
Case Prep: Lateral Lumbar Interbody Fusion (XLIF / OLIF)
Case / Approach Snapshot
- Anatomy at risk: level localization, cord/cauda equina, exiting and traversing roots, dura, vertebral artery or segmental vessels, esophagus/trachea/pleura/viscera by approach, and fusion/instrumentation landmarks.
- Operative steps: position and pad carefully, confirm level, expose the planned corridor, decompress neural elements, reconstruct or instrument when indicated, verify alignment/hardware, and close with attention to hematoma and wound risk; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: wrong level, durotomy, neurologic change, vertebral artery/visceral/pleural injury, graft or hardware problem, epidural hematoma, dysphagia/airway issue, and infection prevention/escalation.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [degenerative disc disease / scoliosis / spondylolisthesis / adjacent segment disease] at [L_-L_] planned for lateral (transpsoas XLIF / anterior-to-psoas OLIF) lumbar interbody fusion [± posterior fixation].
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Transpsoas lateral (LLIF/XLIF/OLIF) approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Lateral Lumbar Interbody Fusion — Taba HA. Neurosurgery clinics of North America 2020. PubMed
- Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF — Mobbs RJ. Journal of spine surgery (Hong Kong) 2015. PubMed
- Lateral lumbar interbody fusion in adult spine deformity - A review of literature — Batheja D. Journal of clinical orthopaedics and trauma 2021. PubMed
- Lateral Lumbar Interbody Fusion-Outcomes and Complications — Salzmann SN. Current reviews in musculoskeletal medicine 2017. PubMed
- The Evolution of Lateral Lumbar Interbody Fusion: A Journey from Past to Present — Wong AXJ. Medicina (Kaunas, Lithuania) 2024. PubMed
- Lateral Lumbar Interbody Fusion: Review of Surgical Technique and Postoperative Multimodality Imaging Findings — Wangaryattawanich P. AJR. American journal of roentgenology 2021. PubMed
- Lateral Lumbar Interbody Fusion — Pawar A. Asian spine journal 2015. PubMed
- Single Position Prone Lateral Lumbar Interbody Fusion: A Review of the Current Literature — Jacome FP. Current reviews in musculoskeletal medicine 2024. PubMed
- Lateral Lumbar Interbody Fusion: Indications, Outcomes, and Complications — Kwon B. The Journal of the American Academy of Orthopaedic Surgeons 2016. PubMed
- Subsidence Rates After Lateral Lumbar Interbody Fusion: A Systematic Review — Macki M. World neurosurgery 2019. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
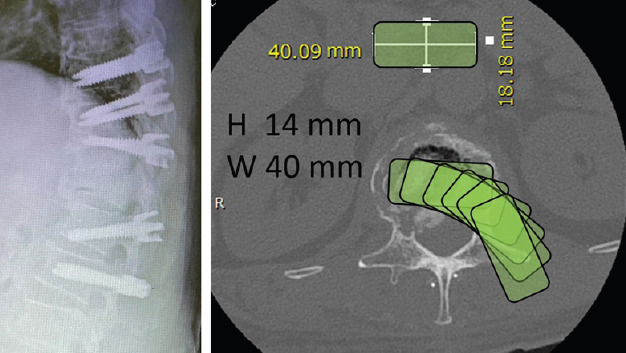 Figure 1. Pre-operative simulation in the PowerPoint® software and the first stage of the operation. The first stage involved pedicle screw insertion only without rod fixation. The pedicle screw… Source: Posterior Insertion of a Lateral Lumbar Interbody Fusion Cage for the Treatment of Osteoporotic Vertebral Fracture with Kyphotic Deformity: A Case Report — Journal of Orthopaedic Case Reports 2022; CC BY-NC-SA.
Figure 1. Pre-operative simulation in the PowerPoint® software and the first stage of the operation. The first stage involved pedicle screw insertion only without rod fixation. The pedicle screw… Source: Posterior Insertion of a Lateral Lumbar Interbody Fusion Cage for the Treatment of Osteoporotic Vertebral Fracture with Kyphotic Deformity: A Case Report — Journal of Orthopaedic Case Reports 2022; CC BY-NC-SA.
 Figure 8. Source: Posterior Insertion of a Lateral Lumbar Interbody Fusion Cage for the Treatment of Osteoporotic Vertebral Fracture with Kyphotic Deformity: A Case Report — J Orthop Case Rep. 2022 Apr;12(4):75–8. doi: 10.13107/jocr.2022.v12.i04.2774; CC BY-NC-SA.
Figure 8. Source: Posterior Insertion of a Lateral Lumbar Interbody Fusion Cage for the Treatment of Osteoporotic Vertebral Fracture with Kyphotic Deformity: A Case Report — J Orthop Case Rep. 2022 Apr;12(4):75–8. doi: 10.13107/jocr.2022.v12.i04.2774; CC BY-NC-SA.
