
Case Prep: Chiari I Malformation Decompression
Case / Approach Snapshot
- Anatomy at risk: target nuclei or cortical regions, trajectories, vessels, ventricles, cranial nerves, white-matter tracts, and stimulation/lesion side-effect pathways.
- Operative steps: confirm diagnosis and target, plan trajectory or exposure, use mapping/monitoring/stereotaxy as appropriate, place/lesion/resect with physiologic confirmation, close hardware or wound, and plan programming/follow-up; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: hemorrhage, seizure, neurologic or mood/cognitive change, lead/device migration or infection, stimulation side effects, hardware failure, and revision or programming strategy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with Chiari I malformation ([___ mm tonsillar descent]) [with/without syrinx] presenting with [suboccipital headaches/numbness/weakness/dysphagia] planned for suboccipital craniectomy and C1 laminectomy [with/without duraplasty] for posterior fossa decompression.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Midline suboccipital craniotomy — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- The Chiari I malformation — McClugage SG. Journal of neurosurgery. Pediatrics 2019. PubMed
- Chiari I malformation in children-the natural history — Chatrath A. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2019. PubMed
- Chiari I malformation in patients with RASopathies — Han Y. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery 2021. PubMed
- Sociodemographics of Chiari I Malformation — Abbas Akbari SH. Neurosurgery clinics of North America 2023. PubMed
- Imaging in Chiari I Malformation — Pindrik J. Neurosurgery clinics of North America 2023. PubMed
- Epidemiology of Chiari I Malformation and Syringomyelia — Holste KG. Neurosurgery clinics of North America 2023. PubMed
- The Chiari-I malformation — Sclafani AP. Ear, nose, & throat journal 1991. PubMed
- Arachnoiditis and Chiari I malformation — Demetriades AK. Acta neurochirurgica 2021. PubMed
- Elucidating the Genetic Basis of Chiari I Malformation — Haller G. Neurosurgery clinics of North America 2023. PubMed
- Spine Deformity Associated with Chiari I Malformation and Syringomyelia — Das S. Neurosurgery clinics of North America 2023. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
 Figure 1. Frontal photograph of left House-Brackmann grade III facial palsy.Smile reveals left oral commissure deviation with blunted excursion and effaced nasolabial fold, consistent with… Source: Non-syndromic Developmental Facial Palsy Co-occurring With Chiari I Malformation: Parallel Manifestations of a Shared Prenatal Disturbance? — Cureus 2026; CC BY.
Figure 1. Frontal photograph of left House-Brackmann grade III facial palsy.Smile reveals left oral commissure deviation with blunted excursion and effaced nasolabial fold, consistent with… Source: Non-syndromic Developmental Facial Palsy Co-occurring With Chiari I Malformation: Parallel Manifestations of a Shared Prenatal Disturbance? — Cureus 2026; CC BY.
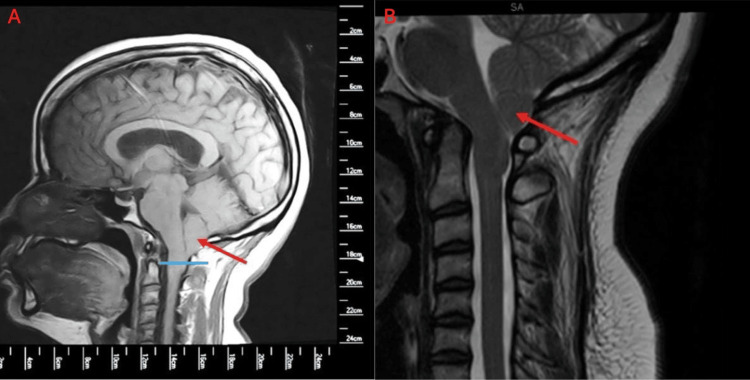 Figure 2. Pre-operative sagittal T1-weighted MRIA. 12-mm cerebellar tonsillar ectopia below McRae line (red arrow, blue line). B. Craniocervical junction crowding with obliterated cerebrospinal… Source: Non-syndromic Developmental Facial Palsy Co-occurring With Chiari I Malformation: Parallel Manifestations of a Shared Prenatal Disturbance? — Cureus 2026; CC BY.
