
Operative Approach: Bifrontal (Subfrontal) Craniotomy
Case / Approach Snapshot
- Anatomy at risk: frontal sinus, supraorbital/supratrochlear pedicles, pericranial flap, anterior third of SSS/falx, frontal bridging veins, olfactory bulbs/tracts, cribriform/ethmoid roof, ethmoidal arteries, optic apparatus, ACA/AComA complex, and anterior skull-base reconstruction planes.
- Operative steps: plan sinus/pericranial reconstruction, raise bicoronal flap and vascularized pericranium, create low bifrontal exposure, cranialize frontal sinus when entered, divide anterior SSS/falx only when appropriate, relax frontal lobes, devascularize tumor/base, protect optic/ACA structures, and close with watertight anterior-fossa separation.
- Rescue plans: frontal sinus violation, pneumatized crista galli, CSF rhinorrhea risk, venous bleeding, frontal-lobe swelling, ethmoidal artery retraction into orbit, optic/ACA adherence, anosmia counseling, and need to convert to unilateral, endonasal, or combined craniofacial strategy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas — olfactory groove / anterior base · Radiopaedia — olfactory groove meningioma · PubMed Central — bifrontal craniotomy
High-Yield Literature
- Microsurgical Anatomy Review of Bifrontal Limited Transbasal Approach - Quantitative and Anatomy Study — Ng AF. World neurosurgery 2020. PubMed
- Anatomical Step-by-Step Dissection of Complex Skull Base Approaches for Trainees: Surgical Anatomy of the Bifrontal Transbasal Approach, Surgical Principles, and Illustrative Cases — Vilany L. Journal of neurological surgery. Part B, Skull base 2024. PubMed
- [Olfactory groove meningiomas. Radical microsurgical treatment through the bifrontal approach] — González-Darder JM. Neurocirugia (Asturias, Spain) 2011. PubMed
- Olfactory groove meningiomas from neurosurgical and ear, nose, and throat perspectives: approaches, techniques, and outcomes — Spektor S. Neurosurgery 2005. PubMed
- Operative Technique and Complication Management in a Case of Giant Esthesioneuroblastoma Resected by a Combined Transcranial and Endonasal Endoscopic Approach: Technical Case Report — McAvoy M. Operative neurosurgery (Hagerstown, Md.) 2023. PubMed
- Vascularized anterolateral thigh free flap for salvage reconstruction of complex anterior skull base and nasion defects after failed conventional reconstruction- how I do it — Liu H. Acta neurochirurgica 2026. PubMed
- Microsurgical Resection of a Primary Intraosseous Meningioma Encasing the Superior Sagittal Sinus — Ene CI. The Journal of craniofacial surgery 2020. PubMed