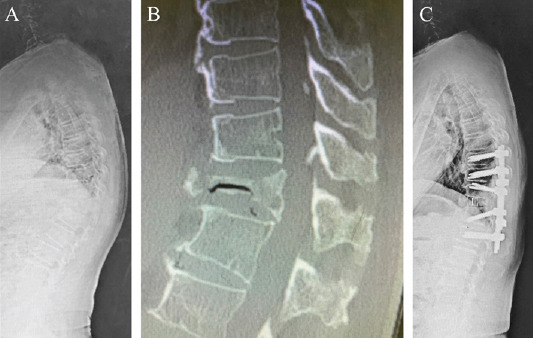 Figure 2. (a) Whole spine radiograph. (b) Computed tomography showing the unstable T11 fracture. (c) Whole spine standing radiograph 2 weeks postoperatively. The local kyphosis angle decreased… Source: Posterior Insertion of a Lateral Lumbar Interbody Fusion Cage for the Treatment of Osteoporotic Vertebral Fracture with Kyphotic Deformity: A Case Report — Journal of Orthopaedic Case Reports 2022; CC BY-NC-SA.
Figure 2. (a) Whole spine radiograph. (b) Computed tomography showing the unstable T11 fracture. (c) Whole spine standing radiograph 2 weeks postoperatively. The local kyphosis angle decreased… Source: Posterior Insertion of a Lateral Lumbar Interbody Fusion Cage for the Treatment of Osteoporotic Vertebral Fracture with Kyphotic Deformity: A Case Report — Journal of Orthopaedic Case Reports 2022; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Back/leg pain, deformity, need for indirect decompression and large interbody
- Failed conservative management
- Lateral approach advantages: large interbody (indirect decompression by restoring height/foraminal volume), minimal posterior disruption, good for deformity/coronal correction
- Levels: L1-2 through L4-5 (XLIF); L5-S1 not accessible via transpsoas (iliac crest/vessels) — OLIF L5-S1 possible via different corridor
Past Medical History
- Prior retroperitoneal/abdominal surgery, vascular disease
- Hip/iliac crest anatomy (limits access to L4-5), psoas anatomy
- Standard PMH
Imaging Review
MRI/X-ray/CT
- Disc/stenosis levels, alignment, coronal/sagittal deformity
- Vascular and psoas anatomy (axial MRI): great vessel position, lumbar plexus position within psoas (more posterior = safer corridor), “at-risk” levels (L4-5 plexus more anterior)
- Iliac crest height (L4-5 access), retroperitoneal anatomy
- Bone quality (subsidence risk)
Labs
- CBC, BMP, Coags, Type and screen, HbA1c
Neurological Examination
- Lower extremity exam, baseline hip flexion (psoas) and thigh sensation (genitofemoral/femoral) — approach can affect these
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: radiolucent lateral-decubitus table with iliac crest near the table break, true AP/lateral fluoroscopy, hips/knees flexed, and secure taping.
- OR setup: radiolucent/Jackson table, fluoroscopy or O-arm/navigation, microscope/loupes for decompression, implant trays/graft ready for fusion, neuromonitoring for myelopathy/cord-risk cases, and postop brace plan confirmed.
- Special needs: arterial line/Foley/type-screen for long fusion/corpectomy, no long paralytic when MEPs are used, MAP/normotension for myelopathy or cord-risk cases, antibiotic redosing, and anticoagulation/DVT plan.
- Immediate postop orders: neuro checks by myotome/sensory level, airway/dysphagia watch for anterior cervical cases, CT/X-rays per construct, drain care, brace/activity orders, DVT prophylaxis timing, bowel regimen, and PT/OT mobilization.
Position
- OR table/bed: radiolucent lateral-decubitus table with iliac crest near the table break, true AP/lateral fluoroscopy, hips/knees flexed, and secure taping.
