
Case Prep: Anterior Lumbar Interbody Fusion (ALIF)
Case / Approach Snapshot
- Anatomy at risk: level localization, cord/cauda equina, exiting and traversing roots, dura, vertebral artery or segmental vessels, esophagus/trachea/pleura/viscera by approach, and fusion/instrumentation landmarks.
- Operative steps: position and pad carefully, confirm level, expose the planned corridor, decompress neural elements, reconstruct or instrument when indicated, verify alignment/hardware, and close with attention to hematoma and wound risk; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: wrong level, durotomy, neurologic change, vertebral artery/visceral/pleural injury, graft or hardware problem, epidural hematoma, dysphagia/airway issue, and infection prevention/escalation.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [degenerative disc disease / spondylolisthesis / flat back / pseudarthrosis] at [L4-5 / L5-S1] planned for anterior lumbar interbody fusion [± posterior instrumentation].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Anterior lumbar interbody fusion: patient selection and workup — Barber SM. Journal of spine surgery (Hong Kong) 2024. PubMed
- Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF — Mobbs RJ. Journal of spine surgery (Hong Kong) 2015. PubMed
- Anterior lumbar interbody fusion — Burke PJ. Radiologic technology 2001. PubMed
- Animal Model for Anterior Lumbar Interbody Fusion: A Literature Review — Yoshizato H. Spine surgery and related research 2024. PubMed
- Expandable Cage Technology-Transforaminal, Anterior, and Lateral Lumbar Interbody Fusion — Macki M. Operative neurosurgery (Hagerstown, Md.) 2021. PubMed
- Lymphocele after anterior lumbar interbody fusion: a review of 1322 patients — Scheer JK. Journal of neurosurgery. Spine 2021. PubMed
- Minimally invasive anterior, lateral, and oblique lumbar interbody fusion: a literature review — Xu DS. Annals of translational medicine 2018. PubMed
- Transforaminal Versus Anterior Lumbar Interbody Fusion at L5-S1 for Degenerative Spine Disease : A Meta-Analysis — Daniels AH. Spine 2025. PubMed
- Anterior lumbar interbody fusion implants: a narrative review of current trends and future directions — Bayaton AJ. Journal of spine surgery (Hong Kong) 2025. PubMed
- Endoscopic Anterior Lumbar Interbody Fusion: Systematic Review and Meta-Analysis — Brown NJ. Asian spine journal 2023. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
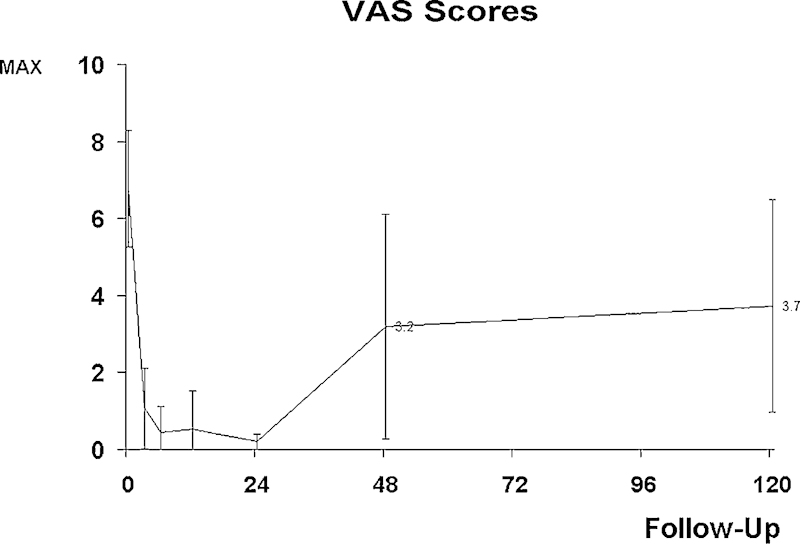 Figure 1. Visual analogue scale (VAS) scores of the study population during the 10-year follow-up. Source: Good Functional Outcome and Adjacent Segment Disc Quality 10 Years after Single-Level Anterior Lumbar Interbody Fusion with Posterior Fixation — Global Spine Journal 2012; open access.
