
Case Prep: Olfactory Groove Meningioma Resection
Case / Approach Snapshot
- Anatomy at risk: tumor compartment, arterial supply, venous drainage/sinuses, cranial nerves, white-matter tracts, pituitary/CSF pathways when relevant, and functional cortex.
- Operative steps: review imaging and goals, choose exposure, obtain brain relaxation, devascularize when possible, debulk internally, dissect capsule from critical structures, verify extent/safety, and reconstruct watertight closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: venous or arterial injury, swelling, seizure, cranial nerve or endocrine change, CSF leak, residual tumor left for safety, staged surgery, radiation, or adjuvant therapy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [size] cm olfactory groove meningioma presenting with [anosmia / personality change / visual decline / headache] planned for [bifrontal / pterional / supraorbital / endoscopic endonasal] approach for resection.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Bifrontal craniotomy — detailed corridor setup, step-by-step technique & figures
Operative figures/atlases are © (linked, not copied). See media-sources.md.
- Technique/approach: The Neurosurgical Atlas — search “olfactory groove meningioma”
- Imaging: Radiopaedia — olfactory groove meningioma
- Open-access figures: PubMed Central
High-Yield Literature
- Olfactory groove meningioma — Adappa ND. Otolaryngologic clinics of North America 2011. PubMed
- Olfactory groove and tuberculum sellae meningioma resection by endoscopic endonasal approach versus transcranial approach: A systematic review and meta-analysis of comparative studies — Lu VM. Clinical neurology and neurosurgery 2018. PubMed
- Smell Outcomes in Olfactory Groove Meningioma Resection Through Unilateral versus Bilateral Transcranial Approaches: A Systematic Review and Meta-analysis — Bamimore MA. World neurosurgery 2022. PubMed
- Exoscopic resection of giant olfactory groove meningioma — Calvanese F. Neurosurgical focus: Video 2024. PubMed
- Transorbital Approach for Olfactory Groove Meningioma — Noiphithak R. World neurosurgery 2022. PubMed
- Taste dysfunction after endoscopic endonasal resection of olfactory groove meningioma: Case series and review of the literature — Fecker AL. American journal of otolaryngology 2024. PubMed
- Nuances of Olfactory Groove Meningioma Surgery: 2-Dimensional Operative Video — Mooney MA. Operative neurosurgery (Hagerstown, Md.) 2021. PubMed
- Endoscopic Endonasal Resection-Olfactory Groove Meningioma: 2-Dimensional Operative Video — Champagne PO. Operative neurosurgery (Hagerstown, Md.) 2020. PubMed
- Prognostic factors for olfactory groove meningioma with nasal cavity extension — Zhang J. Oncotarget 2018. PubMed
- Olfactory groove meningioma presenting solely with visual impairment: illustrative case — Abu Saadeh O. Journal of neurosurgery. Case lessons 2025. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
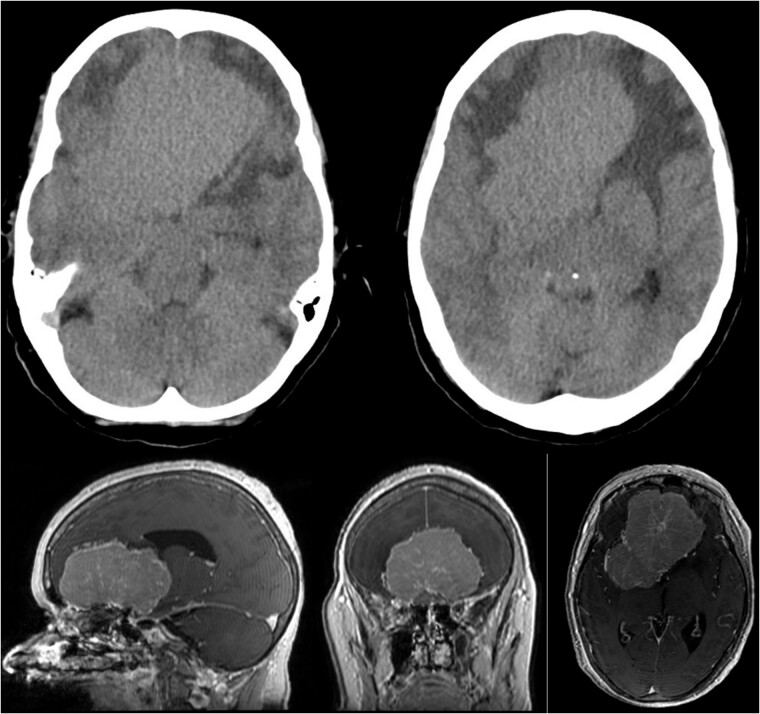 Figure 1. Showing the CT imaging with a hypodense fronto-basal lesion with finger-shaped perifocal edema and the T1-weighted MRI image with homogenous contrast-enhancing frontobasal lesion… Source: Bilateral cranioorbital foramina (Hyrtl foramina): crucial anatomical findings in the management of giant olfactory groove meningioma - a case report and literature review — Journal of Surgical Case Reports 2024; CC BY.
