
Case Prep: Pediatric Posterior Fossa Tumor Resection (Medulloblastoma / Pilocytic Astrocytoma / Ependymoma)
Case / Approach Snapshot
- Anatomy at risk: age-specific skull/soft tissue, developing brain and tracts, CSF pathways, brainstem/lower cranial nerves, tumor or congenital lesion relationships, and blood-volume constraints.
- Operative steps: adapt positioning/anesthesia to age, confirm imaging and goals with family, expose gently, preserve neurovascular/CSF pathways, reconstruct durably for growth, and plan ICU/endocrine/rehab surveillance; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: blood loss, hypothermia, swelling, hydrocephalus, airway/swallowing issues, endocrine/electrolyte shifts, infection, and staged therapy with oncology or rehab teams.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] child with a [midline/4th ventricular / cerebellar hemispheric] posterior fossa tumor ([medulloblastoma / pilocytic astrocytoma / ependymoma]) with [obstructive hydrocephalus] planned for suboccipital craniotomy for resection.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Postoperative facial palsy after pediatric posterior fossa tumor resection — Chu JK. Journal of neurosurgery. Pediatrics 2021. PubMed
- A review of long-term deficits in memory systems following radiotherapy for pediatric posterior fossa tumor — Baudou E. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology 2022. PubMed
- Deep Learning for Pediatric Posterior Fossa Tumor Detection and Classification: A Multi-Institutional Study — Quon JL. AJNR. American journal of neuroradiology 2020. PubMed
- An Analysis of Temporal Trend of Incidence of Post-Resection Cerebrospinal Fluid Diversion in Pediatric Posterior Fossa Tumor Patients and the Predictive Factors — Kumar A. Neurology India 2023. PubMed
- Volumetric predictors for shunt-dependency in pediatric posterior fossa tumors — Wilhelmy F. Scientific reports 2025. PubMed
- Machine Assist for Pediatric Posterior Fossa Tumor Diagnosis: A Multinational Study — Zhang M. Neurosurgery 2021. PubMed
- Impact of a pediatric posterior fossa tumor and its treatments on motor procedural learning — Baudou E. European journal of paediatric neurology : EJPN : official journal of the European Paediatric Neurology Society 2023. PubMed
- Executive and social functioning in pediatric posterior fossa tumor survivors and healthy controls — Ramjan S. Neuro-oncology practice 2023. PubMed
- Intraoperative neurophysiology in posterior fossa tumor surgery in children — Sala F. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2015. PubMed
- Arterial Spin-Labeling Perfusion Metrics in Pediatric Posterior Fossa Tumor Surgery — Toescu SM. AJNR. American journal of neuroradiology 2022. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
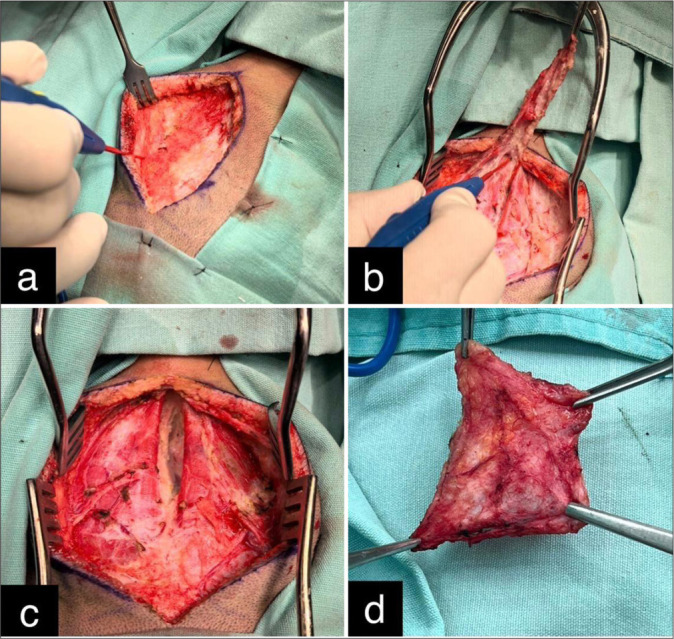 Figure 1:. Intraoperative steps of autologous cervical fascia graft for watertight duroplasty in pediatric posterior fossa surgery: (a) lateral dissection, (b) graft detachment, (c) muscular plane… Source: Autologous cervical fascia duraplasty in pediatric posterior fossa tumor surgery: A low-cost and viable alternative — Surgical Neurology International 2026; CC BY-NC-SA.
