
Operative Approach: Telovelar (Trans-Cerebellomedullary Fissure) Approach to the Fourth Ventricle
Case / Approach Snapshot
- Anatomy at risk: cerebellar tonsils, uvula/nodulus, tela choroidea, inferior medullary velum, taenia, choroid plexus, PICA tonsillomedullary/telovelotonsillar segments, fourth-ventricular floor nuclei, facial colliculus, hypoglossal/vagal trigones, lateral recess/foramen of Luschka, and CSF pathways.
- Operative steps: achieve posterior fossa relaxation, open the cerebellomedullary fissure without vermian splitting, incise tela choroidea along the taenia, extend through inferior medullary velum only as needed, map/protect the floor, debulk lesions away from the brainstem, preserve PICA/perforators, and close watertight with hydrocephalus planning.
- Rescue plans: swollen posterior fossa, hydrocephalus, PICA/choroidal bleeding, floor adherence, lower-cranial-nerve or facial-colliculus stimulation, cerebellar mutism risk, inadequate rostral/lateral recess exposure, CSF leak/pseudomeningocele, and postoperative airway/swallowing compromise.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas — posterior fossa · Rhoton fourth-ventricle anatomy (PMC) · Radiopaedia — medulloblastoma/ependymoma
High-Yield Literature
- Telovelar surgical approach — Ghali MGZ. Neurosurgical review 2021. PubMed
- Microsurgical anatomy of the fourth ventricle — Mercier P. Neuro-Chirurgie 2021. PubMed
- Anatomical Step-by-Step Dissection of Midline Suboccipital Approaches to the Fourth Ventricle for Trainees: Surgical Anatomy of the Telovelar, Transvermian, and Superior Transvelar Routes, Surgical Principles, and Illustrative Cases — Dang DD. Journal of neurological surgery. Part B, Skull base 2024. PubMed
- Microsurgical anatomy and surgical exposure of the cerebellar peduncles — Baran O. Neurosurgical review 2022. PubMed
- Fourth Ventricle Epidermoid Cyst: Case Report of Precision Telovelar Microsurgery, Functional Preservation, and Lifelong Surveillance — Costea D. Diagnostics (Basel, Switzerland) 2025. PubMed
- Neuroendoscopy improves operability and reduces hazardous vermian manipulation during the telovelar approach to the fourth ventricle’s floor: an anatomical study — Serrano Sponton L. Neurosurgical review 2026. PubMed
- Telovelar Approach for Fourth-Ventricular Epidermoid Cyst: Anatomical Respect, Functional Recovery, and Long-Term Stability — Pantu C. Diagnostics (Basel, Switzerland) 2026. PubMed
- Full-Endoscopic Minimally-Invasive Trans-Magendie Approach to the Fourth Ventricle: An Anatomical Feasibility Study — Leone A. World neurosurgery 2025. PubMed
- Telovelar approach for choroid plexus papilloma in the foramen of Luschka: a safe way using a neuromonitor — Lee CC. Clinical neurology and neurosurgery 2012. PubMed
- Subtonsillar and vallecular triangles as gateways to dorsal brainstem and fourth ventricle lesions: descriptive and quantitative analysis of microsurgical anatomy — Gurses ME. Neurosurgical review 2025. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
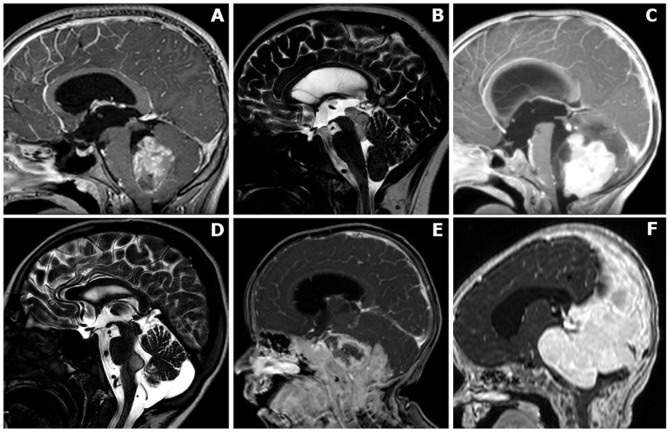 Figure 1. Anatomical classification of posterior fossa tumors requiring surgical access to the fourth ventricle. (A) Mainly/purely intraventricular, without evident brainstem infiltration or… Source: The Clinical and Prognostic Impact of the Choice of Surgical Approach to Fourth Ventricular Tumors in a Single-Center, Single-Surgeon Cohort of 92 Consecutive Pediatric Patients — Frontiers in Oncology 2022; CC BY.
