
Case Prep: Posterior Fossa Tumor Resection (Cerebellar — Metastasis / Hemangioblastoma / Medulloblastoma / Ependymoma)
Case / Approach Snapshot
- Anatomy at risk: tumor compartment, arterial supply, venous drainage/sinuses, cranial nerves, white-matter tracts, pituitary/CSF pathways when relevant, and functional cortex.
- Operative steps: review imaging and goals, choose exposure, obtain brain relaxation, devascularize when possible, debulk internally, dissect capsule from critical structures, verify extent/safety, and reconstruct watertight closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: venous or arterial injury, swelling, seizure, cranial nerve or endocrine change, CSF leak, residual tumor left for safety, staged surgery, radiation, or adjuvant therapy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [left/right/midline/vermian/4th ventricular] posterior fossa [metastasis / hemangioblastoma / medulloblastoma / ependymoma] [with hydrocephalus] presenting with [headache / ataxia / nausea/vomiting] planned for suboccipital craniotomy for resection.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Telovelar approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Posterior Fossa Tumor Rehabilitation: An Up-to-Date Overview — Chieffo DPR. Children (Basel, Switzerland) 2022. PubMed
- Posterior Fossa Tumors — Brandão LA. Neuroimaging clinics of North America 2017. PubMed
- Prevalence of dysphagia following posterior fossa tumor resection: a systematic review and meta‑analysis — Duan Y. BMC cancer 2024. PubMed
- Intraoperative neurophysiology in posterior fossa tumor surgery in children — Sala F. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2015. PubMed
- Cerebellar liponeurocytoma: Rare posterior fossa tumor — Chaouche I. Radiology case reports 2024. PubMed
- Posterior fossa tumors in children: Radiological tips & tricks in the age of genomic tumor classification and advance MR technology — Kerleroux B. Journal of neuroradiology = Journal de neuroradiologie 2020. PubMed
- A review of long-term deficits in memory systems following radiotherapy for pediatric posterior fossa tumor — Baudou E. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology 2022. PubMed
- Craniotomy versus craniectomy in posterior fossa tumor surgery: A systematic review and Meta-Analysis — Correa EM. Neurosurgical review 2025. PubMed
- Postoperative facial palsy after pediatric posterior fossa tumor resection — Chu JK. Journal of neurosurgery. Pediatrics 2021. PubMed
- Cerebellar Mutism Syndrome After Posterior Fossa Tumor Surgery in Children-A Retrospective Single-Center Study — Schmidt S. World neurosurgery 2023. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
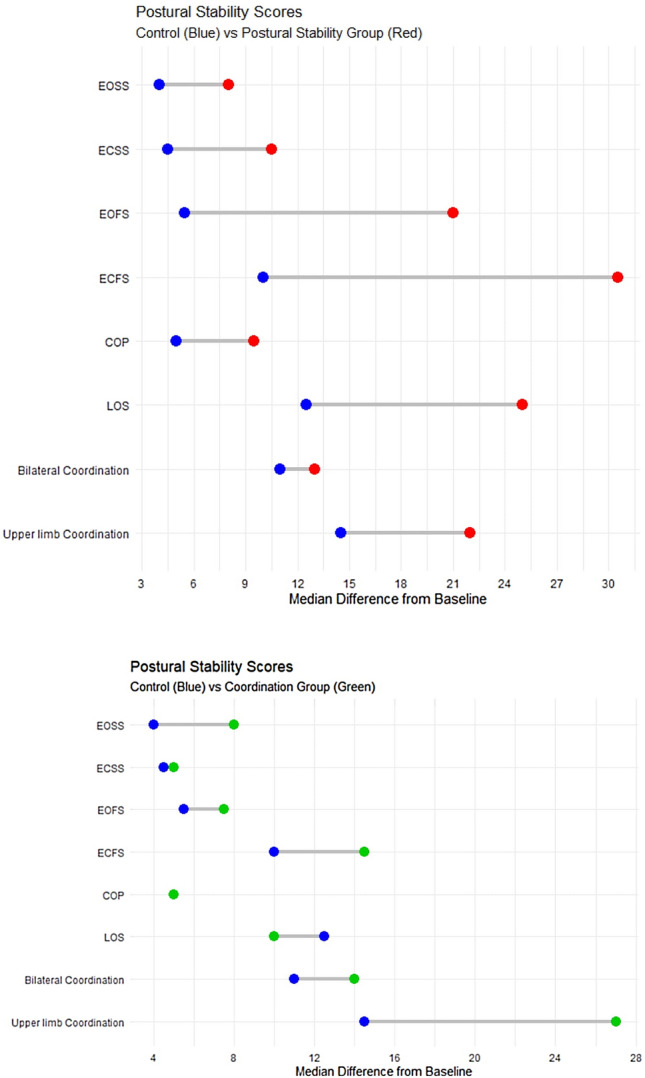 Fig. 2. Postural stability and coordination scores Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — Journal of Cancer Research and Clinical Oncology 2022; CC BY.