Figure 1. Visual analogue scale (VAS) scores of the study population during the 10-year follow-up. Source: Good Functional Outcome and Adjacent Segment Disc Quality 10 Years after Single-Level Anterior Lumbar Interbody Fusion with Posterior Fixation — Global Spine Journal 2012; open access.
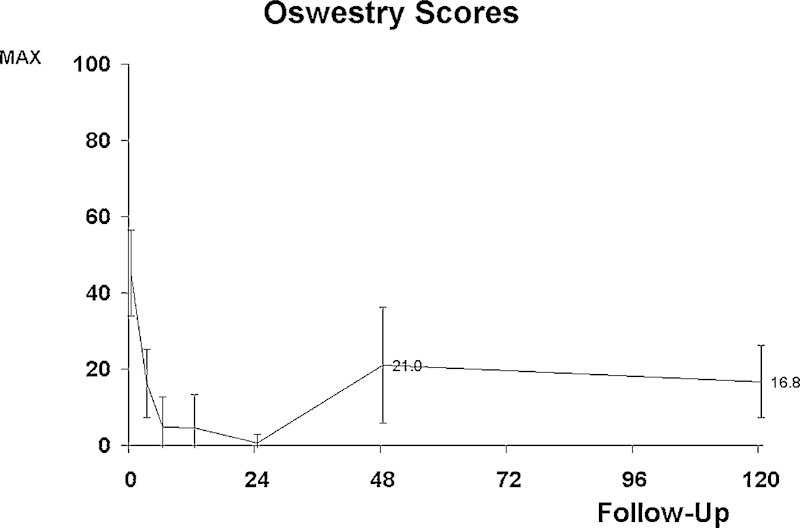 Figure 2. Oswestry Disability Index scores of the study population during the 10-year follow-up. Source: Good Functional Outcome and Adjacent Segment Disc Quality 10 Years after Single-Level Anterior Lumbar Interbody Fusion with Posterior Fixation — Global Spine Journal 2012; open access.
Figure 2. Oswestry Disability Index scores of the study population during the 10-year follow-up. Source: Good Functional Outcome and Adjacent Segment Disc Quality 10 Years after Single-Level Anterior Lumbar Interbody Fusion with Posterior Fixation — Global Spine Journal 2012; open access.
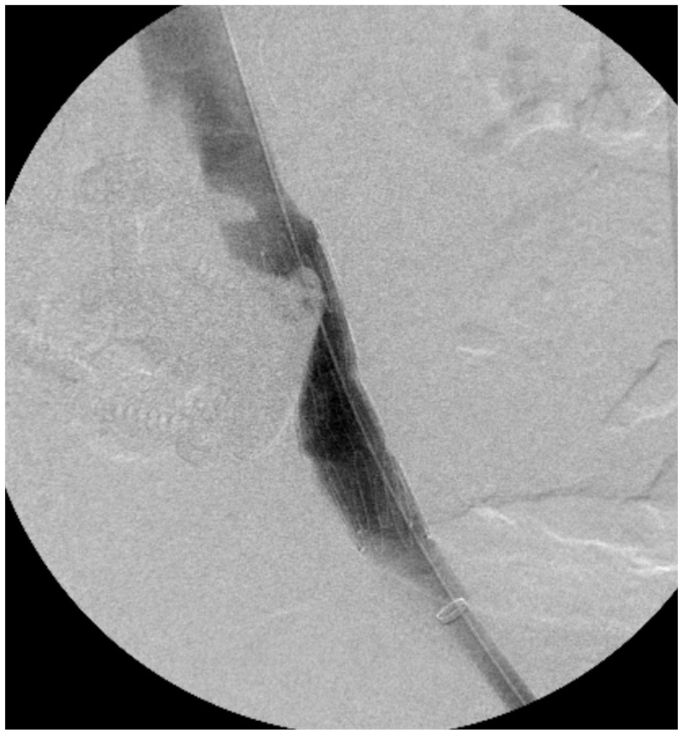 Fig 1. Intraoperative post deployment venogram demonstrates patent left common iliac vein (CIV). Source: Adjunctive endovascular stent graft reinforcement of the common iliac vein for safer anterior lumbar interbody fusion — Journal of Vascular Surgery Cases, Innovations and Techniques 2025; CC BY-NC-ND.
