
Case Prep: Tuberculum Sellae Meningioma Resection
Case / Approach Snapshot
- Anatomy at risk: tumor compartment, arterial supply, venous drainage/sinuses, cranial nerves, white-matter tracts, pituitary/CSF pathways when relevant, and functional cortex.
- Operative steps: review imaging and goals, choose exposure, obtain brain relaxation, devascularize when possible, debulk internally, dissect capsule from critical structures, verify extent/safety, and reconstruct watertight closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: venous or arterial injury, swelling, seizure, cranial nerve or endocrine change, CSF leak, residual tumor left for safety, staged surgery, radiation, or adjuvant therapy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a tuberculum sellae meningioma presenting with [progressive visual loss / bitemporal or junctional field defect] planned for [pterional / supraorbital / endoscopic endonasal] approach for resection.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
CNS Video Library
🧭 Operative approach: Supraorbital keyhole craniotomy — detailed corridor setup, step-by-step technique & figures
Operative figures/atlases are © (linked, not copied). See media-sources.md.
- Technique/approach: The Neurosurgical Atlas — search “tuberculum sellae meningioma”
- Imaging: Radiopaedia — tuberculum sellae meningioma
- Open-access figures: PubMed Central
High-Yield Literature
- International Tuberculum Sellae Meningioma Study: Surgical Outcomes and Management Trends — Magill ST. Neurosurgery 2023. PubMed
- Tuberculum Sellae Meningioma: Report of Two Cases and Literature Review of Limits of the Transcranial and Endonasal Endoscopic Approaches — Silvestri M. Acta neurochirurgica. Supplement 2023. PubMed
- International Tuberculum Sellae Meningioma Study: Preoperative Grading Scale to Predict Outcomes and Propensity-Matched Outcomes by Endonasal Versus Transcranial Approach — Magill ST. Neurosurgery 2023. PubMed
- Surgical Management of Tuberculum Sellae Meningioma: Our Experience and Review of the Literature — Sankhla SK. Neurology India 2021. PubMed
- Olfactory groove and tuberculum sellae meningioma resection by endoscopic endonasal approach versus transcranial approach: A systematic review and meta-analysis of comparative studies — Lu VM. Clinical neurology and neurosurgery 2018. PubMed
