
Case Prep: Anterior Cervical Discectomy and Fusion (ACDF)
Case / Approach Snapshot
- Anatomy at risk: level localization, cord/cauda equina, exiting and traversing roots, dura, vertebral artery or segmental vessels, esophagus/trachea/pleura/viscera by approach, and fusion/instrumentation landmarks.
- Operative steps: position and pad carefully, confirm level, expose the planned corridor, decompress neural elements, reconstruct or instrument when indicated, verify alignment/hardware, and close with attention to hematoma and wound risk; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: wrong level, durotomy, neurologic change, vertebral artery/visceral/pleural injury, graft or hardware problem, epidural hematoma, dysphagia/airway issue, and infection prevention/escalation.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [cervical radiculopathy / cervical myelopathy / both] at [C_-C_] due to [disc herniation / spondylosis / OPLL] presenting with [arm pain/weakness / gait difficulty / hand clumsiness] planned for [single/multi]-level ACDF at [C_-C_].
Figures, Imaging & Video
🎥 Operative video — Inside the OR: Anterior Cervical Discectomy & Fusion · Antonio J. Webb, MD
More operative video: YouTube ▸ · Neurosurgical Atlas ▸
🧭 Operative approach: Anterior cervical (Smith-Robinson) approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Complications of Anterior Cervical Discectomy and Fusion — Robertson SC. Acta neurochirurgica. Supplement 2023. PubMed
- Pharyngesophageal Diverticula Following Anterior Cervical Discectomy and Fusion — Beesley H. The Annals of otology, rhinology, and laryngology 2023. PubMed
- Anterior cervical discectomy and fusion (ACDF) with and without plating: A comparison of radiological and clinical outcomes — Bębenek A. Advances in clinical and experimental medicine : official organ Wroclaw Medical University 2024. PubMed
- Anterior cervical discectomy and fusion: review and update for radiologists — Kani KK. Skeletal radiology 2018. PubMed
- Outpatient anterior cervical discectomy and fusion: A meta-analysis — McClelland S 3rd. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia 2016. PubMed
- Postoperative complications of anterior cervical discectomy and fusion: A comprehensive systematic review and meta-analysis — Tavanaei R. North American Spine Society journal 2025. PubMed
- Safety of Outpatient Anterior Cervical Discectomy and Fusion: A Systematic Review and Meta-Analysis — Yerneni K. Neurosurgery 2020. PubMed
- Dysphagia as a Postoperative Complication of Anterior Cervical Discectomy and Fusion — Tsalimas G. Cureus 2022. PubMed
- Horner Syndrome After Anterior Cervical Discectomy and Fusion: Case Series and Systematic Review — Lubelski D. World neurosurgery 2020. PubMed
- Anterior Cervical Discectomy and Fusion combined with thyroid gland surgery, a tailored case and literature review — Themistoklis KM. BMC musculoskeletal disorders 2019. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
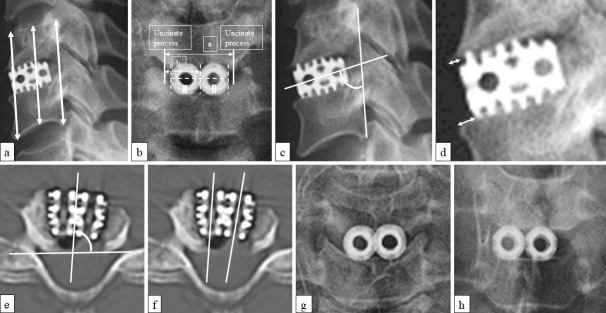 Fig. 1. Various methods of radiographic measurement and representative of both centering cages, which caused no subsidence, and offset cages, which caused subsidence.a) Radiographic measurements… Source: Radiological Factors Affecting Cage Subsidence after Single-level Anterior Cervical Discectomy and Fusion with Double Titanium Cylindrical Cages — Neurologia medico-chirurgica 2025; CC BY-NC-ND.
Fig. 1. Various methods of radiographic measurement and representative of both centering cages, which caused no subsidence, and offset cages, which caused subsidence.a) Radiographic measurements… Source: Radiological Factors Affecting Cage Subsidence after Single-level Anterior Cervical Discectomy and Fusion with Double Titanium Cylindrical Cages — Neurologia medico-chirurgica 2025; CC BY-NC-ND.
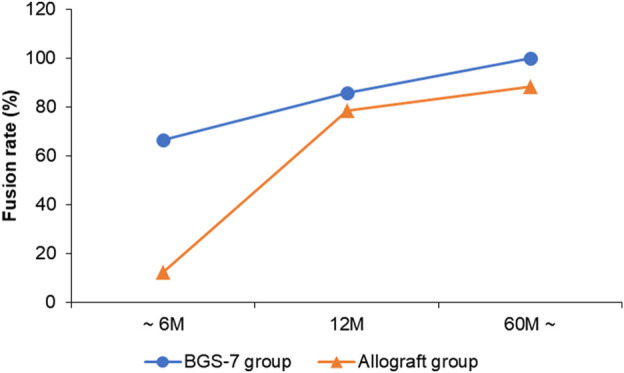 FIGURE 1. Fusion rate of each group over time. Source: Long-term results comparison after anterior cervical discectomy with BGS-7 spacer (NOVOMAX®-C) and allograft spacer: A prospective observational study — Frontiers in Bioengineering and Biotechnology 2023; CC BY.