- Validity of the frontolateral approach as a minimally invasive corridor for olfactory groove meningiomas — El-Bahy K. Acta neurochirurgica 2009. PubMed
- Olfactory groove meningiomas: functional outcome in a series treated microsurgically — Bassiouni H. Acta neurochirurgica 2007. PubMed
- Precision in Complexity: A Protocol-Driven Quantitative Anatomic Strategy for Giant Olfactory Groove Meningioma Resection in a High-Risk Geriatric Patient — Grigorean VT. Diagnostics (Basel, Switzerland) 2026. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
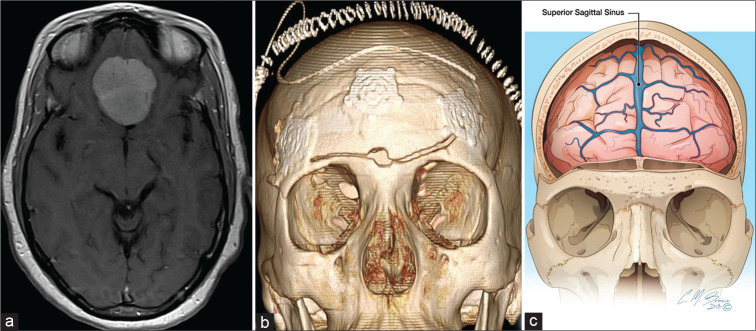 Figure 1:. A 40-year-old man with planum sphenoidale meningioma on an axial T1 magnetic resonance imaging with gadolinium (a), requiring frontal craniotomy. Three-dimensional volume rendering (b)… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
Figure 1:. A 40-year-old man with planum sphenoidale meningioma on an axial T1 magnetic resonance imaging with gadolinium (a), requiring frontal craniotomy. Three-dimensional volume rendering (b)… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
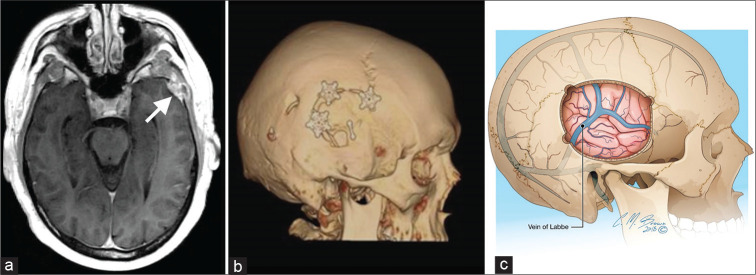 Figure 2:. A 63-year-old man with the left temporal sclerosing meningioma (a – arrow) on axial T1 MRI with gadolinium, requiring temporal craniotomy. Three-dimensional volume rendering (b)… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
Figure 2:. A 63-year-old man with the left temporal sclerosing meningioma (a – arrow) on axial T1 MRI with gadolinium, requiring temporal craniotomy. Three-dimensional volume rendering (b)… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
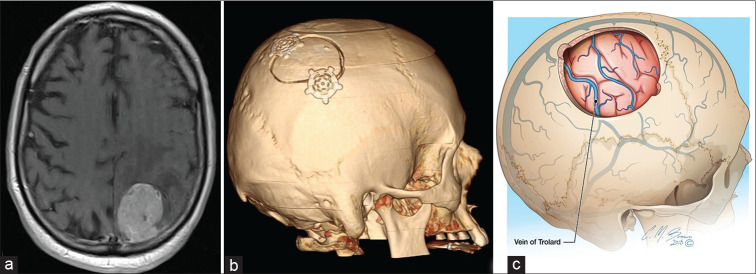 Figure 3:. A 78-year-old man with the left parietal melanoma metastasis (a) on axial T1 MRI with gadolinium. Three-dimensional volume rendering (b) demonstrates parietal craniotomy, the preferred… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
Figure 3:. A 78-year-old man with the left parietal melanoma metastasis (a) on axial T1 MRI with gadolinium. Three-dimensional volume rendering (b) demonstrates parietal craniotomy, the preferred… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
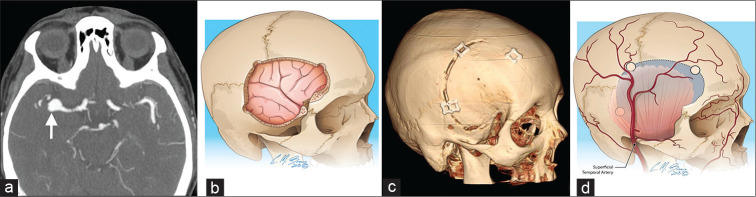 Figure 4:. A 69-year-old woman with the right middle cerebral artery aneurysm (a – arrow) on axial CT angiogram. Sagittal oblique illustration (b) and three-dimensional volume rendering (c)… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