Figure 2. Pre-operative sagittal T1-weighted MRIA. 12-mm cerebellar tonsillar ectopia below McRae line (red arrow, blue line). B. Craniocervical junction crowding with obliterated cerebrospinal… Source: Non-syndromic Developmental Facial Palsy Co-occurring With Chiari I Malformation: Parallel Manifestations of a Shared Prenatal Disturbance? — Cureus 2026; CC BY.
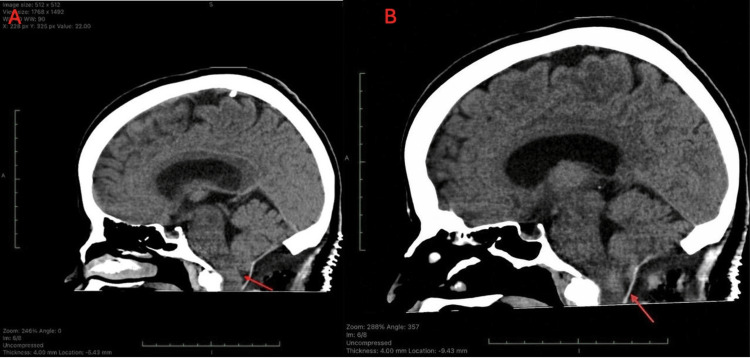 Figure 3. Post-operative sagittal head computed tomography (CT) following posterior fossa decompression and duraplasty.A. Demonstrates suboccipital craniectomy with bony decompression and expanded… Source: Non-syndromic Developmental Facial Palsy Co-occurring With Chiari I Malformation: Parallel Manifestations of a Shared Prenatal Disturbance? — Cureus 2026; CC BY.
Figure 3. Post-operative sagittal head computed tomography (CT) following posterior fossa decompression and duraplasty.A. Demonstrates suboccipital craniectomy with bony decompression and expanded… Source: Non-syndromic Developmental Facial Palsy Co-occurring With Chiari I Malformation: Parallel Manifestations of a Shared Prenatal Disturbance? — Cureus 2026; CC BY.
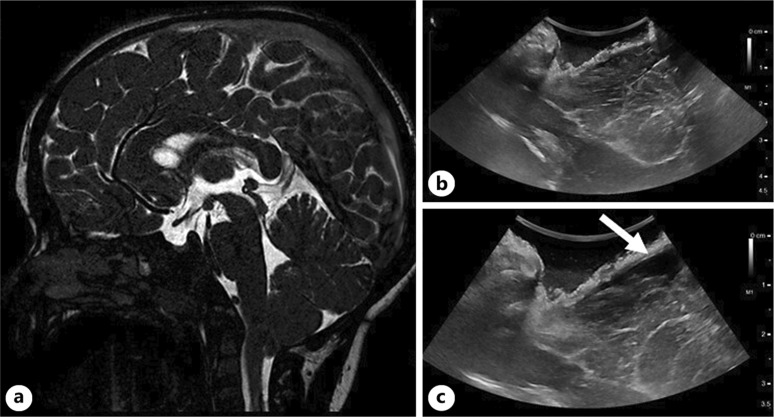 Fig. 2.. Sagittal MR showing CMI in a 3-year-old boy who complained of typical nuchal headache (a). IOUS after bony decompression (b) and after scoring of the posterior atlanto-occipital membrane… Source: Tailoring the Surgical Approach to Chiari I Malformation with Intraoperative Ultrasounds: Advantages, Limitations, and Controversies — Pediatric Neurosurgery 2025; CC BY-NC.