Figure 1. Showing the CT imaging with a hypodense fronto-basal lesion with finger-shaped perifocal edema and the T1-weighted MRI image with homogenous contrast-enhancing frontobasal lesion… Source: Bilateral cranioorbital foramina (Hyrtl foramina): crucial anatomical findings in the management of giant olfactory groove meningioma - a case report and literature review — Journal of Surgical Case Reports 2024; CC BY.
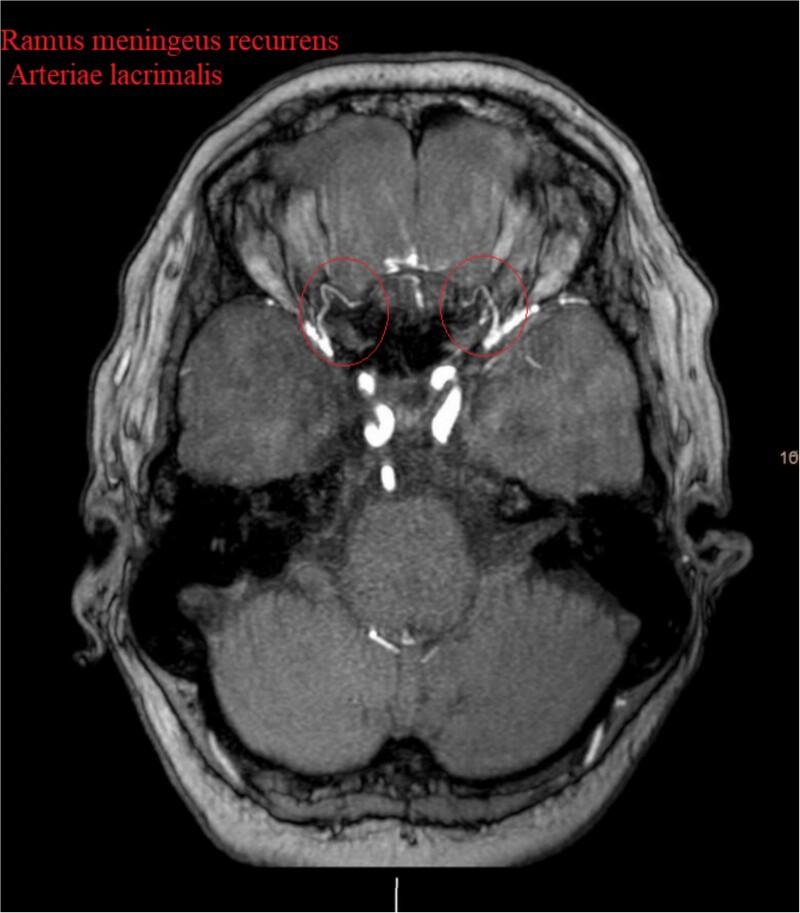 Figure 2. Show the MRA with the bilateral anastomotic branch of the lacrimal artery with the middle meningeal artery. Source: Bilateral cranioorbital foramina (Hyrtl foramina): crucial anatomical findings in the management of giant olfactory groove meningioma - a case report and literature review — Journal of Surgical Case Reports 2024; CC BY.
Figure 2. Show the MRA with the bilateral anastomotic branch of the lacrimal artery with the middle meningeal artery. Source: Bilateral cranioorbital foramina (Hyrtl foramina): crucial anatomical findings in the management of giant olfactory groove meningioma - a case report and literature review — Journal of Surgical Case Reports 2024; CC BY.