Fig. 2. Postural stability and coordination scores Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — Journal of Cancer Research and Clinical Oncology 2022; CC BY.
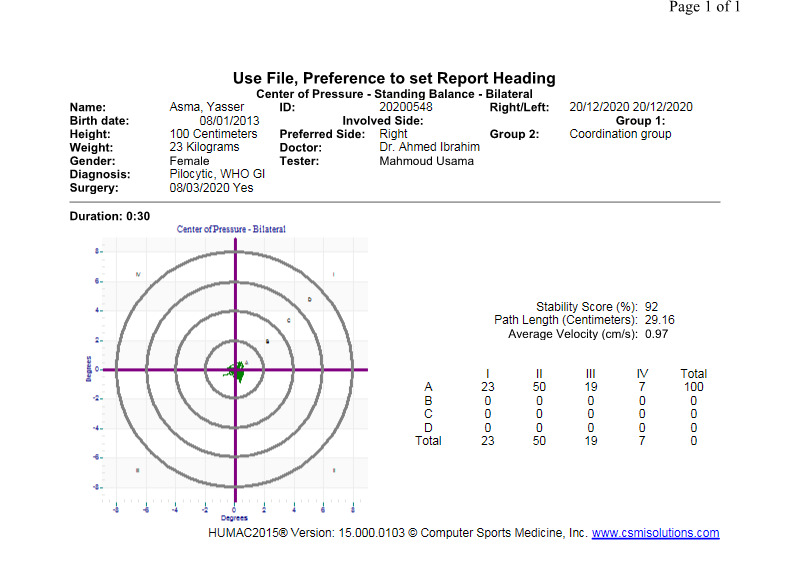 Figure 3. Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — J Cancer Res Clin Oncol. 2022 Dec 16;149(9):5637–44. doi: 10.1007/s00432-022-04490-4; CC BY.
Figure 3. Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — J Cancer Res Clin Oncol. 2022 Dec 16;149(9):5637–44. doi: 10.1007/s00432-022-04490-4; CC BY.
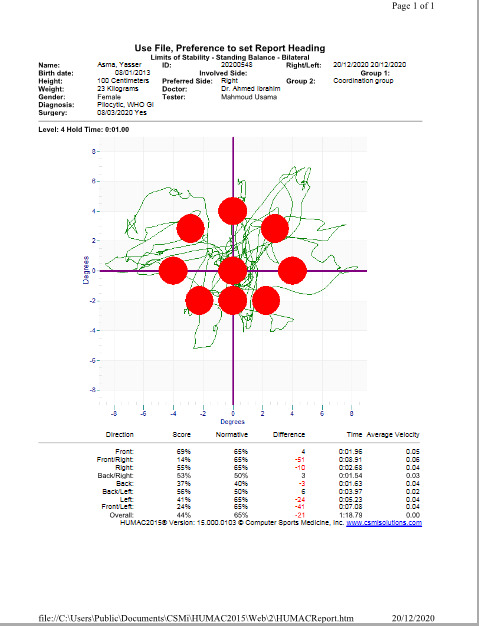 Figure 4. Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — J Cancer Res Clin Oncol. 2022 Dec 16;149(9):5637–44. doi: 10.1007/s00432-022-04490-4; CC BY.