Fig. 2.. Sagittal MR showing CMI in a 3-year-old boy who complained of typical nuchal headache (a). IOUS after bony decompression (b) and after scoring of the posterior atlanto-occipital membrane… Source: Tailoring the Surgical Approach to Chiari I Malformation with Intraoperative Ultrasounds: Advantages, Limitations, and Controversies — Pediatric Neurosurgery 2025; CC BY-NC.
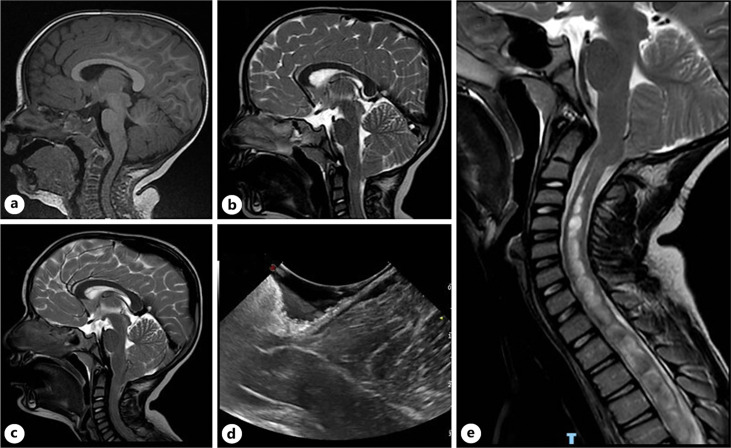 Fig. 3.. a MRI at 2 years of age showing normal findings. MRI at 5 years of age (b) showing asymptomatic tonsillar ectopia that evolved to symptomatic CMI at 9 years of age (c). Despite adequate… Source: Tailoring the Surgical Approach to Chiari I Malformation with Intraoperative Ultrasounds: Advantages, Limitations, and Controversies — Pediatric Neurosurgery 2025; CC BY-NC.
Fig. 3.. a MRI at 2 years of age showing normal findings. MRI at 5 years of age (b) showing asymptomatic tonsillar ectopia that evolved to symptomatic CMI at 9 years of age (c). Despite adequate… Source: Tailoring the Surgical Approach to Chiari I Malformation with Intraoperative Ultrasounds: Advantages, Limitations, and Controversies — Pediatric Neurosurgery 2025; CC BY-NC.
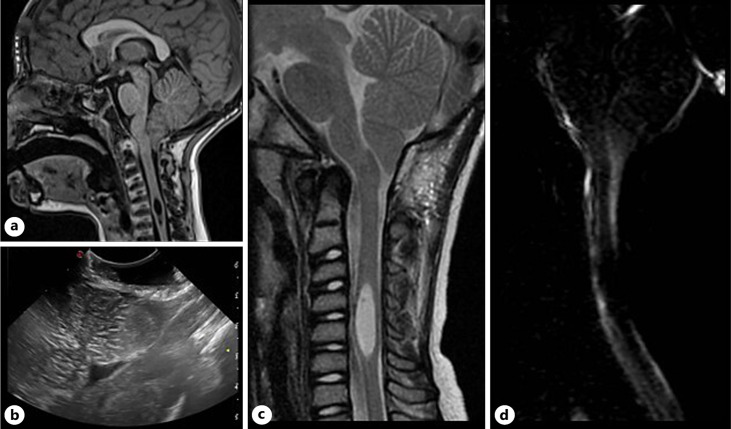 Fig. 4.. Sagittal MR showing CMI with cervical syringomyelia (a) in a 4-year-old boy who received bony decompression based on IOUS findings (b). Postoperative MR confirmed adequate decompression… Source: Tailoring the Surgical Approach to Chiari I Malformation with Intraoperative Ultrasounds: Advantages, Limitations, and Controversies — Pediatric Neurosurgery 2025; CC BY-NC.