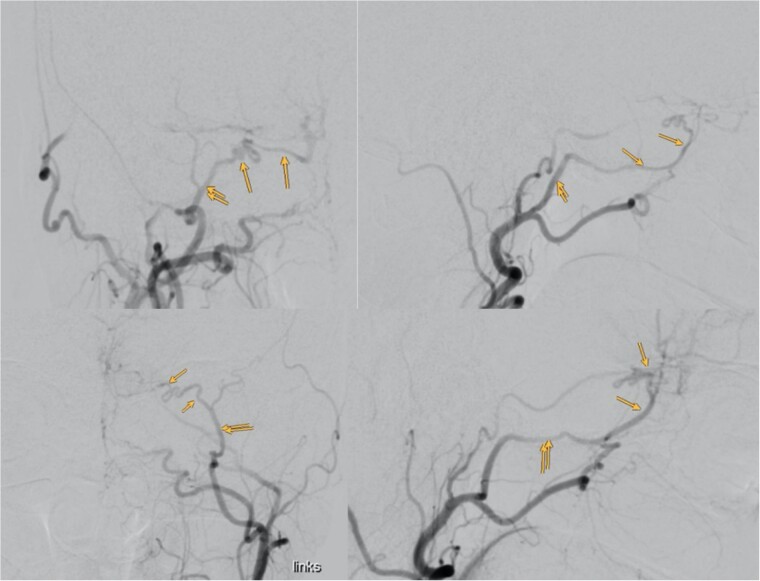 Figure 3. Showing the digital subtraction angiography of the left external carotid artery in four perspectives: posteroanterior view (upper left), lateral view (upper right), posteroanterior view… Source: Bilateral cranioorbital foramina (Hyrtl foramina): crucial anatomical findings in the management of giant olfactory groove meningioma - a case report and literature review — Journal of Surgical Case Reports 2024; CC BY.
Figure 3. Showing the digital subtraction angiography of the left external carotid artery in four perspectives: posteroanterior view (upper left), lateral view (upper right), posteroanterior view… Source: Bilateral cranioorbital foramina (Hyrtl foramina): crucial anatomical findings in the management of giant olfactory groove meningioma - a case report and literature review — Journal of Surgical Case Reports 2024; CC BY.
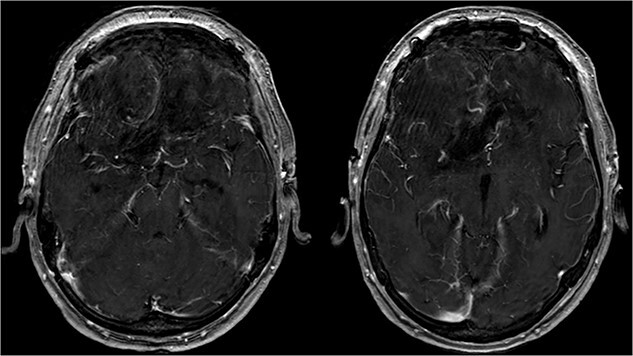 Figure 4. Showing the postoperative T1-weighted MRI with no residual tumor tissue. Source: Bilateral cranioorbital foramina (Hyrtl foramina): crucial anatomical findings in the management of giant olfactory groove meningioma - a case report and literature review — Journal of Surgical Case Reports 2024; CC BY.
Figure 4. Showing the postoperative T1-weighted MRI with no residual tumor tissue. Source: Bilateral cranioorbital foramina (Hyrtl foramina): crucial anatomical findings in the management of giant olfactory groove meningioma - a case report and literature review — Journal of Surgical Case Reports 2024; CC BY.
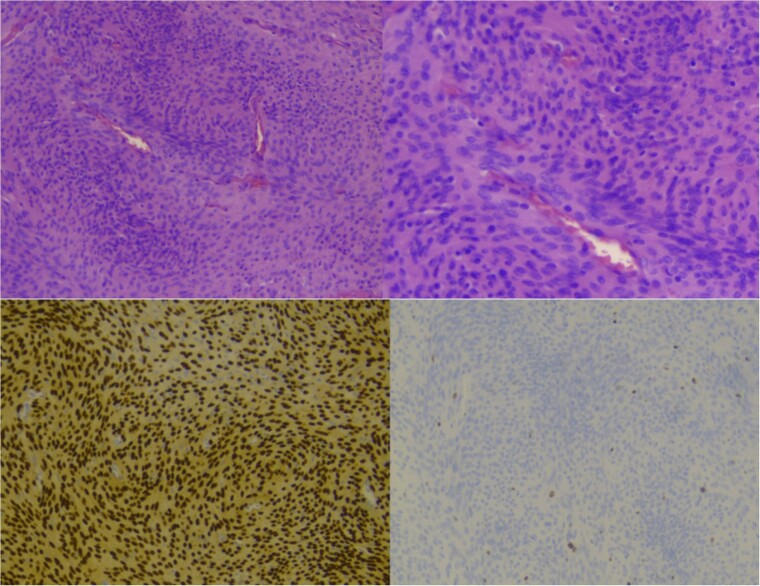 Figure 5. Showing staining with hematoxylin and eosin, low power lens (upper left), high power lens (upper right) and moleculopathological analysis with ki67 (lower left), progesteron receptor… Source: Bilateral cranioorbital foramina (Hyrtl foramina): crucial anatomical findings in the management of giant olfactory groove meningioma - a case report and literature review — Journal of Surgical Case Reports 2024; CC BY.
