
Case Prep: Craniopharyngioma Resection
Case / Approach Snapshot
- Anatomy at risk: tumor compartment, arterial supply, venous drainage/sinuses, cranial nerves, white-matter tracts, pituitary/CSF pathways when relevant, and functional cortex.
- Operative steps: review imaging and goals, choose exposure, obtain brain relaxation, devascularize when possible, debulk internally, dissect capsule from critical structures, verify extent/safety, and reconstruct watertight closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: venous or arterial injury, swelling, seizure, cranial nerve or endocrine change, CSF leak, residual tumor left for safety, staged surgery, radiation, or adjuvant therapy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [adamantinomatous / papillary] craniopharyngioma ([sellar/suprasellar/third ventricular]) presenting with [visual loss / endocrinopathy / hydrocephalus] planned for [endoscopic endonasal / pterional / transcallosal] resection.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
CNS Video Library
🧭 Operative approach: Supraorbital keyhole craniotomy — detailed corridor setup, step-by-step technique & figures
Operative figures/atlases are © (linked, not copied). See media-sources.md.
- Technique/approach: The Neurosurgical Atlas — search “craniopharyngioma”
- Imaging: Radiopaedia — craniopharyngioma
- Open-access figures: PubMed Central
High-Yield Literature
- Craniopharyngioma surgery — Honegger J. Pituitary 2008. PubMed
- Craniopharyngioma — Boop FA. Journal of neurosurgery 2007. PubMed
- Precision Oncology for Papillary Craniopharyngioma — Blakeley JO. The New England journal of medicine 2023. PubMed
- Pediatric craniopharyngioma — Drapeau A. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2019. PubMed
- The craniopharyngioma — Oskouian RJ. Frontiers of hormone research 2006. PubMed
- Craniopharyngioma — Till K. Child’s brain 1982. PubMed
- Advances in the management of craniopharyngioma in children and adults — Jensterle M. Radiology and oncology 2019. PubMed
- [Craniopharyngioma] — Yamada S. Nihon rinsho. Japanese journal of clinical medicine 2006. PubMed
- [Craniopharyngioma] — Bingas B. Fortschritte der Neurologie, Psychiatrie, und ihrer Grenzgebiete 1968. PubMed
- [Craniopharyngioma] — Maruno M. Nihon rinsho. Japanese journal of clinical medicine 2005. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
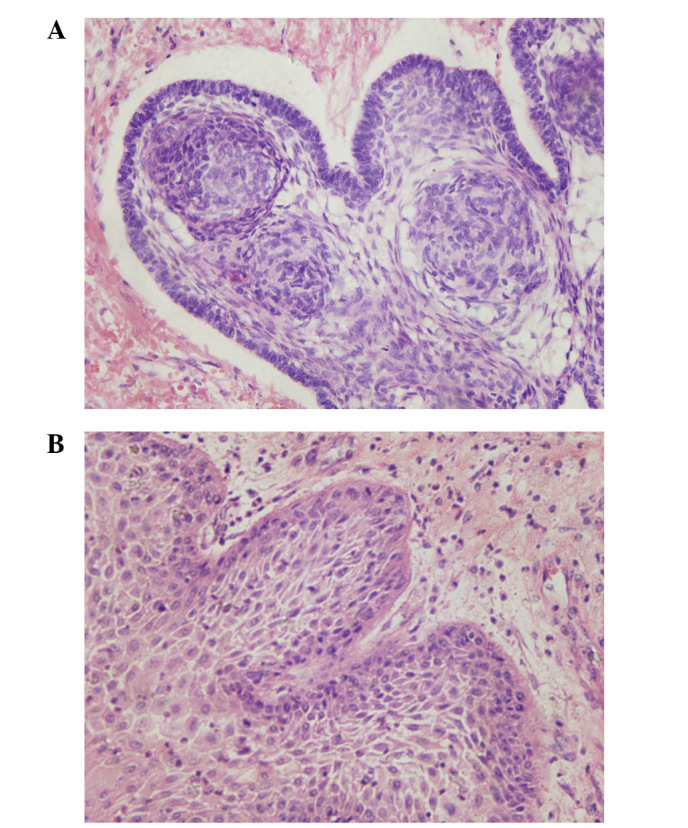 Figure 1. (A) Adamantinomatous and (B) squamous-papillary craniopharyngioma section images captured using light microscopy (stain, hematoxylin and eosin; magnification, ×400). Source: Craniopharyngioma: Survivin expression and ultrastructure — Oncology Letters 2015; CC BY.