Figure 4:. A 69-year-old woman with the right middle cerebral artery aneurysm (a – arrow) on axial CT angiogram. Sagittal oblique illustration (b) and three-dimensional volume rendering (c)… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
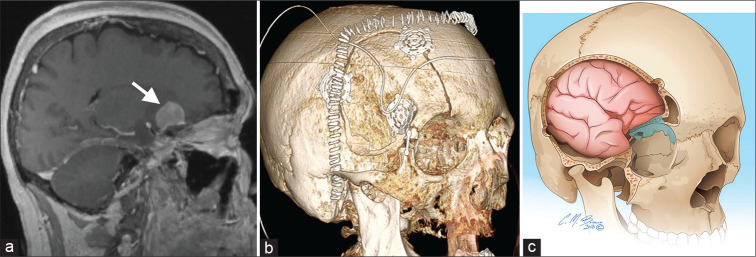 Figure 5:. A 55-year-old woman with the right paraclinoid meningioma (a – arrow) on sagittal T1 magnetic resonance imaging. Three-dimensional volume rendering (b) demonstrates post-operative… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
Figure 5:. A 55-year-old woman with the right paraclinoid meningioma (a – arrow) on sagittal T1 magnetic resonance imaging. Three-dimensional volume rendering (b) demonstrates post-operative… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
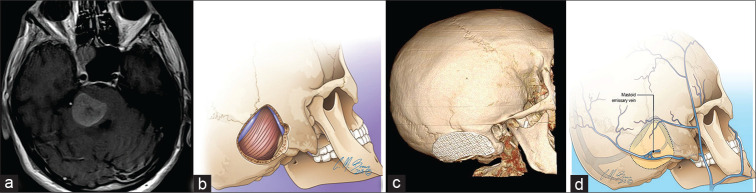 Figure 6:. A 59-year-old man with pontine melanoma metastasis (a) on axial T1 magnetic resonance imaging. Sagittal oblique illustration (b) and three-dimensional volume rendering (c) demonstrating… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
Figure 6:. A 59-year-old man with pontine melanoma metastasis (a) on axial T1 magnetic resonance imaging. Sagittal oblique illustration (b) and three-dimensional volume rendering (c) demonstrating… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
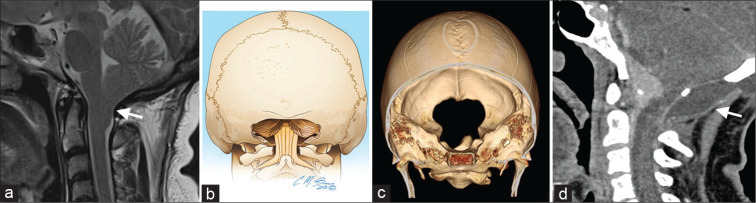 Figure 7:. A 45-year-old woman with Chiari I malformation (a – arrow) on axial and sagittal T2W magnetic resonance imaging. Coronal view illustration (b) and three-dimensional volume rendering (c)… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
Figure 7:. A 45-year-old woman with Chiari I malformation (a – arrow) on axial and sagittal T2W magnetic resonance imaging. Coronal view illustration (b) and three-dimensional volume rendering (c)… Source: An Illustrative Review of Common Modern Craniotomies — Journal of Clinical Imaging Science 2020; CC BY-NC-SA.
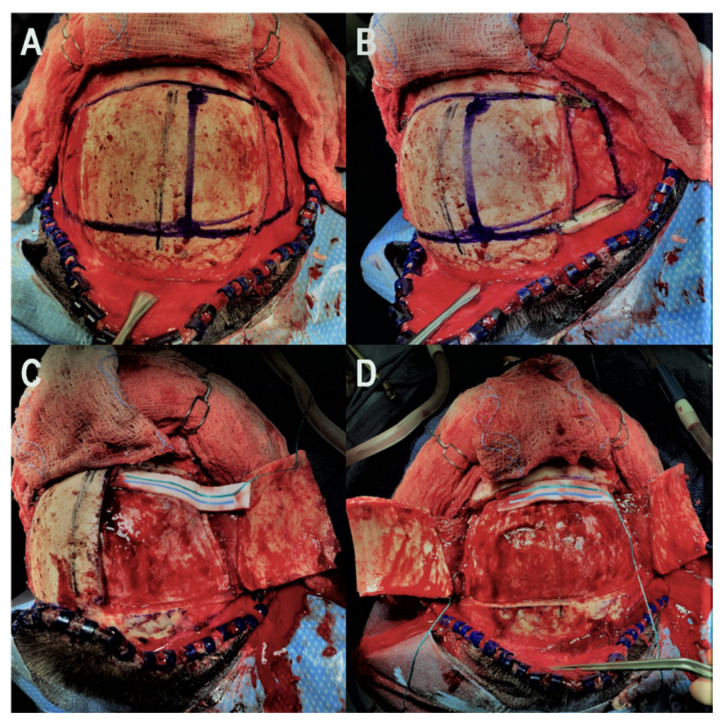 Figure 1. Illustration of the key steps for the bifrontal osteoplastic flap technique. (A): The midline is identified using the sagittal suture and the six necessary burr holes are marked. (B):… Source: Bifrontal Osteoplastic Flap: An Option to Decrease Infection in Bifrontal Craniotomies with Skull Base Osteotomies — Brain Sciences 2022; CC BY.
Figure 1. Illustration of the key steps for the bifrontal osteoplastic flap technique. (A): The midline is identified using the sagittal suture and the six necessary burr holes are marked. (B):… Source: Bifrontal Osteoplastic Flap: An Option to Decrease Infection in Bifrontal Craniotomies with Skull Base Osteotomies — Brain Sciences 2022; CC BY.