FIGURE 1. Fusion rate of each group over time. Source: Long-term results comparison after anterior cervical discectomy with BGS-7 spacer (NOVOMAX®-C) and allograft spacer: A prospective observational study — Frontiers in Bioengineering and Biotechnology 2023; CC BY.
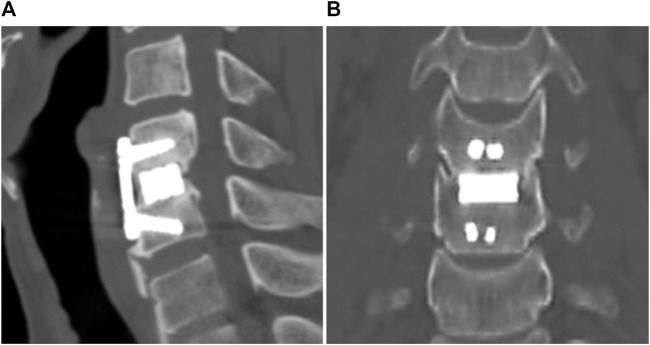 FIGURE 2. One year post-operative images from CT scan. (A) Sagittal view, (B) coronal view. Source: Long-term results comparison after anterior cervical discectomy with BGS-7 spacer (NOVOMAX®-C) and allograft spacer: A prospective observational study — Frontiers in Bioengineering and Biotechnology 2023; CC BY.
FIGURE 2. One year post-operative images from CT scan. (A) Sagittal view, (B) coronal view. Source: Long-term results comparison after anterior cervical discectomy with BGS-7 spacer (NOVOMAX®-C) and allograft spacer: A prospective observational study — Frontiers in Bioengineering and Biotechnology 2023; CC BY.
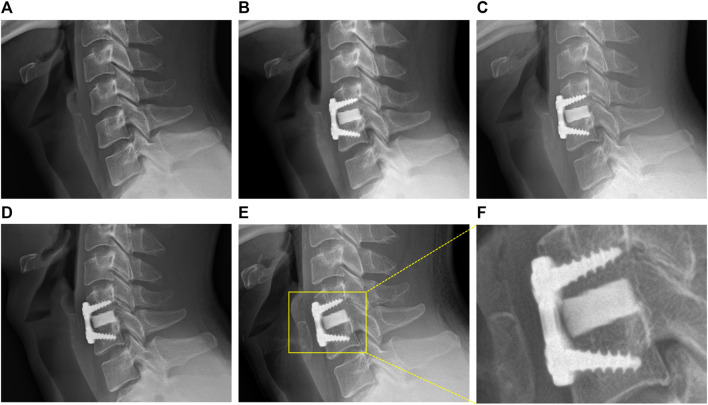 FIGURE 3. Representative images of BGS-7 spacer-induced segmental fusion progression after ACDF surgery during 5 years. (A) Pre-OP, (B) 1 month, (C) 3 months, (D) 1 year, (E) present, (F) present… Source: Long-term results comparison after anterior cervical discectomy with BGS-7 spacer (NOVOMAX®-C) and allograft spacer: A prospective observational study — Frontiers in Bioengineering and Biotechnology 2023; CC BY.
FIGURE 3. Representative images of BGS-7 spacer-induced segmental fusion progression after ACDF surgery during 5 years. (A) Pre-OP, (B) 1 month, (C) 3 months, (D) 1 year, (E) present, (F) present… Source: Long-term results comparison after anterior cervical discectomy with BGS-7 spacer (NOVOMAX®-C) and allograft spacer: A prospective observational study — Frontiers in Bioengineering and Biotechnology 2023; CC BY.
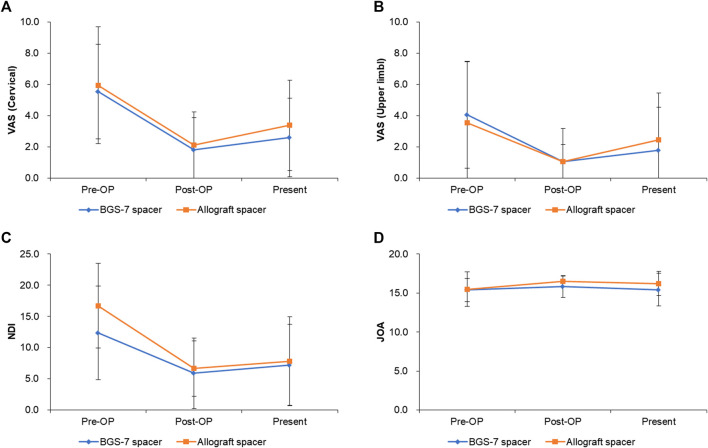 FIGURE 4. Clinical outcomes for each group after ACDF surgery during 5 years. (A) VAS (cervical), (B) VAS(upper limb), (C) NDI, (D) JOA. Source: Long-term results comparison after anterior cervical discectomy with BGS-7 spacer (NOVOMAX®-C) and allograft spacer: A prospective observational study — Frontiers in Bioengineering and Biotechnology 2023; CC BY.