Fig 1. Intraoperative post deployment venogram demonstrates patent left common iliac vein (CIV). Source: Adjunctive endovascular stent graft reinforcement of the common iliac vein for safer anterior lumbar interbody fusion — Journal of Vascular Surgery Cases, Innovations and Techniques 2025; CC BY-NC-ND.
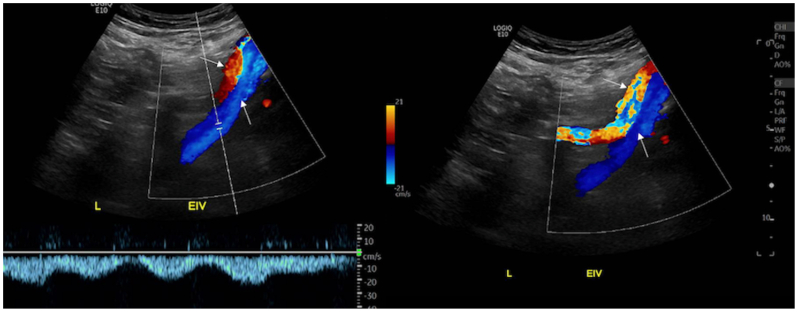 Fig 2. Postoperative lower extremity venous duplex ultrasound demonstrates good flow through the left common and external iliac vein. Normal venous Doppler waveform is shown on the left. Bottom… Source: Adjunctive endovascular stent graft reinforcement of the common iliac vein for safer anterior lumbar interbody fusion — Journal of Vascular Surgery Cases, Innovations and Techniques 2025; CC BY-NC-ND.
Fig 2. Postoperative lower extremity venous duplex ultrasound demonstrates good flow through the left common and external iliac vein. Normal venous Doppler waveform is shown on the left. Bottom… Source: Adjunctive endovascular stent graft reinforcement of the common iliac vein for safer anterior lumbar interbody fusion — Journal of Vascular Surgery Cases, Innovations and Techniques 2025; CC BY-NC-ND.
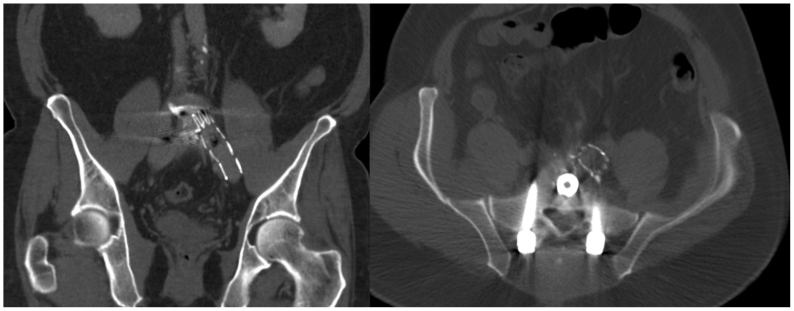 Fig 3. Coronal (left) and transverse (right) non-contrast computed tomography scans demonstrate left common iliac vein (CIV) stent with no hematoma in the retroperitoneum. Source: Adjunctive endovascular stent graft reinforcement of the common iliac vein for safer anterior lumbar interbody fusion — Journal of Vascular Surgery Cases, Innovations and Techniques 2025; CC BY-NC-ND.