Figure 4. Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — J Cancer Res Clin Oncol. 2022 Dec 16;149(9):5637–44. doi: 10.1007/s00432-022-04490-4; CC BY.
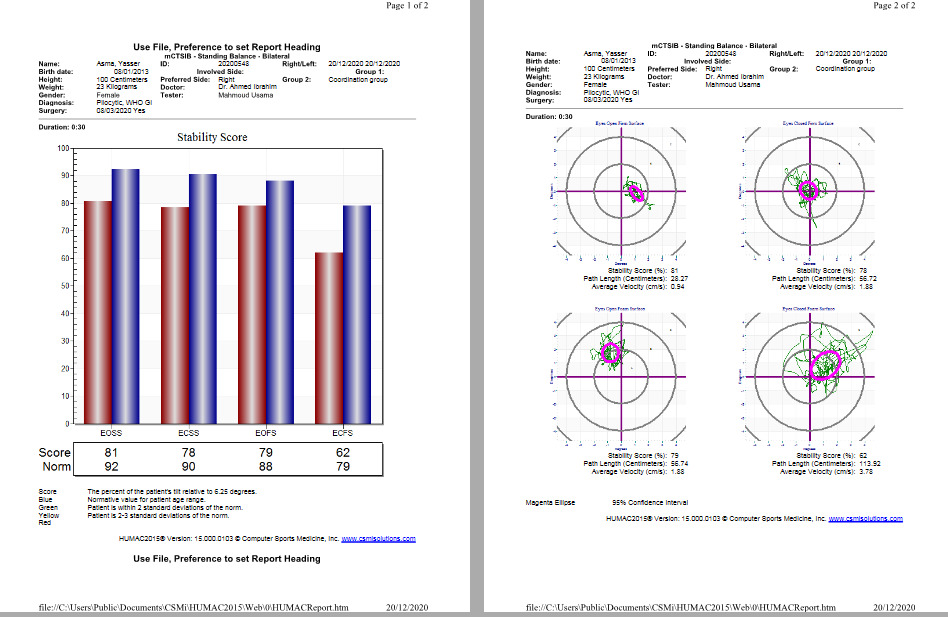 Figure 5. Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — J Cancer Res Clin Oncol. 2022 Dec 16;149(9):5637–44. doi: 10.1007/s00432-022-04490-4; CC BY.
Figure 5. Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — J Cancer Res Clin Oncol. 2022 Dec 16;149(9):5637–44. doi: 10.1007/s00432-022-04490-4; CC BY.
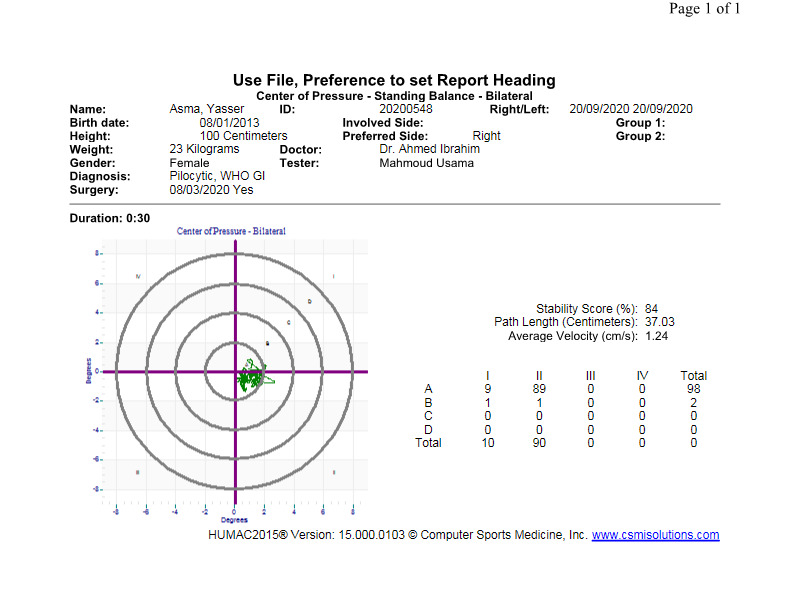 Figure 6. Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — J Cancer Res Clin Oncol. 2022 Dec 16;149(9):5637–44. doi: 10.1007/s00432-022-04490-4; CC BY.