Figure 1:. Intraoperative steps of autologous cervical fascia graft for watertight duroplasty in pediatric posterior fossa surgery: (a) lateral dissection, (b) graft detachment, (c) muscular plane… Source: Autologous cervical fascia duraplasty in pediatric posterior fossa tumor surgery: A low-cost and viable alternative — Surgical Neurology International 2026; CC BY-NC-SA.
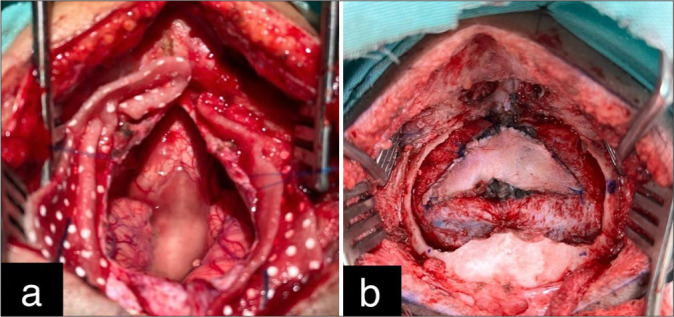 Figure 2:. Intraoperative images of posterior fossa exposure and dural repair using an autologous cervical fascia graft: (a) cerebellum and brainstem with dura opened. (b) Final view showing… Source: Autologous cervical fascia duraplasty in pediatric posterior fossa tumor surgery: A low-cost and viable alternative — Surgical Neurology International 2026; CC BY-NC-SA.
Figure 2:. Intraoperative images of posterior fossa exposure and dural repair using an autologous cervical fascia graft: (a) cerebellum and brainstem with dura opened. (b) Final view showing… Source: Autologous cervical fascia duraplasty in pediatric posterior fossa tumor surgery: A low-cost and viable alternative — Surgical Neurology International 2026; CC BY-NC-SA.
 Figure 3. Source: Autologous cervical fascia duraplasty in pediatric posterior fossa tumor surgery: A low-cost and viable alternative — Surg Neurol Int. 2026 Feb 6;17:68. doi: 10.25259/SNI_1177_2025; CC BY-NC-SA.
Figure 3. Source: Autologous cervical fascia duraplasty in pediatric posterior fossa tumor surgery: A low-cost and viable alternative — Surg Neurol Int. 2026 Feb 6;17:68. doi: 10.25259/SNI_1177_2025; CC BY-NC-SA.
 Figure 4. Source: Autologous cervical fascia duraplasty in pediatric posterior fossa tumor surgery: A low-cost and viable alternative — Surg Neurol Int. 2026 Feb 6;17:68. doi: 10.25259/SNI_1177_2025; CC BY-NC-SA.
Figure 4. Source: Autologous cervical fascia duraplasty in pediatric posterior fossa tumor surgery: A low-cost and viable alternative — Surg Neurol Int. 2026 Feb 6;17:68. doi: 10.25259/SNI_1177_2025; CC BY-NC-SA.