Fig. 4.. Sagittal MR showing CMI with cervical syringomyelia (a) in a 4-year-old boy who received bony decompression based on IOUS findings (b). Postoperative MR confirmed adequate decompression… Source: Tailoring the Surgical Approach to Chiari I Malformation with Intraoperative Ultrasounds: Advantages, Limitations, and Controversies — Pediatric Neurosurgery 2025; CC BY-NC.
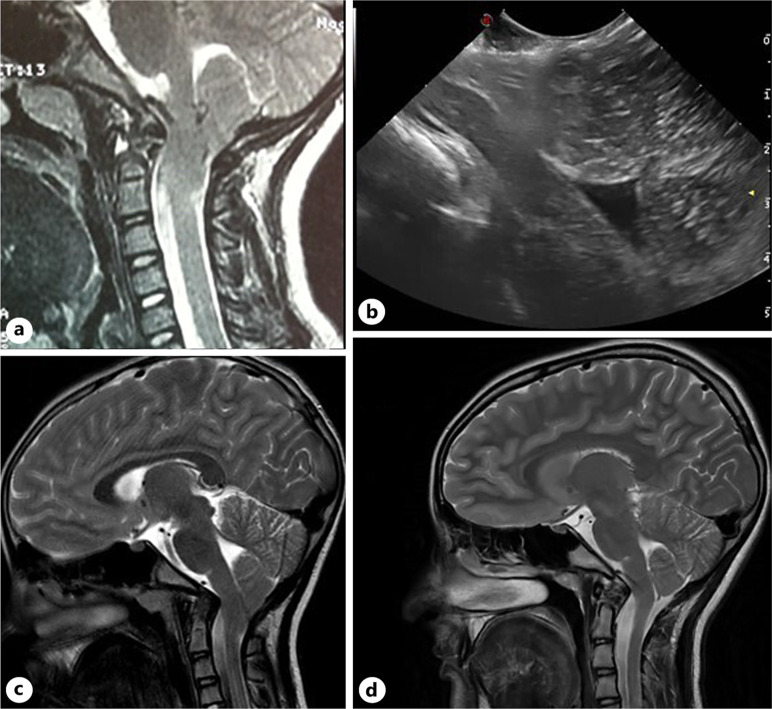 Fig. 5.. Sagittal MR showing symptomatic complex Chiari in an 8-year-old girl (a) who received bony decompression based on IOUS findings (b). c Radiological outcome on postoperative MR was… Source: Tailoring the Surgical Approach to Chiari I Malformation with Intraoperative Ultrasounds: Advantages, Limitations, and Controversies — Pediatric Neurosurgery 2025; CC BY-NC.
Fig. 5.. Sagittal MR showing symptomatic complex Chiari in an 8-year-old girl (a) who received bony decompression based on IOUS findings (b). c Radiological outcome on postoperative MR was… Source: Tailoring the Surgical Approach to Chiari I Malformation with Intraoperative Ultrasounds: Advantages, Limitations, and Controversies — Pediatric Neurosurgery 2025; CC BY-NC.
