
Approach: Pterional (Frontotemporal) Craniotomy
Case / Approach Snapshot
- Anatomy at risk: corridor-defining nerves, arteries, veins/sinuses, cisterns, bone landmarks, muscle/fascial planes, and closure structures that determine exposure and morbidity.
- Operative steps: confirm position and trajectory, mark landmarks, protect soft tissue and named neurovascular structures, perform the bone/soft-tissue corridor, open/close dura or target compartment deliberately, and verify hemostasis/reconstruction; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: brain relaxation failure, venous or sinus bleeding, cranial nerve/perforator risk, exposure that is too narrow, CSF leak, cosmetic/temporalis/frontalis problems, and conversion to a wider or alternate corridor.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
High-Yield Literature
- Anterior interhemispheric vs. pterional approach in the microsurgical management of anterior communicating artery aneurysms: a comparative analysis employing a novel multidimensional matching-tool — Swiatek VM. Neurosurgical review 2024. PubMed
- Temporalis Muscle Dissection Techniques in the Pterional Approach: Quantitative Impact on Operative Corridor and Surgical Freedom — Hasimoglu S. World neurosurgery 2026. PubMed
- Tuberculum sellae meningiomas: microsurgical anatomy and surgical technique — Jallo GI. Neurosurgery 2002. PubMed
- Cranio-Orbito-Zygomatic Approach: Core Techniques for Tailoring Target Exposure and Surgical Freedom — Luzzi S. Brain sciences 2022. PubMed
- The pterional approach for the microsurgical removal of olfactory groove meningiomas — Turazzi S. Neurosurgery 1999. PubMed
- Microsurgical Anatomy of the Interfascial Vein. Its Significance in the Interfascial Dissection of the Pterional Approach — Campero A. Operative neurosurgery (Hagerstown, Md.) 2017. PubMed
- Lipotranferences in post neurosurgical esthetic defects — Demichelis MDRE. Surgical neurology international 2023. PubMed
- Minimally invasive approaches to aneurysms of the anterior circulation: selection criteria and clinical outcomes — Gandhi S. Journal of neurosurgical sciences 2018. PubMed
- Applying objective metrics to neurosurgical skill development with simulation and spaced repetition learning — Robertson FC. Journal of neurosurgery 2023. PubMed
- Diagnosis and surgical treatment of cavernous sinus hemangiomas: an experience of 20 cases — Zhou LF. Surgical neurology 2003. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
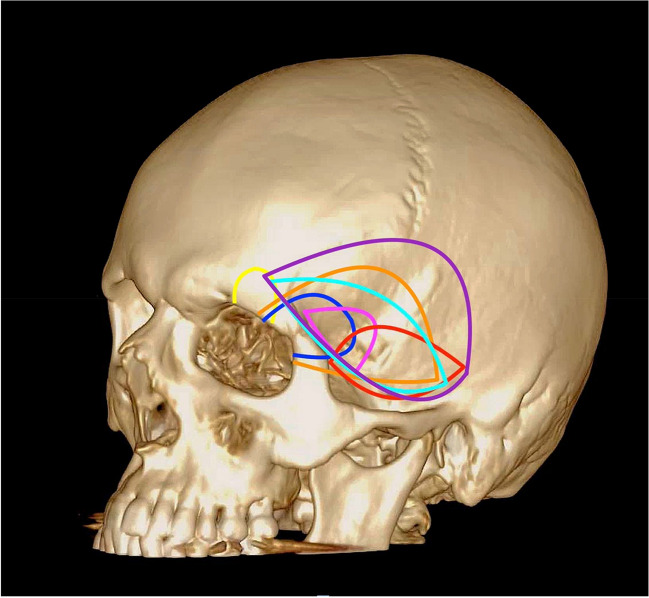 Fig. 2. Schematic illustration demonstrating the anatomical locations of the described craniotomies. Each coloured line represents a different anatomical location for the reviewed craniotomies:… Source: ‘What’s in a name’, a systematic review of the pterional craniotomy for aneurysm surgery and its many modifications with a proposal for simplified nomenclature — Acta Neurochirurgica 2024; CC BY.
Fig. 2. Schematic illustration demonstrating the anatomical locations of the described craniotomies. Each coloured line represents a different anatomical location for the reviewed craniotomies:… Source: ‘What’s in a name’, a systematic review of the pterional craniotomy for aneurysm surgery and its many modifications with a proposal for simplified nomenclature — Acta Neurochirurgica 2024; CC BY.
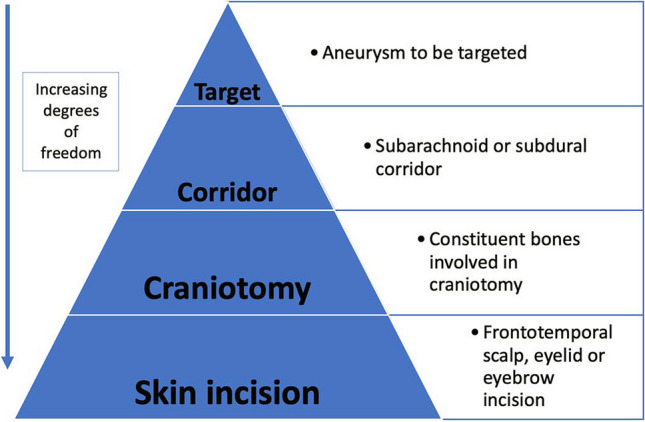 Fig. 3. Proposal of how to apply the ‘inside-out’ concept for aneurysm surgery and a way to simplify the approach related nomenclature Source: ‘What’s in a name’, a systematic review of the pterional craniotomy for aneurysm surgery and its many modifications with a proposal for simplified nomenclature — Acta Neurochirurgica 2024; CC BY.
Fig. 3. Proposal of how to apply the ‘inside-out’ concept for aneurysm surgery and a way to simplify the approach related nomenclature Source: ‘What’s in a name’, a systematic review of the pterional craniotomy for aneurysm surgery and its many modifications with a proposal for simplified nomenclature — Acta Neurochirurgica 2024; CC BY.
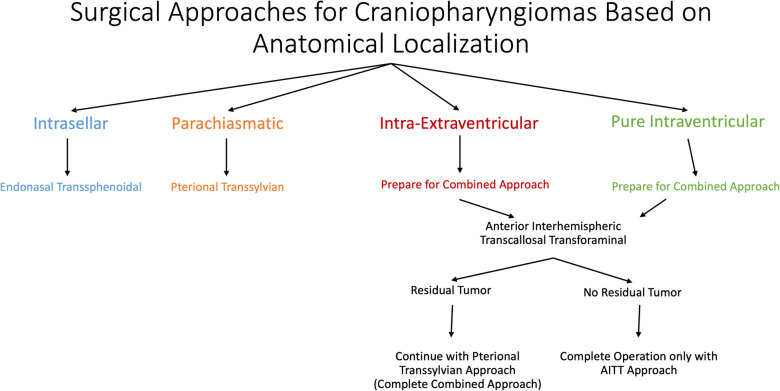 Fig. 2. Surgical approaches for craniopharyngiomas based on anatomical localization. The endonasal transsphenoidal approach was preferred for intrasellar tumors. For parachiasmatic tumors, the… Source: Revisiting the combined approach of Yaşargil for microsurgical removal of intra-extraventricular and pure intraventricular craniopharyngiomas — Acta Neurochirurgica 2025; CC BY.