- Surgical management of tuberculum sellae meningioma: Transcranial approach or endoscopic endonasal approach? — Qian K. Frontiers in surgery 2022. PubMed
- Contralateral supraorbital eyebrow approach for tuberculum sellae meningioma — Das KK. Acta neurochirurgica 2023. PubMed
- Tuberculum sellae meningioma surgery: visual outcomes and surgical aspects of contralateral approach — Voznyak O. Neurosurgical review 2021. PubMed
- Contralateral subfrontal approach for tuberculum sellae meningioma: techniques and clinical outcomes — Kim YJ. Journal of neurosurgery 2023. PubMed
- Microsurgical Resection of Tuberculum Sellae Meningioma through Pterional Approach with Extradural Optic Canal Unroofing — Matsuo S. Journal of neurological surgery. Part B, Skull base 2022. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
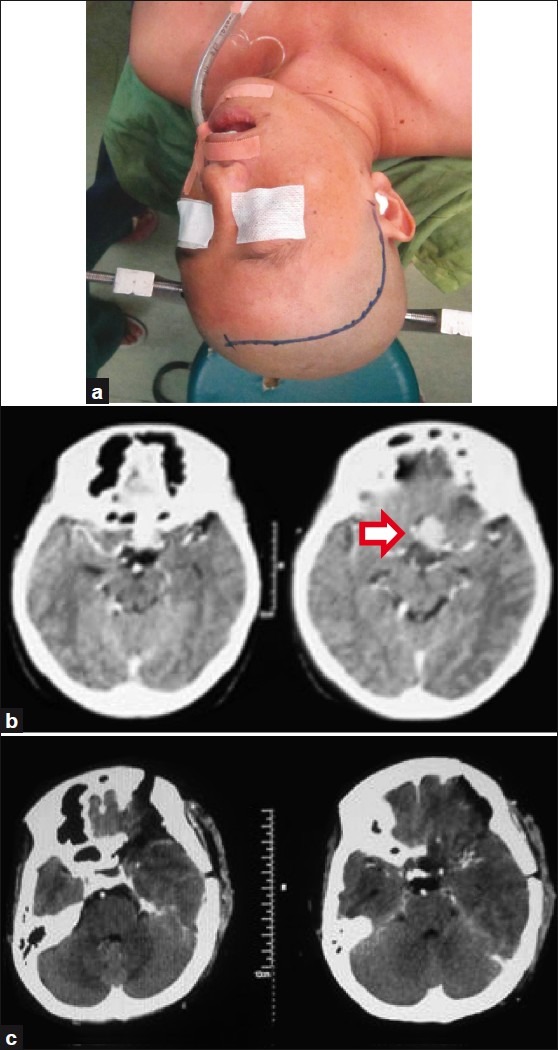 Figure 1. Pterional approach marking (a) A representative head CT scan before; (b) and after pterional approach surgery; (c) Red arrow: Tuberculum sellae meningioma Source: Pterional approach versus unilateral frontal approach on tuberculum sellae meningioma: Single centre experiences — Asian Journal of Neurosurgery 2012; CC BY-NC-SA.
Figure 1. Pterional approach marking (a) A representative head CT scan before; (b) and after pterional approach surgery; (c) Red arrow: Tuberculum sellae meningioma Source: Pterional approach versus unilateral frontal approach on tuberculum sellae meningioma: Single centre experiences — Asian Journal of Neurosurgery 2012; CC BY-NC-SA.
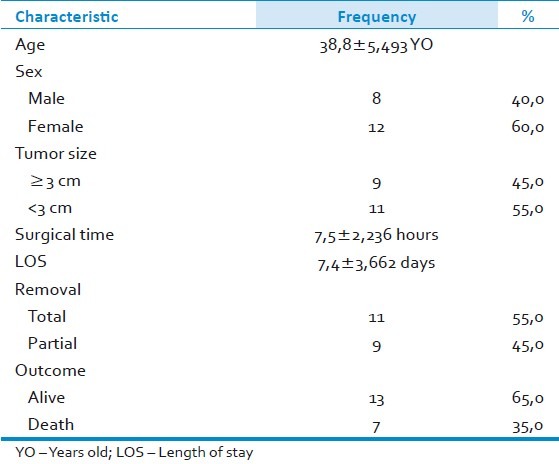 Figure 2. Source: Pterional approach versus unilateral frontal approach on tuberculum sellae meningioma: Single centre experiences — Asian J Neurosurg. 2012 Jan-Mar;7(1):21–4. doi: 10.4103/1793-5482.95691; CC BY-NC-SA.
Figure 2. Source: Pterional approach versus unilateral frontal approach on tuberculum sellae meningioma: Single centre experiences — Asian J Neurosurg. 2012 Jan-Mar;7(1):21–4. doi: 10.4103/1793-5482.95691; CC BY-NC-SA.
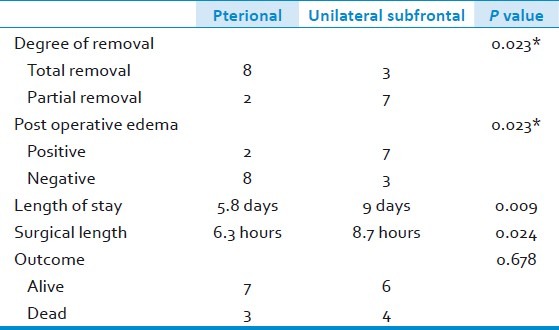 Figure 3. Source: Pterional approach versus unilateral frontal approach on tuberculum sellae meningioma: Single centre experiences — Asian J Neurosurg. 2012 Jan-Mar;7(1):21–4. doi: 10.4103/1793-5482.95691; CC BY-NC-SA.