Figure 5. Showing staining with hematoxylin and eosin, low power lens (upper left), high power lens (upper right) and moleculopathological analysis with ki67 (lower left), progesteron receptor… Source: Bilateral cranioorbital foramina (Hyrtl foramina): crucial anatomical findings in the management of giant olfactory groove meningioma - a case report and literature review — Journal of Surgical Case Reports 2024; CC BY.
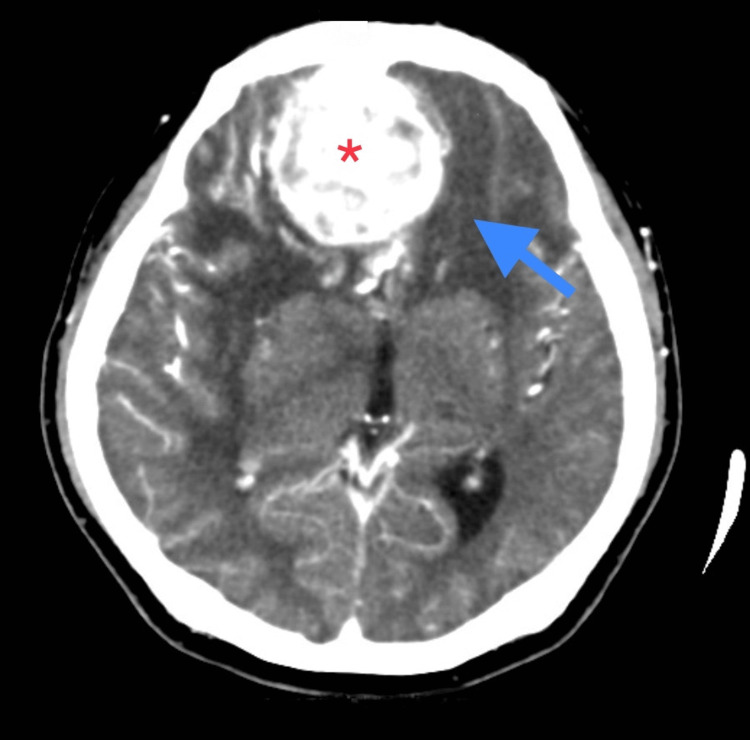 Figure 1. CECT Brain (axial view) showing bi-frontal extra-axial space-occupying lesion (red asterisk) measuring 4.8 x 5.0 x 4.8 cm with skull base erosion. There is a presence of perilesional… Source: Visual Loss As Primary Manifestation of Olfactory Groove Meningioma — Cureus 2023; CC BY.
Figure 1. CECT Brain (axial view) showing bi-frontal extra-axial space-occupying lesion (red asterisk) measuring 4.8 x 5.0 x 4.8 cm with skull base erosion. There is a presence of perilesional… Source: Visual Loss As Primary Manifestation of Olfactory Groove Meningioma — Cureus 2023; CC BY.