FIGURE 4. Clinical outcomes for each group after ACDF surgery during 5 years. (A) VAS (cervical), (B) VAS(upper limb), (C) NDI, (D) JOA. Source: Long-term results comparison after anterior cervical discectomy with BGS-7 spacer (NOVOMAX®-C) and allograft spacer: A prospective observational study — Frontiers in Bioengineering and Biotechnology 2023; CC BY.
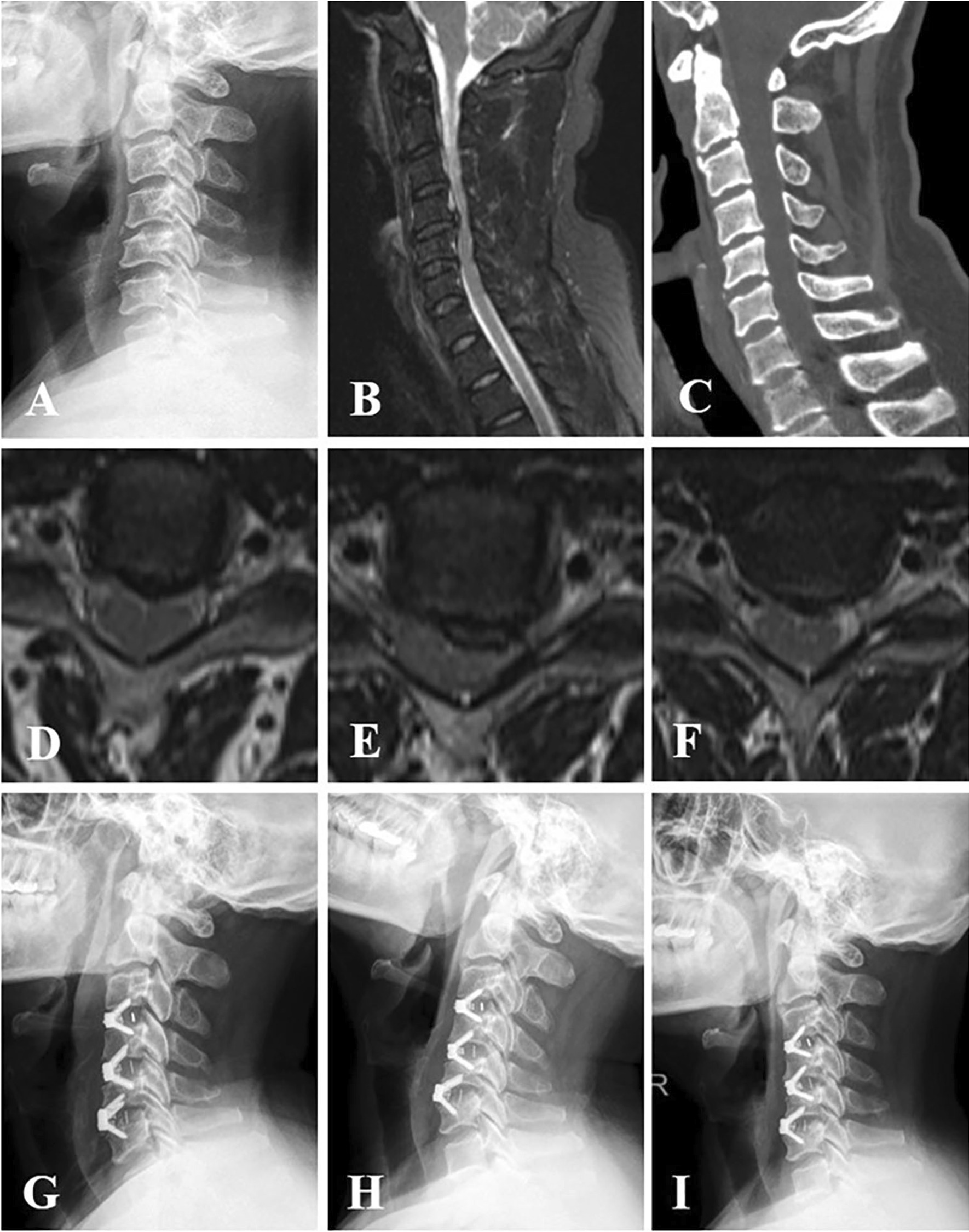 Fig. 1. A 53-year-old man who had experienced numbness in both hands and felt stepping on cotton in lower limbs for 1.5 years was diagnosed as cervical spondylotic myelopathy. A Preoperative… Source: Clinical and imaging outcomes of self-locking stand-alone cages and anterior cage-with-plate in three-level anterior cervical discectomy and fusion: a retrospective comparative study — Journal of Orthopaedic Surgery and Research 2023; CC BY.
Fig. 1. A 53-year-old man who had experienced numbness in both hands and felt stepping on cotton in lower limbs for 1.5 years was diagnosed as cervical spondylotic myelopathy. A Preoperative… Source: Clinical and imaging outcomes of self-locking stand-alone cages and anterior cage-with-plate in three-level anterior cervical discectomy and fusion: a retrospective comparative study — Journal of Orthopaedic Surgery and Research 2023; CC BY.