Fig. 2. Surgical approaches for craniopharyngiomas based on anatomical localization. The endonasal transsphenoidal approach was preferred for intrasellar tumors. For parachiasmatic tumors, the… Source: Revisiting the combined approach of Yaşargil for microsurgical removal of intra-extraventricular and pure intraventricular craniopharyngiomas — Acta Neurochirurgica 2025; CC BY.
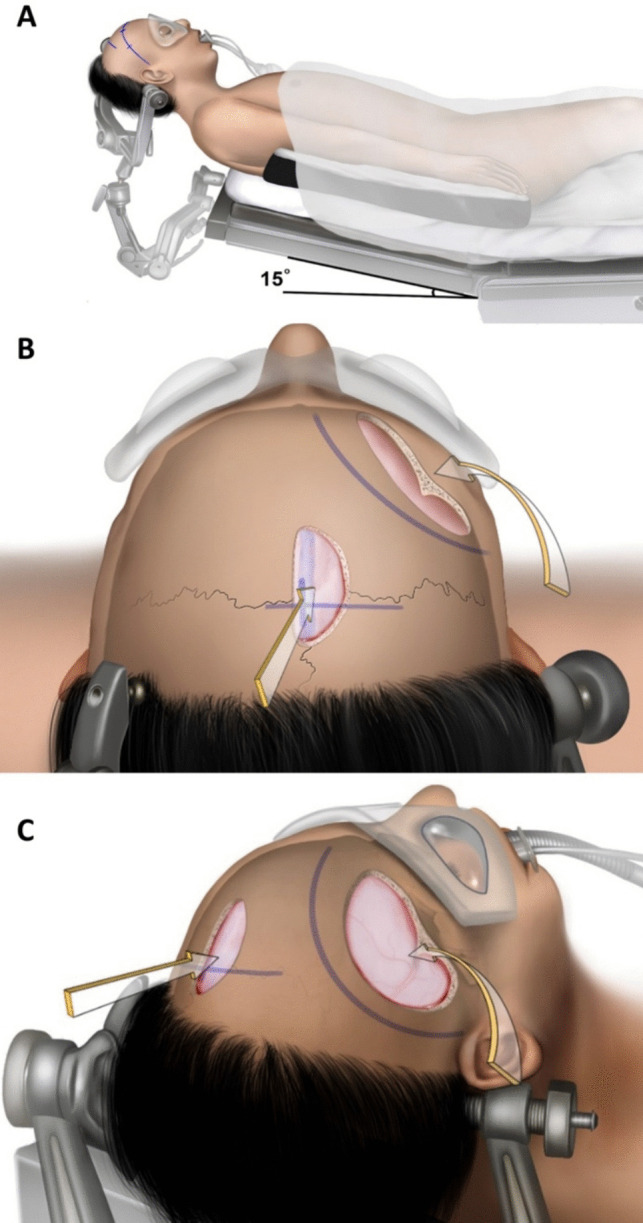 Fig. 3. Surgical position and skin incisions. A First, for the interhemispheric approach, the head is fixed in the supine position with neutral, slight flexion. B After a linear skin incision is… Source: Revisiting the combined approach of Yaşargil for microsurgical removal of intra-extraventricular and pure intraventricular craniopharyngiomas — Acta Neurochirurgica 2025; CC BY.
Fig. 3. Surgical position and skin incisions. A First, for the interhemispheric approach, the head is fixed in the supine position with neutral, slight flexion. B After a linear skin incision is… Source: Revisiting the combined approach of Yaşargil for microsurgical removal of intra-extraventricular and pure intraventricular craniopharyngiomas — Acta Neurochirurgica 2025; CC BY.
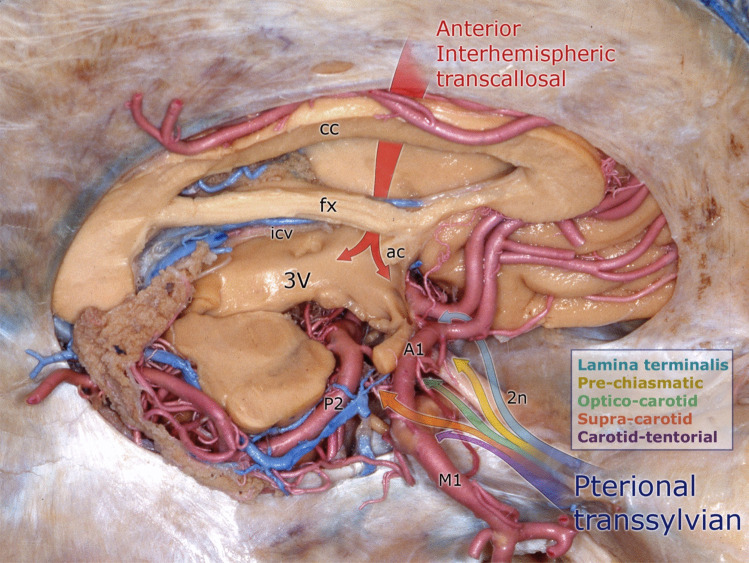 Fig. 4. Demonstration of the combined approach on an anatomical specimen. Red arrow: interhemispheric transcallosal route. The multicolor arrow indicates the pterional transsylvian route with… Source: Revisiting the combined approach of Yaşargil for microsurgical removal of intra-extraventricular and pure intraventricular craniopharyngiomas — Acta Neurochirurgica 2025; CC BY.
Fig. 4. Demonstration of the combined approach on an anatomical specimen. Red arrow: interhemispheric transcallosal route. The multicolor arrow indicates the pterional transsylvian route with… Source: Revisiting the combined approach of Yaşargil for microsurgical removal of intra-extraventricular and pure intraventricular craniopharyngiomas — Acta Neurochirurgica 2025; CC BY.
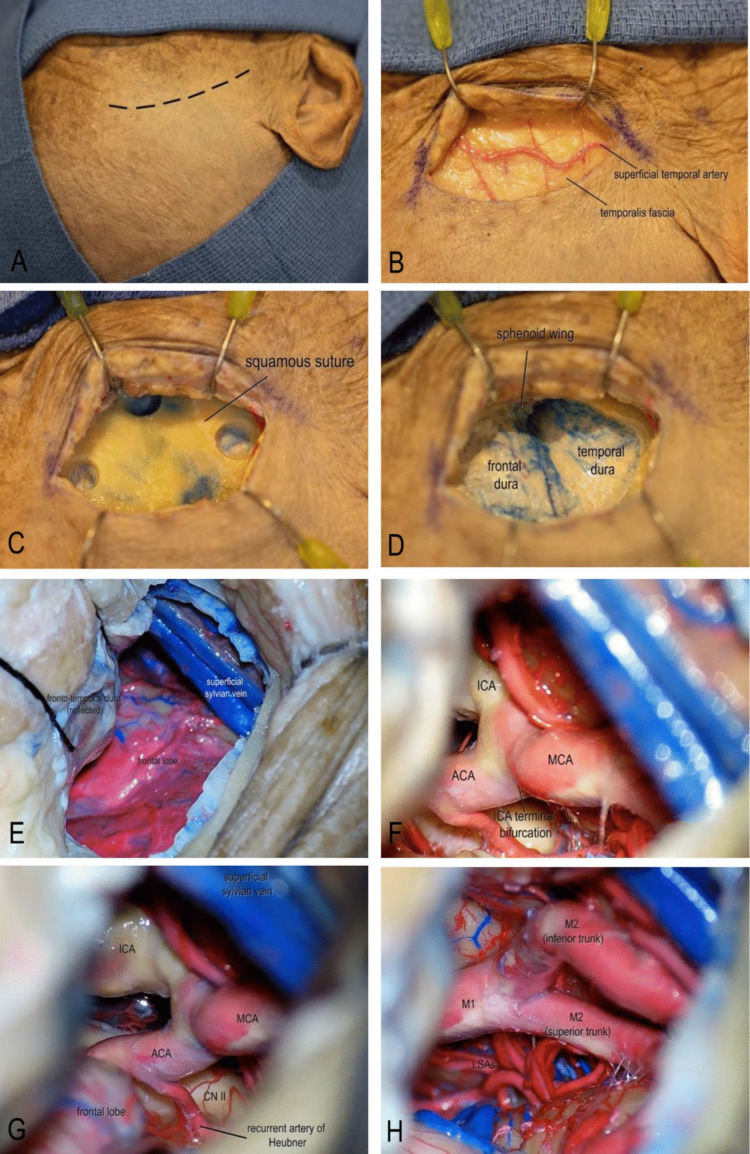 Fig. 1. Step-by-step illustration of the standardized mini-pterional approach. A A curvilinear frontotemporal skin incision centered over the pterion was made. B After skin incision, the… Source: Microscopic transorbital vs mini-pterional approach to MCA bifurcation aneurysms: a quantitative cadaveric comparative study with surgical implications — Acta Neurochirurgica 2026; CC BY.