Figure 1. Anatomical classification of posterior fossa tumors requiring surgical access to the fourth ventricle. (A) Mainly/purely intraventricular, without evident brainstem infiltration or… Source: The Clinical and Prognostic Impact of the Choice of Surgical Approach to Fourth Ventricular Tumors in a Single-Center, Single-Surgeon Cohort of 92 Consecutive Pediatric Patients — Frontiers in Oncology 2022; CC BY.
 Fig. 1. These sketches resume the cerebellomedullary fissure approaches upon the external surface of the fourth ventricle and shall be the map for designing the same dissection lines on the… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
Fig. 1. These sketches resume the cerebellomedullary fissure approaches upon the external surface of the fourth ventricle and shall be the map for designing the same dissection lines on the… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
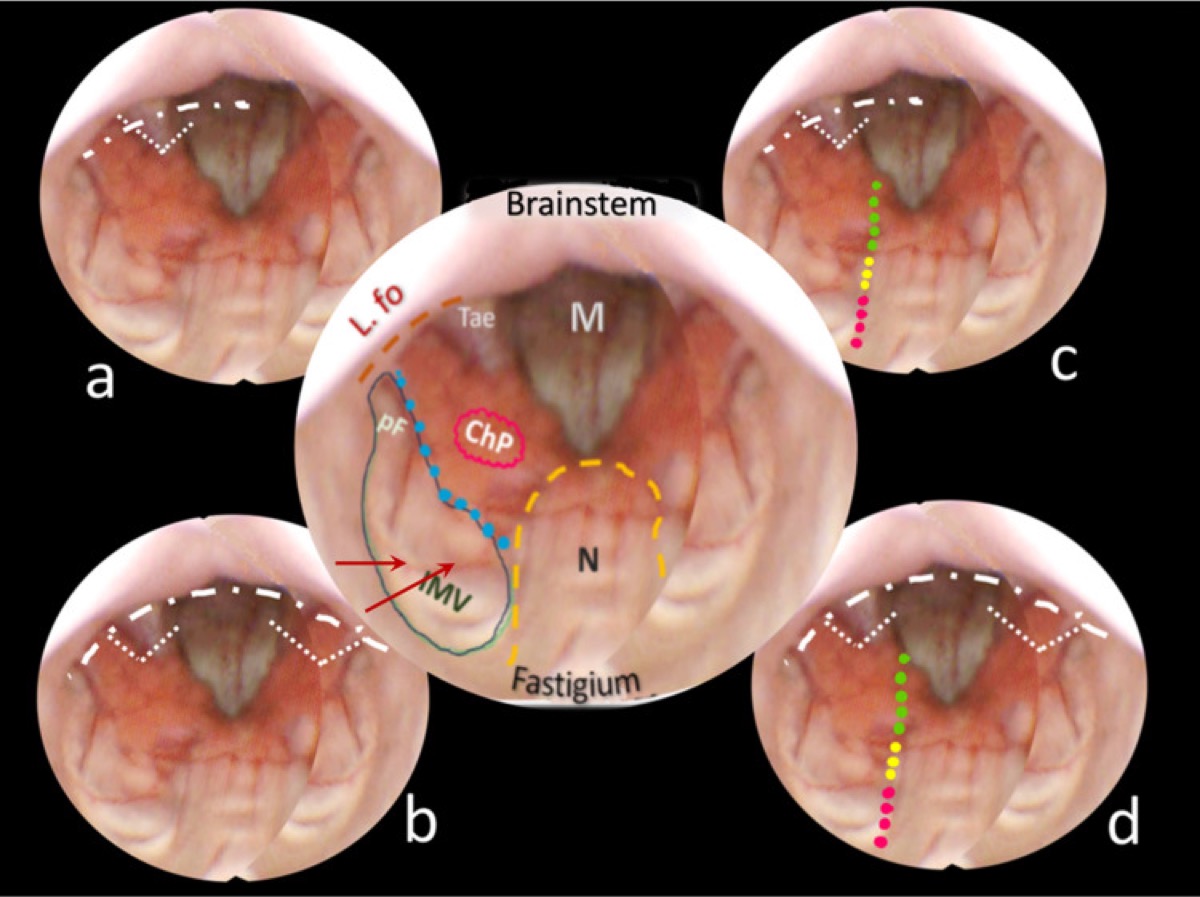
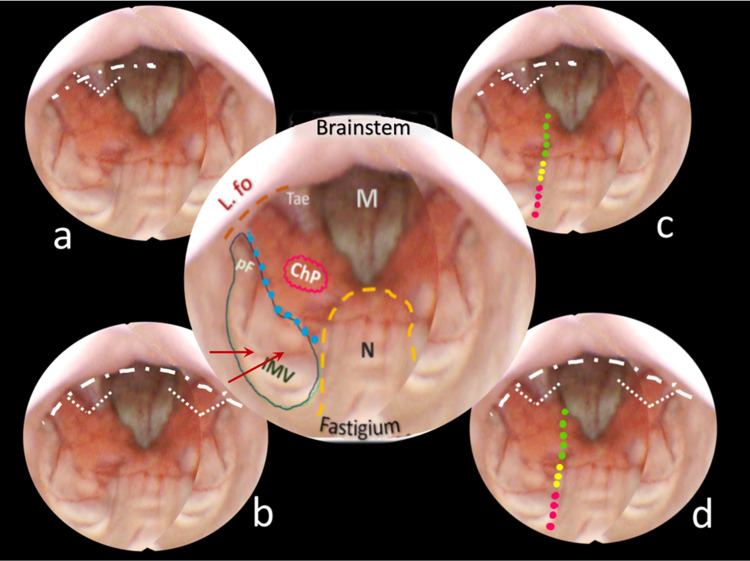 Fig. 2. Central round: an anatomical mapping of almost the entire fourth ventricle. The image is captured once the endoscopic camera tip has emerged from the aqueduct and is moving caudally. The… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