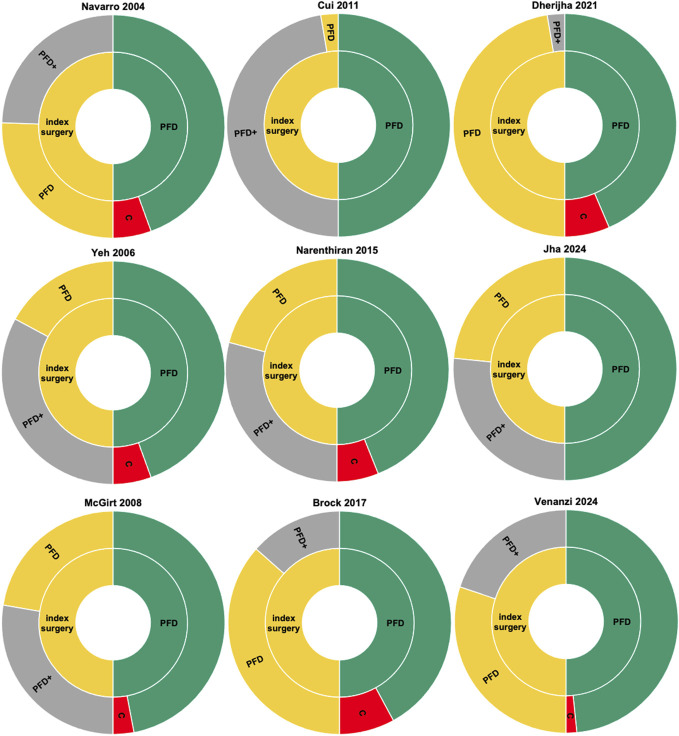 FIGURE 2.. Sunburst graph for each study. Left half shows the PFD (yellow) and PFD+ (gray) rates of index surgeries. Right half illustrates the proportion of successful PFD (green) and the… Source: Intraoperative Ultrasound in Chiari 1 Decompression: Clarity or Confusion? A Systematic Review — Neurosurgery 2026; CC BY.
FIGURE 2.. Sunburst graph for each study. Left half shows the PFD (yellow) and PFD+ (gray) rates of index surgeries. Right half illustrates the proportion of successful PFD (green) and the… Source: Intraoperative Ultrasound in Chiari 1 Decompression: Clarity or Confusion? A Systematic Review — Neurosurgery 2026; CC BY.
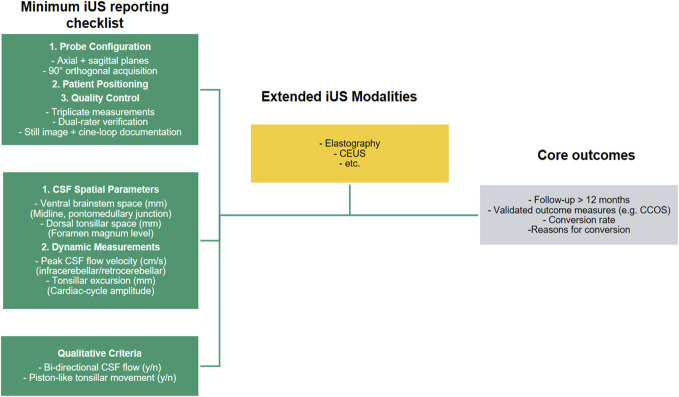 FIGURE 3.. Proposed reporting framework for iUS studies, highlighting a minimum reporting checklist (green), possible emerging techniques (yellow), and relevant outcome measures (grey). Specific… Source: Intraoperative Ultrasound in Chiari 1 Decompression: Clarity or Confusion? A Systematic Review — Neurosurgery 2026; CC BY.
FIGURE 3.. Proposed reporting framework for iUS studies, highlighting a minimum reporting checklist (green), possible emerging techniques (yellow), and relevant outcome measures (grey). Specific… Source: Intraoperative Ultrasound in Chiari 1 Decompression: Clarity or Confusion? A Systematic Review — Neurosurgery 2026; CC BY.