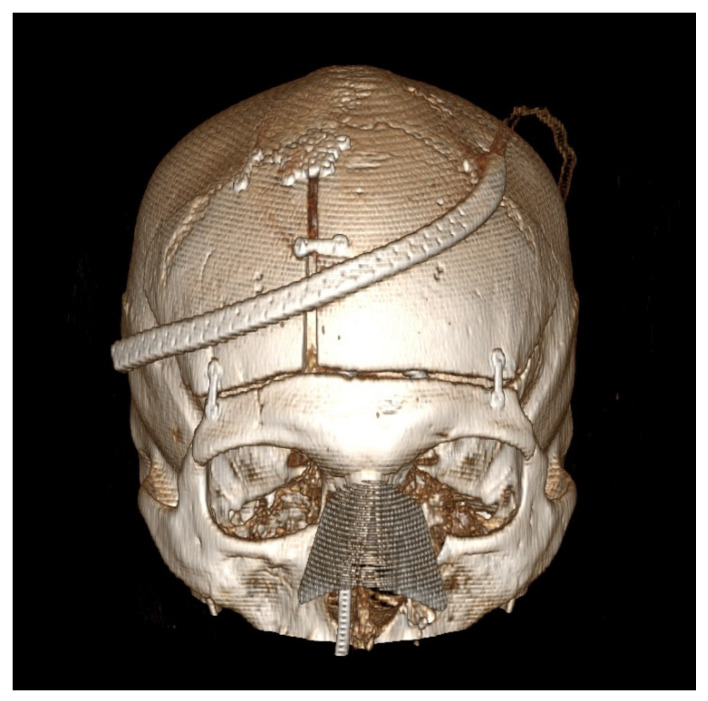 Figure 2. Post-operative computed tomography 3D reconstruction of the patient is presented in Figure 1. This patient underwent a combined bifrontal osteoplastic flap and transnasal approach for… Source: Bifrontal Osteoplastic Flap: An Option to Decrease Infection in Bifrontal Craniotomies with Skull Base Osteotomies — Brain Sciences 2022; CC BY.
Figure 2. Post-operative computed tomography 3D reconstruction of the patient is presented in Figure 1. This patient underwent a combined bifrontal osteoplastic flap and transnasal approach for… Source: Bifrontal Osteoplastic Flap: An Option to Decrease Infection in Bifrontal Craniotomies with Skull Base Osteotomies — Brain Sciences 2022; CC BY.
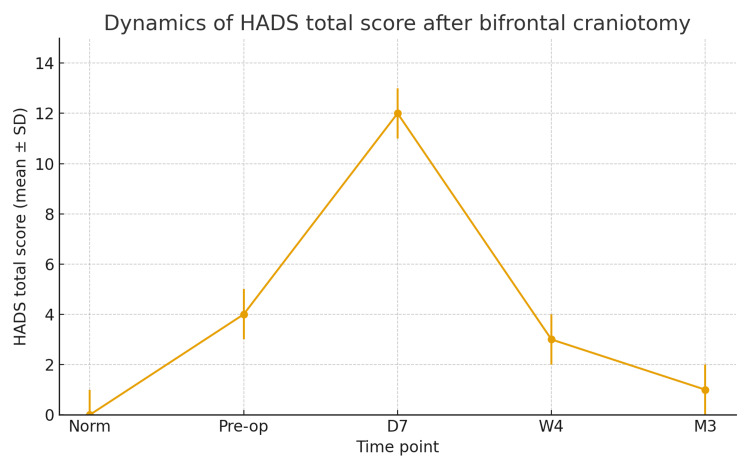 Figure 1. HADS score timeline.HADS: Hospital Anxiety and Depression Scale Source: Transient Psychiatric Disturbances Following Bifrontal Craniotomy for Suprasellar Tumors — Cureus 2025; CC BY.
Figure 1. HADS score timeline.HADS: Hospital Anxiety and Depression Scale Source: Transient Psychiatric Disturbances Following Bifrontal Craniotomy for Suprasellar Tumors — Cureus 2025; CC BY.
The bifrontal (subfrontal) craniotomy is the wide, bilateral midline corridor to the anterior cranial fossa floor. Through a bicoronal incision, a frontal bone flap crossing the superior sagittal sinus is elevated and the frontal lobes are gently retracted to expose the planum, cribriform plate, crista galli, both orbital roofs, and the suprasellar region in a single bilateral field. It is the classic approach for large midline anterior skull base tumors (olfactory groove and planum meningiomas, sinonasal tumors with intracranial extension) and for anterior skull base / CSF-leak reconstruction, where its bilateral exposure and vascularized pericranial flap are decisive.
General Considerations
- What it accesses: the entire anterior cranial fossa floor bilaterally — crista galli/cribriform, planum sphenoidale, both orbital roofs, the suprasellar cistern, and (posteriorly) the optic nerves/chiasm and the ACA/AComA complex.
- Why bilateral: large midline tumors that cross the midline and splay both frontal lobes are addressed in one field with excellent orientation; the approach also gives the best access for watertight anterior-fossa-floor reconstruction (large dural/bony defects, CSF leaks) using a long pericranial flap.
