
Case Prep: Glioma Resection (Supratentorial)
Case / Approach Snapshot
- Anatomy at risk: tumor compartment, arterial supply, venous drainage/sinuses, cranial nerves, white-matter tracts, pituitary/CSF pathways when relevant, and functional cortex.
- Operative steps: review imaging and goals, choose exposure, obtain brain relaxation, devascularize when possible, debulk internally, dissect capsule from critical structures, verify extent/safety, and reconstruct watertight closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: venous or arterial injury, swelling, seizure, cranial nerve or endocrine change, CSF leak, residual tumor left for safety, staged surgery, radiation, or adjuvant therapy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [size] cm [left/right] [frontal/temporal/parietal/insular] [WHO grade II/III/IV] glioma presenting with [seizures/focal deficit/headaches/cognitive changes] planned for [awake/asleep] craniotomy for maximal safe resection.
Figures, Imaging & Video
🎥 Operative videos & resources
- Atlas / approach: Pterional craniotomy chapter for frontal/temporal/insular corridors; use approach-specific pages for midline, posterior fossa, or awake mapping cases
- Video searches: glioma resection awake mapping on YouTube · 5-ALA glioma resection
- Open-access figures: PubMed Central — glioma resection awake mapping · Radiopaedia — high-grade glioma
🧭 Operative approach: Pterional craniotomy — detailed corridor setup, step-by-step technique & figures
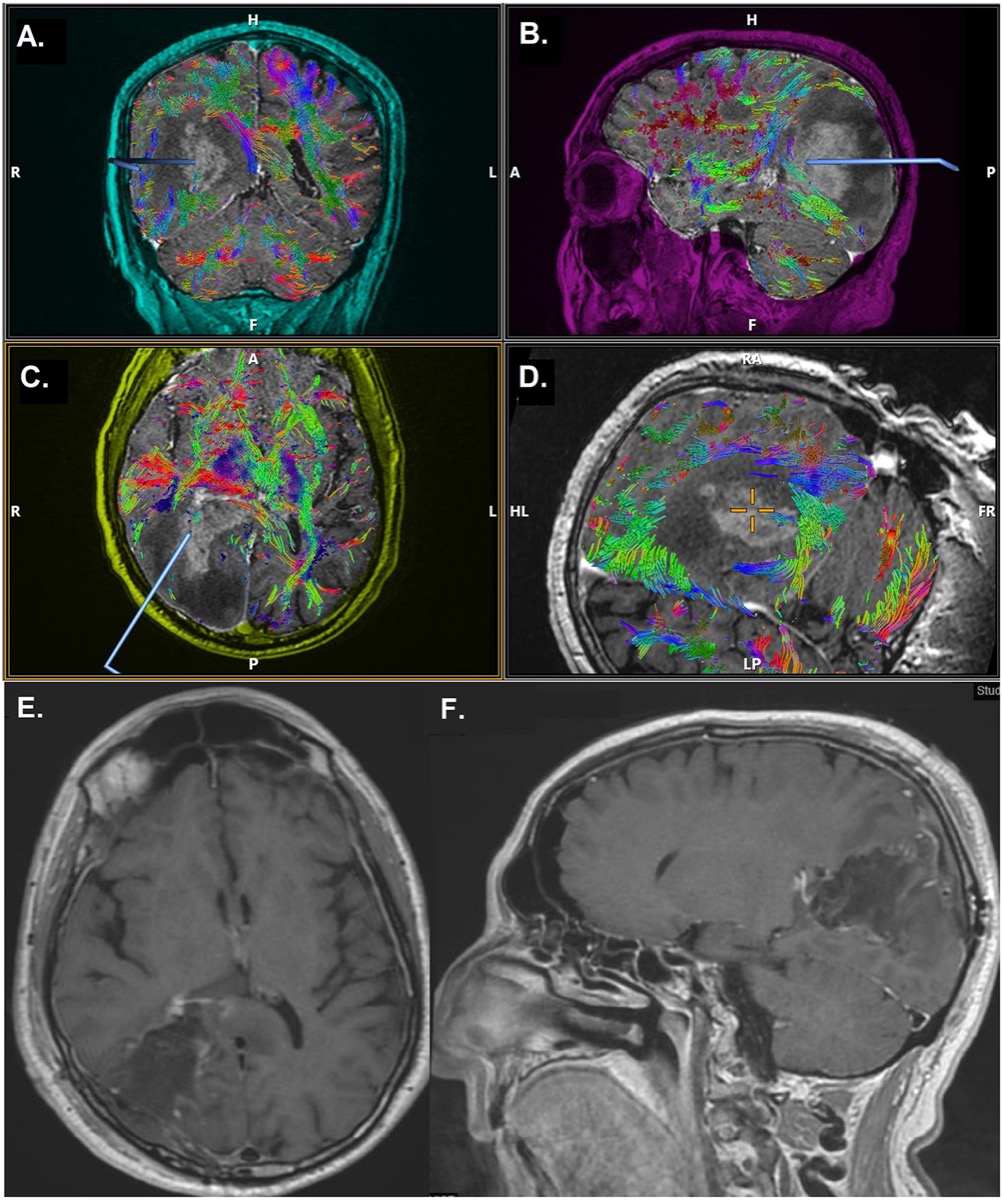
Preoperative MRI + DTI and postoperative gross-total-resection MRI. Source: Maragkos et al., Front Neurol 2021;12:644804, Fig 1. CC BY 4.0.