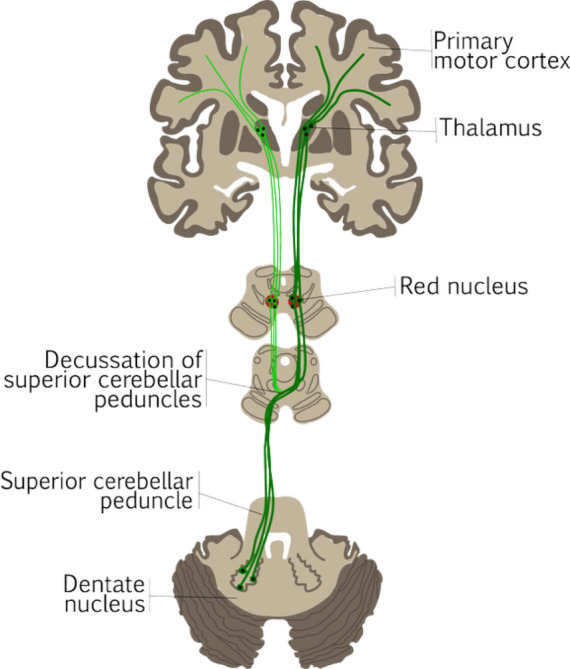 Fig. 1. Anatomical illustration of the dentato-rubro-thalamic tract (DRTT). The dark green tract represents the decussating DRTT, the classic component that decussates from the dentate nucleus… Source: Evaluation of tractography parameters for dentato-rubro-thalamic tract reconstruction during pediatric posterior fossa tumor surgery — Magma (New York, N.y.) 2025; CC BY.
Fig. 1. Anatomical illustration of the dentato-rubro-thalamic tract (DRTT). The dark green tract represents the decussating DRTT, the classic component that decussates from the dentate nucleus… Source: Evaluation of tractography parameters for dentato-rubro-thalamic tract reconstruction during pediatric posterior fossa tumor surgery — Magma (New York, N.y.) 2025; CC BY.
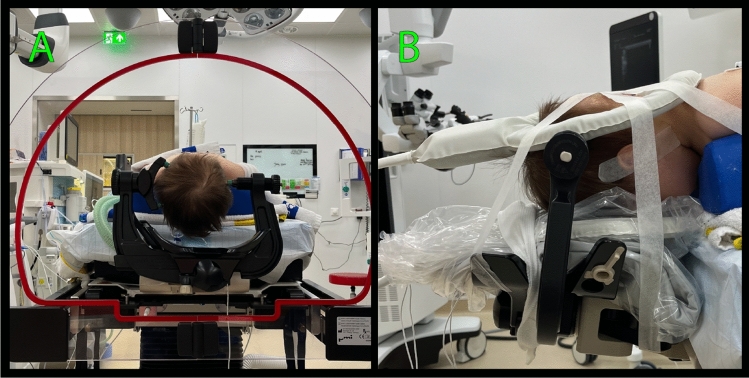 Fig. 2. Example of patient preparation for MR acquisition before surgery. A After positioning the patient in the surgical prone position (i.e., laying on their stomach with their chest lifted… Source: Evaluation of tractography parameters for dentato-rubro-thalamic tract reconstruction during pediatric posterior fossa tumor surgery — Magma (New York, N.y.) 2025; CC BY.
Fig. 2. Example of patient preparation for MR acquisition before surgery. A After positioning the patient in the surgical prone position (i.e., laying on their stomach with their chest lifted… Source: Evaluation of tractography parameters for dentato-rubro-thalamic tract reconstruction during pediatric posterior fossa tumor surgery — Magma (New York, N.y.) 2025; CC BY.
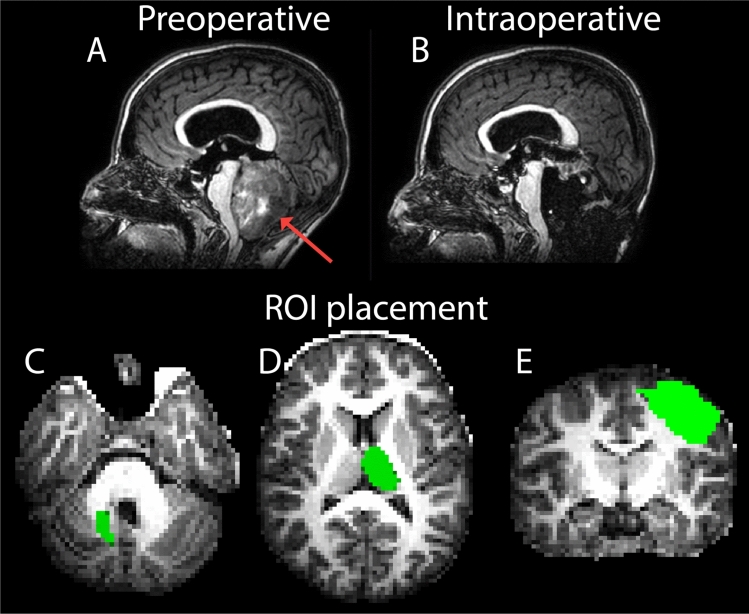 Fig. 3. Example of T1-weighted images before and during surgery and placement of the regions of interest used for fiber tractography. T1-weighted (T1w) images of a 14-year-old girl with a 4th… Source: Evaluation of tractography parameters for dentato-rubro-thalamic tract reconstruction during pediatric posterior fossa tumor surgery — Magma (New York, N.y.) 2025; CC BY.