Fig. 1. Step-by-step illustration of the standardized mini-pterional approach. A A curvilinear frontotemporal skin incision centered over the pterion was made. B After skin incision, the… Source: Microscopic transorbital vs mini-pterional approach to MCA bifurcation aneurysms: a quantitative cadaveric comparative study with surgical implications — Acta Neurochirurgica 2026; CC BY.
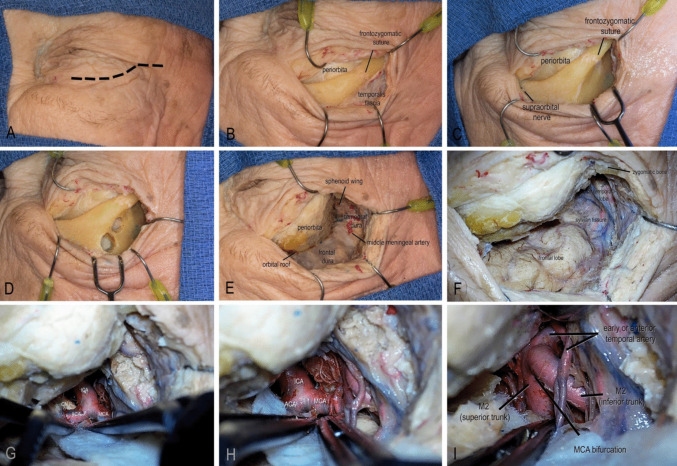 Fig. 2. Step-by-step illustration of the eyelid transorbital approach. A The incision was planned along the natural eyelid crease, extending laterally from the medial limbus to the lateral… Source: Microscopic transorbital vs mini-pterional approach to MCA bifurcation aneurysms: a quantitative cadaveric comparative study with surgical implications — Acta Neurochirurgica 2026; CC BY.
Fig. 2. Step-by-step illustration of the eyelid transorbital approach. A The incision was planned along the natural eyelid crease, extending laterally from the medial limbus to the lateral… Source: Microscopic transorbital vs mini-pterional approach to MCA bifurcation aneurysms: a quantitative cadaveric comparative study with surgical implications — Acta Neurochirurgica 2026; CC BY.
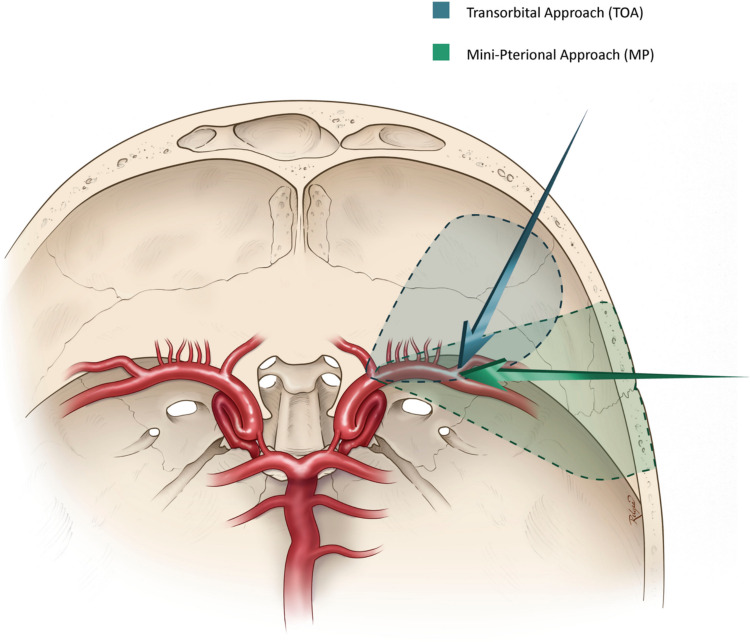 Fig. 3. Axial illustration demonstrating the MP and TOA approaches and their respective angles to the MCA bifurcation Source: Microscopic transorbital vs mini-pterional approach to MCA bifurcation aneurysms: a quantitative cadaveric comparative study with surgical implications — Acta Neurochirurgica 2026; CC BY.
Fig. 3. Axial illustration demonstrating the MP and TOA approaches and their respective angles to the MCA bifurcation Source: Microscopic transorbital vs mini-pterional approach to MCA bifurcation aneurysms: a quantitative cadaveric comparative study with surgical implications — Acta Neurochirurgica 2026; CC BY.
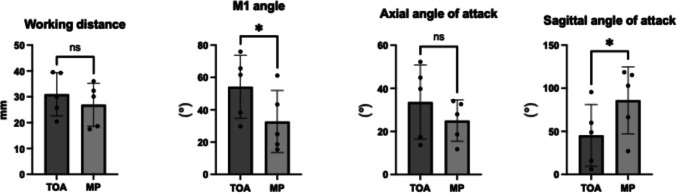 Fig. 4. Quantitative analysis represented as bar charts. * Indicates statistically significant difference, p < 0.005. (TOA = transorbital approach, MP = mini-pterional approach) Source: Microscopic transorbital vs mini-pterional approach to MCA bifurcation aneurysms: a quantitative cadaveric comparative study with surgical implications — Acta Neurochirurgica 2026; CC BY.
Fig. 4. Quantitative analysis represented as bar charts. * Indicates statistically significant difference, p < 0.005. (TOA = transorbital approach, MP = mini-pterional approach) Source: Microscopic transorbital vs mini-pterional approach to MCA bifurcation aneurysms: a quantitative cadaveric comparative study with surgical implications — Acta Neurochirurgica 2026; CC BY.