Figure 6. Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — J Cancer Res Clin Oncol. 2022 Dec 16;149(9):5637–44. doi: 10.1007/s00432-022-04490-4; CC BY.
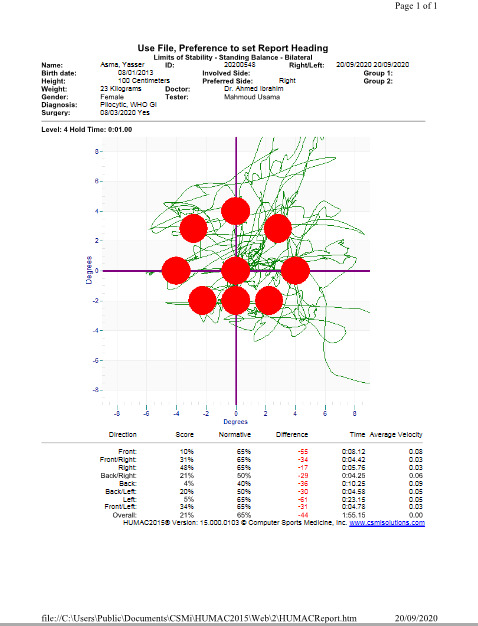 Figure 7. Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — J Cancer Res Clin Oncol. 2022 Dec 16;149(9):5637–44. doi: 10.1007/s00432-022-04490-4; CC BY.
Figure 7. Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — J Cancer Res Clin Oncol. 2022 Dec 16;149(9):5637–44. doi: 10.1007/s00432-022-04490-4; CC BY.
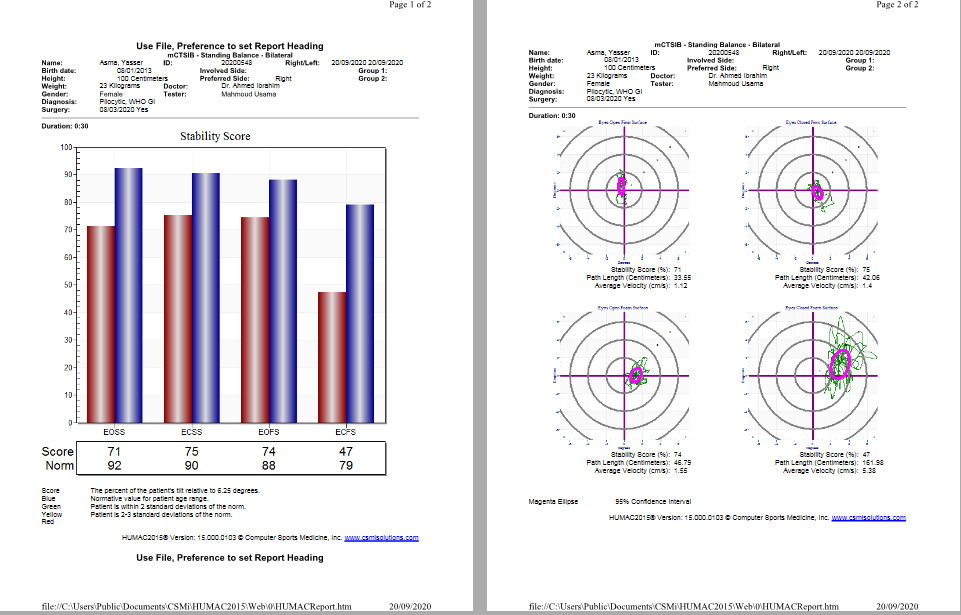 Figure 8. Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — J Cancer Res Clin Oncol. 2022 Dec 16;149(9):5637–44. doi: 10.1007/s00432-022-04490-4; CC BY.