Fig. 3. Example of T1-weighted images before and during surgery and placement of the regions of interest used for fiber tractography. T1-weighted (T1w) images of a 14-year-old girl with a 4th… Source: Evaluation of tractography parameters for dentato-rubro-thalamic tract reconstruction during pediatric posterior fossa tumor surgery — Magma (New York, N.y.) 2025; CC BY.
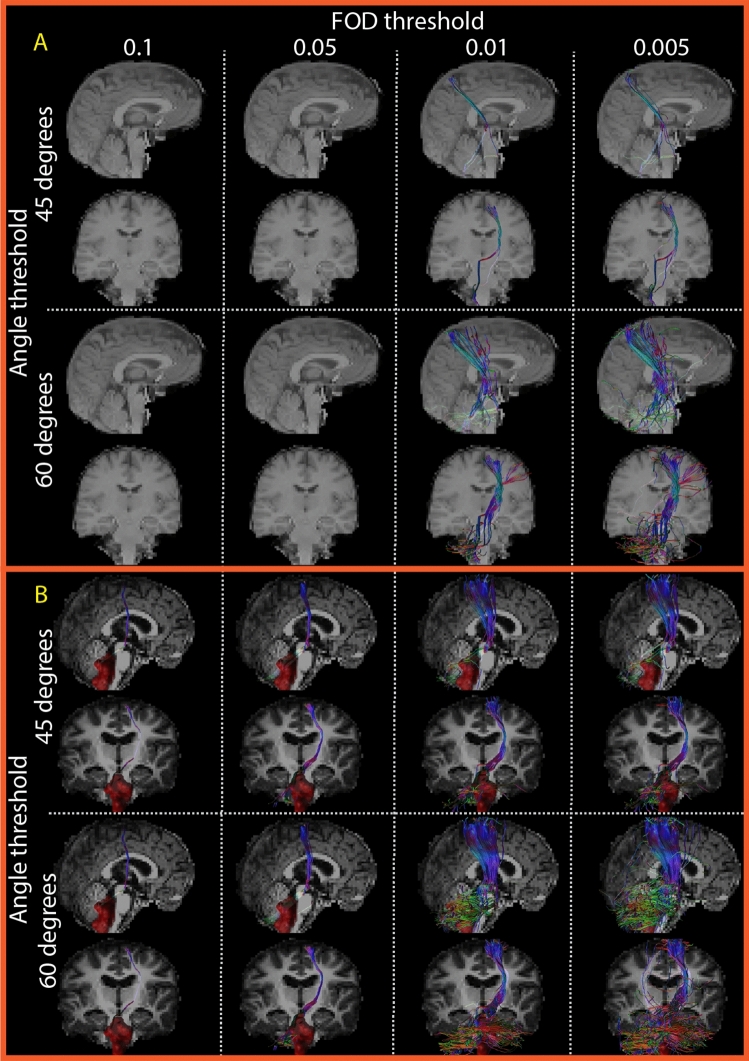 Fig. 4. Example of eight fiber tractography parameter combinations for one side dentato-rubro-thalamic tract. All panels show the dentato-rubro-thalamic tract (DRTT) crossing from the dentate… Source: Evaluation of tractography parameters for dentato-rubro-thalamic tract reconstruction during pediatric posterior fossa tumor surgery — Magma (New York, N.y.) 2025; CC BY.
