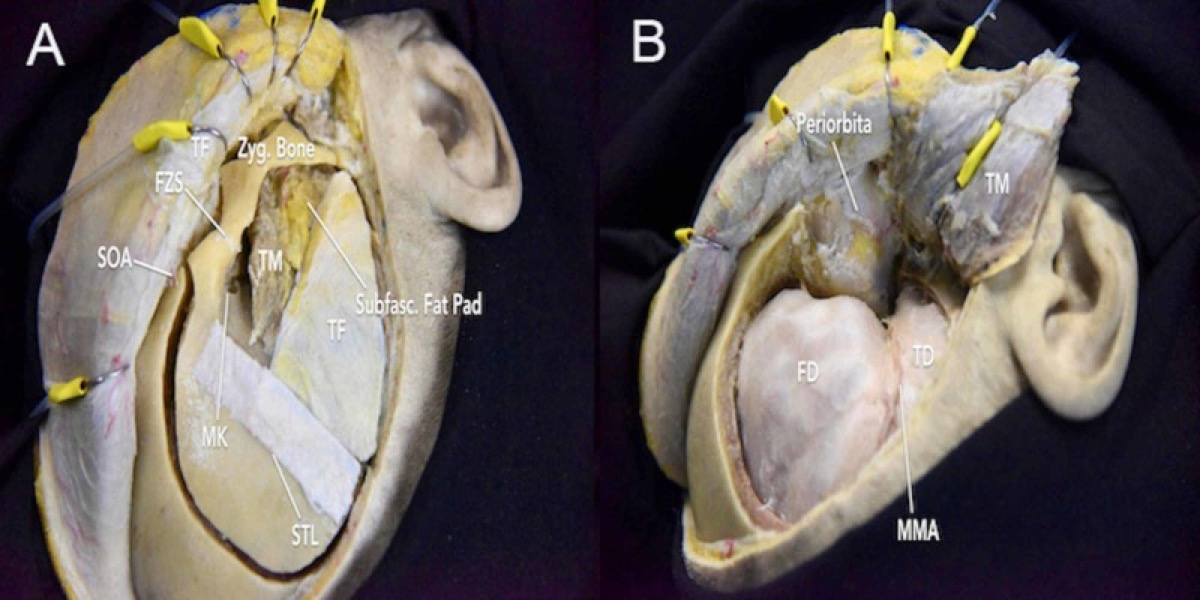
- Use an interfascial or subfascial dissection to carry the superficial temporal fat pad and the frontalis branch of CN VII down with the flap (see pterional chapter). Expose the superior and lateral orbital rim, the frontozygomatic suture, the body of the zygoma, and the zygomatic arch subperiosteally. Preserve the supraorbital nerve (release from its notch/foramen with a small osteotome if it is in a true foramen).
Rodriguez Rubio R, et al. “Immersive Surgical Anatomy of the Frontotemporal-Orbitozygomatic Approach,” Cureus 2019;11(11):e6053 — CC BY. The fat pad and facial-nerve branch are kept within the flap.
- Temporalis: reflect (interfascial cuff for reattachment, or single myocutaneous layer) and mobilize inferiorly; for the zygomatic osteotomy the muscle is retracted to expose the arch. Preserving the deep temporal pedicle limits atrophy/trismus (see pterional chapter).
Bone Work — Pterional Flap + Orbitozygomatic Osteotomy
Step 1 — Pterional craniotomy
Perform the standard pterional craniotomy and sphenoid-wing removal first (one-piece OZ keeps the flap connected to the bar; two/three-piece removes the pterional flap separately). Strip dura off the orbital roof and flatten the sphenoid ridge as in the extended pterional.
Step 2 — Expose orbit and protect periorbita
With malleable retractors, separate the periorbita from the orbital roof and lateral wall (extraperiosteal) above, and from the inferior orbital fissure below; protect the globe and periorbita throughout. The MacCarty keyhole is completed so frontal dura and periorbita are both visible.
Step 3 — The osteotomy cuts (reciprocating saw / craniotome)
The classic two-piece orbitozygomatic bar is freed by cuts that, together, isolate the orbital rim + lateral orbital wall + zygoma as one unit:
- Superior orbital rim — across the orbital roof, from the MacCarty keyhole medially toward (but sparing) the supraorbital notch.
- Lateral orbital wall — from the keyhole down the greater wing of the sphenoid to the inferior orbital fissure, protecting periorbita.
- Zygomatic body — across the frontozygomatic suture / lateral orbital rim above and the zygomatic body (toward the IOF) so the cuts connect.
- Zygomatic arch — an oblique cut through the arch (anterior to the articular eminence) so the bar, with the malar eminence, lifts free.