Figure 8. Source: Impact of physical activity on postural stability and coordination in children with posterior fossa tumor: randomized control phase III trial — J Cancer Res Clin Oncol. 2022 Dec 16;149(9):5637–44. doi: 10.1007/s00432-022-04490-4; CC BY.
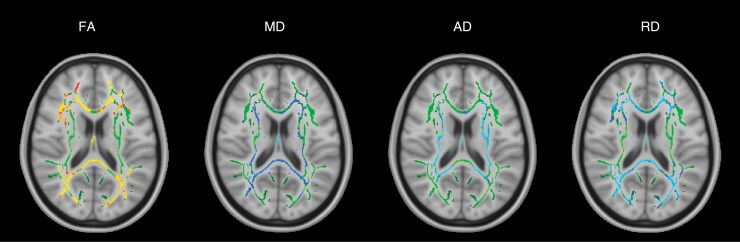 Figure 1.. TBSS results for the group of all 8 posterior fossa tumor patients at the presurgical time point. Green denotes the white matter skeleton where voxels are not significantly different… Source: Evidence of supratentorial white matter injury prior to treatment in children with posterior fossa tumors using diffusion MRI — Neuro-Oncology Advances 2025; CC BY.
Figure 1.. TBSS results for the group of all 8 posterior fossa tumor patients at the presurgical time point. Green denotes the white matter skeleton where voxels are not significantly different… Source: Evidence of supratentorial white matter injury prior to treatment in children with posterior fossa tumors using diffusion MRI — Neuro-Oncology Advances 2025; CC BY.
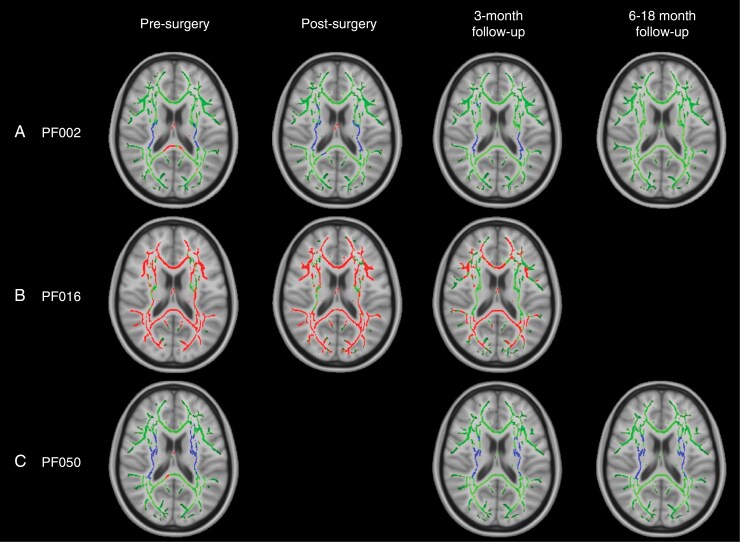 Figure 2.. TBSS results for individual patients with widespread, significant changes in FA, including pilocytic astrocytoma patients PF002 (A) and PF016 (B) and medulloblastoma patient PF050 (C)…. Source: Evidence of supratentorial white matter injury prior to treatment in children with posterior fossa tumors using diffusion MRI — Neuro-Oncology Advances 2025; CC BY.
Figure 2.. TBSS results for individual patients with widespread, significant changes in FA, including pilocytic astrocytoma patients PF002 (A) and PF016 (B) and medulloblastoma patient PF050 (C)…. Source: Evidence of supratentorial white matter injury prior to treatment in children with posterior fossa tumors using diffusion MRI — Neuro-Oncology Advances 2025; CC BY.