Fig. 4. Example of eight fiber tractography parameter combinations for one side dentato-rubro-thalamic tract. All panels show the dentato-rubro-thalamic tract (DRTT) crossing from the dentate… Source: Evaluation of tractography parameters for dentato-rubro-thalamic tract reconstruction during pediatric posterior fossa tumor surgery — Magma (New York, N.y.) 2025; CC BY.
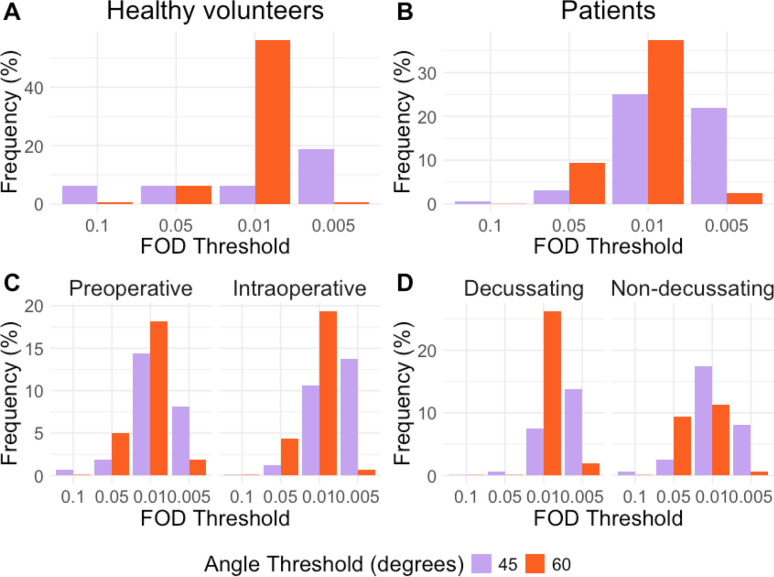 Fig. 5. Qualitative results fiber tractography parameter combinations. In healthy volunteers (A) and pediatric posterior fossa tumor patients (B), an FOD threshold of 0.01 and an angle threshold… Source: Evaluation of tractography parameters for dentato-rubro-thalamic tract reconstruction during pediatric posterior fossa tumor surgery — Magma (New York, N.y.) 2025; CC BY.
Fig. 5. Qualitative results fiber tractography parameter combinations. In healthy volunteers (A) and pediatric posterior fossa tumor patients (B), an FOD threshold of 0.01 and an angle threshold… Source: Evaluation of tractography parameters for dentato-rubro-thalamic tract reconstruction during pediatric posterior fossa tumor surgery — Magma (New York, N.y.) 2025; CC BY.
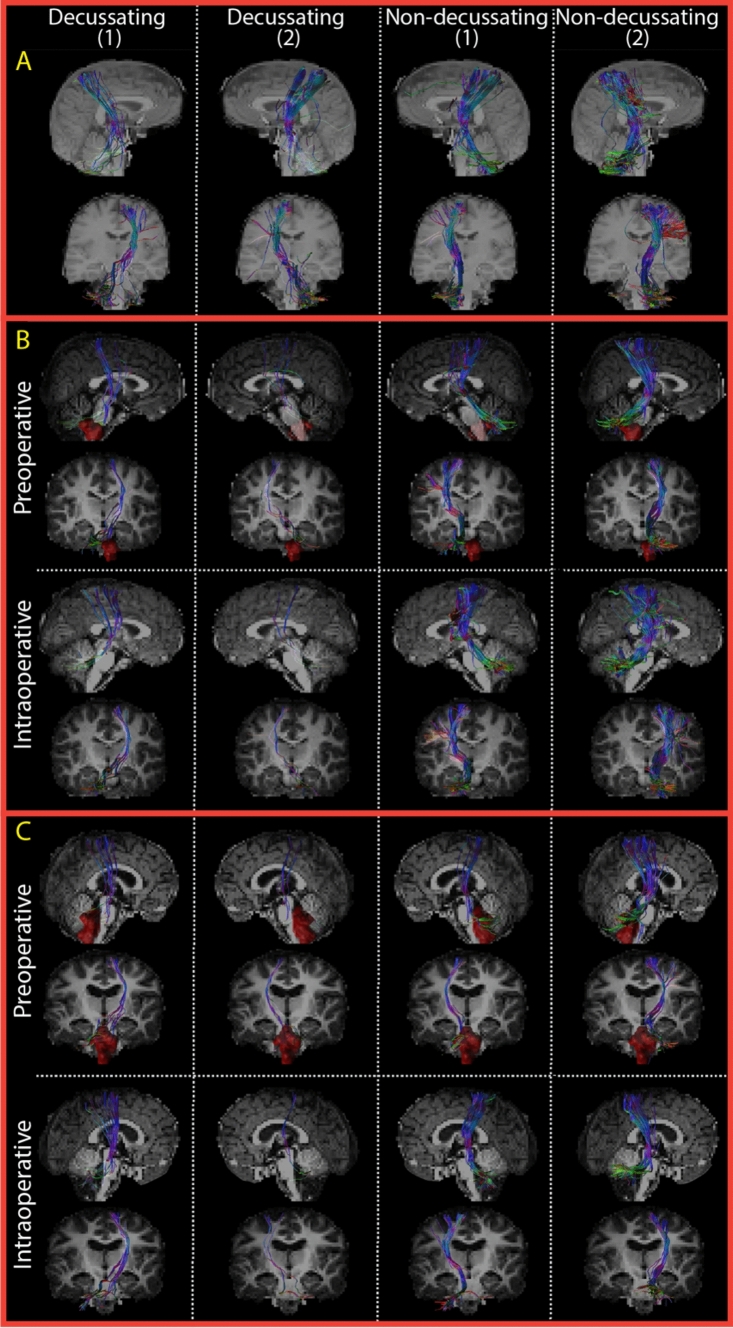 Fig. 6. Dentato-rubro-thalamic tracts (DRTT) reconstructed with the best parameter combination of our dataset. The first two columns show both DRTTs (1 and 2) crossing from the dentate nucleus… Source: Evaluation of tractography parameters for dentato-rubro-thalamic tract reconstruction during pediatric posterior fossa tumor surgery — Magma (New York, N.y.) 2025; CC BY.
Fig. 6. Dentato-rubro-thalamic tracts (DRTT) reconstructed with the best parameter combination of our dataset. The first two columns show both DRTTs (1 and 2) crossing from the dentate nucleus… Source: Evaluation of tractography parameters for dentato-rubro-thalamic tract reconstruction during pediatric posterior fossa tumor surgery — Magma (New York, N.y.) 2025; CC BY.