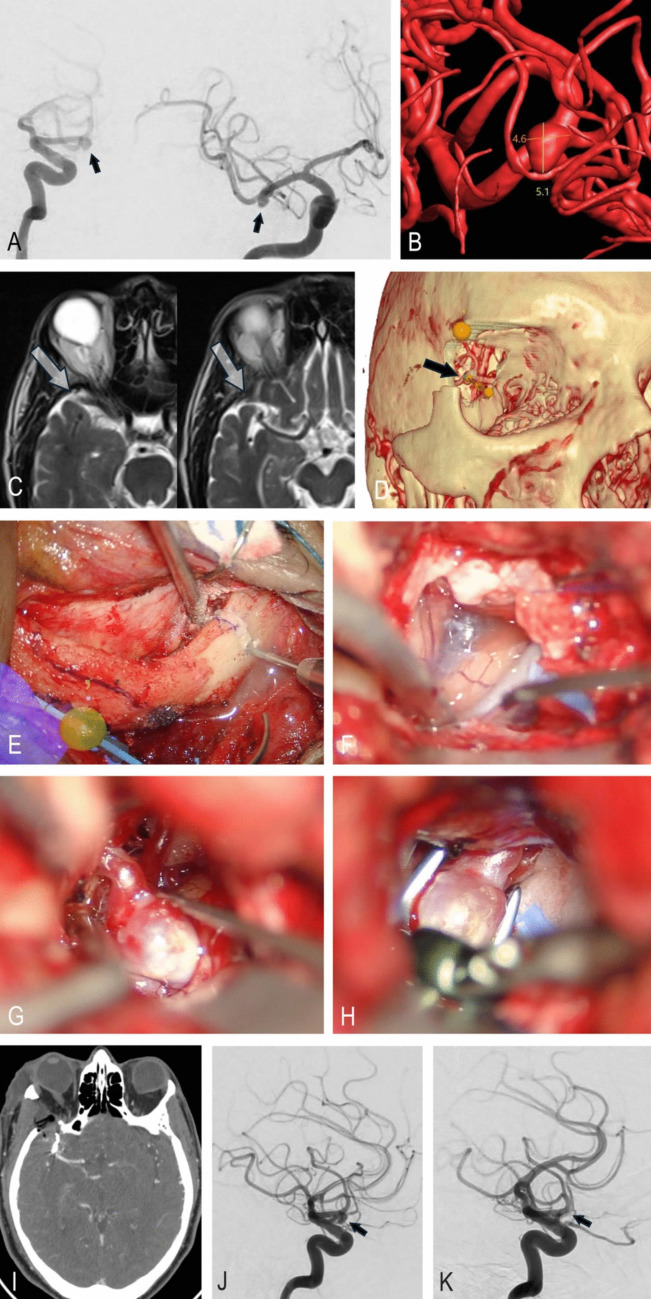 Fig. 5. Illustrative case. A Preoperative lateral and anteroposterior DSA showing a right MCA bifurcation aneurysm (black arrows). B 3D reconstructed aneurysm model with size measurements and… Source: Microscopic transorbital vs mini-pterional approach to MCA bifurcation aneurysms: a quantitative cadaveric comparative study with surgical implications — Acta Neurochirurgica 2026; CC BY.
Fig. 5. Illustrative case. A Preoperative lateral and anteroposterior DSA showing a right MCA bifurcation aneurysm (black arrows). B 3D reconstructed aneurysm model with size measurements and… Source: Microscopic transorbital vs mini-pterional approach to MCA bifurcation aneurysms: a quantitative cadaveric comparative study with surgical implications — Acta Neurochirurgica 2026; CC BY.
Detailed operative reference written for a senior resident / fellow / attending. Pathology guides (e.g., MCA aneurysm, sphenoid wing meningioma) link here for technique.
Atlas operative videos — open on the Pterional Craniotomy chapter page: How Do I Do It · Improving the Efficiency of Exposure · Nuances & Pitfalls · Subfascial Technique · Placement of the Pins. (Rhoton: Preserving the Frontalis Muscle.)
1. General Considerations
The pterional (frontotemporal) craniotomy is the workhorse of supratentorial surgery — the most flexible, efficient corridor to the anterior and middle skull base. Its leverage comes from removing the sphenoid wing so you look down the subfrontal corridor and along the ridge into the sylvian fissure, minimizing frontal-lobe retraction.
- Standard vs extended: the extended pterional adds (1) osteotomy of the lateral sphenoid wing to the superior orbital fissure, (2) drilling/flattening of the orbital roof, and (3) rongeuring temporal squama to the middle-fossa floor — capturing much of the orbitozygomatic benefit with less morbidity/cosmetic cost. These bone-removal maneuvers, not a bigger skin flap, are what create the exposure.
- Philosophy: tailor rotation, sphenoid drilling, and the sylvian split to the specific target. Yaşargil’s principle — spend time on the approach/bone work and arachnoid dissection so the deep work is safe. Routine indiscriminate use of one fixed exposure should be avoided.
- Keyhole variants: mini-pterional and supraorbital “eyebrow” achieve similar deep reach for selected parasellar/anterior lesions.
2. Indications
- Aneurysms: MCA, AComA, PComA, ICA bifurcation, ophthalmic/paraclinoid; basilar apex (with extension ± OZ); selected contralateral ophthalmic/MCA/P1.
- Tumors: sphenoid wing / clinoidal / tuberculum sellae / planum meningiomas; suprasellar, parasellar, cavernous-sinus tumors; anterior temporal & insular lesions.
- Generally NOT: purely third-ventricular tumors; pituitary adenomas (endoscopic endonasal preferred); giant midline anterior-fossa-floor meningiomas may still favor a unilateral subfrontal/extended pterional over bifrontal in many hands.
3. Preoperative Considerations
- AEDs for cortical/temporal lesions; some stop ~7 days post-op if seizure-free.
- Lumbar drain for large skull-base lesions filling the basal cisterns (blocked CSF pathways prevent relaxation on dural opening).
- Mannitol per mass effect; dexamethasone for vasogenic edema; embolization used sparingly for vascular meningiomas/AVMs.
- Neuronavigation (CTA/MR); IONM (SSEP/MEP); EEG for burst suppression if temporary clipping anticipated.
- BP: normotensive throughout, except AVM (SBP kept ~20–30% below baseline).
Logistics, OR Setup & Orders
- OR setup: Mayfield/head holder plan, microscope/endoscope, navigation, vascular instruments/ICG when applicable, skull base reconstruction supplies, and approach-specific retractors/drills ready before opening.
- Special needs: arterial line for major intracranial or vascular cases, Foley for long cases, neuromonitoring by corridor, dexamethasone/antiepileptic/BP plan by pathology, and blood products for vascular or skull base exposure.
- Immediate postop orders: disposition and neuro-check frequency, HOB/activity, postop CT/MRI/CTA timing, BP goals, steroid/antiepileptic plan, DVT prophylaxis timing, drain management, and focused cranial nerve/visual/language/motor exams.