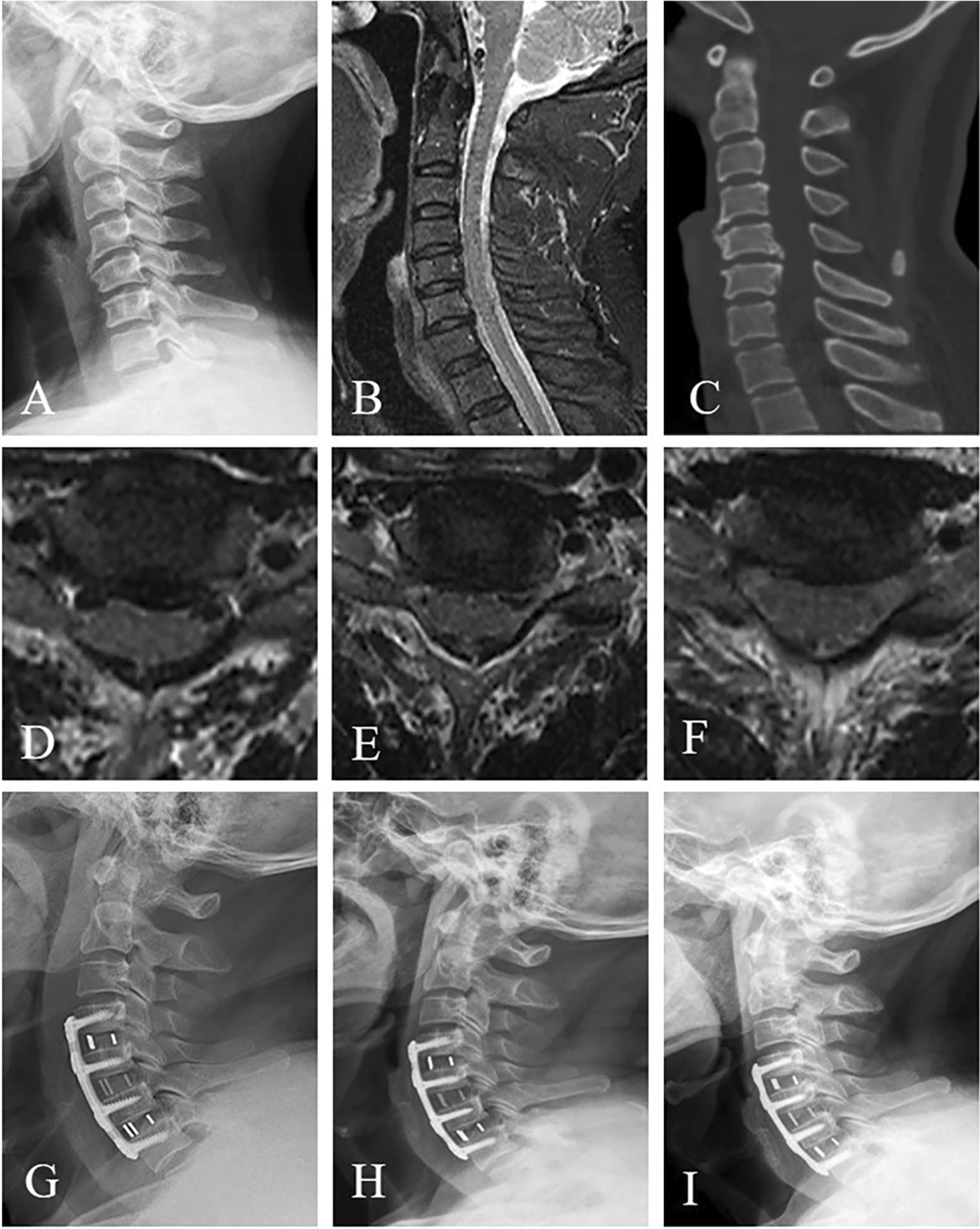 Fig. 2. A 63-year-old man who had experienced numbness in both hands and felt stepping on cotton in lower limbs for 3 years was diagnosed as cervical spondylotic myelopathy. A Preoperative… Source: Clinical and imaging outcomes of self-locking stand-alone cages and anterior cage-with-plate in three-level anterior cervical discectomy and fusion: a retrospective comparative study — Journal of Orthopaedic Surgery and Research 2023; CC BY.
Fig. 2. A 63-year-old man who had experienced numbness in both hands and felt stepping on cotton in lower limbs for 3 years was diagnosed as cervical spondylotic myelopathy. A Preoperative… Source: Clinical and imaging outcomes of self-locking stand-alone cages and anterior cage-with-plate in three-level anterior cervical discectomy and fusion: a retrospective comparative study — Journal of Orthopaedic Surgery and Research 2023; CC BY.