Figure 3. Source: Pterional approach versus unilateral frontal approach on tuberculum sellae meningioma: Single centre experiences — Asian J Neurosurg. 2012 Jan-Mar;7(1):21–4. doi: 10.4103/1793-5482.95691; CC BY-NC-SA.
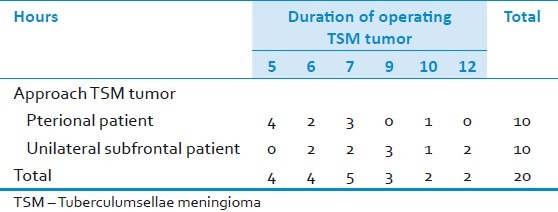 Figure 4. Source: Pterional approach versus unilateral frontal approach on tuberculum sellae meningioma: Single centre experiences — Asian J Neurosurg. 2012 Jan-Mar;7(1):21–4. doi: 10.4103/1793-5482.95691; CC BY-NC-SA.
Figure 4. Source: Pterional approach versus unilateral frontal approach on tuberculum sellae meningioma: Single centre experiences — Asian J Neurosurg. 2012 Jan-Mar;7(1):21–4. doi: 10.4103/1793-5482.95691; CC BY-NC-SA.
 Figure 5. Source: Pterional approach versus unilateral frontal approach on tuberculum sellae meningioma: Single centre experiences — Asian J Neurosurg. 2012 Jan-Mar;7(1):21–4. doi: 10.4103/1793-5482.95691; CC BY-NC-SA.
Figure 5. Source: Pterional approach versus unilateral frontal approach on tuberculum sellae meningioma: Single centre experiences — Asian J Neurosurg. 2012 Jan-Mar;7(1):21–4. doi: 10.4103/1793-5482.95691; CC BY-NC-SA.
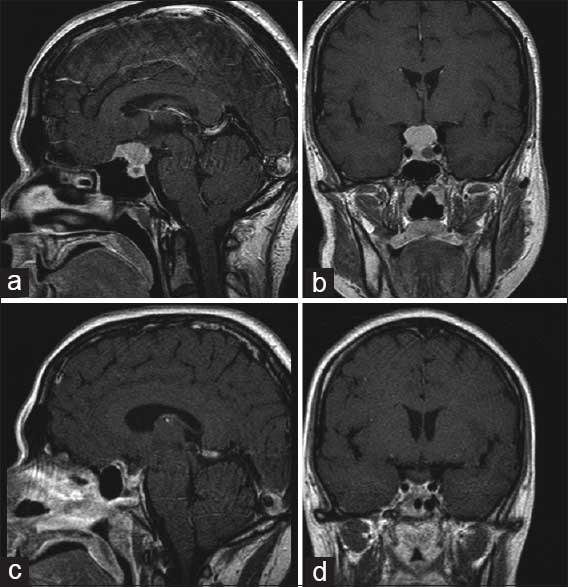 Figure 1. Magnetic resonance images: T1 weighted contrast-enhanced sagittal (a) and coronal (b) preoperative images showing coexistent macroadenoma and tuberculum sellae meningioma. Postoperative… Source: Endoscopic endonasal transsphenoidal approach for resection of a coexistent pituitary macroadenoma and a tuberculum sellae meningioma — Asian Journal of Neurosurgery 2014; CC BY-NC-SA.
Figure 1. Magnetic resonance images: T1 weighted contrast-enhanced sagittal (a) and coronal (b) preoperative images showing coexistent macroadenoma and tuberculum sellae meningioma. Postoperative… Source: Endoscopic endonasal transsphenoidal approach for resection of a coexistent pituitary macroadenoma and a tuberculum sellae meningioma — Asian Journal of Neurosurgery 2014; CC BY-NC-SA.