4. Operative Anatomy (what you must own)
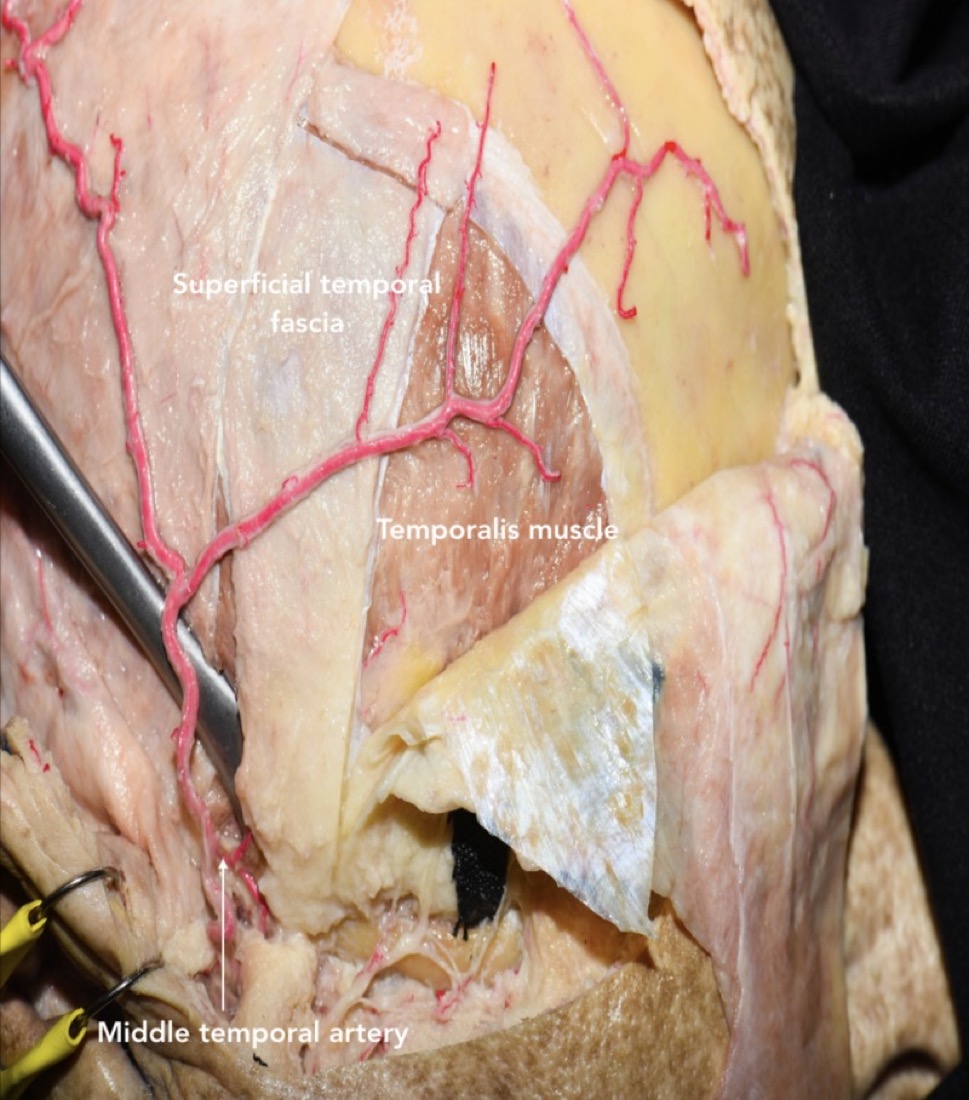
- Scalp — 5 layers (SCALP): Skin · subCutaneous (vessels/nerves) · Aponeurosis (galea) · Loose areolar · Pericranium. The galea continues over the temporal region as the temporoparietal fascia (TPF).
- Temporal fascia: below the TPF and loose areolar plane lies the temporalis (deep temporal) fascia, which near the arch splits into superficial and deep laminae enclosing the superficial temporal fat pad.
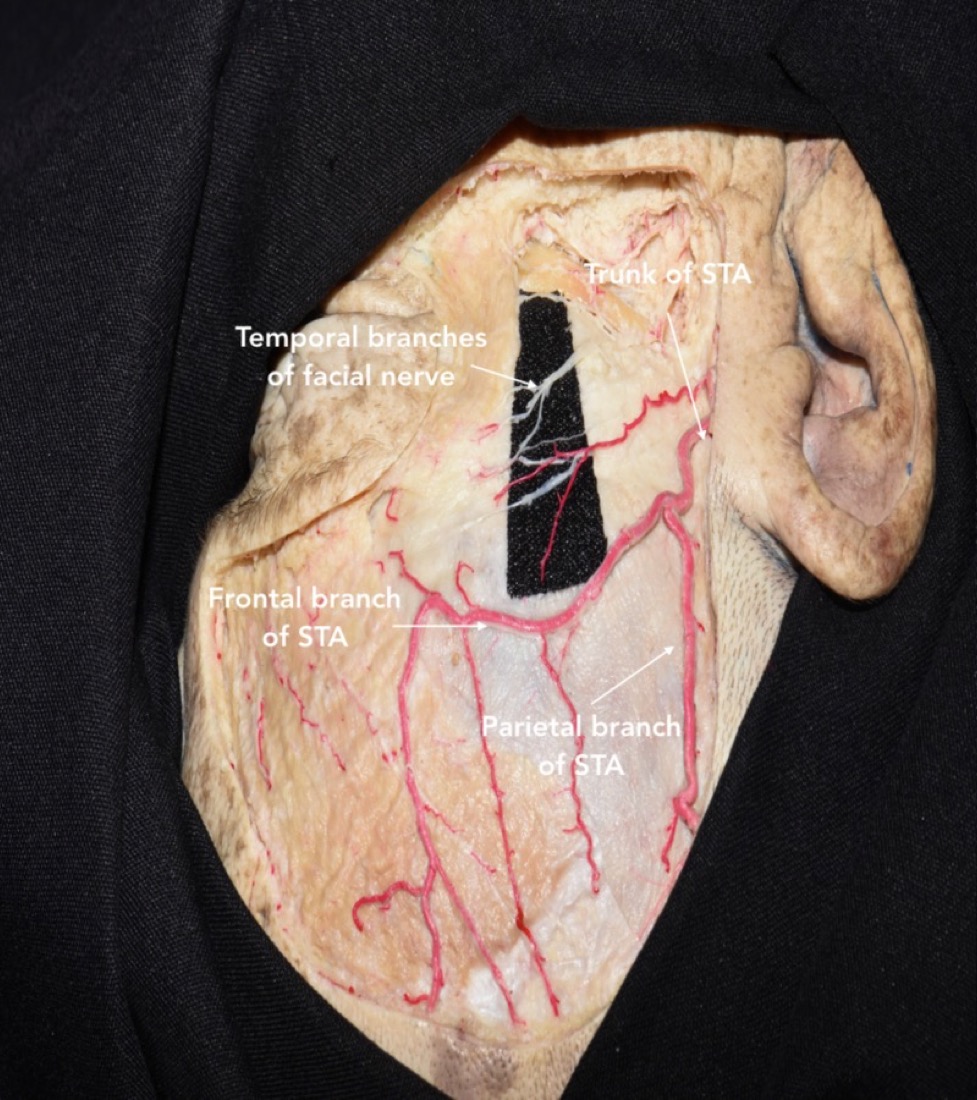
- Frontotemporal (frontalis) branches of CN VII: run within/over the fat pad as they cross the zygomatic arch toward frontalis — the structure most often injured. Protected by interfascial or subfascial dissection (carry the fat pad down with the flap) or a single-layer myocutaneous flap.
- STA: main trunk anterior to the tragus; frontal & parietal branches — preserve if any chance of future bypass; the incision should not extend below the zygoma (facial-nerve trunk risk).