History of Present Illness
- Chief complaint: Morning headache, vomiting, ataxia, lethargy, head tilt, diplopia (raised ICP from 4th ventricle obstruction)
- Duration (often weeks), gait/balance, cranial nerve symptoms
- Common pediatric posterior fossa tumors:
- Medulloblastoma (midline/vermian, 4th ventricle, malignant, drop mets — stage neuraxis)
- Pilocytic astrocytoma (cerebellar hemisphere, cystic + mural nodule, benign, excellent prognosis with GTR)
- Ependymoma (4th ventricle floor, extends through foramina, adherent to floor)
- ATRT (young, aggressive)
Past Medical History
- Developmental history, prior illness, syndromic associations (Gorlin → medulloblastoma; NF1 → astrocytoma)
Imaging Review
MRI brain + entire neuraxis (T1±Gad, T2, DWI)
- Location (midline vs hemispheric vs 4th ventricle floor), enhancement, cyst+nodule (pilocytic), restricted diffusion (medulloblastoma/ATRT — hypercellular)
- 4th ventricle / brainstem floor relationship, extension through foramina (Luschka/Magendie — ependymoma)
- Hydrocephalus, tonsillar herniation
- Spine MRI for drop metastases (medulloblastoma, ependymoma — before or ~2 weeks after surgery to avoid postop artifact)
Labs
- CBC, BMP, Coags, type and crossmatch (pediatric blood volume), pre-op anesthesia
Neurological Examination
- Cerebellar (truncal + appendicular), CN exam, gait, fundoscopy (papilledema), head tilt, mental status
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: pediatric anesthesia/equipment, warming, weight-based implants/antibiotics, navigation/endoscope/microscope as needed, blood availability for tumor/myelomeningocele cases, and family-centered postop handoff.