Fig. 2. Central round: an anatomical mapping of almost the entire fourth ventricle. The image is captured once the endoscopic camera tip has emerged from the aqueduct and is moving caudally. The… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
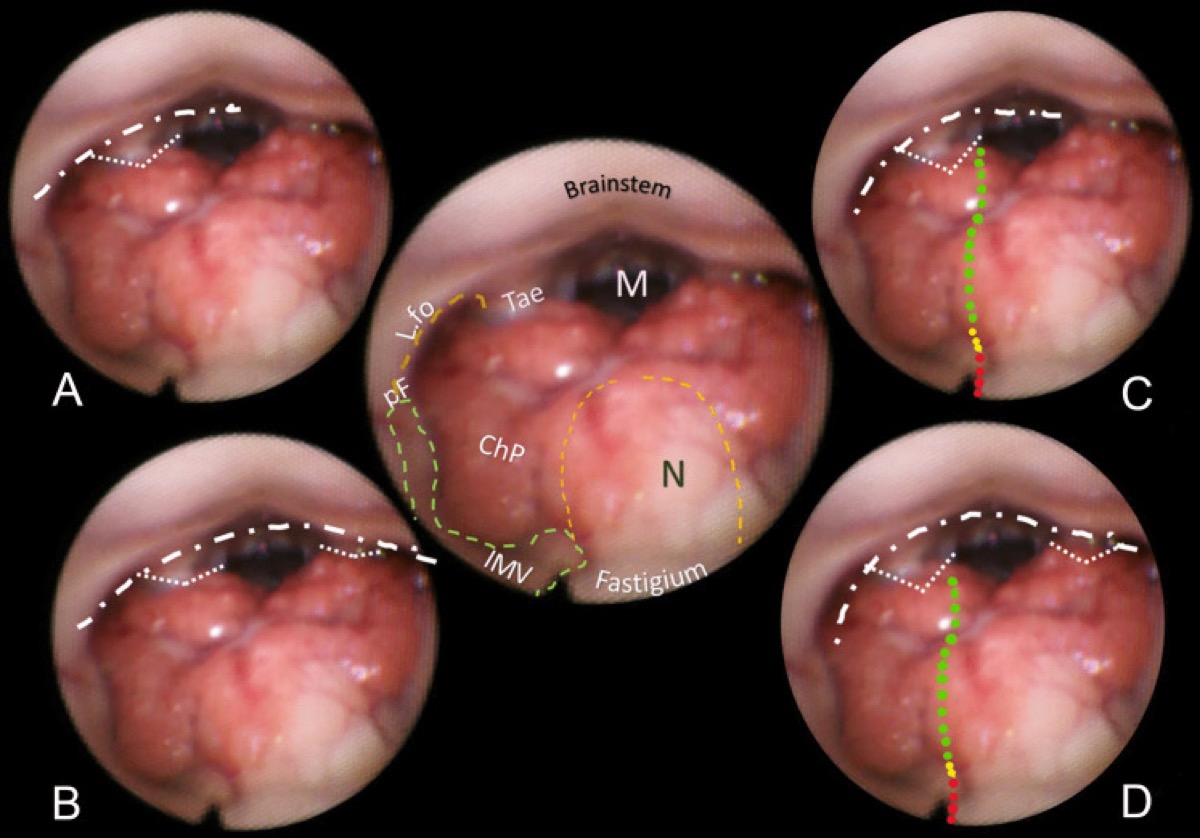
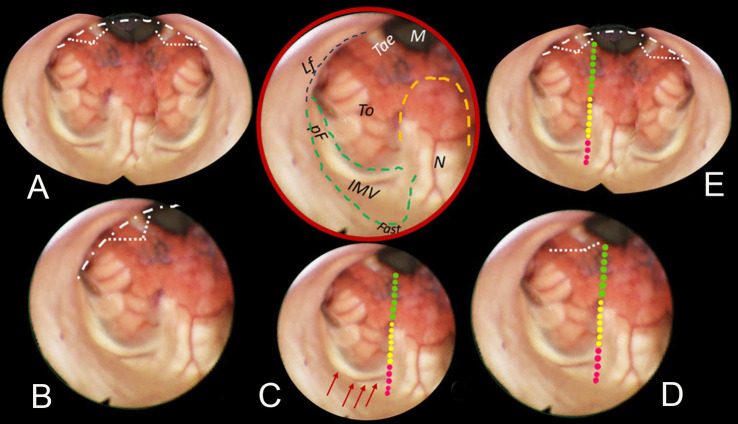 Fig. 3. Brown-bordered upper central round: anatomical perspective of almost the entire fourth ventricle. The nodulus (N, orange dashed line) and the inferior medullary velum (IMV, green dashed… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
Fig. 3. Brown-bordered upper central round: anatomical perspective of almost the entire fourth ventricle. The nodulus (N, orange dashed line) and the inferior medullary velum (IMV, green dashed… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
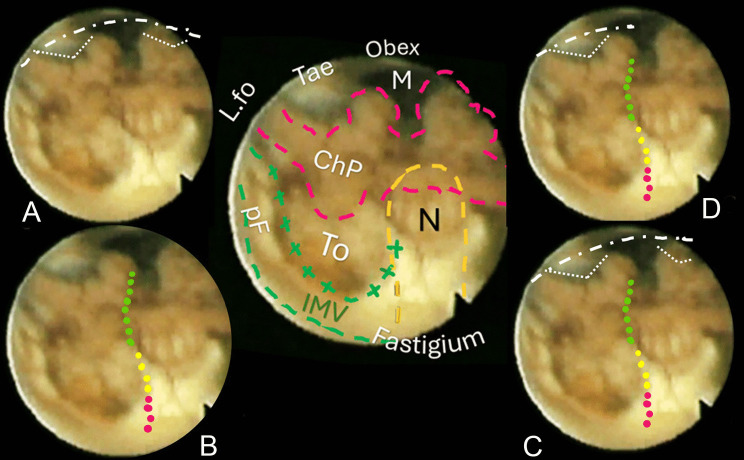 Fig. 4. Central sketch: anatomical morphology of the roof of the fourth ventricle. The nodulus (N, orange dashed line) lies caudal to the Fastigium, as well as the inferior medullary velum (IMV,… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