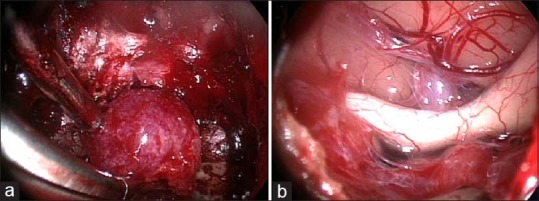 Figure 2. (a) The intraoperative endoscopic view (screenshot) of the endonasal transsphenoidal approach to the planum sphenoidale and tuberculum sellae and identification of the meningioma. (b)… Source: Endoscopic endonasal transsphenoidal approach for resection of a coexistent pituitary macroadenoma and a tuberculum sellae meningioma — Asian Journal of Neurosurgery 2014; CC BY-NC-SA.
Figure 2. (a) The intraoperative endoscopic view (screenshot) of the endonasal transsphenoidal approach to the planum sphenoidale and tuberculum sellae and identification of the meningioma. (b)… Source: Endoscopic endonasal transsphenoidal approach for resection of a coexistent pituitary macroadenoma and a tuberculum sellae meningioma — Asian Journal of Neurosurgery 2014; CC BY-NC-SA.
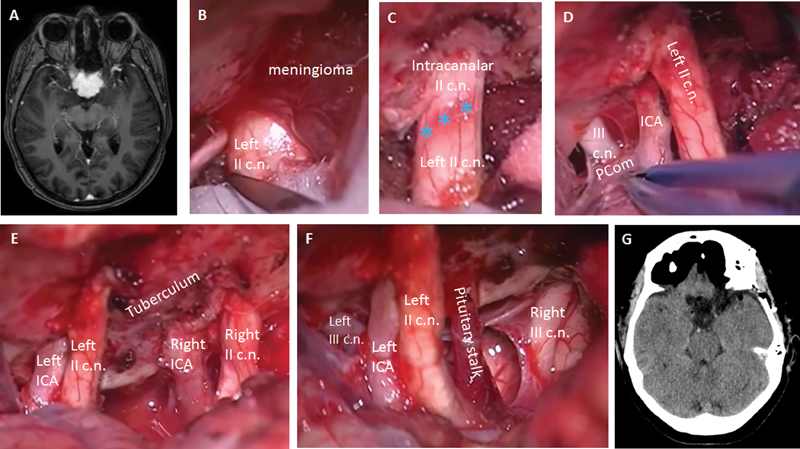 Fig. 1. ( A ) Preoperative MRI shows a contrast-enhanced tuberculum sellae lesion, suspicious of meningioma. ( B ) The left optic nerve (II c.n.) is evidenced through a left pterional approach…. Source: Tuberculum Sellae Meningioma Resection: Technical Nuances on the Frontopterional Approach — Journal of Neurological Surgery. Part B, Skull Base 2018; CC BY-NC-ND.
Fig. 1. ( A ) Preoperative MRI shows a contrast-enhanced tuberculum sellae lesion, suspicious of meningioma. ( B ) The left optic nerve (II c.n.) is evidenced through a left pterional approach…. Source: Tuberculum Sellae Meningioma Resection: Technical Nuances on the Frontopterional Approach — Journal of Neurological Surgery. Part B, Skull Base 2018; CC BY-NC-ND.
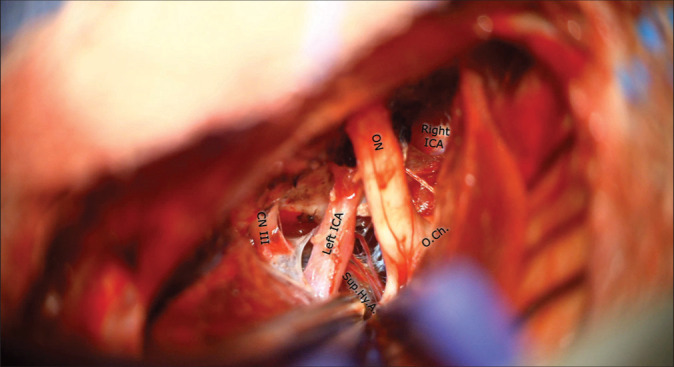 Figure. Figure 1 Source: Keyhole supraorbital eyebrow approach for the resection of a tuberculum sellae meningioma with intraoperative endoscopic assistance — Surgical Neurology International 2022; CC BY-NC-SA.