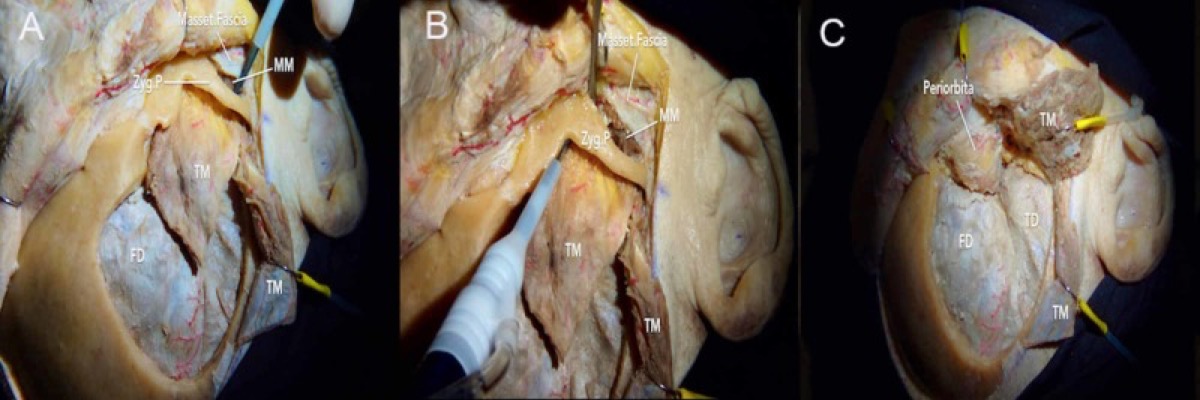
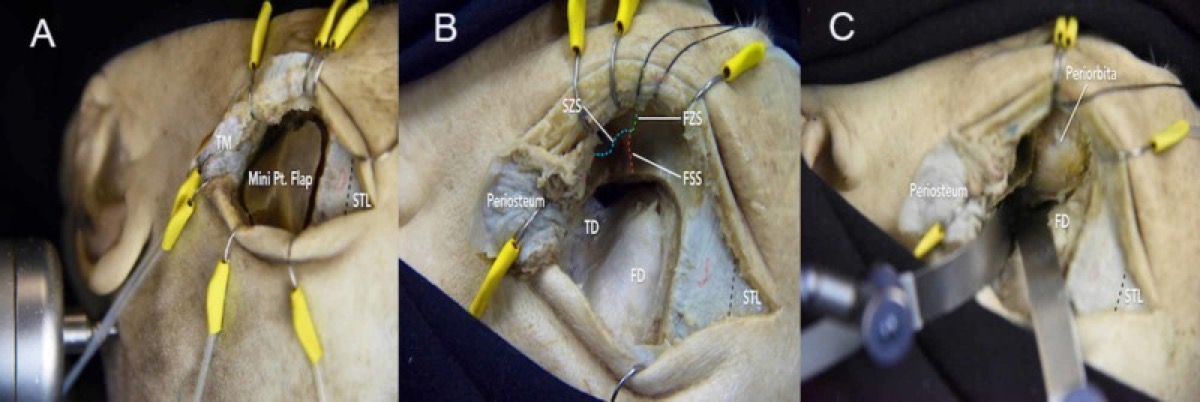
Rodriguez Rubio R, et al. Cureus 2019;11(11):e6053 — CC BY. Two-piece frontotemporal-orbitozygomatic technique.
Rodriguez Rubio R, et al. Cureus 2019;11(11):e6053 — CC BY. One-piece variant — flap and bar removed together.
Step 4 — Flatten residual bone
Drill the remaining lateral sphenoid wing, orbital roof irregularities, and the anterior clinoid (extradural anterior clinoidectomy when needed for paraclinoid/cavernous targets) until the floor is flat — this is where the OZ working angle is truly won.
Dural Opening & Intradural Work
- Open the dura curvilinearly and reflect it anteroinferiorly toward the now-flattened base; the frontal and temporal lobes fall away, exposing the basal cisterns with little or no retraction.
- Release CSF from the carotid/chiasmatic/Sylvian cisterns; split the Sylvian fissure as needed. The expanded corridor supports subfrontal, trans-Sylvian, subtemporal, and transcavernous trajectories — proceed to the pathology-specific intradural steps (basilar apex clipping, cavernous/parasellar tumor, craniopharyngioma via the opticocarotid/lamina terminalis windows).
Closure & Reconstruction
- Watertight dura (graft any defect; especially if the SOF/orbit or ventricle was entered). Reconstruct the orbital roof if removed (the periorbita must be supported to prevent pulsatile exophthalmos/enophthalmos) — bone, mesh, or graft.
- Replace the orbitozygomatic bar and pterional flap with low-profile titanium plates; precise anatomic reduction of the orbital rim and zygomatic arch is essential for cosmesis (malar projection, no step-off). Burr-hole covers/cranioplasty for contour.
- Obliterate/patch the frontal sinus with pericranium if entered. Reattach temporalis to its cuff anatomically; suspend to limit hollowing. Layered scalp closure; periorbital pressure dressing reduces edema.
Further operative anatomy & technique
Rodriguez Rubio R et al., Cureus 2019;11(11):e6053 — CC BY.
Rodriguez Rubio R et al., Cureus 2019;11(11):e6053 — CC BY.