Figure 1. (A) Adamantinomatous and (B) squamous-papillary craniopharyngioma section images captured using light microscopy (stain, hematoxylin and eosin; magnification, ×400). Source: Craniopharyngioma: Survivin expression and ultrastructure — Oncology Letters 2015; CC BY.
History of Present Illness
- Chief complaint: Visual decline, endocrine dysfunction (growth failure in children, hypogonadism/DI/hypopituitarism in adults), headache, hydrocephalus
- Bimodal age: children (adamantinomatous) and adults (papillary)
- Hypothalamic symptoms: obesity, temperature/sleep dysregulation, behavioral
Imaging Review
MRI (T1±Gad, T2, sella protocol)
- Location: sellar, suprasellar, retrochiasmatic, third ventricle
- Cystic (machinery oil fluid) + solid + calcification (adamantinomatous); papillary often solid
- Optic chiasm/nerve relationship (pre/post-fixed)
- Hypothalamic involvement (CRITICAL — predicts morbidity; Puget grade 0-2)
- ICA, ACA, stalk, third ventricle, hydrocephalus
CT
- Calcification (adamantinomatous hallmark), sellar anatomy, sphenoid pneumatization (endonasal)
Endocrine + Ophthalmology
- Full pituitary panel, AM cortisol, DI assessment (Na, urine osm), visual fields/acuity
Labs
- CBC, BMP (Na baseline), Coags, full endocrine panel, AM cortisol (stress-dose if deficient), Type and screen
Neurological Examination
- Vision, endocrine, hypothalamic function, cognition
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: navigation, endoscope/microscope as approach requires, ENT co-surgeon for endonasal cases, Doppler, lumbar drain only when indicated, reconstruction materials, and visual/endocrine baseline available.
- Special needs: steroid strategy individualized (Cushing workup may require avoiding preop steroids), DI/sodium protocol, AM cortisol/endocrine labs, visual-check plan, arterial line for large/vascular cases, and CSF-leak/nasal precautions.
- Immediate postop orders: neuro and visual checks, strict I/O with sodium/urine specific gravity schedule when pituitary stalk risk exists, cortisol/endocrine replacement plan, nasal precautions, MRI/CT timing, steroid taper, and DVT prophylaxis timing.
Approach Selection
- Endoscopic endonasal extended transsphenoidal: Favored for midline retrochiasmatic/infrachiasmatic tumors — direct access, superior visual outcomes, but CSF leak risk; needs nasoseptal flap
- Pterional/orbitozygomatic: Lateral suprasellar extension, vessel encasement
- Transcallosal/transcortical-transventricular: Predominantly third-ventricular tumors
- Goal debate: Gross total resection (cure but hypothalamic morbidity risk) vs planned subtotal + radiation (function preservation) — especially if hypothalamic involvement
Position
- Endonasal: supine, slight extension, navigation, possible lumbar drain
- Transcranial: per approach
Key Surgical Steps (Endoscopic Endonasal Extended)
- Nasal phase, nasoseptal flap, wide sphenoidotomy, posterior ethmoidectomy
- Remove tuberculum/planum bone (transtuberculum-transplanum), expose suprasellar dura
- Open dura above and below superior intercavernous sinus (ligate)
- Identify chiasm, stalk, superior hypophyseal arteries, ICAs
- Cyst drainage, debulk solid tumor, peel capsule off chiasm/hypothalamus/vessels
- Hypothalamic adherence — judgment point: leave residual on hypothalamus rather than cause injury
- Preserve stalk if possible (often sacrificed → panhypopituitarism/DI)
- Multilayer skull base reconstruction (fascia/collagen inlay + nasoseptal flap + sealant) — high CSF leak risk
Critical Anatomy & Structures at Risk
- Hypothalamus — adherence; injury → obesity, memory, temperature, electrolyte, behavioral devastation
- Optic chiasm/nerves and superior hypophyseal arteries (visual outcome)
- Pituitary stalk/gland — endocrine outcome (DI nearly universal if sacrificed)
- ICA, ACA, perforators
- Third ventricle/foramen of Monro
Equipment
- Endoscope/microscope, navigation, drill, CUSA, ICG