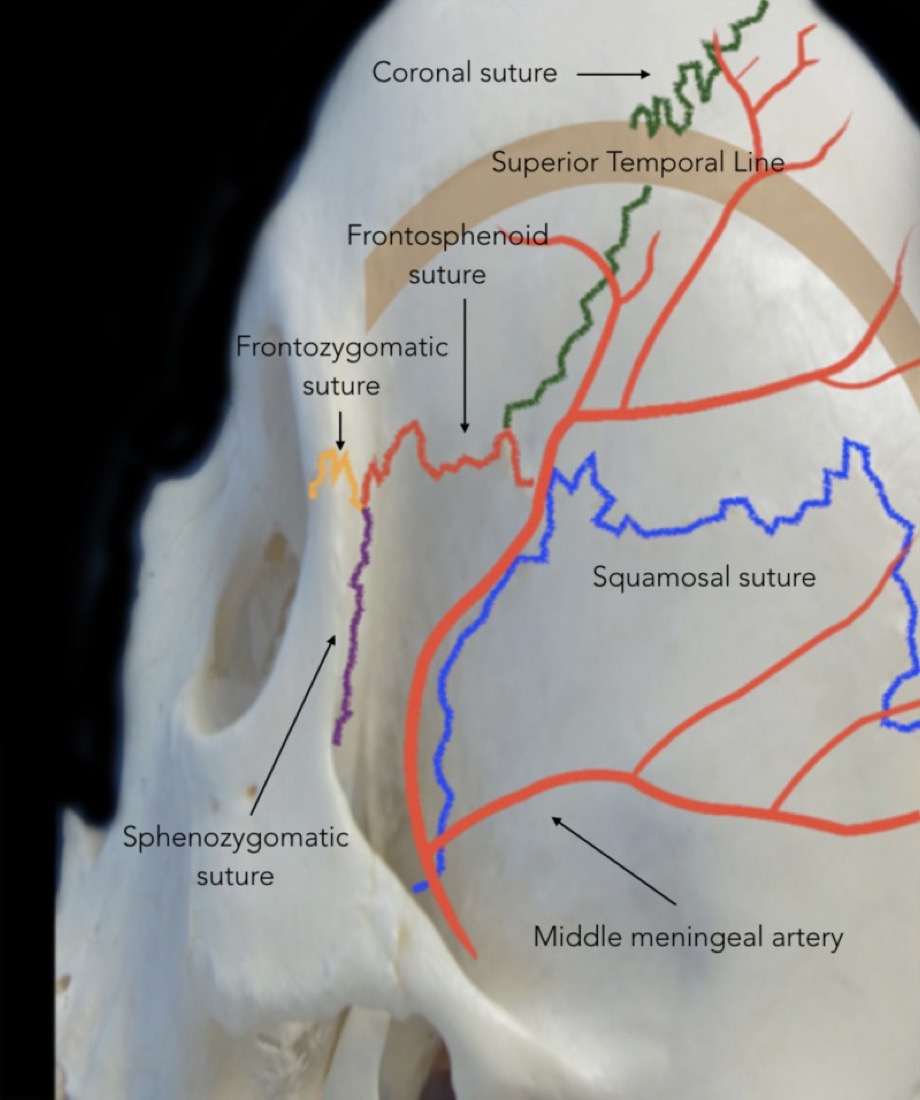
- Keyhole (MacCarty point): frontal process of zygoma + superior temporal line + frontozygomatic suture; one burr hole exposes periorbita below and frontal dura above.
- Pterion: frontal-parietal-temporal-sphenoid confluence; anterior division of the MMA runs beneath — bleeds when the wing is drilled.
- Sphenoid wing → superior orbital fissure → orbital roof; sylvian fissure; deep targets: ICA & branches, optic nerve/chiasm, A1/M1, basal cisterns.
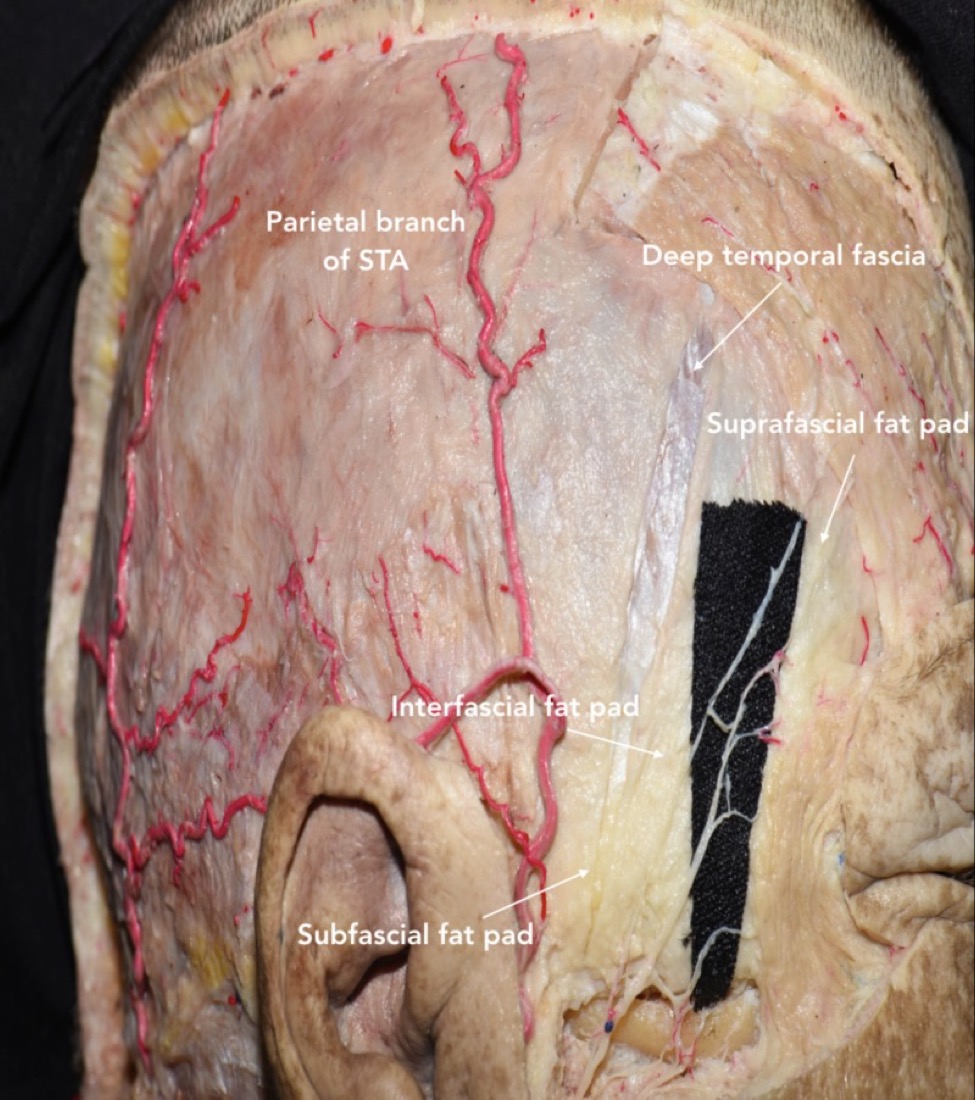 Cadaveric dissection — Rodriguez Rubio R et al., Cureus 2019;11(7):e5216 (CC BY).
Cadaveric dissection — Rodriguez Rubio R et al., Cureus 2019;11(7):e5216 (CC BY).
 Cadaveric dissection — Rodriguez Rubio R et al., Cureus 2019;11(7):e5216 (CC BY).
Cadaveric dissection — Rodriguez Rubio R et al., Cureus 2019;11(7):e5216 (CC BY).
5. Positioning
- Supine, knees flexed, table up ~15–20° (reverse Trendelenburg); head above the heart.
- Mayfield 3-pin: double-pin rocker on the contralateral superior temporal line, single pin on the ipsilateral mastoid — all well behind the planned incision, out of the flap, away from the temporalis and frontal sinus/orbit.
- Rotation (target-driven): closer to midline / more anterior ⇒ turn LESS. ~30° AComA; ~45° MCA; less rotation + more deflection for superiorly-extending suprasellar tumors; basal lesions (ophthalmic/PComA, cavernous sinus) ⇒ less deflection, more rotation to keep the orbital rim in the superior plane.