Fig. 4. Central sketch: anatomical morphology of the roof of the fourth ventricle. The nodulus (N, orange dashed line) lies caudal to the Fastigium, as well as the inferior medullary velum (IMV,… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
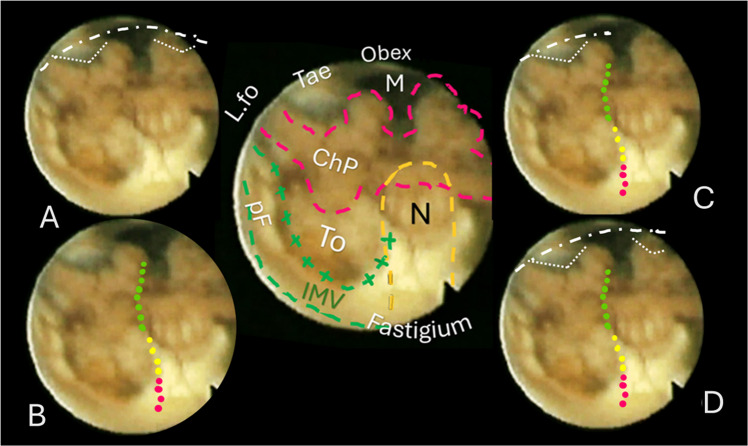 Fig. 5. The case of a normal pressure hydrocephalus. Ventricular distention caused an apparent downshift of the choroidal plexus and distension of the cranial part of the roof with enlargement… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
Fig. 5. The case of a normal pressure hydrocephalus. Ventricular distention caused an apparent downshift of the choroidal plexus and distension of the cranial part of the roof with enlargement… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
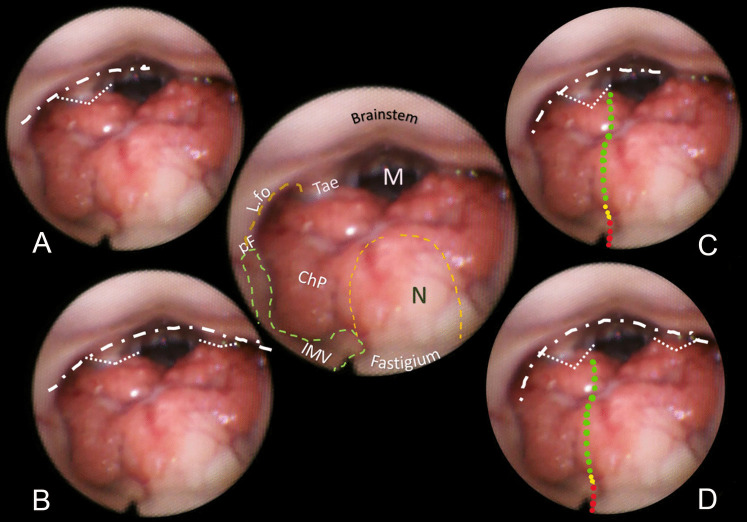 Fig. 6. Central round: view of a normal fourth ventricle after endoscopic aqueductoplasty in a 61-year-old man, and comparison with previous figures for anatomical morphology and shortcuts. A… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