- The cost is olfaction and frontal-lobe handling. For olfactory groove meningiomas the olfactory tracts are usually sacrificed (anosmia); bifrontal retraction and anterior SSS ligation carry frontal-lobe and venous considerations. Lateralized or smaller lesions are increasingly done via supraorbital keyhole, unilateral subfrontal/pterional, or endoscopic endonasal routes — reserve the full bifrontal for large midline disease and reconstruction needs.
Indications
- Large olfactory groove meningioma (prototype) → olfactory-groove-meningioma.md
- Planum / large tuberculum sellae meningioma crossing midline → tuberculum-sellae-meningioma.md
- Sinonasal tumors with intracranial extension (cranionasal/craniofacial), esthesioneuroblastoma
- Traumatic anterior skull base fractures / CSF rhinorrhea repair, anterior fossa reconstruction
Corridor Selection
| Lesion pattern | Bifrontal advantage | Alternative to consider |
|---|---|---|
| Large midline olfactory groove tumor with bilateral extension | Bilateral devascularization and reconstruction field | Unilateral subfrontal/pterional for smaller lateralized tumors |
| Large planum/tuberculum tumor with major optic canal work | Wide midline access and optic apparatus control | Pterional/OZ for lateral optic canal/cavernous extension; endonasal for selected midline inferior tumors |
| Sinonasal tumor crossing skull base | Combined craniofacial field and pericranial flap | Endoscopic endonasal alone for limited midline disease |
| Traumatic anterior fossa CSF leak with broad defect | Direct multilayer floor repair | Endoscopic repair for focal medial leaks |
| Small anterior skull-base lesion with preserved olfaction priority | Often excessive | Supraorbital keyhole, pterional, or endonasal depending on origin |
The bifrontal approach is a reconstruction-heavy corridor. If a robust pericranial flap and sinus plan are not needed, ask whether a unilateral or endonasal route gives the same target control with less frontal-lobe cost.
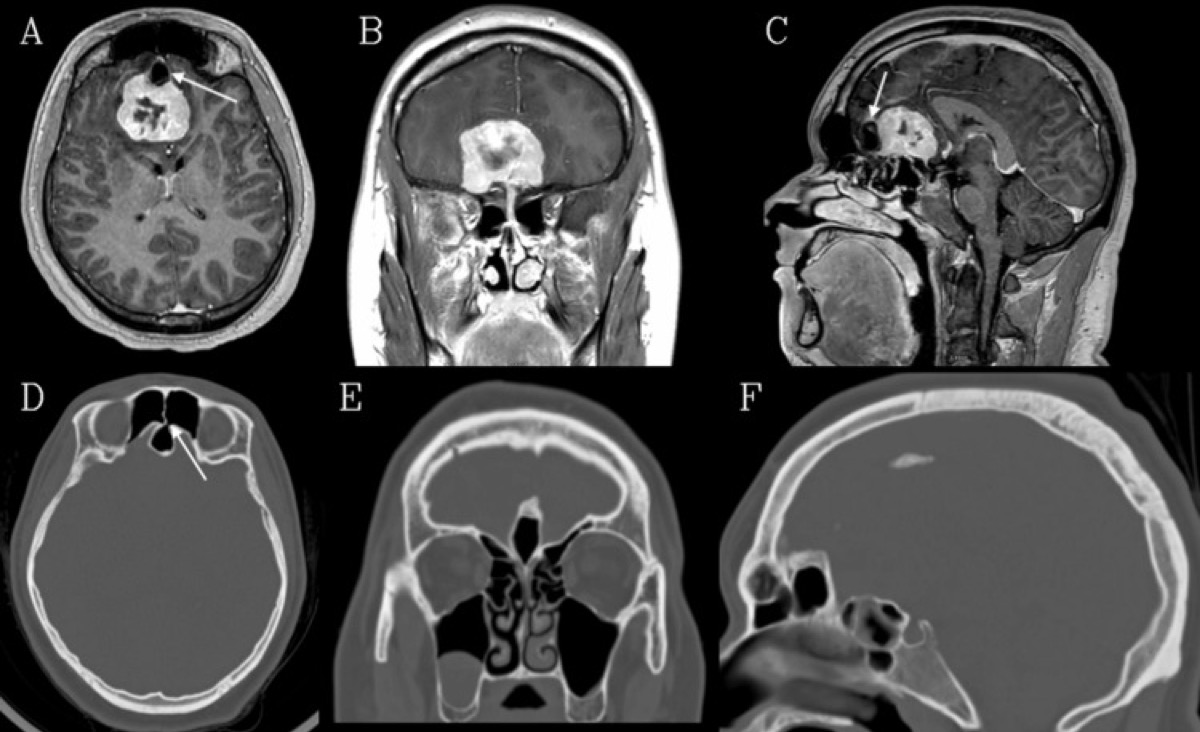
Cureus 2026;18:e101289 (PMC12889192) — CC BY 4.0. The prototypical bifrontal target; the pneumatized crista galli (arrows) warns of an anterior-fossa CSF communication.