- Extension until the malar eminence is the highest point → frontal lobe falls off the anterior fossa floor by gravity; vertex down ~15°.
- Ipsilateral shoulder roll if neck mobility is limited; re-check IONM after positioning. Nuance: over-rotation drops the temporal lobe into your subfrontal view and tents the sylvian veins — under-rotate and let gravity, not retractors, do the work.
6. Skin Marking & Incision
- Curvilinear (reverse question-mark) behind the hairline: start ~1 cm anterior to the tragus at the zygomatic root, curve posterosuperiorly, then forward to the midline / contralateral mid-pupillary line.
- Keep the STA posterior in the flap when feasible; frontalis branch stays anterior to the incision. For a pure subfrontal target, do not extend far behind the hairline; keep the flap’s connecting line within ~1 cm of the keyhole.
7. Scalp Incision Technique
- Infiltrate; Raney clips / bipolar for hemostasis. As the incision reaches the superior temporal line, slide a periosteal elevator under the subcutaneous tissue to protect the STA and temporalis, then cut skin onto the elevator.
- STA: identify, dissect to the frontal/parietal bifurcation; coagulate & divide the frontal branch (preserve parietal) for a standard flap — but preserve branches if a bypass is conceivable or for a large posteriorly-extended flap (flap vascularity/healing).
8. Frontalis-Branch Protection — choose your technique
- Single-layer myocutaneous flap (one layer): raise skin + temporalis together; fast, robust vascularity. Nuance: reflect maximally anteroinferiorly to reveal the pterion; place rolled gauze under the flap to prevent kinking/ischemia of the scalp.
- Interfascial: ~4 cm above the orbital rim, incise the superficial layer of temporalis fascia at the upper edge of the fat pad and carry the fat pad + superficial layer (with the nerve on its outer surface) down with the flap.
- Subfascial: elevate beneath the superficial temporal fat pad off the deep layer.
- Pearl: never skeletonize the frontalis branch off the fat pad — keep it sandwiched in tissue. Frontalis palsy is the signature avoidable complication.
9. Temporalis Dissection & Reflection
- Incise temporalis with monopolar in two limbs (along the superior temporal line and the inferior incision) leaving a fascial cuff superiorly for reattachment, OR reflect as one myocutaneous layer.
- Preserve the deep temporal fascia / deep temporal neurovascular pedicle (avoid heavy monopolar on the deep surface) to minimize temporalis atrophy & trismus.
- Reflect inferiorly over the zygoma; secure with fishhooks; expose the frontal process of the zygoma just anterior to the keyhole for orbital-roof extension.
 Cadaveric dissection — Rodriguez Rubio R et al., Cureus 2019;11(7):e5216 (CC BY).
Cadaveric dissection — Rodriguez Rubio R et al., Cureus 2019;11(7):e5216 (CC BY).
10. Keyhole & Burr Hole(s)
- Single burr hole just inferior to the most posterior exposed superior temporal line; sweep the dura free with a #3 Penfield to mobilize the whole flap toward the pterion. Nuance: a single hole behind the hairline, under muscle minimizes cosmetic defect vs. the classic 2-hole (keyhole + zygomatic root) technique.
- The MacCarty keyhole is used when orbit + anterior fossa need to be entered together; a “modified pterional without MacCarty keyhole” is also valid.
 Cadaveric dissection — Rodriguez Rubio R et al., Cureus 2019;11(7):e5216 (CC BY).
Cadaveric dissection — Rodriguez Rubio R et al., Cureus 2019;11(7):e5216 (CC BY).
11. Craniotomy
- Footplate craniotome (B1): two osteotomies. After the first cut, the drill stalls at the lateral sphenoid wing → turn 180° at the pterion to create room, remove the heel, and start the second osteotomy. Outline matches pathology (MCA vs AComA outlines differ; anterior-fossa tumors follow the AComA outline).
- Pitfall: the footplate tears dura on the turns, especially the frontal turn — go slow, lift, and irrigate.
12. Frontal Sinus Management
- The anteromedial cut may enter the frontal sinus (supraorbital notch is an unreliable lateral landmark — use navigation). If entered: exenterate the mucosa, pack with muscle/bone wax, and plan a pericranial buttress at closure to prevent CSF leak / mucocele.
13. Sphenoid Wing Drilling — the key step
- After elevating the flap, strip dura off the orbital roof (Penfield #1) and mobilize dura off both frontal and temporal surfaces of the ridge.
- Remove the lateral/mid sphenoid ridge aggressively — rongeur first for speed, then a side-cutting air drill — until flat to the skull base. Control MMA bleeding at the wing.
- Extended pterional: continue to the superior orbital fissure, flatten the orbital roof and supraorbital edge — critical for an unobstructed subfrontal view toward the midline anterior skull base.
14. Dural Opening
- Curvilinear, reflected anteroinferiorly toward the sphenoid ridge; tack-up sutures placed close to the brain to pull dura + muscle out of the subfrontal working zone. Three tack-ups typically. Protect cortex and sylvian/superficial middle cerebral vein.
15. Brain Relaxation & Intradural Orientation
- Relax via cisternal CSF egress (carotid, chiasmatic, lamina terminalis), lumbar drain, mannitol, head-up. Split the sylvian fissure (inside-out or outside-in) to the extent the target requires, preserving the superficial middle cerebral vein. → proceed to pathology-specific intradural steps (see the relevant guide).
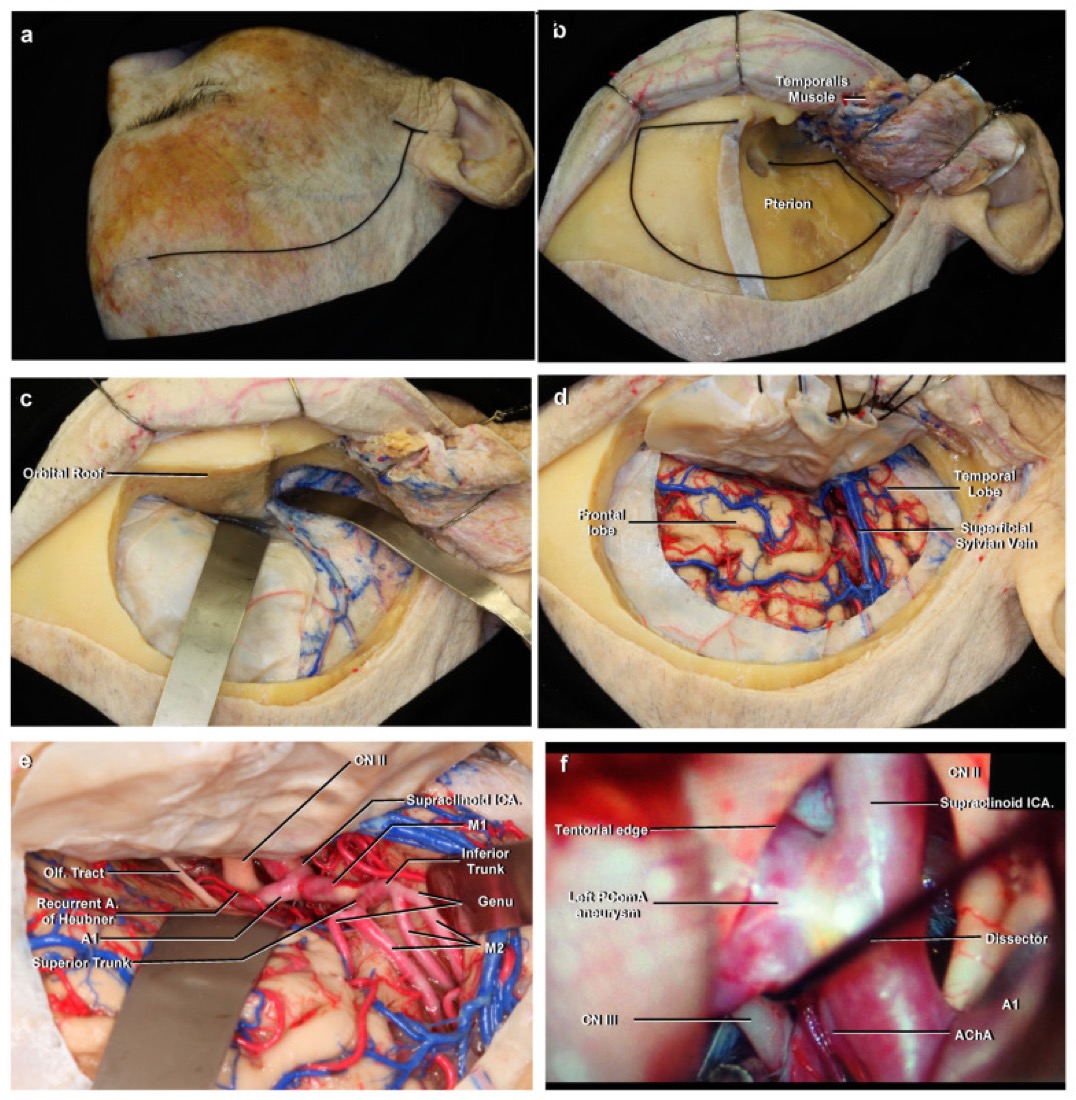 Poblete T et al., “Microsurgical Anatomy of the Anterior Circulation…” Brain Sci 2021;11(4):519 (CC BY 4.0).