Fig. 6. Central round: view of a normal fourth ventricle after endoscopic aqueductoplasty in a 61-year-old man, and comparison with previous figures for anatomical morphology and shortcuts. A… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
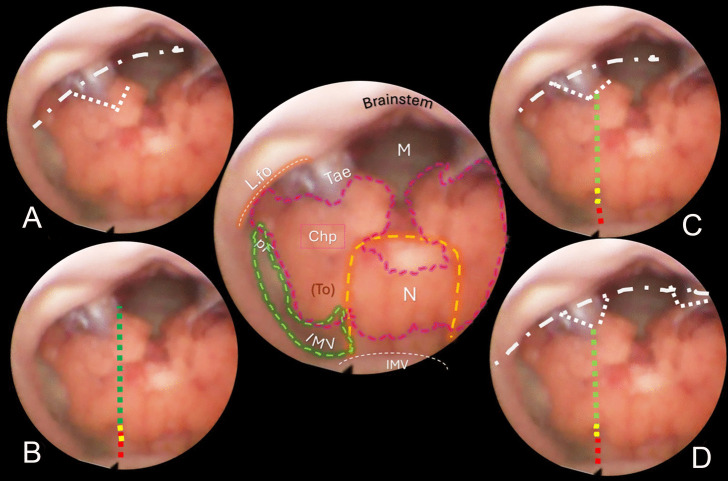 Fig. 7. Central round: shape of a normal fourth ventricle after endoscopic aqueductoplasty. The ventricular inferior roof is prevalently dwelt in by the choroid plexus (Chp) that reaches the… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
Fig. 7. Central round: shape of a normal fourth ventricle after endoscopic aqueductoplasty. The ventricular inferior roof is prevalently dwelt in by the choroid plexus (Chp) that reaches the… Source: The telovelar approach reshaped: a new perspective from inside the fourth ventricle — Child’s Nervous System 2026; CC BY.
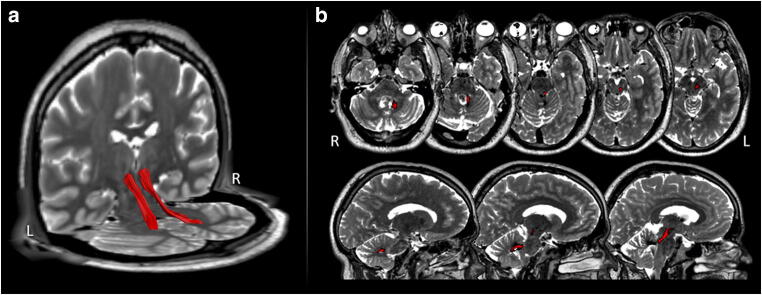 Fig. 3. Dentatorubrothalamic tract dissection: 3D (a) and 2D (b) dissection of the dentatorubrothalamic tracts (red) imposed on the patient’s T2 volumetric MRI Source: Medial-tonsillar telovelar approach for resection of a superior medullary velum cerebral cavernous malformation: anatomical and tractography study of the surgical approach and functional implications — Acta Neurochirurgica 2020; CC BY.