History of Present Illness
- Chief complaint: Occipital/suboccipital headaches (worse with Valsalva/cough/strain), numbness, weakness
- Duration and progression:
- Symptoms:
- Headaches: Suboccipital, exacerbated by Valsalva, cough, straining (classic)
- Numbness: Cape-like distribution (shoulders/arms) if syrinx
- Weakness: Hand weakness if syrinx (central cord pattern)
- Dysphagia: Brainstem compression
- Sleep apnea: Central type from brainstem compression
- Ataxia/balance difficulty
- Nystagmus (downbeat nystagmus classic)
- Syrinx symptoms: Dissociated sensory loss (loss of pain/temp, preserved light touch), hand weakness/atrophy, scoliosis (in children)
Past Medical History
- Connective tissue disorders (Ehlers-Danlos — associated with Chiari, craniocervical instability)
- Craniocervical instability (must rule out BEFORE decompression alone)
- Scoliosis (may be syrinx-related in children)
- Sleep apnea (central type)
- Tethered cord (associated in some patients)
- Allergies:
- Medications:
Imaging Review
MRI Brain/Cervical Spine
- Tonsillar descent: ___ mm below foramen magnum (McRae line)
- ≥ 5 mm = Chiari I malformation
- 3-5 mm = borderline (correlate with symptoms)
- Tonsillar morphology: Peg-shaped (pathologic) vs round (normal variant)
- Crowding at foramen magnum: CSF space obliteration around tonsils and brainstem
- Syringomyelia: Present/absent; location, extent, size
- Brainstem compression: Ventral compression, medullary kinking
- Fourth ventricle: Position, patency
- Hydrocephalus: Present/absent (must rule out as cause of tonsillar herniation)
- Other Chiari features: Basilar invagination, retroflexed odontoid, small posterior fossa
- CSF flow study (cine MRI): Absent or reduced CSF flow at foramen magnum (supports surgical indication)
CT Cervical Spine/Craniocervical Junction
- Bony anatomy of craniocervical junction
- Rule out:
- Basilar invagination (odontoid tip above Chamberlain line)
- Atlantoaxial instability
- Os odontoideum
- Occipitalization of atlas
- If bony abnormality: May need OCF (occipitocervical fusion) rather than simple decompression
Flexion/Extension X-rays
- Rule out craniocervical instability — especially if EDS or prior decompression failed
- ADI (atlantodental interval) > 3 mm = instability
Labs
- CBC, BMP, Coags
- Type and screen
- If EDS suspected: Genetics referral
Neurological Examination
Motor
- Hand intrinsics (syrinx — central cord pattern)
- Upper and lower extremity strength
- Spasticity/hyperreflexia (if myelopathy from syrinx)
Sensory
- Cape-like dissociated sensory loss (pain/temp lost, light touch preserved — syrinx)
- Posterior column function (vibration, proprioception)
Cranial Nerves
- Nystagmus: Downbeat (classic Chiari)
- Dysphagia: CN IX, X
- Tongue: CN XII (if brainstem compression)
- Lower cranial nerves: Palate, voice, shoulder shrug
Cerebellar
- Gait, tandem walk, coordination, Romberg
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: Mayfield, microscope, cranial nerve monitoring/BAER for MVD, Teflon/felt and microinstruments, dural graft/sealant for Chiari, and watertight closure materials.
- Special needs: arterial line optional by comorbidity/position, antiemetic plan, steroid plan by edema/aseptic meningitis risk, airway/OSA precautions, and CSF-leak/pseudomeningocele strategy.
- Immediate postop orders: posterior fossa neuro checks, facial/hearing/swallow exam as relevant, nausea/pain control, HOB 30, CT/MRI if concern or protocol, wound/CSF leak watch, and activity restrictions.