Relevant Surgical Anatomy
- Scalp / bicoronal flap & pericranium: the vascularized pericranial flap (supraorbital/supratrochlear pedicled) is harvested with the exposure — the workhorse of anterior-fossa-floor reconstruction.
- Frontal sinus: routinely entered by a low bifrontal flap → must be cranialized (mucosa exenterated, duct plugged, buttressed) to prevent mucocele/CSF leak.
- Superior sagittal sinus (SSS) & falx: the anterior third of the SSS can be ligated and divided (with the falx) to open the interhemispheric midline; the posterior SSS cannot.
- Anterior fossa floor: crista galli, cribriform plate, anterior/posterior ethmoidal arteries (the dural blood supply of olfactory groove meningiomas — coagulated early at the base), olfactory bulbs/tracts, planum, tuberculum/optic canals.
- Posterior limit: optic nerves/chiasm and the ACA–AComA complex — the deep neurovascular boundary.
Preoperative Evaluation
- CT (bone): frontal sinus and crista galli pneumatization, cribriform/ethmoid involvement, hyperostosis, and bony invasion (see figure); plan sinus cranialization and floor reconstruction.
- MRI ± CTA: tumor extent/vascularity, brain edema, optic apparatus and ACA encasement; consider preoperative embolization for very vascular tumors.
- Vision and endocrine baseline; counsel re: anosmia and CSF-leak risk. Plan the pericranial flap.
Reconstruction Plan Before Incision
- Identify frontal sinus boundaries and nasofrontal ducts on CT; decide whether the sinus will be avoided, exenterated, or fully cranialized.
- Check for pneumatized crista galli, ethmoid roof defects, and sinonasal extension; these often determine the need for multilayer repair.
- Plan a pericranial flap long enough to reach the planum/cribriform defect without tension; preserve pedicles during scalp reflection.
- Decide whether lumbar drainage is needed and when it is safe; avoid early overdrainage before dural opening if there is major mass effect.
- Coordinate ENT/plastics when sinonasal resection, orbital wall work, free flap, or complex revision reconstruction is expected.
Logistics, OR Setup & Orders
- OR setup: Mayfield/head holder plan, microscope/endoscope, navigation, vascular instruments/ICG when applicable, skull base reconstruction supplies, and approach-specific retractors/drills ready before opening.
- Special needs: arterial line for major intracranial or vascular cases, Foley for long cases, neuromonitoring by corridor, dexamethasone/antiepileptic/BP plan by pathology, and blood products for vascular or skull base exposure.
- Immediate postop orders: disposition and neuro-check frequency, HOB/activity, postop CT/MRI/CTA timing, BP goals, steroid/antiepileptic plan, DVT prophylaxis timing, drain management, and focused cranial nerve/visual/language/motor exams.
Anesthesia & Neuromonitoring
- GA; lumbar drain to aid frontal-lobe relaxation (drain after dura is open); navigation; vision-relevant monitoring as indicated. Normotension.
Positioning
- Supine, head neutral, in Mayfield, with slight extension so the frontal lobes fall away from the anterior fossa floor (gravity retraction); vertex neutral. Bicoronal field prepped.
Incision, Pericranial Flap & Craniotomy
- Bicoronal incision behind the hairline; reflect the scalp and harvest a long, robust pericranial flap (preserve its supraorbital/supratrochlear pedicles) for later floor reconstruction.
- Bifrontal bone flap low to the anterior fossa floor, crossing the SSS (strip the sinus off the inner table carefully).
- Frontal sinus cranialization when entered: exenterate mucosa, occlude the nasofrontal duct, and buttress with pericranium — a key CSF-leak/mucocele preventer.
- Open the dura along the floor; ligate and divide the anterior SSS and falx if a midline interhemispheric corridor is needed.