History of Present Illness
- Chief complaint: Headache (often morning, raised ICP), nausea/vomiting, ataxia, dysmetria, gait instability
- Hydrocephalus from 4th ventricle/aqueduct obstruction — may need preop CSF diversion
- Tumor type clues: hemangioblastoma (cyst + mural nodule, VHL, polycythemia), metastasis (known primary), medulloblastoma/ependymoma (children, 4th ventricle)
Imaging Review
MRI (T1±Gad, T2, FLAIR, DWI) + spine (if medullo/ependymoma — drop mets)
- Location: hemispheric, vermian, 4th ventricular, CPA
- Enhancement, cyst + nodule (hemangioblastoma), restricted diffusion (medulloblastoma)
- 4th ventricle/brainstem relationship, extension through foramina (Luschka/Magendie)
- Hydrocephalus, tonsillar herniation
- Vascular flow voids (hemangioblastoma — consider angiography/embolization)
CT
- Hydrocephalus, calcification, acute bleed
Workup
- VHL evaluation (hemangioblastoma), primary search (metastasis), neuraxis MRI (embryonal/ependymal)
Labs
- CBC (polycythemia in hemangioblastoma), BMP, Coags, Type and crossmatch
Neurological Examination
- Cerebellar (appendicular + truncal), CN exam, gait, papilledema, lower CN function (4th ventricle floor)
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: Mayfield, navigation, microscope/endoscope, cranial nerve monitoring/BAER when relevant, EVD/CSF diversion plan, watertight closure and fat/fascia graft materials, and blood available for vascular tumors.
- Special needs: arterial line, Foley, dexamethasone for edema, antiemetic plan, lower-CN airway/swallow contingency, EVD/ETV plan for hydrocephalus, and audiology/facial-nerve baseline when relevant.
- Immediate postop orders: ICU neuro checks, CN/eye movement/facial/swallow/voice exams, HOB 30, CT for hemorrhage/hydrocephalus, MRI for EOR, CSF-leak/pseudomeningocele watch, dex taper, and early swallow/ENT consult when lower CN risk exists.
Hydrocephalus Management
- Preop EVD or intraop ventriculostomy if significant hydrocephalus; some place EVD at start of case; ETV alternative; avoid rapid overdrainage (upward herniation risk)
Position
- Prone (most common) or Concorde/sitting (sitting: gravity retraction, less bleeding pooling, but VAE risk); Mayfield, neck flexed (2 fingerbreadths chin-to-sternum), shoulders taped down
Approach: Midline (or paramedian) Suboccipital Craniotomy ± C1 laminectomy
Key Surgical Steps
- Midline incision inion to C2, avascular midline raphe
- Suboccipital craniotomy; C1 laminectomy if tonsillar/4th ventricular extension
- Open dura (Y-shaped), watch for occipital sinus bleeding
- Telovelar approach to 4th ventricle (through cerebellomedullary fissure — avoids vermian split) for 4th ventricular tumors
- Tumor resection:
- Metastasis: circumferential, en bloc when possible (less seeding)
- Hemangioblastoma: do NOT enter the vascular nodule — circumferential dissection, coagulate feeders, remove nodule en bloc (drain cyst, resect nodule); AVM-like bleeding if entered
- Medulloblastoma/ependymoma: internal debulking, dissect off 4th ventricle floor (do not pursue tumor adherent to floor — brainstem injury), preserve PICA
- Restore CSF pathways
- Watertight dural closure (CSF leak/pseudomeningocele common in posterior fossa)
Critical Anatomy & Structures at Risk
- Brainstem / floor of 4th ventricle — CN nuclei (facial colliculus, hypoglossal/vagal trigones); injury → CN palsies, cardiorespiratory instability
- PICA and branches
- Cerebellar peduncles (ataxia, mutism)
- Vermis (truncal ataxia; posterior fossa/cerebellar mutism syndrome in children)
- Occipital sinus, transverse/sigmoid sinuses, torcula
Equipment
- Microscope, navigation, CUSA, ICG (hemangioblastoma)
- EVD kit, bipolar, hemostatic agents, dural substitute
- Preop embolization (vascular hemangioblastoma)
Monitoring
- SSEPs, MEPs, CN EMG (VII, IX-XII), BAER; precordial Doppler if sitting
Anesthesia
- Arterial line, crossmatched blood, VAE precautions if sitting (Doppler, central line, end-tidal CO2), antiemetics, mannitol