Figure. Figure 1 Source: Keyhole supraorbital eyebrow approach for the resection of a tuberculum sellae meningioma with intraoperative endoscopic assistance — Surgical Neurology International 2022; CC BY-NC-SA.
 Figure 10. Source: Keyhole supraorbital eyebrow approach for the resection of a tuberculum sellae meningioma with intraoperative endoscopic assistance — Surg Neurol Int. 2022 Mar 18;13:93. doi: 10.25259/SNI_1173_2021; CC BY-NC-SA.
Figure 10. Source: Keyhole supraorbital eyebrow approach for the resection of a tuberculum sellae meningioma with intraoperative endoscopic assistance — Surg Neurol Int. 2022 Mar 18;13:93. doi: 10.25259/SNI_1173_2021; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Progressive asymmetric visual loss (chiasmal compression) — the hallmark
- Classic: junctional scotoma or bitemporal field defect
- Headache, endocrine usually intact (vs pituitary)
Imaging Review
MRI (T1+Gad, thin-cut sella, T2) + MRA
- Tumor centered on tuberculum sellae, suprasellar
- Optic nerve/chiasm displacement (usually superior/posterior) — chiasm prefixed?
- Optic canal extension (common — must decompress)
- ICA and branches relationship; ACA complex superiorly
- Pituitary stalk/gland (usually separate, displaced inferiorly)
- Vascular supply
CT
- Hyperostosis of tuberculum/planum, optic canal anatomy, sphenoid pneumatization (for endonasal)
Ophthalmology
- Formal fields, acuity, OCT/RNFL
Labs
- CBC, BMP, Coags, Type and screen; pituitary panel (baseline)
Neurological Examination
- Detailed visual assessment, EOM, endocrine review
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: navigation, endoscope/microscope as approach requires, ENT co-surgeon for endonasal cases, Doppler, lumbar drain only when indicated, reconstruction materials, and visual/endocrine baseline available.
- Special needs: steroid strategy individualized (Cushing workup may require avoiding preop steroids), DI/sodium protocol, AM cortisol/endocrine labs, visual-check plan, arterial line for large/vascular cases, and CSF-leak/nasal precautions.
- Immediate postop orders: neuro and visual checks, strict I/O with sodium/urine specific gravity schedule when pituitary stalk risk exists, cortisol/endocrine replacement plan, nasal precautions, MRI/CT timing, steroid taper, and DVT prophylaxis timing.