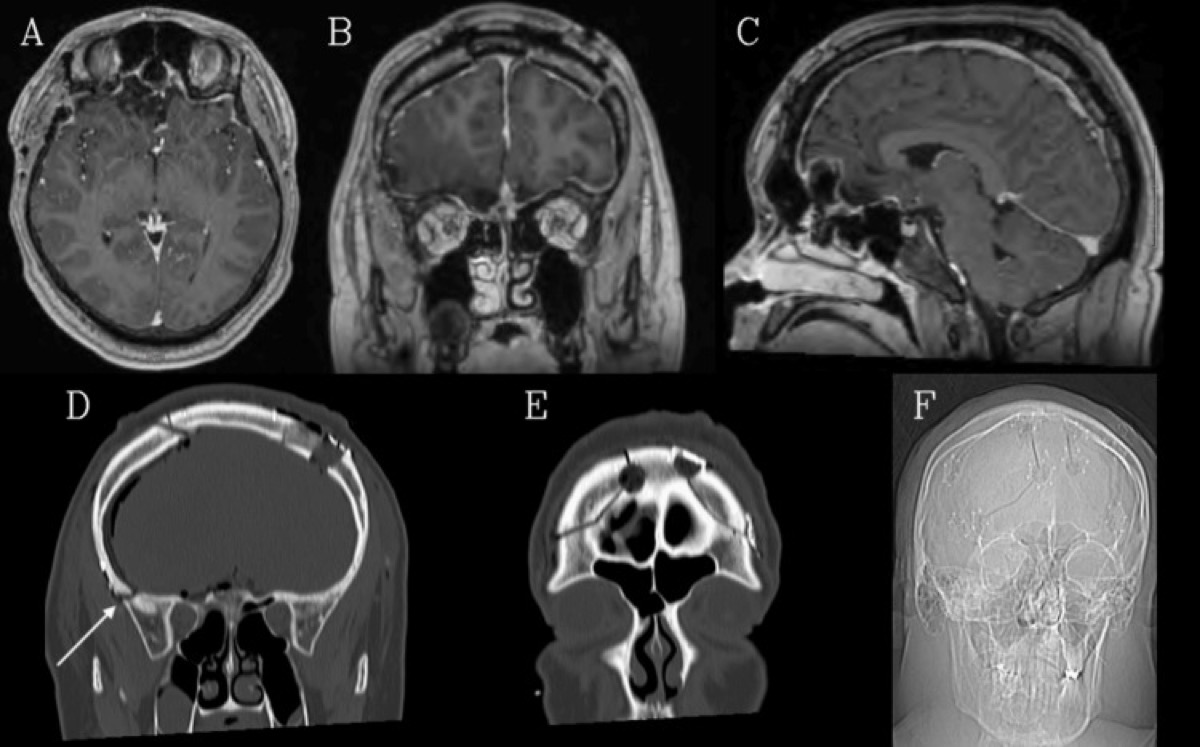
Cureus 2026;18:e101289 — CC BY 4.0. Bifrontal craniotomy outlines after midline anterior-skull-base tumor resection.
Subfrontal Exposure & Tumor Work
- After CSF release (lumbar drain), gently elevate the frontal lobes to expose the floor. Devascularize the tumor base early by coagulating the ethmoidal arteries at the cribriform; drill hyperostotic bone/crista galli and remove involved dura (Simpson grade).
- Internally debulk, then dissect the capsule off the frontal lobes, optic nerves/chiasm, and ACA–AComA complex posteriorly, preserving perforators. For invasive tumors, resect involved cribriform/ethmoid and plan a cranionasal reconstruction.
Tumor and Skull-Base Work Sequence
- Open cisterns or drain CSF after the dura is open to relax the frontal lobes.
- Identify both olfactory bulbs/tracts early; if preservation is unrealistic, sacrifice deliberately rather than avulsing them during retraction.
- Coagulate ethmoidal/cribriform dural supply at the base before deep debulking to reduce blood loss.
- Debulk centrally, then roll the capsule away from frontal lobes, optic nerves, chiasm, ACA/AComA, and perforators under direct vision.
- Drill hyperostotic crista galli/planum/orbital roof bone until healthy bone margins are reached, balancing Simpson grade with reconstruction risk.
- Treat invaded dura and sinonasal communication as a skull-base reconstruction problem, not merely a tumor-removal problem.
Intraoperative Rescue
- Frontal-lobe swelling: stop fixed retraction, drain CSF safely, optimize venous outflow/head position, mannitol/hyperventilation as appropriate, and avoid pushing deeper until the brain relaxes.
- Anterior SSS/falx bleeding: control with clips/suture/packing only in the anterior third; preserve posterior drainage and bridging veins.
- Ethmoidal artery bleeding into orbit: coagulate/clip at the cranial base before it retracts; monitor orbit and avoid orbital compartment syndrome.
- ACA/perforator adherence: leave a rind rather than avulsing a perforator; postoperative radiosurgery is better than an avoidable infarct.