Potential Complications
- Posterior fossa syndrome / cerebellar mutism (children, vermian/dentate)
- CN deficits, swallowing/airway compromise (4th ventricle floor)
- Hydrocephalus persistence → shunt
- CSF leak/pseudomeningocele
- Hemorrhage (hemangioblastoma), VAE (sitting), aseptic meningitis
Operative Note Template
Preoperative Diagnosis: [Midline/hemispheric/4th-ventricular] posterior fossa [metastasis / hemangioblastoma / medulloblastoma / ependymoma] [with obstructive hydrocephalus]
Postoperative Diagnosis: Same
Procedure: Suboccipital craniotomy [with C1 laminectomy] for resection of posterior fossa tumor [with EVD placement]
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids / Blood products: [crossmatched] Adjuncts: Neuronavigation, CUSA, ICG (hemangioblastoma), SSEP/MEP/CN EMG/BAER, [VAE precautions if sitting] Implants: Dural substitute; [EVD] Complications: None
Indications: [Age]yo [M/F] with a [location] posterior fossa tumor and [obstructive hydrocephalus]. [Preoperative embolization was performed for the vascular hemangioblastoma.] Risks/benefits/alternatives discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and the patient positioned prone (Concorde) [/ sitting with VAE precautions] in Mayfield with the neck flexed. [An EVD was placed for hydrocephalus.] A midline suboccipital incision was made, the avascular raphe followed, and a suboccipital craniotomy performed [with C1 laminectomy for 4th-ventricular/tonsillar extension]; the occipital sinus was controlled.
The dura was opened and CSF released for relaxation. [The 4th ventricle was accessed via a telovelar approach through the cerebellomedullary fissure, avoiding a vermian split.] The tumor was resected [tumor-specific: cyst drained and mural nodule removed en bloc for pilocytic; vascular nodule circumferentially devascularized and removed en bloc without entering it for hemangioblastoma; internally debulked and dissected off the 4th-ventricle floor without pursuing adherent tumor for medulloblastoma/ependymoma]. The PICA, brainstem, and floor of the 4th ventricle were preserved and CSF pathways restored.
A watertight dural closure was performed (to prevent pseudomeningocele/CSF leak), the bone flap replaced, and the wound closed in layers. The patient was transferred to the ICU in stable condition.
Postoperative Plan
- ICU, neuro checks q1h, posterior fossa precautions (consciousness, breathing, CN, swallowing)
- Swallow eval before PO, eye/airway protection
- CT 6h, MRI postop (EOR); EVD/hydrocephalus management
- Antiemetics, steroid taper, DVT prophylaxis
- Pathology-specific: tumor board; medulloblastoma → craniospinal RT + chemo, neuraxis staging; metastasis → SRS/WBRT; hemangioblastoma → VHL workup
Chief-Level Case Review
Use these as the senior-level mental model for Posterior Fossa Tumor Resection (Cerebellar — Metastasis / Hemangioblastoma / Medulloblastoma / Ependymoma):
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Posterior Fossa Tumor Resection (Cerebellar — Metastasis / Hemangioblastoma / Medulloblastoma / Ependymoma):
- What is the surgical goal: gross-total, maximal safe, decompression, diagnosis, or cytoreduction?
- What eloquent cortex, tract, cranial nerve, vessel, or sinus defines the stopping point?
- What adjunct changes the case: navigation, mapping, 5-ALA, ultrasound, endoscope, ICG, or neuromonitoring?
- What is the edema, steroid, seizure, DVT, and postop imaging plan?
- What complication would you check for first in PACU based on this lesion location?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Extent-of-resection goal and functional stopping points: [attending-specific]
- Mapping/monitoring, 5-ALA, ultrasound, ICG, endoscope, or tractography preferences: [attending-specific]
- Steroid, antiepileptic, mannitol/hypertonic saline, and antibiotic plan: [attending-specific]
- Postop MRI timing, ICU/floor threshold, and adjuvant-referral workflow: [attending-specific]