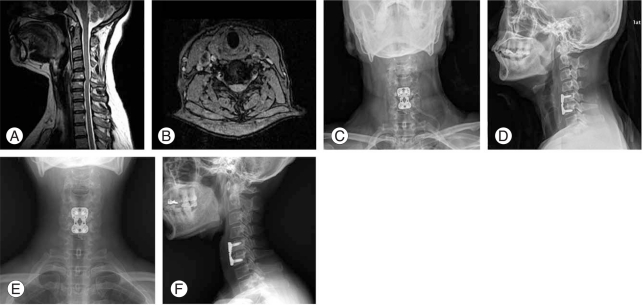 Fig. 1. A 45-year-old female diagnosed with spinal stenosis at C5-6. (A, B) Preoperative magnetic resonance imaging. (C, D) Postoperative radiographs. (E, F) Follow-up radiograph 12 months… Source: Comparative Study of Clinical Outcomes of Anterior Cervical Discectomy and Fusion Using Autobone Graft or Cage with Bone Substitute — Asian Spine Journal 2011; CC BY-NC.
Fig. 1. A 45-year-old female diagnosed with spinal stenosis at C5-6. (A, B) Preoperative magnetic resonance imaging. (C, D) Postoperative radiographs. (E, F) Follow-up radiograph 12 months… Source: Comparative Study of Clinical Outcomes of Anterior Cervical Discectomy and Fusion Using Autobone Graft or Cage with Bone Substitute — Asian Spine Journal 2011; CC BY-NC.
 Fig. 2. A 47-year-old female diagnosed with herniated nucleus pulposus on C5-6. (A, B) Preoperative magnetic resonance imaging. (C, D) Postoperative radiograph. (E, F) Follow-up radiograph taken… Source: Comparative Study of Clinical Outcomes of Anterior Cervical Discectomy and Fusion Using Autobone Graft or Cage with Bone Substitute — Asian Spine Journal 2011; CC BY-NC.
Fig. 2. A 47-year-old female diagnosed with herniated nucleus pulposus on C5-6. (A, B) Preoperative magnetic resonance imaging. (C, D) Postoperative radiograph. (E, F) Follow-up radiograph taken… Source: Comparative Study of Clinical Outcomes of Anterior Cervical Discectomy and Fusion Using Autobone Graft or Cage with Bone Substitute — Asian Spine Journal 2011; CC BY-NC.
History of Present Illness
- Chief complaint: Radicular arm pain (dermatomal) / myelopathy symptoms / neck pain
- Duration and progression:
- Radiculopathy:
- Pain distribution (which dermatome): C5 (lateral arm), C6 (lateral forearm, thumb/index), C7 (posterior arm, middle finger), C8 (medial forearm, ring/small), T1 (medial arm)
- Weakness pattern:
- Numbness pattern:
- Failed conservative management (PT, NSAIDs, injections): duration ___
- Myelopathy:
- Gait instability / balance difficulty
- Hand clumsiness / fine motor difficulty (buttons, writing)
- Hoffmann sign, hyperreflexia
- Bowel/bladder symptoms
- mJOA score: ___ / 18 (< 12 = moderate myelopathy; < 9 = severe)
- Nurick grade:
- Neck pain (axial):
Past Medical History
- Prior cervical spine surgery
- Dysphagia (baseline — critical for ACDF approach)
- Vocal cord pathology / hoarseness (get ENT eval if prior anterior cervical surgery or hoarseness)
- GERD
- Thyroid surgery (recurrent laryngeal nerve at risk)
- Smoking (fusion rates reduced)
- Diabetes (affects fusion and wound healing)
- Osteoporosis (subsidence risk)
- Rheumatoid arthritis (atlantoaxial instability, subaxial disease)
- Allergies:
- Medications (NSAIDs, steroids):
Imaging Review
X-rays (AP, Lateral, Flexion/Extension)
- Alignment: Lordosis maintained / kyphosis / straightened
- Disc height loss at involved levels
- Osteophytes
- Spondylolisthesis
- Flexion/extension: Dynamic instability (> 3.5 mm translation or > 11 degrees angulation)
- Number of levels to fuse and impact on overall cervical motion
MRI Cervical Spine
- Disc herniation: Location (central, paracentral, foraminal), size, direction
- Cord compression: Yes/no, degree
- Cord signal change: T2 hyperintensity (myelomalacia/edema = worse prognosis for myelopathy recovery)
- Foraminal stenosis: Degree at each level
- Level(s) correlating with symptoms:
- Adjacent segment disease: Pre-existing degeneration above/below planned fusion
CT Cervical Spine
- Bony anatomy for approach planning
- Osteophyte anatomy (uncovertebral joint osteophytes = foraminal stenosis)
- OPLL presence and type (segmental, continuous, mixed)
- Endplate morphology
Navigation (if used)
- CT loaded for intraoperative navigation
- Level confirmation planned with fluoroscopy
Labs
- CBC
- BMP
- Coagulation
- Type and screen
- HbA1c (diabetes — fusion risk)
- Vitamin D, calcium (osteoporosis)
- Nicotine/cotinine (smoking cessation)
- Albumin/prealbumin (nutritional status if concern)
Neurological Examination
Motor (myotomal)
- C5: Deltoid, biceps (___/5)
- C6: Wrist extensors, biceps (___/5)
- C7: Triceps, wrist flexors, finger extensors (___/5)
- C8: Finger flexors, interossei (___/5)
- T1: Intrinsic hand muscles (___/5)
- Lower extremities: Iliopsoas, quads, TA, EHL, gastroc
Sensory (dermatomal)
- C5: Lateral arm (regimental badge)
- C6: Lateral forearm, thumb, index
- C7: Middle finger
- C8: Ring and small finger, medial forearm
- T1: Medial arm
Reflexes
- Biceps (C5-6):
- Brachioradialis (C5-6):
- Triceps (C7):
- Patellar (L3-4):
- Achilles (S1):
- Hoffmann sign (myelopathy):
- Babinski (myelopathy):
- Clonus (myelopathy):
- Inverted brachioradialis reflex (C5-6 myelopathy):
Myelopathy Signs
- Hoffmann:
- Hyperreflexia:
- Clonus:
- Gait: Wide-based, spastic
- Grip and release test (< 20 in 10 sec = abnormal):
- Lhermitte sign:
- Romberg:
Baseline Swallowing Assessment
- Any pre-existing dysphagia (document — ACDF can worsen)
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: standard supine radiolucent OR table, often reversed for C-arm access; tape shoulders caudally for lower-cervical lateral fluoroscopy.