Fig 3. Coronal (left) and transverse (right) non-contrast computed tomography scans demonstrate left common iliac vein (CIV) stent with no hematoma in the retroperitoneum. Source: Adjunctive endovascular stent graft reinforcement of the common iliac vein for safer anterior lumbar interbody fusion — Journal of Vascular Surgery Cases, Innovations and Techniques 2025; CC BY-NC-ND.
 Fig 4. Coronal (left) and sagittal (right) x-rays of lumbar spine demonstrate stable L5-S1 anterior lumbar interbody fusion (ALIF) and left common iliac vein (CIV) stent at 4-month follow-up. Source: Adjunctive endovascular stent graft reinforcement of the common iliac vein for safer anterior lumbar interbody fusion — Journal of Vascular Surgery Cases, Innovations and Techniques 2025; CC BY-NC-ND.
Fig 4. Coronal (left) and sagittal (right) x-rays of lumbar spine demonstrate stable L5-S1 anterior lumbar interbody fusion (ALIF) and left common iliac vein (CIV) stent at 4-month follow-up. Source: Adjunctive endovascular stent graft reinforcement of the common iliac vein for safer anterior lumbar interbody fusion — Journal of Vascular Surgery Cases, Innovations and Techniques 2025; CC BY-NC-ND.
 Figure 3.. Risk of total complications across comparative study in obese and normal BMI patients. Source: Obesity: An Independent Risk Factor for Complications in Anterior Lumbar Interbody Fusion? A Systematic Review — Global Spine Journal 2022; CC BY-NC-ND.
Figure 3.. Risk of total complications across comparative study in obese and normal BMI patients. Source: Obesity: An Independent Risk Factor for Complications in Anterior Lumbar Interbody Fusion? A Systematic Review — Global Spine Journal 2022; CC BY-NC-ND.
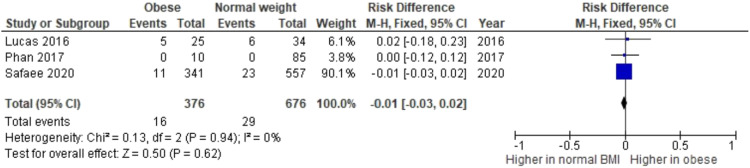 Figure 4.. Risk of vascular complications arising from each study group. Source: Obesity: An Independent Risk Factor for Complications in Anterior Lumbar Interbody Fusion? A Systematic Review — Global Spine Journal 2022; CC BY-NC-ND.
Figure 4.. Risk of vascular complications arising from each study group. Source: Obesity: An Independent Risk Factor for Complications in Anterior Lumbar Interbody Fusion? A Systematic Review — Global Spine Journal 2022; CC BY-NC-ND.
 Figure 9. Source: Obesity: An Independent Risk Factor for Complications in Anterior Lumbar Interbody Fusion? A Systematic Review — Global Spine J. 2022 Feb 22;12(8):1894–903. doi: 10.1177/21925682211072849; CC BY-NC-ND.
Figure 9. Source: Obesity: An Independent Risk Factor for Complications in Anterior Lumbar Interbody Fusion? A Systematic Review — Global Spine J. 2022 Feb 22;12(8):1894–903. doi: 10.1177/21925682211072849; CC BY-NC-ND.
 Figure 10. Source: Obesity: An Independent Risk Factor for Complications in Anterior Lumbar Interbody Fusion? A Systematic Review — Global Spine J. 2022 Feb 22;12(8):1894–903. doi: 10.1177/21925682211072849; CC BY-NC-ND.
Figure 10. Source: Obesity: An Independent Risk Factor for Complications in Anterior Lumbar Interbody Fusion? A Systematic Review — Global Spine J. 2022 Feb 22;12(8):1894–903. doi: 10.1177/21925682211072849; CC BY-NC-ND.