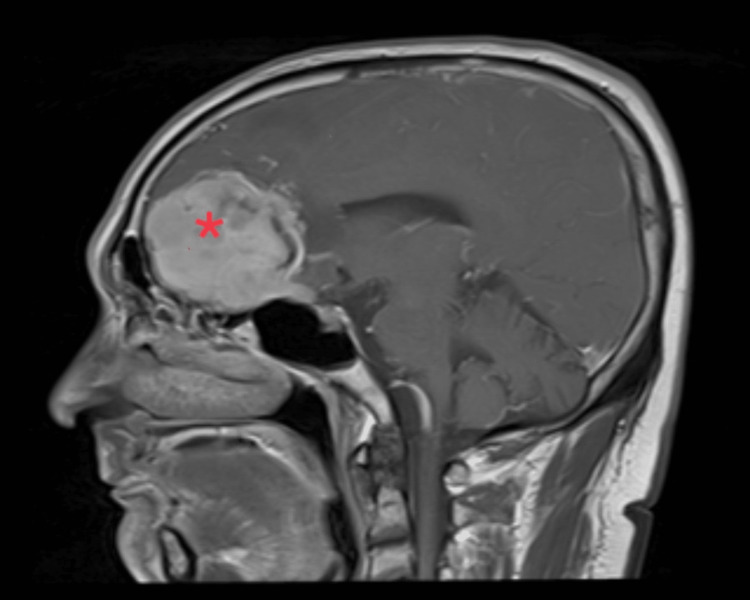 Figure 2. MRI (sagittal view) showing the anterior skull base meningioma (red asterisk) causing mass effect (right more than left), left midline shift, and contralateral early hydrocephalus. Source: Visual Loss As Primary Manifestation of Olfactory Groove Meningioma — Cureus 2023; CC BY.
Figure 2. MRI (sagittal view) showing the anterior skull base meningioma (red asterisk) causing mass effect (right more than left), left midline shift, and contralateral early hydrocephalus. Source: Visual Loss As Primary Manifestation of Olfactory Groove Meningioma — Cureus 2023; CC BY.
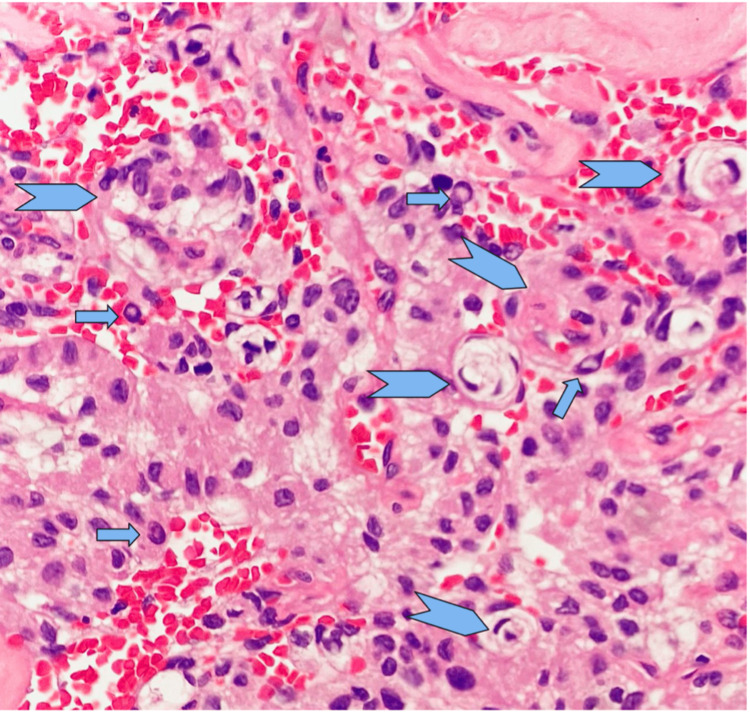 Figure 3. A generally uniform oval nucleus with a central clearing (arrow) and an indistinct cytoplasmic border. In areas, vague whorls of tumour cells are also present (arrow head). Source: Visual Loss As Primary Manifestation of Olfactory Groove Meningioma — Cureus 2023; CC BY.
Figure 3. A generally uniform oval nucleus with a central clearing (arrow) and an indistinct cytoplasmic border. In areas, vague whorls of tumour cells are also present (arrow head). Source: Visual Loss As Primary Manifestation of Olfactory Groove Meningioma — Cureus 2023; CC BY.