- OR setup: radiolucent/Jackson table, fluoroscopy or O-arm/navigation, microscope/loupes for decompression, implant trays/graft ready for fusion, neuromonitoring for myelopathy/cord-risk cases, and postop brace plan confirmed.
- Special needs: arterial line/Foley/type-screen for long fusion/corpectomy, no long paralytic when MEPs are used, MAP/normotension for myelopathy or cord-risk cases, antibiotic redosing, and anticoagulation/DVT plan.
- Immediate postop orders: neuro checks by myotome/sensory level, airway/dysphagia watch for anterior cervical cases, CT/X-rays per construct, drain care, brace/activity orders, DVT prophylaxis timing, bowel regimen, and PT/OT mobilization.
Diagnosis & Indication
- Working diagnosis: [Cervical radiculopathy / cervical spondylotic myelopathy] at [C_-C_]
- Surgical indication:
- Radiculopathy: Failed 6-12 weeks conservative treatment, progressive weakness, intolerable pain
- Myelopathy: Any myelopathy with imaging correlation (surgery prevents progression; delay worsens outcomes)
- Goals: Decompression of neural elements, restoration/maintenance of lordosis, solid fusion
Level Selection
- Correlate symptoms + exam + imaging — only fuse levels that are clinically relevant
- Number of levels: Single / 2-level / 3-level (> 3 levels: consider posterior approach or hybrid)
- Adjacent segment consideration: Avoid unnecessary levels to preserve remaining motion
Position
- OR table/bed: standard supine radiolucent OR table, often reversed for C-arm access; tape shoulders caudally for lower-cervical lateral fluoroscopy.
- Patient position: Supine
- Head position: Slight extension (improves lordosis and surgical angle). Neutral rotation. NO excessive extension (can worsen myelopathy intraoperatively)
- Head fixation: Horseshoe headrest (routine) or Mayfield (if navigation or significant instability)
- Neck: Mild extension — place a small roll between scapulae
- Arms: Tucked at sides, taped to bed. Shoulders pulled caudally with tape for fluoroscopic visualization of lower cervical levels
- Table: Reverse Trendelenburg (reduce venous engorgement)
- Gardner-Wells tongs: Consider for reducible deformity
Approach: Anterior Cervical (Smith-Robinson)
Side of approach:
- Left-sided approach preferred — recurrent laryngeal nerve (RLN) has a consistent course in the tracheoesophageal groove on the left; on the right, the RLN is non-recurrent in ~1% and takes a variable course
- Right-sided approach: If prior left-sided surgery, left-sided pathology requiring direct visualization, or surgeon preference
- If prior anterior approach: Obtain ENT evaluation with vocal cord assessment preoperatively
Key Surgical Steps
- Fluoroscopic level confirmation — mark the incision centered over the target disc space
- Transverse skin incision — in a skin crease at the appropriate level
- C3-4: Hyoid bone
- C4-5: Superior thyroid cartilage
- C5-6: Cricoid cartilage
- C6-7: 1-2 fingerbreadths above clavicle
- Platysma division — along skin incision or vertically
- Deep dissection: Develop interval between:
- Medial: Trachea, esophagus, recurrent laryngeal nerve
- Lateral: Carotid sheath (carotid artery, internal jugular vein, vagus nerve)
- Retract medial structures MEDIALLY, carotid sheath LATERALLY
- Identify prevertebral fascia and anterior longitudinal ligament
- Confirm level with fluoroscopy — place needle/marker in disc space
- Longus colli muscle dissection — release medially bilaterally from vertebral bodies; place retractor blades under longus colli (NOT on muscle surface — protects esophagus and RLN)
- Place self-retaining retractor (Caspar/Trimline distraction pins or table-mounted retractor)
- Discectomy:
- Incise anterior annulus with #15 blade
- Remove disc material with pituitary rongeurs and curettes
- Identify and remove posterior annulus
- Remove cartilaginous endplates (BUT preserve bony endplates for cage support)
- Uncovertebral joints: Identify bilaterally — marks lateral extent of decompression
- Posterior decompression:
- Remove posterior longitudinal ligament (PLL) to ensure complete decompression
- Use Kerrison rongeurs and curettes
- Decompress bilaterally to the uncovertebral joints
- Foraminotomy: If foraminal stenosis, decompress foramina with Kerrison or high-speed drill
- Confirm thecal sac and nerve root decompression
- Endplate preparation:
- Remove cartilaginous endplate with curettes (preserve bony endplate)
- Create flat, parallel surfaces for cage
- Slight concavity is acceptable
- Cage/graft selection and placement:
- Size: Trial cage for appropriate height (restore disc height and lordosis)