Approach Selection
- Pterional/supraorbital (transcranial): Lateral view, early ICA/optic control, good for lateral extension or vessel encasement
- Endoscopic endonasal: Direct inferior-to-superior access, early devascularization, decompresses optic canals medially, no brain/optic nerve retraction — favored for midline tumors without significant lateral/vascular encasement; requires skull base reconstruction
- Side (transcranial): side of worse vision or larger tumor extension
Position
- Pterional: supine, rotated 20-30 degrees contralateral, extended, Mayfield
- Endonasal: supine, slight extension, navigation
Key Surgical Steps (Transcranial)
- Pterional/supraorbital craniotomy, drill sphenoid wing
- Open sylvian/basal cisterns, drain CSF
- Identify ipsilateral optic nerve, ICA, chiasm
- Unroof optic canal to decompress and free the optic nerve (improves visual outcome)
- Devascularize tumor base at tuberculum/planum
- Internal debulking; dissect tumor off optic apparatus (preserve pial vessels/superior hypophyseal arteries to chiasm)
- Protect ACA complex superiorly, ICA laterally, stalk inferiorly
- Resect base dura/bone (Simpson I if safe)
- Reconstruction, closure
Critical Anatomy & Structures at Risk
- Optic nerves / chiasm — primary structure; preserve superior hypophyseal artery branches to chiasm (visual outcome)
- ICA and branches
- ACA / A1 complex (superior)
- Pituitary stalk and gland
- Optic canal (decompress)
Equipment
- Microscope (± endoscope), navigation, high-speed drill (optic canal), CUSA, ICG
- Skull base reconstruction (nasoseptal flap if endonasal; graft/sealant)
Monitoring
- SSEPs; VEPs (optional)
Anesthesia
- Arterial line, mannitol, dexamethasone, lumbar drain (endonasal)
Potential Complications
- Visual worsening — devascularization of chiasm (superior hypophyseal artery injury)
- ICA injury, CSF leak (esp. endonasal), hypopituitarism/DI
- Residual in optic canal → recurrence
Operative Note Template
Preoperative Diagnosis: Tuberculum sellae meningioma with progressive [asymmetric] visual loss
Postoperative Diagnosis: Same
Procedure: [Pterional / endoscopic endonasal extended transtuberculum] approach for resection of tuberculum sellae meningioma [with optic canal decompression]
Surgeon / Assistant: [± ENT co-surgeon if endonasal] Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Neuronavigation, high-speed drill (optic canal), microscope/endoscope, ICG; [lumbar drain if endonasal] Implants: Dural substitute [/ nasoseptal flap, fascia/fat, sealant if endonasal] Complications: None
Indications: [Age]yo [M/F] with a tuberculum sellae meningioma causing progressive visual decline (chiasmal compression, [junctional/bitemporal] field defect). Approach selected for [midline without vascular encasement → endonasal / lateral extension/vessel encasement → pterional]. Risks (visual worsening, ICA injury, CSF leak, endocrine) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and navigation registered. [Pterional: the head was rotated ~20–30° contralateral, a pterional craniotomy performed, the sphenoid wing drilled, and the basal cisterns opened with CSF egress to relax the brain. The ipsilateral optic nerve, ICA, and chiasm were identified.] The involved optic canal was unroofed to decompress and free the optic nerve.
The tumor base at the tuberculum/planum was devascularized, the tumor internally debulked, and the capsule dissected off the optic apparatus and chiasm, preserving the superior hypophyseal artery branches supplying the chiasm; the ACA complex, ICA, and stalk were protected. The involved dura/bone was addressed (Simpson [I/II]) and the skull base reconstructed [multilayer with nasoseptal flap if endonasal].
Closure was completed and the patient transferred to the ICU with serial visual checks.
Postoperative Plan
- ICU, neuro checks q1h, visual checks
- Endonasal: DI/Na monitoring, CSF leak precautions, AM cortisol
- MRI postop, ophthalmology and endocrine follow-up
- Steroid taper, DVT prophylaxis
Chief-Level Case Review
Use these as the senior-level mental model for Tuberculum Sellae Meningioma Resection:
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Tuberculum Sellae Meningioma Resection:
- What is the surgical goal: gross-total, maximal safe, decompression, diagnosis, or cytoreduction?
- What eloquent cortex, tract, cranial nerve, vessel, or sinus defines the stopping point?
- What adjunct changes the case: navigation, mapping, 5-ALA, ultrasound, endoscope, ICG, or neuromonitoring?
- What is the edema, steroid, seizure, DVT, and postop imaging plan?
- What complication would you check for first in PACU based on this lesion location?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Extent-of-resection goal and functional stopping points: [attending-specific]
- Mapping/monitoring, 5-ALA, ultrasound, ICG, endoscope, or tractography preferences: [attending-specific]
- Steroid, antiepileptic, mannitol/hypertonic saline, and antibiotic plan: [attending-specific]
- Postop MRI timing, ICU/floor threshold, and adjuvant-referral workflow: [attending-specific]