Fig. 3. Dentatorubrothalamic tract dissection: 3D (a) and 2D (b) dissection of the dentatorubrothalamic tracts (red) imposed on the patient’s T2 volumetric MRI Source: Medial-tonsillar telovelar approach for resection of a superior medullary velum cerebral cavernous malformation: anatomical and tractography study of the surgical approach and functional implications — Acta Neurochirurgica 2020; CC BY.
The telovelar approach reaches the entire fourth ventricle through the cerebellomedullary fissure — without splitting the vermis. By opening the tela choroidea (and, when more rostral reach is needed, the inferior medullary velum), the surgeon enters the ventricle along its natural roof, exposing the floor from the obex to the aqueduct and out to the lateral recess/foramen of Luschka. It has largely replaced the transvermian approach because sparing the vermis markedly reduces cerebellar mutism and ataxia.
General Considerations
- What it accesses: the whole fourth ventricle (floor from obex to aqueduct), the lateral recess and foramen of Luschka, and — via safe entry zones — the dorsal pons/medulla.
- The roof is the door, not the vermis. The fourth-ventricular roof has a lower membranous part (tela choroidea) and an upper neural part (inferior medullary velum). Opening the tela (± velum) on one or both sides exposes the ventricle without any vermian incision — the central advantage over the transvermian route.
- Graded opening: unilateral tela opening for caudal/floor lesions; add the inferior medullary velum and/or extend along the taenia/lateral recess for rostral or laterally extending tumors.
Indications
- Fourth-ventricular tumors — ependymoma, medulloblastoma, subependymoma, choroid plexus, pilocytic astrocytoma → pediatric posterior fossa tumor, posterior fossa tumor
- Dorsal pontine/medullary lesions via floor safe-entry zones (cavernoma, focal glioma)
- Lateral recess / foramen of Luschka lesions; rhomboid-fossa lesions
Approach Selection: Telovelar vs Alternatives
| Lesion pattern | Telovelar fit | Alternative |
|---|---|---|
| Fourth-ventricle tumor with caudal or midventricular origin | Best workhorse route | Transvermian rarely needed |
| Tumor reaching aqueduct/fastigium | Telovelar plus inferior medullary velum opening | Supracerebellar/infratentorial or occipital routes for pineal/aqueductal-dominant disease |
| Lateral recess / foramen of Luschka extension | Telovelar with lateral taenia/recess dissection | Retrosigmoid for predominantly CPA/lateral disease |
| Dorsal brainstem cavernoma at a safe-entry zone | Telovelar if lesion presents to fourth-ventricle floor | Far-lateral/retrosigmoid for lateral medullary/pontine presentation |
| Large vermian/cerebellar tumor | Midline suboccipital transcerebellar route | Telovelar only if fourth-ventricle component requires it |
The telovelar approach is not simply “posterior fossa exposure.” It is a deliberate fourth-ventricle roof opening; if the lesion is not intraventricular, dorsal brainstem, or lateral recess, choose the corridor that reaches the pathology without unnecessary floor exposure.
Relevant Surgical Anatomy
- Cerebellomedullary fissure: the cleft between the cerebellar tonsil/uvula above and the medulla below — the natural plane the approach develops.
- Fourth-ventricular roof: tela choroidea (lower, membranous, with choroid plexus) and inferior medullary velum (upper, between nodulus/uvula); the taenia is the line of attachment of the tela.
- Tonsil, uvula, nodulus (retracted, not resected); foramen of Magendie (median) and Luschka (lateral recess).
- PICA (telovelar/tonsillomedullary segments and choroidal branches) courses in the fissure — protect it.
- Floor (rhomboid fossa) safe zones: the facial colliculus, hypoglossal and vagal trigones, striae medullares mark cranial-nerve nuclei to avoid; entry through the suprafacial/infrafacial triangles or median sulcus as appropriate.

Telovelar approach reshaped, *Neurosurg Rev 2026 (PMC12963120) — CC BY 4.0. External cerebellomedullary-fissure dissection mapped to the internal fourth-ventricular anatomy.*
Telovelar approach reshaped, *Neurosurg Rev 2026 — CC BY 4.0. The tela choroidea and inferior medullary velum are the layers opened to enter the ventricle.*
Preoperative Evaluation
- MRI — tumor extent, floor involvement/adherence, rostral (aqueduct) and lateral-recess extension, brainstem invasion; hydrocephalus (very common with fourth-ventricular tumors).
- CTA / MRV for PICA and the venous sinuses; DTI if a brainstem safe-entry plan is needed.