History of Present Illness
- Chief complaint: Axial low back pain (discogenic), deformity, or need for large interbody/lordosis restoration
- Failed conservative management
- ALIF advantages: large interbody footprint, excellent disc height/lordosis restoration, direct anterior column support, no posterior muscle dissection; ideal at L5-S1 and L4-5 (below bifurcation challenges)
Past Medical History
- Prior abdominal/retroperitoneal surgery (adhesions — access surgeon consideration)
- Vascular disease, prior DVT, males: retrograde ejaculation risk (superior hypogastric plexus — counsel)
- Single kidney, large vessel anatomy
- Standard PMH
Imaging Review
MRI/X-ray/CT
- Disc degeneration (Modic), alignment, lordosis, spondylolisthesis
- Vascular anatomy (MRI/CTA): great vessel bifurcation level, iliac vessels, left iliac vein course (L5-S1 in the bifurcation window; L4-5 requires mobilizing vessels)
- Sacral slope, pelvic parameters (deformity planning)
- Bone quality (osteoporosis → subsidence)
Labs
- CBC, BMP, Coags, Type and crossmatch (vascular injury risk), HbA1c
Neurological Examination
- Lower extremity exam, baseline; document for comparison
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: supine radiolucent table with C-arm access and vascular/retroperitoneal exposure setup.
- OR setup: radiolucent/Jackson table, fluoroscopy or O-arm/navigation, microscope/loupes for decompression, implant trays/graft ready for fusion, neuromonitoring for myelopathy/cord-risk cases, and postop brace plan confirmed.
- Special needs: arterial line/Foley/type-screen for long fusion/corpectomy, no long paralytic when MEPs are used, MAP/normotension for myelopathy or cord-risk cases, antibiotic redosing, and anticoagulation/DVT plan.
- Immediate postop orders: neuro checks by myotome/sensory level, airway/dysphagia watch for anterior cervical cases, CT/X-rays per construct, drain care, brace/activity orders, DVT prophylaxis timing, bowel regimen, and PT/OT mobilization.
Approach Team
- Access (vascular/general) surgeon typically performs the anterior retroperitoneal exposure; spine surgeon does discectomy/implant
Position
- OR table/bed: supine radiolucent table with C-arm access and vascular/retroperitoneal exposure setup.
- Supine on radiolucent table, slight Trendelenburg, arms out; fluoroscopy AP/lateral
Key Surgical Steps
- Anterior retroperitoneal approach (access surgeon): transverse or paramedian incision, develop retroperitoneal plane (left-sided), mobilize peritoneal contents medially
- Vessel mobilization: identify and protect great vessels; at L5-S1 work in the bifurcation window between iliac vessels; at L4-5 mobilize the left iliac vessels (ligate iliolumbar vein if needed); protect superior hypogastric plexus (presacral — use blunt dissection, avoid monopolar at L5-S1 → retrograde ejaculation)
- Confirm level (fluoroscopy), expose anterior annulus
- Complete discectomy: wide annulotomy, thorough disc removal, endplate preparation (preserve bony endplate)
- Release posterior annulus/PLL as needed for distraction/lordosis
- Trial and place large ALIF interbody (PEEK/titanium) packed with graft (allograft/autograft/BMP — BMP commonly used in ALIF but counsel re: risks); integrated screws or anterior buttress plate for fixation
- Restore disc height/segmental lordosis; confirm position on fluoroscopy
- Hemostasis, vessel re-inspection, closure (access surgeon)
- ± Staged/same-day posterior instrumentation (pedicle screws) for stability (esp. spondylolisthesis, multilevel, standalone insufficient)
Critical Anatomy & Structures at Risk
- Great vessels — aorta/IVC bifurcation, left common iliac vein (most commonly injured — torrential bleeding)
- Superior hypogastric plexus (presacral) — retrograde ejaculation in males (avoid monopolar at L5-S1)
- Ureter (left, retroperitoneal), sympathetic chain
- L5 nerve root (anteriorly at L5-S1), bowel/peritoneum
Equipment
- ALIF interbody implants + trials, anterior fixation (integrated screws/plate)