- Special needs: weight-based fluids/meds, latex allergy precautions for myelomeningocele, steroid/endocrine/DI plan when sellar/posterior fossa risk exists, EVD/CSF diversion plan, and age-appropriate neuro baseline.
- Immediate postop orders: PICU/step-down neuro checks, airway/swallow monitoring when relevant, CT/MRI timing, drain/EVD/shunt orders, antibiotics/steroid taper, pain control, wound/skin precautions, and PT/OT/rehab planning.
Hydrocephalus Management
- Preop EVD or ETV if significant hydrocephalus (many pediatric posterior fossa tumors present with hydrocephalus); some resolve after resection; avoid rapid overdrainage (upward herniation)
Position
- Prone (Concorde) — preferred in children (avoid sitting/VAE in small children generally); Mayfield (age-appropriate pin pressures; in very young children use horseshoe/skull clamp caution — thin skull) or padded headrest; neck flexed, shoulders down
Approach: Midline Suboccipital Craniotomy ± C1 laminectomy
Key Surgical Steps
- Midline incision (inion to C2), avascular midline raphe
- Suboccipital craniotomy (craniotomy preferred over craniectomy in children — replace bone); C1 laminectomy if tonsillar/4th ventricular extension
- Open dura (Y-shaped), manage occipital sinus bleeding
- Telovelar approach (through cerebellomedullary fissure) to the 4th ventricle — avoids splitting the vermis (reduces cerebellar mutism)
- Tumor resection:
- Pilocytic: drain cyst, resect mural nodule + tumor (GTR usually curative)
- Medulloblastoma: internal debulking, circumferential dissection, avoid pursuing tumor adherent to 4th ventricle floor/brainstem (leave residual rather than injure floor)
- Ependymoma: often adherent to floor and extends through foramina — meticulous dissection, accept small residual on floor over deficit
- Preserve PICA, brainstem, dentate nuclei/peduncles
- Restore CSF pathways, watertight dural closure (CSF leak/pseudomeningocele common in children)
Critical Anatomy & Structures at Risk
- Brainstem / floor of 4th ventricle (CN nuclei — facial colliculus, vagal/hypoglossal trigones) — cerebellar mutism syndrome, CN palsies, cardiorespiratory
- Dentate nuclei / cerebellar peduncles / vermis — mutism, ataxia
- PICA, occipital/transverse sinuses
- Pediatric blood volume (transfusion)
Equipment
- Microscope, navigation, CUSA, ultrasonic aspirator (pediatric settings)
- EVD kit, bipolar, hemostatic agents, dural substitute, crossmatched blood
Monitoring
- SSEPs, MEPs, CN EMG (VII, IX-XII), BAER; pediatric IONM
Anesthesia
- Arterial line, crossmatched blood, pediatric fluid/thermoregulation, antiemetics, VAE precautions, careful pediatric dosing
Potential Complications
- Posterior fossa syndrome / cerebellar mutism (up to ~25% with midline/vermian/dentate involvement — transient mutism, emotional lability, ataxia; recovery over weeks-months, often incomplete)
- CN deficits, swallowing/airway compromise (floor)
- Hydrocephalus persistence → shunt, CSF leak/pseudomeningocele
- Blood loss, aseptic meningitis
Operative Note Template
Preoperative Diagnosis: [Midline/4th-ventricular] pediatric posterior fossa tumor ([medulloblastoma/pilocytic astrocytoma/ependymoma]) with obstructive hydrocephalus
Postoperative Diagnosis: Same (pending pathology)
Procedure: Suboccipital craniotomy [with C1 laminectomy] for resection of pediatric posterior fossa tumor [with EVD]
Surgeon / Assistant: Anesthesia: Pediatric general endotracheal EBL / Fluids / Blood products: [crossmatched] Adjuncts: Microscope, navigation, CUSA, [ICG]; SSEP/MEP/CN EMG/BAER; EVD Implants: Dural substitute; [EVD] Complications: None
Indications: [Age] child with a [location] posterior fossa tumor and hydrocephalus. [Preop EVD/ETV managed hydrocephalus.] Risks (cerebellar mutism, CN/floor injury, hydrocephalus, CSF leak) discussed with family.