- Hydrocephalus plan: preop EVD vs intraoperative ventricular access vs ETV; counsel re: postoperative shunt need (esp. medulloblastoma).
Floor-Risk Planning
- Identify whether tumor is merely displacing the floor or infiltrating/adherent to it; the floor-adherent portion sets the resection limit.
- Note facial colliculus distortion, lower medullary extension, obex involvement, aqueductal obstruction, and lateral recess extension.
- Review swallowing, voice, gag/cough, ocular motility, facial function, ataxia, and long-tract signs before surgery; small postoperative changes matter.
- Plan IONM electrodes for the actual risk: facial EMG, lower cranial nerves, MEP/SSEP, BAER, and direct floor mapping when floor work is expected.
- Discuss with ICU/anesthesia whether postoperative extubation is safe if lower cranial nerve dysfunction, brainstem edema, or long case swelling is likely.
Logistics, OR Setup & Orders
- OR setup: Mayfield, microscope/endoscope as needed, navigation, cranial nerve monitoring/BAER when relevant, Doppler/air-embolism readiness for sitting or semisitting positions, and watertight closure materials.
- Special needs: arterial line, Foley, antiemetic plan, dexamethasone when tumor/edema risk warrants it, EVD/CSF diversion plan, VAE monitoring when sitting, and lower-CN airway/swallow contingency.
- Immediate postop orders: posterior fossa neuro checks, CN V-XII and swallow/voice screen, HOB elevation, CT for hemorrhage/hydrocephalus when indicated, MRI for tumor EOR, CSF leak/pseudomeningocele watch, and nausea control.
Anesthesia & Neuromonitoring
- GA/TIVA; fourth-ventricular floor mapping, lower-CN EMG (IX/X, XII), facial EMG, SSEP/MEP, BAER. Arrhythmia/hemodynamic vigilance during floor manipulation. VAE precautions if a sitting position is used.
Positioning
- Prone “Concorde” (head flexed, slightly elevated) is the workhorse; sitting/semi-sitting is used by some for gravity drainage (VAE trade-off). Mayfield fixation; neck flexion opens the suboccipital–C1 interval and the cerebellomedullary fissure (avoid over-flexion / airway-ETT kinking and cervicomedullary compression).
Craniotomy
- Midline suboccipital craniotomy/craniectomy (± C1 arch removal for low/Magendie tumors and CSF access) — see midline suboccipital craniotomy. Open the dura in a Y/V, release CSF from the cisterna magna; the tonsils relax.
Telovelar Dissection (the approach proper)
- Retract the cerebellar tonsils laterally/superiorly (dynamic, not fixed) to open the cerebellomedullary fissure; identify the tela choroidea and the taenia.
- Incise the tela choroidea (unilateral or bilateral) along the taenia, coagulating the choroid plexus — this alone exposes the caudal floor and ventricle.
- For rostral exposure (toward the aqueduct), incise the inferior medullary velum; extend laterally along the recess toward Luschka for laterally projecting tumors. The entire floor up to the aqueduct is now exposed without a vermian split.
- Tumor work: internally debulk, define the tumor–floor plane, and protect the floor (no fixed retraction; map safe-entry zones); preserve PICA branches and floor perforators.
Exposure Extension Logic
- Caudal floor/obex lesion: wide foramen of Magendie and tela opening may be enough; avoid unnecessary rostral velum work.
- Rostral fourth ventricle/aqueduct: add inferior medullary velum opening and work upward under the nodulus with gentle dynamic retraction.
- Lateral recess/Luschka: follow the taenia laterally and protect PICA/choroidal branches; do not pull the tumor medially by force if the lower cranial nerves are stretched laterally.
- Bilateral tumor: open the fissure bilaterally rather than over-retracting one tonsil across the midline.
- Floor-adherent tumor: debulk and define the plane, then stop at unsafe adherence; staged adjuvant therapy beats a permanent brainstem deficit.
Intraoperative Rescue
- Bradycardia/hypertension/arrhythmia during floor work: stop manipulation immediately, irrigate, communicate with anesthesia, and resume only after mapping/orientation is clear.
- PICA injury: maintain visualization, control with gentle bipolar/clip only when needed, and preserve parent flow/perforators; blind coagulation in the fissure is dangerous.
- Loss of lower-CN/facial responses: pause, raise MAP, reduce traction, reassess floor anatomy, and leave adherent tumor if signals do not recover.
- Inadequate rostral exposure: extend velum opening or bone/C1 exposure thoughtfully; do not solve it by splitting vermis casually.
- Swollen posterior fossa: release CSF, optimize venous drainage/head position, consider EVD, and avoid fixed tonsillar retraction.