Diagnosis & Indication
- Working diagnosis: Symptomatic Chiari I malformation [with/without syrinx]
- Surgical indication: Symptomatic Chiari with imaging evidence of crowding at foramen magnum and/or reduced CSF flow on cine MRI; progressive syrinx
- Goals: Restore CSF flow at the foramen magnum; decompress the posterior fossa; syrinx should stabilize or improve over months
- NOT indicated for: Incidental Chiari without symptoms; headaches that do not fit Chiari pattern
Surgical Options
- Bone-only decompression: Suboccipital craniectomy + C1 laminectomy + scoring/release of outer dural layer — simpler, lower CSF leak risk, may be sufficient
- Decompression with duraplasty: Full dural opening with expansile duraplasty — more definitive CSF flow restoration, higher risk of CSF leak
- With tonsillar reduction: Shrinkage/coagulation of tonsil tips — rarely needed
- Occipitocervical fusion: If instability present — different procedure entirely
Position
- Patient position: Prone (most common) or Concorde (sitting-like but prone, head elevated)
- Head: Flexed (chin toward chest) to open the foramen magnum; Mayfield skull clamp
- Table: Slight reverse Trendelenburg
- Arms: Tucked at sides
- Key: Avoid excessive flexion (can worsen brainstem compression before decompression)
- Tape shoulders caudally (improve visualization)
Incision
- Midline posterior incision from just below the inion to the C2 spinous process
- Length: ~6-8 cm
Key Surgical Steps
- Midline incision from below inion to C2 spinous process
- Subperiosteal dissection of suboccipital muscles from occiput and C1 posterior arch
- Stay strictly midline to minimize bleeding (avascular midline raphe)
- Identify and preserve the C2 nerve root and vertebral arteries (V3 segment runs on superior surface of C1 arch)
- Suboccipital craniectomy:
- Remove bone from foramen magnum upward (2.5-3 cm x 3 cm)
- Center on midline, extend laterally to the edges of the foramen magnum
- Use Kerrison rongeurs or drill
- C1 laminectomy:
- Remove the posterior arch of C1
- Vertebral arteries run on the SUPERIOR surface of C1 arch — stay ON the posterior arch, within 1.5 cm of midline
- DO NOT extend laterally beyond 1.5 cm from midline (VA at risk)
- Assess dura:
- If bone-only decompression: Score/release the outer dural layer and stop
- If duraplasty planned: Continue
- Dural opening (if duraplasty):
- Y-shaped or cruciate dural incision
- Carefully open — tonsils may be adherent to dura
- Open arachnoid membranes at foramen magnum
- Release arachnoid adhesions between tonsils and brainstem
- Inspect foramen magnum:
- Confirm CSF flow around the tonsils
- Release any obstructing arachnoid bands
- Tonsillar reduction: Subpial coagulation of tonsillar tips (if tonsils still block foramen — rarely needed)
- Confirm obex is visible (fourth ventricle outlet)
- Duraplasty:
- Sew in a dural graft to expand the posterior fossa dural space
- Graft options: Autologous pericranium, bovine pericardium, DuraGen, Gore-Tex
- Watertight closure is CRITICAL (CSF leak is the most common complication)
- Running or interrupted 4-0 or 5-0 braided suture
- Dural sealant: Apply (DuraSeal, fibrin glue) over the suture line
- Closure:
- Muscle closure in layers (watertight muscle closure helps prevent CSF leak)
- Fascial closure
- Subcutaneous
- Skin
Critical Anatomy & Structures at Risk
- Vertebral arteries (V3 segment) — run on the SUPERIOR surface of C1 posterior arch, within the sulcus arteriosus; injury during C1 laminectomy is catastrophic; stay within 1.5 cm of midline
- Cerebellar tonsils — compressed against foramen magnum; handle gently
- PICA (posterior inferior cerebellar artery) — loops around the tonsils; identify and preserve during dural opening
- Brainstem (medulla) — directly deep to the tonsils
- C2 nerve root / ganglion — may need to be retracted for C1 arch exposure
- Cervical spinal cord — deep to C1 arch during laminectomy
- Fourth ventricle / obex — visible after tonsillar separation; avoid manipulation
Equipment
- Operating microscope or loupes + headlight
- High-speed drill (for craniectomy)
- Kerrison rongeurs
- Ultrasound (intraoperative — can confirm tonsillar position and CSF flow before and after decompression)