- Material: PEEK, titanium, allograft, or ACDF-specific interbody
- Graft: Fill cage with local bone, allograft chips, or bone substitute (BMP controversial in cervical)
- Place cage under fluoroscopic guidance — posterior edge 2-3 mm from posterior vertebral body line
- Confirm alignment and position
- Plate fixation:
- Anterior cervical plate spanning fused segments
- Screws: Bicortical preferred (but unicortical with locking plate acceptable)
- Ensure screws do not violate adjacent disc spaces (accelerates ASD)
- Confirm hardware position with fluoroscopy — lateral and AP
- Closure:
- Irrigate
- Hemostasis (bipolar, Surgicel, bone wax)
- Consider drain (if concern for hematoma — especially multi-level, coagulopathy)
- Close platysma with 3-0 Vicryl
- Skin: Subcuticular 4-0 Monocryl or Dermabond
Critical Anatomy & Structures at Risk
- Recurrent laryngeal nerve — runs in tracheoesophageal groove; retract GENTLY medially. Injury → hoarseness (unilateral) or airway compromise (bilateral)
- Esophagus — directly anterior to cervical spine; retract medially. Injury → mediastinitis (devastating)
- Vertebral arteries — in transverse foramina bilaterally; lateral limits of decompression are the uncovertebral joints
- Carotid artery / internal jugular vein — in carotid sheath laterally; retract gently
- Superior laryngeal nerve — at risk with high cervical approach (C3-4, above hyoid)
- Spinal cord — directly posterior; careful with instruments at posterior vertebral body
- Nerve roots — in foramina bilaterally
- Sympathetic chain — on longus colli; injury → Horner syndrome
- Thoracic duct — at risk with LEFT-sided approach at C7-T1 (drains into left subclavian/IJV junction)
Equipment
- Operating microscope OR loupes + headlight
- C-arm fluoroscopy
- Caspar distraction pins and retractor system
- High-speed drill (for osteophyte removal and foraminotomy)
- Kerrison rongeurs (1mm, 2mm)
- Pituitary rongeurs, curettes, nerve hooks
- Interbody cage(s) and trials
- Anterior cervical plate and screws
- Bone graft material (allograft, local bone, substitute)
- Hemostatic agents (Surgicel, Gelfoam, bone wax)
- Drain (if planned)
Monitoring
- SSEPs (baseline before and after positioning — flexion/extension can worsen myelopathy)
- MEPs
- EMG (triggered — for nerve root monitoring during decompression)
- CRITICAL: Check signals AFTER positioning and BEFORE incision — positioning can cause cord compression
Anesthesia Considerations
- Arterial line (multi-level or myelopathy)
- Foley (if long case)
- Cefazolin 2g IV
- Dexamethasone 10 mg IV (if myelopathy or significant compression)
- Keep MAP > 85 (spinal cord perfusion)
- No paralytic after intubation (MEP monitoring)
- Fiberoptic intubation (if severe myelopathy or limited neck mobility — avoid hyperextension)
- Keep shoulder tape accessible for removal if needed for fluoroscopy
Potential Complications & Contingencies
- Dysphagia — most common complication (up to 50% transient); usually resolves in days-weeks. Minimize retraction time, release periodically
- Recurrent laryngeal nerve palsy — hoarseness; usually transient. ENT evaluation if persistent > 6 weeks
- Esophageal injury — rare but devastating; irrigate wound, primary repair, drainage, broad-spectrum antibiotics
- Vertebral artery injury — rare; pack with hemostatic agents, may need angiography/embolization
- Hematoma with airway compromise — EMERGENT — if expanding neck hematoma, open wound at bedside to decompress, then return to OR
- Spinal cord injury — careful instrumentation, monitoring, maintain perfusion
- Hardware failure / subsidence — appropriate cage sizing, endplate preservation, smoking cessation
- Adjacent segment disease — long-term; correlates with number of fused levels
Operative Note Template
Preoperative Diagnosis: Cervical [radiculopathy/myelopathy] at [C_-C_] due to [disc herniation/spondylosis/OPLL]
Postoperative Diagnosis: Same
Procedure: Anterior cervical discectomy and fusion at [C_-C_] [and C_-C_] with interbody cage placement and anterior cervical plating
Surgeon: Assistant: Anesthesia: General endotracheal anesthesia ([fiberoptic intubation])
EBL: Fluids: Specimens: [Disc material / None] Drains: [None / JP drain] Complications: None Implants: [Cage type/size at each level], [Plate type/length, screw sizes]
Indications: The patient is a [age]yo [M/F] with [cervical radiculopathy/myelopathy] at [C_-C_] who failed [conservative management / has progressive myelopathy]. MRI demonstrated [findings]. After discussion of risks, benefits, and alternatives, the patient elected to proceed with ACDF.