- Nasoseptal flap, fascia lata/fat graft, dural substitute, sealant, lumbar drain
Monitoring
- SSEPs; VEPs (optional)
Anesthesia
- Arterial line, Foley (strict I/O for DI), stress-dose steroids if adrenal insufficient, careful Na management
Potential Complications
- Diabetes insipidus (often permanent) + triphasic response
- Hypothalamic obesity/dysfunction, panhypopituitarism
- CSF leak (endonasal), visual change, vascular injury
- Recurrence (high; long-term surveillance)
Operative Note Template
Preoperative Diagnosis: [Adamantinomatous/papillary] craniopharyngioma ([sellar/suprasellar/third-ventricular]) with [visual loss/endocrinopathy/hydrocephalus]
Postoperative Diagnosis: Same
Procedure: [Endoscopic endonasal extended transsphenoidal / pterional] resection of craniopharyngioma [with nasoseptal flap reconstruction]
Surgeon / Assistant: [± ENT co-surgeon] Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Neuronavigation, endoscope/microscope, ICG, micro-Doppler; strict I/O (DI), lumbar drain Implants: Fascia/fat graft, nasoseptal flap, dural sealant Complications: None
Indications: [Age]yo [M/F] with a craniopharyngioma causing [progressive visual loss/endocrine dysfunction/hydrocephalus]. Approach chosen for [midline retrochiasmatic extent → endonasal / lateral or vascular extension → transcranial]. Risks (DI, hypopituitarism, hypothalamic injury, CSF leak, visual change) discussed; stress-dose steroids given.
Description of Procedure: After consent and time-out, general anesthesia was induced with a Foley for strict I/O and stress-dose steroids, and navigation registered. [Endonasal: a nasoseptal flap was raised, wide sphenoidotomy and posterior ethmoidectomy performed, and the tuberculum/planum removed to expose the suprasellar dura, which was opened after ligating the superior intercavernous sinus.] The chiasm, stalk, superior hypophyseal arteries, and ICAs were identified.
The cyst was drained and the solid tumor debulked; the capsule was carefully peeled off the optic apparatus, hypothalamus, and vessels, preserving the superior hypophyseal artery branches to the chiasm. Where tumor was densely adherent to the hypothalamus, residual was left rather than risk injury. [The stalk was preserved / sacrificed.] [Endonasal: a multilayer skull base reconstruction was performed with fascia/fat inlay, the vascularized nasoseptal flap, and sealant.]
Closure was completed and the patient transferred to the ICU with intensive DI/sodium monitoring.
Postoperative Plan
- ICU, neuro checks q1h
- Intensive DI/Na management — strict I/O, q4-6h Na, DDAVP protocol, triphasic vigilance
- AM cortisol / stress-dose steroids, full endocrine replacement, endocrine consult
- CSF leak precautions, lumbar drain management
- MRI postop, ophthalmology, visual fields
- Residual → radiation/proton therapy planning; long-term surveillance
- Hypothalamic dysfunction monitoring (weight, behavior)
Chief-Level Case Review
Use these as the senior-level mental model for Craniopharyngioma Resection:
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Craniopharyngioma Resection:
- What is the surgical goal: gross-total, maximal safe, decompression, diagnosis, or cytoreduction?
- What eloquent cortex, tract, cranial nerve, vessel, or sinus defines the stopping point?
- What adjunct changes the case: navigation, mapping, 5-ALA, ultrasound, endoscope, ICG, or neuromonitoring?
- What is the edema, steroid, seizure, DVT, and postop imaging plan?
- What complication would you check for first in PACU based on this lesion location?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Extent-of-resection goal and functional stopping points: [attending-specific]
- Mapping/monitoring, 5-ALA, ultrasound, ICG, endoscope, or tractography preferences: [attending-specific]
- Steroid, antiepileptic, mannitol/hypertonic saline, and antibiotic plan: [attending-specific]
- Postop MRI timing, ICU/floor threshold, and adjuvant-referral workflow: [attending-specific]