Poblete T et al., “Microsurgical Anatomy of the Anterior Circulation…” Brain Sci 2021;11(4):519 (CC BY 4.0).
16. Closure
- Dura: approximate; watertight closure not obligatory for a supratentorial craniotomy unless the ventricle was entered or hydrocephalus/raised CSF pressure is expected — then close watertight ± graft.
- Bone flap: ≥3 mini-plates; central dural tack-up optional; the behind-hairline burr hole preserves keyhole bone for cosmesis.
- Temporalis: reattach fascia to its superior cuff (single-layer flap: reattach posteriorly; approximate fascia gently to limit jaw-movement pain). Subgaleal drain only if scalp hemostasis is problematic. Layered scalp closure.
17. Nuances & Pitfalls (high-yield)
- Frontalis palsy — interfascial/subfascial or single-layer flap; never dissect the nerve free.
- Temporalis atrophy/trismus — preserve deep temporal pedicle; reattach anatomically; avoid monopolar on the deep muscle surface.
- Under-drilled sphenoid wing = “deep, narrow” exposure — the most common technical shortfall; flatten to base ± orbital roof.
- Frontal sinus entry — exenterate/pack + pericranial buttress.
- Dural tear on craniotome turns — anticipate at the frontal turn.
- MMA/wing bleeding — control early; wax the wing.
- Sylvian/bridging vein sacrifice — venous infarct; preserve the SMCV.
- Over-rotation/under-extension — temporal lobe obscures the subfrontal corridor.
18. Complications
Frontalis (CN VII) palsy; temporalis atrophy / trismus; CSF leak / mucocele (sinus, dura); wound infection; seizures; retraction injury; vascular injury (SMCV, MCA/ICA branches, perforators); cosmetic contour deformity; pseudomeningocele.
Figure Use & Attribution
About the figures (read once): Operative step illustrations/photos (Neurosurgical Atlas, Rhoton) are copyrighted and are linked, not copied. Embedded images here are public-domain anatomy plates (+ open-access CC-BY figures where added). See media-sources.md.
Chief-Level Corridor Review
Use these as the senior-level mental model for Approach: Pterional (Frontotemporal) Craniotomy:
- Decision point: Define the exposure goal before incision: target, working angles, proximal/distal control, and the structure that cannot tolerate retraction.
- Technical lever: Know the first irreversible step: bone removal, dural opening, vascular control, or muscle/fascial division that commits the corridor.
- Bailout: Verbalize the bailout: extend exposure, change trajectory, add CSF drainage, obtain proximal control, convert to a larger corridor, or stop for imaging.
- Postop watch: Protect closure from the start: vascularized tissue, watertight dural/reconstruction plan, dead-space control, and drain strategy should be chosen before the final intradural step.
Common Pimp Questions
Use these to pressure-test preparation for Pterional (Frontotemporal) Craniotomy:
- What patient position and head rotation make gravity work for this corridor?
- What named nerve, vessel, sinus, or muscle/fascial plane is most commonly injured?
- What bone work or soft-tissue step creates the exposure rather than simply using more retraction?
- What is the bailout if exposure is inadequate, bleeding occurs, or the brain is tight?
- What closure maneuver prevents the signature complication of this approach?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Exact head rotation/flexion/extension and pin placement: [attending-specific]
- Skin incision length, flap type, and muscle/fascial preservation technique: [attending-specific]
- Drill, rongeur, endoscope, microscope, retractor, and navigation preferences: [attending-specific]
- Drain use, closure materials, watertightness threshold, and postop imaging routine: [attending-specific]
Case Guides Using This Approach
- Anterior Communicating Artery (AComA) Aneurysm Clipping
- Arteriovenous Malformation (AVM) Resection
- EC-IC Bypass (STA-MCA)
- Glioma Resection (Supratentorial)
- Insular Glioma Resection
- MCA Aneurysm Clipping
- Posterior Communicating Artery (PComA) Aneurysm Clipping
- Sphenoid Wing Meningioma Resection
References
- Yaşargil MG. Microneurosurgery, Vol. I. Georg Thieme Verlag; 1984:217–220.
- Krayenbühl N, Isolan GR, Hafez A, Yaşargil MG. The relationship of the fronto-temporal branches of the facial nerve to the fascias of the temporal region: a literature review applied to practical anatomical dissection. Neurosurg Rev. 2007;30(1):8–15.
- Shimizu S, Tanriover N, Rhoton AL Jr, Yoshioka N, Fujii K. MacCarty keyhole and inferior orbital fissure in orbitozygomatic craniotomy. Neurosurgery. 2005;57(1 Suppl):152–159.
- Figueiredo EG, Deshmukh P, Nakaji P, et al. The minipterional craniotomy: technical description and anatomic assessment. Neurosurgery. 2007;61(5 Suppl 2):256–265.
- Rodriguez Rubio R, Chae R, Vigo V, Abla AA, McDermott M. Immersive Surgical Anatomy of the Pterional Approach. Cureus. 2019;11(7):e5216. (CC BY — cadaveric figures embedded above) — PMC6759424
- Poblete T, Casanova D, Soto M, Campero A, Mura J. Microsurgical Anatomy of the Anterior Circulation of the Brain Adjusted to the Neurosurgeon’s Daily Practice. Brain Sci. 2021;11(4):519. (CC BY 4.0 — figure embedded above) — PMC8073207
- Rhoton AL Jr. Cranial Anatomy and Surgical Approaches. Congress of Neurological Surgeons.
- The Neurosurgical Atlas (Cohen-Gadol AA) — Pterional Craniotomy chapter (operative figures/videos, linked).
- Further open-access technique papers: PubMed Central — pterional craniotomy; Surgical Neurology International — suprafascial dissection.