Description of Procedure: [Standard: consent verified, site marked, anesthesia induced, monitoring established with stable baselines BEFORE AND AFTER positioning…]
The patient was positioned supine with the neck in slight extension over an interscapular roll. The head was placed on a horseshoe headrest. The arms were tucked at sides and shoulders taped caudally. Monitoring signals were confirmed stable after positioning.
The anterior neck was prepped and draped in sterile fashion. The surgical level was confirmed with lateral fluoroscopy using a spinal needle placed at the target disc space.
Incision: A transverse skin incision was made at the level of [landmark] on the [left/right] side. The platysma was divided [in line with the incision / vertically]. The deep cervical fascia was incised and the interval between the carotid sheath laterally and the tracheoesophageal structures medially was developed with blunt dissection. The prevertebral fascia was identified. The level was confirmed with fluoroscopy.
Exposure: The longus colli muscles were elevated bilaterally off the vertebral bodies with electrocautery. Self-retaining retractor blades were placed under the longus colli muscles. [Caspar distraction pins were placed in the adjacent vertebral bodies.]
Discectomy and decompression: [For each level:] The anterior annulus at [C_-C_] was incised with a #15 blade. The disc material was removed with pituitary rongeurs and curettes. The cartilaginous endplates were removed. Under the microscope [/ with loupes], the posterior annulus and posterior longitudinal ligament were removed with Kerrison rongeurs, decompressing the thecal sac. [Bilateral foraminotomies were performed with a ___ mm Kerrison rongeur / high-speed drill, decompressing the exiting nerve roots.] [An extruded disc fragment was identified [location] and removed.] Complete decompression was confirmed by visualization of the thecal sac and bilateral nerve roots with free passage of a nerve hook.
Fusion: The endplates were prepared with a curette to create a flat surface while preserving the bony endplates. A [type, size] interbody cage packed with [allograft bone / local bone / bone substitute] was placed under fluoroscopic guidance. Appropriate position was confirmed with the posterior edge seated 2-3 mm anterior to the posterior vertebral body line.
Plating: A [type, length] anterior cervical plate was applied spanning [C_ to C_]. [Number] screws were placed at each level. Final fluoroscopic images (lateral and AP) confirmed appropriate hardware position, alignment, and restoration of disc height and lordosis.
Closure: The wound was irrigated. Hemostasis was confirmed. [A drain was placed.] The platysma was closed with 3-0 Vicryl interrupted sutures. The skin was closed with 4-0 Monocryl subcuticular suture and Dermabond. A sterile dressing was applied.
Postoperative: The patient was awakened, extubated [without difficulty / over a tube exchanger], and found to be neurologically [intact / improved from baseline]. Monitoring signals remained stable throughout. The patient was transferred to the PACU in stable condition.
Postoperative Plan
- Airway monitoring: Monitor for neck swelling / hematoma q1h x 6h (hematoma can cause airway compromise)
- Floor admission (ICU if multi-level, myelopathy, or airway concern)
- Neuro checks q2h x 24h
- HOB 30 degrees
- NPO or clear liquids until swallowing assessed — soft diet then advance as tolerated
- Cervical collar: Soft collar for comfort (rigid collar if multi-level or instability)
- X-rays: AP/lateral cervical spine POD1 (or intraoperative finals sufficient)
- DVT prophylaxis: SCDs, consider heparin SQ
- Pain management: Acetaminophen, ice, muscle relaxant PRN, limit narcotics
- Dexamethasone taper if given
- CRITICAL: Educate nursing — if patient develops acute neck swelling, stridor, or difficulty breathing → CALL SURGEON IMMEDIATELY → may need bedside wound opening
- Smoking cessation counseling (critical for fusion)
- Activity: No heavy lifting > 10 lbs x 6 weeks; no contact sports
- Driving: No driving in cervical collar; typically resume at 2-4 weeks
- Follow-up: Clinic 2 weeks (wound check), 6 weeks (X-ray), 3 months (CT for fusion), 6 months, 1 year
- Dysphagia: Expect mild-moderate; typically resolves in 1-4 weeks. If persistent > 6 weeks → ENT evaluation, modified barium swallow
Chief-Level Case Review
Use these as the senior-level mental model for Anterior Cervical Discectomy and Fusion (ACDF):
- Decision point: Localize twice and instrument once: numbering, transitional anatomy, prior hardware, rib count, navigation dataset, and fluoroscopic level confirmation are mandatory.
- Technical lever: Positioning is treatment: table choice, abdomen-free prone setup, alignment goals, shoulders/hips, eyes/plexus pressure, neuromonitoring baselines, and fluoroscopic access all change the case.
- Bailout: Protect neural elements by sequence: decompression before correction when needed, MAP support for cord risk, no long paralytic with MEPs, and immediate response to signal change.
- Postop watch: Finish with construct logic: decompression adequacy, screw purchase, alignment, fusion bed/graft, drain plan, brace/activity orders, postop CT/X-rays, and DVT timing.
Common Pimp Questions
Use these to pressure-test preparation for Anterior Cervical Discectomy and Fusion (ACDF):
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]