Description of Procedure: After consent and time-out, pediatric general anesthesia was induced and neuromonitoring established. The patient was positioned prone (Concorde) with [age-appropriate head fixation]. [An EVD was placed.] A midline suboccipital craniotomy [with C1 laminectomy] was performed (bone replaced — craniotomy preferred in children) and the dura opened, managing the occipital sinus.
The 4th ventricle was accessed via a vermis-sparing telovelar approach. The tumor was resected [pilocytic: cyst + nodule; medulloblastoma/ependymoma: debulked and dissected without pursuing tumor adherent to the 4th-ventricle floor/brainstem], preserving PICA, the brainstem, and the floor. A watertight dural closure was performed and the bone replaced.
The patient was transferred to the PICU with posterior-fossa precautions and vigilance for cerebellar mutism; neuraxis staging MRI/CSF cytology were planned (embryonal/ependymal tumors).
Postoperative Plan
- PICU, neuro checks q1h, posterior fossa precautions (consciousness, breathing, CN, swallowing)
- Watch for cerebellar mutism (may be delayed 1-2 days), swallow eval before PO, airway/eye protection
- CT 6h, MRI postop < 48h (EOR); EVD/hydrocephalus management
- Antiemetics, steroid taper, DVT prophylaxis (age-appropriate)
- Neuraxis staging MRI + LP CSF cytology (medulloblastoma/ependymoma — for staging, ~2 weeks post-op)
- Pediatric neuro-oncology/tumor board: medulloblastoma → risk-stratified craniospinal RT (age > 3) + chemo; ependymoma → RT ± second-look surgery; pilocytic → observation if GTR
- Molecular subgrouping (medulloblastoma: WNT/SHH/Group 3/4), rehab, long-term follow-up
Chief-Level Case Review
Use these as the senior-level mental model for Pediatric Posterior Fossa Tumor Resection (Medulloblastoma / Pilocytic Astrocytoma / Ependymoma):
- Decision point: The setup is age-specific: blood volume, warming, positioning pressure, airway, latex risk, family counseling, and ICU/PICU handoff differ from adults.
- Technical lever: Preserve future options: growth, shunt dependence, cranioplasty/bone healing, endocrine/neurocognitive trajectory, and adjuvant therapy influence today’s choices.
- Bailout: Have a complication script: blood loss, CSF leak, hydrocephalus, wound breakdown, posterior fossa mutism, infection, and airway/swallow risk should be anticipated.
- Postop watch: Postop communication matters: family expectations, neurologic baseline, therapy needs, school/developmental supports, and surveillance imaging/labs should be clear.
Common Pimp Questions
Use these to pressure-test preparation for Pediatric Posterior Fossa Tumor Resection (Medulloblastoma / Pilocytic Astrocytoma / Ependymoma):
- What age-specific anatomy, blood volume, temperature, and positioning issue changes the plan?
- What is the neurologic, developmental, or syndromic baseline?
- What skin, wound, CSF, or infection risk is highest in this child?
- What family-facing expectation should be clarified before surgery?
- What postop bed, feeding, pain, imaging, and activity plan is safest?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Blood availability threshold, warming strategy, antibiotic dosing, and Foley/drain use: [attending-specific]
- Positioning aids, pinning versus horseshoe, and skin-prep preference: [attending-specific]
- Family update cadence and expected ICU/floor disposition: [attending-specific]
- Postop feeding, pain regimen, wound care, and activity restrictions: [attending-specific]