Nuances & Pitfalls (surgeon-level)
- Protect the periorbita — a tear lets orbital fat herniate into the field and predisposes to enophthalmos; repair and support the roof at closure.
- Reconstruct the orbital rim/roof precisely — the two feared cosmetic/functional sequelae are temporal hollowing (temporalis handling) and enophthalmos/pulsatile exophthalmos (roof/periorbita).
- Spare the supraorbital nerve (forehead numbness) — release it from its notch/foramen rather than transecting.
- Mind the frontal sinus medially (navigation; exenterate + pericranial buttress if entered) and the IOF inferiorly (venous/maxillary branches — pack/wax).
- Don’t over-build the approach. Decide preoperatively whether an extended pterional suffices; the OZ’s morbidity is mostly cosmetic and is justified only when the working angle is genuinely needed.
- Facial-nerve frontal branch — same rules as pterional: interfascial/subfascial flap, never skeletonize the nerve.
- Temporalis — preserve the deep pedicle and reattach anatomically to limit trismus/atrophy.
Complications
Frontalis (CN VII) palsy; temporal hollowing/atrophy, trismus; enophthalmos / pulsatile exophthalmos / diplopia; periorbital edema and ecchymosis; supraorbital hypesthesia; CSF leak / frontal-sinus mucocele; cosmetic step-off (rim/arch malreduction); vascular and cranial-nerve injury from the deep work; infection.
Cross-links
- Builds on: pterional-craniotomy.md · related: subtemporal-craniotomy.md · supraorbital-keyhole-craniotomy.md
- Pathology: basilar-tip-aneurysm.md · sphenoid-wing-meningioma.md · tuberculum-sellae-meningioma.md · craniopharyngioma.md · petroclival-meningioma.md
Figure Use & Attribution
About the figures. Copyrighted operative figures/videos are linked (Neurosurgical Atlas); embedded images are public-domain (Gray’s Anatomy) or CC‑BY (open-access cadaveric anatomy), credited beneath each image. See media-sources.md and figures/CREDITS.md.
Atlas chapters & video: Orbitozygomatic Craniotomy — Neurosurgical Atlas · Orbitozygomatic Osteotomy: Bone Work (Case) · Orbitozygomatic Operative Neuroanatomy
Chief-Level Corridor Review
Use these as the senior-level mental model for Orbitozygomatic (Frontotemporal-Orbitozygomatic, FTOZ) Craniotomy:
- Decision point: Define the exposure goal before incision: target, working angles, proximal/distal control, and the structure that cannot tolerate retraction.
- Technical lever: Know the first irreversible step: bone removal, dural opening, vascular control, or muscle/fascial division that commits the corridor.
- Bailout: Verbalize the bailout: extend exposure, change trajectory, add CSF drainage, obtain proximal control, convert to a larger corridor, or stop for imaging.
- Postop watch: Protect closure from the start: vascularized tissue, watertight dural/reconstruction plan, dead-space control, and drain strategy should be chosen before the final intradural step.
Common Pimp Questions
Use these to pressure-test preparation for Orbitozygomatic (Frontotemporal-Orbitozygomatic, FTOZ) Craniotomy:
- What patient position and head rotation make gravity work for this corridor?
- What named nerve, vessel, sinus, or muscle/fascial plane is most commonly injured?
- What bone work or soft-tissue step creates the exposure rather than simply using more retraction?
- What is the bailout if exposure is inadequate, bleeding occurs, or the brain is tight?
- What closure maneuver prevents the signature complication of this approach?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Exact head rotation/flexion/extension and pin placement: [attending-specific]
- Skin incision length, flap type, and muscle/fascial preservation technique: [attending-specific]
- Drill, rongeur, endoscope, microscope, retractor, and navigation preferences: [attending-specific]
- Drain use, closure materials, watertightness threshold, and postop imaging routine: [attending-specific]
Case Guides Using This Approach
References
- Zabramski JM, Kiriş T, Sankhla SK, Cabiol J, Spetzler RF. Orbitozygomatic craniotomy. Technical note. J Neurosurg. 1998;89(2):336–341.
- Lemole GM Jr, Henn JS, Zabramski JM, Spetzler RF. Modifications to the orbitozygomatic approach. J Neurosurg. 2003;99(5):924–930.
- Shimizu S, Tanriover N, Rhoton AL Jr, Yoshioka N, Fujii K. MacCarty keyhole and inferior orbital fissure in orbitozygomatic craniotomy. Neurosurgery. 2005;57(1 Suppl):152–159.
- Rodriguez Rubio R, et al. Immersive Surgical Anatomy of the Frontotemporal-Orbitozygomatic Approach. Cureus. 2019;11(11):e6053. CC BY. PMC6945284
- Tanriover N, Rhoton AL Jr, et al. Microsurgical anatomy of the orbitozygomatic region.
- Cohen-Gadol AA. Orbitozygomatic Craniotomy. The Neurosurgical Atlas. link