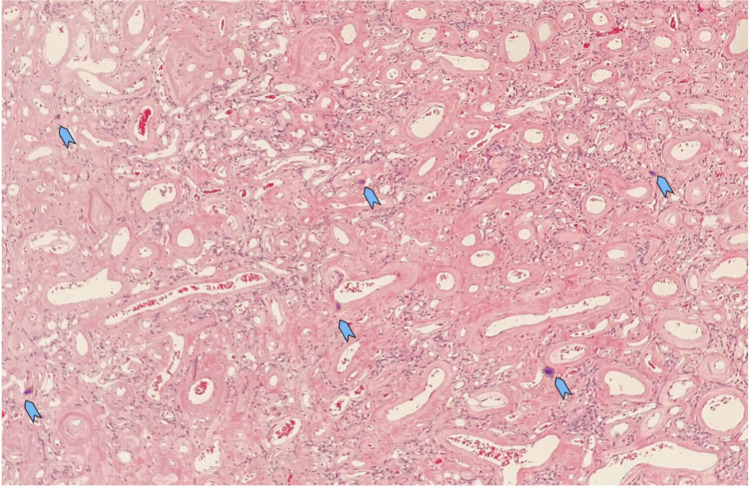 Figure 4. The vascular channels are variable in size with a thickened hyalinised wall. There are several foci of tiny psammoma bodies noted (arrow head) Source: Visual Loss As Primary Manifestation of Olfactory Groove Meningioma — Cureus 2023; CC BY.
Figure 4. The vascular channels are variable in size with a thickened hyalinised wall. There are several foci of tiny psammoma bodies noted (arrow head) Source: Visual Loss As Primary Manifestation of Olfactory Groove Meningioma — Cureus 2023; CC BY.
 Figure 10. Source: Modern Microsurgical Resection of Olfactory Groove Meningiomas by Classical Bicoronal Subfrontal Approach without Orbital Osteotomies — Asian J Neurosurg. 2018 Apr-Jun;13(2):258–63. doi: 10.4103/ajns.AJNS_66_16; CC BY-NC-SA.
Figure 10. Source: Modern Microsurgical Resection of Olfactory Groove Meningiomas by Classical Bicoronal Subfrontal Approach without Orbital Osteotomies — Asian J Neurosurg. 2018 Apr-Jun;13(2):258–63. doi: 10.4103/ajns.AJNS_66_16; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Anosmia (often unnoticed), personality/cognitive change (frontal), visual decline (posterior extension to optic apparatus), headache
- Foster Kennedy syndrome (classic): ipsilateral optic atrophy + contralateral papilledema + anosmia
- Often large at presentation (frontal lobes silent)
Imaging Review
MRI (T1+Gad, T2, FLAIR)
- Midline anterior skull base mass, bilateral often
- Size, posterior extension to planum/tuberculum/optic apparatus
- Anterior cerebral artery (ACA/A2) relationship — vessels often draped over posterior tumor
- Peritumoral edema, brain invasion, vascular supply (ethmoidal/ophthalmic branches)
- Sinus/cribriform invasion (transcranial vs endonasal planning)
CT
- Hyperostosis, cribriform plate erosion, ethmoid/sinus extension
Ophthalmology
- Acuity, fields, fundoscopy
Labs
- CBC, BMP, Coags, Type and crossmatch
Neurological Examination
- Smell (each nostril), vision, frontal/cognitive/behavioral assessment
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: Mayfield, navigation with latest MRI/DTI/functional data, microscope/exoscope, ultrasound/5-ALA/fluorescence when used, CUSA, cortical/subcortical mapping tools for eloquent lesions, and specimens/pathology workflow ready.
- Special needs: arterial line for large/eloquent/vascular tumors, dexamethasone plan, seizure prophylaxis for cortical lesions or seizure history, mannitol/hypertonic availability, language/motor mapping plan, and blood available for meningioma/skull-base cases.
- Immediate postop orders: neuro checks with deficit-specific exam, MRI brain with contrast within 24-48h when resection assessment matters, CT for hemorrhage concern, dex taper, antiepileptic duration, DVT timing, pathology/molecular follow-up, and rehab consults as needed.