- Unexpected sinus contamination: complete cranialization, remove mucosa, obliterate ducts, isolate with vascularized pericranium, and consider antibiotics/drainage strategy.
Closure & Anterior-Fossa Reconstruction
- Watertight dural closure (graft as needed); lay the vascularized pericranial flap across the anterior fossa floor to seal any dural/bony defect and separate cranium from sinonasal cavity — the cornerstone of CSF-leak prevention.
- Complete frontal-sinus cranialization; replace the bone flap; meticulous scalp closure. Lumbar drain managed per leak risk.
Nuances & Pitfalls (surgeon-level)
- Anosmia is expected with OGM resection — counsel preoperatively; bilateral olfactory tracts are usually sacrificed.
- Frontal sinus & pneumatized crista galli (see figure) are the CSF-leak/mucocele traps — cranialize the sinus and reconstruct the floor with pericranium.
- SSS: only the anterior third may be ligated; preserve the rest to avoid venous infarction.
- Frontal-lobe retraction/edema: relax with the lumbar drain and gravity; minimize/avoid fixed retraction; bifrontal contusion/edema causes abulia/cognitive change.
- Control the ethmoidal arteries early at the base — both to devascularize the tumor and to prevent retraction of a bleeding vessel into the orbit.
- Posterior limit: protect the optic apparatus and ACA complex; don’t chase tumor blindly into the chiasmatic/interpeduncular region.
- Harvest a generous pericranial flap at the start — you cannot make it later.
Complications
Anosmia; CSF rhinorrhea / mucocele; frontal-lobe retraction injury, edema/contusion, abulia/cognitive change; SSS/venous infarction; visual loss; ACA/perforator injury; seizures; wound/bone-flap infection; cosmetic/contour issues.
Cross-links
- Pathology: olfactory-groove-meningioma.md · tuberculum-sellae-meningioma.md
- Related corridors: supraorbital-keyhole-craniotomy.md · anterior-interhemispheric-approach.md · endoscopic-endonasal-approach.md · pterional-craniotomy.md
Figure Use & Attribution
About the figures. Copyrighted operative figures/videos are linked (Neurosurgical Atlas); embedded images are public-domain (Gray’s Anatomy) or CC‑BY (open-access), credited beneath each image. See media-sources.md and figures/CREDITS.md.
Atlas chapters: Olfactory Groove Meningioma (bifrontal technique) — Neurosurgical Atlas · Pterional Craniotomy
Chief-Level Corridor Review
Use these as the senior-level mental model for Bifrontal (Subfrontal) Craniotomy:
- Decision point: Define the exposure goal before incision: target, working angles, proximal/distal control, and the structure that cannot tolerate retraction.
- Technical lever: Know the first irreversible step: bone removal, dural opening, vascular control, or muscle/fascial division that commits the corridor.
- Bailout: Verbalize the bailout: extend exposure, change trajectory, add CSF drainage, obtain proximal control, convert to a larger corridor, or stop for imaging.
- Postop watch: Protect closure from the start: vascularized tissue, watertight dural/reconstruction plan, dead-space control, and drain strategy should be chosen before the final intradural step.
Common Pimp Questions
Use these to pressure-test preparation for Bifrontal (Subfrontal) Craniotomy:
- What patient position and head rotation make gravity work for this corridor?
- What named nerve, vessel, sinus, or muscle/fascial plane is most commonly injured?
- What bone work or soft-tissue step creates the exposure rather than simply using more retraction?
- What is the bailout if exposure is inadequate, bleeding occurs, or the brain is tight?
- What closure maneuver prevents the signature complication of this approach?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Exact head rotation/flexion/extension and pin placement: [attending-specific]
- Skin incision length, flap type, and muscle/fascial preservation technique: [attending-specific]
- Drill, rongeur, endoscope, microscope, retractor, and navigation preferences: [attending-specific]
- Drain use, closure materials, watertightness threshold, and postop imaging routine: [attending-specific]
Case Guides Using This Approach
References
- Tomasello F, et al. Bifrontal approach for anterior skull base meningiomas (olfactory tract preservation considerations).
- Spektor S, et al. Olfactory groove meningiomas: comparison of bifrontal vs unilateral approaches.
- DeMonte F, et al. Anterior skull base surgery and pericranial flap reconstruction.
- Crista Galli Pneumatization Complicating Olfactory Groove Meningioma Resection. Cureus. 2026;18:e101289. CC BY 4.0. (figures embedded above) — PMC12889192
- Cohen-Gadol AA. Olfactory Groove Meningioma / bifrontal technique. The Neurosurgical Atlas. link