Closure
- Watertight dural closure (graft as needed), fat graft the suboccipital defect, wax air cells; replace bone (cranioplasty) when feasible. Manage hydrocephalus (EVD weaning, shunt if needed). Layered muscle closure to prevent pseudomeningocele/CSF leak.
Further operative anatomy & technique
Telovelar approach reshaped, Neurosurg Rev 2026 — CC BY 4.0.
Nuances & Pitfalls (surgeon-level)
- Spare the vermis — that is the entire point; the telovelar route avoids the vermian-split contribution to cerebellar mutism, though mutism can still occur with dentate/vermian/brainstem injury — counsel families (children).
- The floor is sacred. Tumor adherent to the floor is left rather than chased; never use fixed retraction on the rhomboid fossa; respect the facial colliculus and lower-CN trigones (floor mapping) — injury causes CN palsies, dysphagia, and hemodynamic instability.
- Protect PICA and its telovelar/choroidal branches in the fissure.
- Hydrocephalus is the rule — plan CSF diversion; watch for postoperative deterioration and the need for a shunt.
- Tonsillar retraction should be gentle/dynamic — over-retraction bruises the tonsils/PICA.
- Lateral recess/Luschka extension needs deliberate taenia dissection laterally — know where the lower cranial nerves exit.
Complications
Cerebellar mutism (less than transvermian) / ataxia; fourth-ventricular floor injury → CN VI/VII and lower-CN palsies, dysphagia, gaze palsy, hemodynamic instability; PICA injury; hydrocephalus / CSF leak / pseudomeningocele; pseudobulbar/respiratory issues; meningitis.
Cross-links
- Pathology: pediatric posterior fossa tumor · posterior fossa tumor
- Related corridors: midline-suboccipital-craniotomy.md · retrosigmoid-craniotomy.md · supracerebellar-infratentorial-approach.md
Figure Use & Attribution
About the figures. Copyrighted operative figures/videos are linked (Neurosurgical Atlas, Rhoton); embedded images are public-domain (Gray’s Anatomy) or CC‑BY (open-access), credited beneath each image. See media-sources.md and figures/CREDITS.md.
References: Neurosurgical Atlas — Suboccipital Craniotomy · Radiopaedia — fourth ventricle · PubMed Central — telovelar
Chief-Level Corridor Review
Use these as the senior-level mental model for Telovelar (Trans-Cerebellomedullary Fissure) Approach to the Fourth Ventricle:
- Decision point: Define the exposure goal before incision: target, working angles, proximal/distal control, and the structure that cannot tolerate retraction.
- Technical lever: Know the first irreversible step: bone removal, dural opening, vascular control, or muscle/fascial division that commits the corridor.
- Bailout: Verbalize the bailout: extend exposure, change trajectory, add CSF drainage, obtain proximal control, convert to a larger corridor, or stop for imaging.
- Postop watch: Protect closure from the start: vascularized tissue, watertight dural/reconstruction plan, dead-space control, and drain strategy should be chosen before the final intradural step.
Common Pimp Questions
Use these to pressure-test preparation for Telovelar (Trans-Cerebellomedullary Fissure) Approach to the Fourth Ventricle:
- What patient position and head rotation make gravity work for this corridor?
- What named nerve, vessel, sinus, or muscle/fascial plane is most commonly injured?
- What bone work or soft-tissue step creates the exposure rather than simply using more retraction?
- What is the bailout if exposure is inadequate, bleeding occurs, or the brain is tight?
- What closure maneuver prevents the signature complication of this approach?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Exact head rotation/flexion/extension and pin placement: [attending-specific]
- Skin incision length, flap type, and muscle/fascial preservation technique: [attending-specific]
- Drill, rongeur, endoscope, microscope, retractor, and navigation preferences: [attending-specific]
- Drain use, closure materials, watertightness threshold, and postop imaging routine: [attending-specific]
Case Guides Using This Approach
References
- Mussi AC, Rhoton AL Jr. Telovelar approach to the fourth ventricle: microsurgical anatomy. J Neurosurg. 2000;92(5):812–823.
- Matsushima T, Rhoton AL Jr, et al. Microsurgical anatomy of the cerebellomedullary fissure.
- Tanriover N, et al. Comparison of the transvermian and telovelar approaches to the fourth ventricle.
- Deshmukh VR, et al. Quantification and comparison of telovelar and transvermian approaches. Neurosurgery. 2006.
- The telovelar approach reshaped: a new perspective from inside the fourth ventricle. Neurosurg Rev. 2026. CC BY 4.0. (figures embedded above) — PMC12963120