Approach Selection
- Bifrontal: Wide exposure for large tumors, bilateral; access to cribriform; allows skull base repair
- Pterional / unilateral subfrontal: Lateral-to-medial, early ACA/optic control, less brain retraction (good for small-moderate)
- Supraorbital (eyebrow) keyhole: Small-moderate tumors, minimally invasive
- Endoscopic endonasal: Selected tumors (devascularizes base early, no brain retraction) but anosmia guaranteed, CSF leak/reconstruction challenge; limited for large lateral extension
Position
- Bifrontal/supraorbital: supine, neutral, slight extension (frontal lobes fall back), Mayfield
- Pterional: rotated 20-30 degrees contralateral
Key Surgical Steps (Bifrontal example)
- Bicoronal incision, pericranial flap harvested (for skull base repair)
- Bifrontal craniotomy (low to floor of anterior fossa); may ligate/divide anterior SSS and falx
- Early devascularization of tumor base along cribriform/planum (ethmoidal feeders)
- Open dura, internal debulking (CUSA)
- Circumferential dissection; identify and protect ACA/A2 complex posteriorly (draped over tumor)
- Protect optic nerves/chiasm at posterior margin
- Resect hyperostotic cribriform bone, dura (Simpson I)
- Anterior skull base reconstruction — vascularized pericranial flap; multilayer repair to prevent CSF leak
- Hemostasis, closure
Critical Anatomy & Structures at Risk
- ACA / A2 / frontopolar arteries — posterior tumor surface; injury → frontal infarct
- Optic nerves / chiasm — posterior extension
- Frontal lobes — minimize retraction (cognitive/personality)
- Anterior skull base / cribriform — CSF leak source; needs robust repair
- Superior sagittal sinus (anterior) — may ligate anterior third
Equipment
- Microscope (± endoscope), navigation, CUSA, high-speed drill
- Pericranial flap for reconstruction, dural substitute, sealant
- Lumbar drain (optional), ICG
Monitoring
- SSEPs; VEPs (optional)
Anesthesia
- Arterial line, crossmatched blood, mannitol, dexamethasone, lumbar drain optional
Potential Complications
- CSF rhinorrhea (cribriform defect) — robust vascularized repair
- ACA injury → frontal infarct
- Visual decline
- Frontal lobe/cognitive dysfunction (retraction)
- Anosmia (expected), meningitis
Operative Note Template
Preoperative Diagnosis: Olfactory groove meningioma [with anosmia / visual decline / frontal dysfunction]
Postoperative Diagnosis: Same
Procedure: [Bifrontal] craniotomy for resection of olfactory groove meningioma with anterior skull base reconstruction
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids / Blood products: [crossmatched] Adjuncts: Neuronavigation, CUSA, high-speed drill, ICG; [lumbar drain] Implants: Vascularized pericranial flap, dural substitute, sealant Complications: None
Indications: [Age]yo [M/F] with a large olfactory groove meningioma causing [cognitive change/visual decline/anosmia]. A bifrontal approach was chosen for this large midline tumor with skull base reconstruction. Risks (CSF rhinorrhea, ACA injury, frontal/cognitive dysfunction, visual change) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and navigation registered. A bicoronal incision was made and a vascularized pericranial flap harvested for skull base repair. A bifrontal craniotomy was performed low to the anterior fossa floor [with anterior SSS/falx division], and the dura opened.
The tumor base along the cribriform/planum was devascularized early (ethmoidal feeders). The tumor was internally debulked (CUSA) and dissected circumferentially, identifying and protecting the ACA/A2 complex draped over the posterior tumor and the optic nerves/chiasm posteriorly. Hyperostotic cribriform bone and involved dura were resected (Simpson I). A multilayer anterior skull base reconstruction was performed with the vascularized pericranial flap and sealant to prevent CSF leak.
Hemostasis was obtained, the bone flap replaced, and the wound closed in layers. The patient was transferred to the ICU with CSF-leak precautions.
Postoperative Plan
- ICU, neuro checks q1h
- CSF leak precautions (HOB, no straining/nose blowing); lumbar drain if placed
- CT/MRI postop, watch for rhinorrhea, pneumocephalus
- Steroid taper, seizure prophylaxis, DVT prophylaxis
- Ophthalmology follow-up; cognitive assessment
Chief-Level Case Review
Use these as the senior-level mental model for Olfactory Groove Meningioma Resection:
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Olfactory Groove Meningioma Resection:
- What is the surgical goal: gross-total, maximal safe, decompression, diagnosis, or cytoreduction?
- What eloquent cortex, tract, cranial nerve, vessel, or sinus defines the stopping point?
- What adjunct changes the case: navigation, mapping, 5-ALA, ultrasound, endoscope, ICG, or neuromonitoring?
- What is the edema, steroid, seizure, DVT, and postop imaging plan?
- What complication would you check for first in PACU based on this lesion location?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Extent-of-resection goal and functional stopping points: [attending-specific]
- Mapping/monitoring, 5-ALA, ultrasound, ICG, endoscope, or tractography preferences: [attending-specific]
- Steroid, antiepileptic, mannitol/hypertonic saline, and antibiotic plan: [attending-specific]
- Postop MRI timing, ICU/floor threshold, and adjuvant-referral workflow: [attending-specific]