- Dural graft material (pericranium, bovine pericardium, DuraGen)
- Dural sealant (DuraSeal, fibrin glue)
- Microsurgical instruments (for arachnoid dissection)
- Bipolar (for tonsillar reduction if needed)
Monitoring
- SSEPs
- MEPs
- Standard ASA monitors
Anesthesia
- General endotracheal anesthesia
- Arterial line (optional for straightforward cases)
- Foley
- Cefazolin 2g IV
- Dexamethasone 10 mg IV
- No paralytic (if MEP monitoring)
- Caution with positioning: Avoid excessive neck flexion — can worsen brainstem compression before decompression
Potential Complications
- CSF leak / pseudomeningocele — most common complication; meticulous dural closure + sealant; if post-op leak → wound revision or lumbar drain
- Infection / meningitis — aseptic meningitis (from blood in CSF) vs bacterial
- Vertebral artery injury — during C1 laminectomy; stay near midline (< 1.5 cm lateral)
- Cerebellar/brainstem injury — gentle handling of tonsils, careful dural opening
- Recurrence of symptoms — inadequate decompression, scarring, or craniocervical instability unmasked
- Worsened symptoms — rare; from manipulation of brainstem/tonsils or destabilizing craniocervical junction
- Craniocervical instability — excessive bone removal can destabilize; do not remove C2 arch or occipital condyles
Postoperative Plan
- Floor or step-down (ICU if significant brainstem compression pre-op)
- Neuro checks q2h x 24h
- HOB 30 degrees (unless duraplasty CSF leak concern → may need flat bed rest initially)
- CT head/neck within 24 hours (confirm adequate decompression, rule out hematoma)
- MRI at 3-6 months: Assess tonsillar position, CSF flow restoration, syrinx resolution/improvement
- Pain management: Posterior cervical/occipital muscle pain is significant; acetaminophen, NSAIDs, muscle relaxants, limited opioids
- Diet: Start clear liquids, advance as tolerated (monitor swallowing if pre-op dysphagia)
- Cervical collar: Soft collar for comfort x 2-4 weeks (optional)
- Activity: No heavy lifting x 6 weeks
- DVT prophylaxis: SCDs, heparin SQ POD1
- Wound monitoring: CSF leak (clear fluid from incision, positional headache, pseudomeningocele)
- Follow-up: 2-4 weeks clinic; MRI at 3-6 months and 1 year
- Syrinx: Expect gradual improvement over 6-12 months; stable syrinx may not resolve but shouldn’t progress
- If symptoms recur or not improved: Reassess for instability, inadequate decompression, tethered cord
Chief-Level Case Review
Use these as the senior-level mental model for Chiari I Malformation Decompression:
- Decision point: Define the symptom physiology: target circuit or offending vessel/nerve must match the history, exam, imaging, and intraoperative monitoring plan.
- Technical lever: Small errors matter: trajectory, lead/contact position, arachnoid dissection, cranial-nerve handling, or mapping threshold can be the difference between success and morbidity.
- Bailout: Have a stop rule: unacceptable mapping response, BAER/MEP/SSEP change, hemorrhage, CSF loss, poor target confidence, or patient intolerance should trigger a defined pivot.
- Postop watch: Postop success requires programming/follow-up details: neurologic exam, imaging, medication adjustment, device restrictions, wound care, and symptom-specific outcome tracking.
Common Pimp Questions
Use these to pressure-test preparation for Chiari I Malformation Decompression:
- What is the symptom target and what finding proves the correct neural structure is being treated?
- What imaging, tractography, MER, stimulation, or mapping information changes the trajectory?
- What medication adjustments or anesthesia constraints matter on the day of surgery?
- What complication would be subtle but important to detect in recovery?
- What postop programming, imaging, seizure, swallow, or cranial-nerve plan is needed?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Awake/asleep technique, MER/stimulation thresholds, and imaging confirmation: [attending-specific]
- Medication hold/restart protocol and programming timeline: [attending-specific]
- Hardware brand, tunneling side, battery pocket, and antibiotic envelope preference: [attending-specific]
- Postop CT/MRI timing and symptom-specific neuro checks: [attending-specific]