- True lateral decubitus (typically right-side-up/left-side-down for left retroperitoneal approach), break the table to open the disc space/iliac-rib window, secure with tape, axillary roll, pad pressure points
- Fluoroscopy must give true AP and lateral (square the patient to the table)
Key Surgical Steps (XLIF — Transpsoas)
- Lateral fluoroscopic localization, mark disc trajectory
- Small lateral flank incision, blunt finger dissection through retroperitoneal space to the psoas (sweep peritoneum anteriorly)
- Transpsoas dilation with EMG-guided dilators — directional EMG to locate/avoid the lumbar plexus (advance through posterior-to-mid psoas at safe zone); place expandable retractor
- Confirm position on fluoroscopy (mid-disc, avoiding posterior plexus and anterior vessels)
- Discectomy with contralateral annular release, endplate prep (preserve endplate)
- Trial and place wide lateral interbody cage (spanning both lateral cortical apophyseal rings for support) packed with graft
- Restore disc/foraminal height (indirect decompression), correct coronal alignment
- OLIF variant: anterior-to-psoas corridor (between psoas and great vessels) — avoids traversing psoas/plexus but requires vessel retraction
- ± Lateral plate/screw or staged posterior pedicle screw fixation (often needed for stability)
- Closure
Critical Anatomy & Structures at Risk
- Lumbar plexus (within/posterior psoas) — femoral nerve, genitofemoral nerve → thigh weakness (hip flexion/knee extension), anterior thigh numbness/pain (especially L4-5); EMG monitoring essential
- Great vessels (aorta/IVC, segmental vessels) — anterior; OLIF retracts vessels
- Psoas muscle — transient hip flexor weakness/thigh pain (common, usually transient)
- Ureter, bowel, sympathetic chain (retroperitoneal)
- Subsidence (lateral cage on apophyseal ring — good support, but osteoporosis risk)
Equipment
- Lateral access/retractor system with EMG-directional dilators, neuromonitoring
- Lateral interbody cages + trials, graft, ± lateral plate
- Fluoroscopy, posterior pedicle screw set (if combined)
Monitoring
- EMG (free-run + triggered/directional — essential for psoas transit), MEP/SSEP for deformity
Anesthesia
- No paralytic (EMG), lateral positioning precautions, arterial line for deformity, type and screen
Potential Complications
- Lumbar plexus injury — thigh weakness (hip flexion, quads), numbness, pain (esp. L4-5); often transient psoas-related, but femoral nerve injury can be lasting
- Vascular injury, bowel/ureter injury
- Subsidence, cage migration, pseudarthrosis
- Ileus, incisional flank bulge/hernia, sympathetic changes
Operative Note Template
Preoperative Diagnosis: [Degenerative disc disease / scoliosis / adjacent segment disease] at [L_-L_]
Postoperative Diagnosis: Same
Procedure: Lateral lumbar interbody fusion ([XLIF transpsoas / OLIF anterior-to-psoas] at [L_-L_]) [± posterior pedicle screw fixation]
Surgeon / Assistant: Anesthesia: General endotracheal, no paralytic (EMG) EBL / Fluids: Adjuncts: Lateral access retractor with directional EMG dilators, fluoroscopy; neuromonitoring Implants: Lateral interbody cage, graft [± lateral plate; posterior screws] Complications: None
Indications: [Age]yo [M/F] with [pathology] at [L_-L_] amenable to indirect decompression via a large lateral interbody. Risks (lumbar plexus/thigh symptoms, vascular/visceral injury) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced (no paralytic for EMG) and the patient placed in true lateral decubitus with the table broken to open the disc space; true AP/lateral fluoroscopy was squared. A lateral flank incision was made and blunt retroperitoneal finger dissection carried to the psoas, sweeping the peritoneum anteriorly.
[XLIF: the psoas was traversed with EMG-directional dilators to locate and avoid the lumbar plexus, and the retractor docked mid-disc.] [OLIF: an anterior-to-psoas corridor between the psoas and great vessels was developed.] A discectomy with contralateral annular release and endplate preparation was performed, and a wide interbody cage spanning the apophyseal ring was placed with graft, restoring disc/foraminal height and coronal alignment. [Posterior pedicle screw fixation was added for stability.]
Closure was performed. The patient was transferred with documentation of hip-flexion/quad strength and thigh sensation (plexus).
Postoperative Plan
- Floor, neuro checks — document hip flexion strength, quad strength, thigh sensation (plexus)
- Counsel: transient thigh pain/numbness/hip flexor weakness common (usually resolves weeks-months)
- Mobilize POD0/1, X-rays, DVT prophylaxis
- Diet advance (ileus watch), activity/brace per surgeon
- Follow-up for fusion and plexopathy resolution
Chief-Level Case Review
Use these as the senior-level mental model for Lateral Lumbar Interbody Fusion (XLIF / OLIF):
- Decision point: Localize twice and instrument once: numbering, transitional anatomy, prior hardware, rib count, navigation dataset, and fluoroscopic level confirmation are mandatory.
- Technical lever: Positioning is treatment: table choice, abdomen-free prone setup, alignment goals, shoulders/hips, eyes/plexus pressure, neuromonitoring baselines, and fluoroscopic access all change the case.
- Bailout: Protect neural elements by sequence: decompression before correction when needed, MAP support for cord risk, no long paralytic with MEPs, and immediate response to signal change.
- Postop watch: Finish with construct logic: decompression adequacy, screw purchase, alignment, fusion bed/graft, drain plan, brace/activity orders, postop CT/X-rays, and DVT timing.
Common Pimp Questions
Use these to pressure-test preparation for Lateral Lumbar Interbody Fusion (XLIF / OLIF):
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]