- Vascular instruments/retractors (access), fluoroscopy
- Bone graft/BMP, hemostatic agents, vascular repair capability/vascular surgery available
Monitoring
- SSEPs/EMG optional; vascular monitoring
Anesthesia
- Arterial line, large-bore IV/central access, crossmatched blood (vessel injury), vascular surgery backup, Foley
Potential Complications
- Vascular injury (iliac vein) — major hemorrhage; vascular repair
- Retrograde ejaculation (hypogastric plexus), sympathetic dysfunction (leg warmth/color change)
- Ileus, bowel/ureter injury, incisional hernia, DVT
- Subsidence, pseudarthrosis, implant migration, BMP-related complications (ectopic bone, swelling)
Operative Note Template
Preoperative Diagnosis: [Degenerative disc disease / spondylolisthesis / flatback] at [L4-5 / L5-S1]
Postoperative Diagnosis: Same
Procedure: Anterior lumbar interbody fusion at [L_-S_] [with integrated screws/anterior plate] [± posterior pedicle screw fixation]
Surgeon / Assistant: Spine + access (vascular/general) surgeon Anesthesia: General endotracheal EBL / Fluids / Blood products: [crossmatched; vascular repair available] Adjuncts: Fluoroscopy Implants: ALIF interbody (PEEK/Ti) + integrated screws/plate, bone graft [± BMP] Complications: None
Indications: [Age]yo [M/F] with [discogenic pain/spondylolisthesis] at [L_-S_] needing large interbody support and lordosis restoration. The anterior approach was chosen for direct anterior column access. Risks (vascular injury, retrograde ejaculation, ileus) discussed; males counseled re: retrograde ejaculation.
Description of Procedure: After consent and time-out, general anesthesia was induced with the patient supine. The access surgeon performed a retroperitoneal (left-sided) approach, mobilizing the peritoneal contents medially and protecting the great vessels [working in the bifurcation window at L5-S1 / mobilizing the left iliac vessels at L4-5], with blunt dissection over the L5-S1 disc to protect the superior hypogastric plexus (no monopolar). The level was confirmed.
A complete discectomy was performed with endplate preparation (preserving bony endplates). A large ALIF interbody packed with graft was sized, placed, and secured with integrated screws/plate, restoring disc height and segmental lordosis, confirmed on fluoroscopy. Vessels were re-inspected and hemostasis confirmed; the access surgeon closed the approach. [Posterior pedicle screw fixation was performed in the same/staged setting for added stability.]
The patient was transferred with distal pulse/vascular and neuro monitoring.
Postoperative Plan
- Floor/step-down, neuro and vascular checks (distal pulses, leg perfusion)
- Monitor for ileus (advance diet slowly), abdominal exam
- X-rays POD1, DVT prophylaxis (higher DVT risk — vessel manipulation)
- Activity, brace per surgeon, smoking cessation
- Counsel males re: retrograde ejaculation; follow-up for fusion (CT 6-12 months)
Chief-Level Case Review
Use these as the senior-level mental model for Anterior Lumbar Interbody Fusion (ALIF):
- Decision point: Localize twice and instrument once: numbering, transitional anatomy, prior hardware, rib count, navigation dataset, and fluoroscopic level confirmation are mandatory.
- Technical lever: Positioning is treatment: table choice, abdomen-free prone setup, alignment goals, shoulders/hips, eyes/plexus pressure, neuromonitoring baselines, and fluoroscopic access all change the case.
- Bailout: Protect neural elements by sequence: decompression before correction when needed, MAP support for cord risk, no long paralytic with MEPs, and immediate response to signal change.
- Postop watch: Finish with construct logic: decompression adequacy, screw purchase, alignment, fusion bed/graft, drain plan, brace/activity orders, postop CT/X-rays, and DVT timing.
Common Pimp Questions
Use these to pressure-test preparation for Anterior Lumbar Interbody Fusion (ALIF):
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]