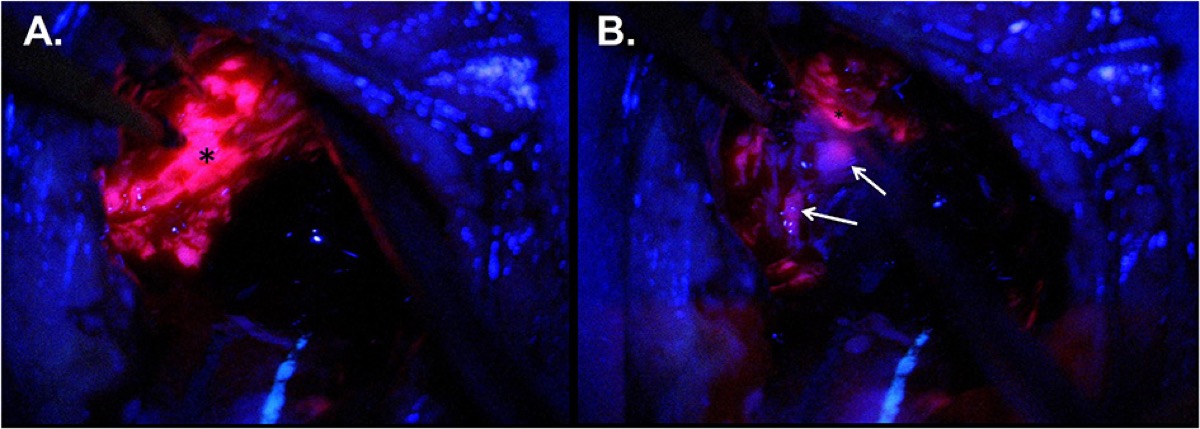
Intraoperative 5-ALA fluorescence guiding resection of tumor bulk and infiltrative margin. Source: Maragkos et al., Front Neurol 2021;12:644804, Fig 2. CC BY 4.0.
High-Yield Literature
- [Pediatric Hemispheric Glioma] — Nakano Y. No shinkei geka. Neurological surgery 2022. PubMed
- H3 K27M-altered glioma and diffuse intrinsic pontine glioma: Semi-systematic review of treatment landscape and future directions — van den Bent M. Neuro-oncology 2024. PubMed
- Glioma stem cells: drivers of tumor progression and recurrence — He J. Stem cell research & therapy 2025. PubMed
- Glioma and Neurokinin-1 Receptor Antagonists: A New Therapeutic Approach — Muñoz M. Anti-cancer agents in medicinal chemistry 2019. PubMed
- Pediatric-Type Diffuse Low Grade Glioma — Kotch C. Advances in cancer research 2025. PubMed
- A map of the altered glioma metabolism — Deshmukh R. Trends in molecular medicine 2021. PubMed
- Updates in Pediatric Glioma Pathology — Hakar MH. Surgical pathology clinics 2020. PubMed
- Neuroscience in glioma biology (Review) — Zhang C. Oncology reports 2025. PubMed
- Recent advances in glioma microenvironment-response nanoplatforms for phototherapy and sonotherapy — Li X. Pharmacological research 2022. PubMed
- What Epigenetics Teaches Us About Neuron-Glioma Interactions — Chakraborty C. BioEssays : news and reviews in molecular, cellular and developmental biology 2025. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
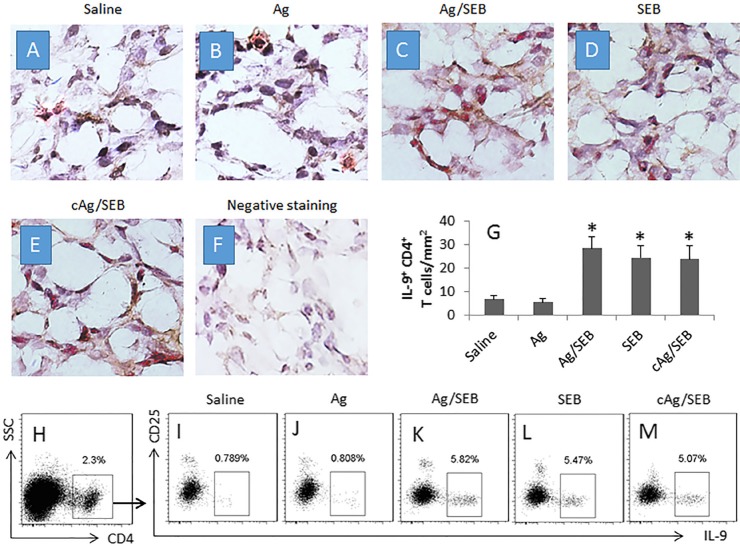 Figure 2. Counts of IL-9+ CD4+ T cells in glioma tissue(A–F) the photomicrographs show the IL-9+ (in red) CD4+ (in brown) T cells in glioma tissue from glioma-bearing mice. Panel F is negative… Source: Induction of specific T helper-9 cells to inhibit glioma cell growth — Oncotarget 2017; CC BY.
Figure 2. Counts of IL-9+ CD4+ T cells in glioma tissue(A–F) the photomicrographs show the IL-9+ (in red) CD4+ (in brown) T cells in glioma tissue from glioma-bearing mice. Panel F is negative… Source: Induction of specific T helper-9 cells to inhibit glioma cell growth — Oncotarget 2017; CC BY.
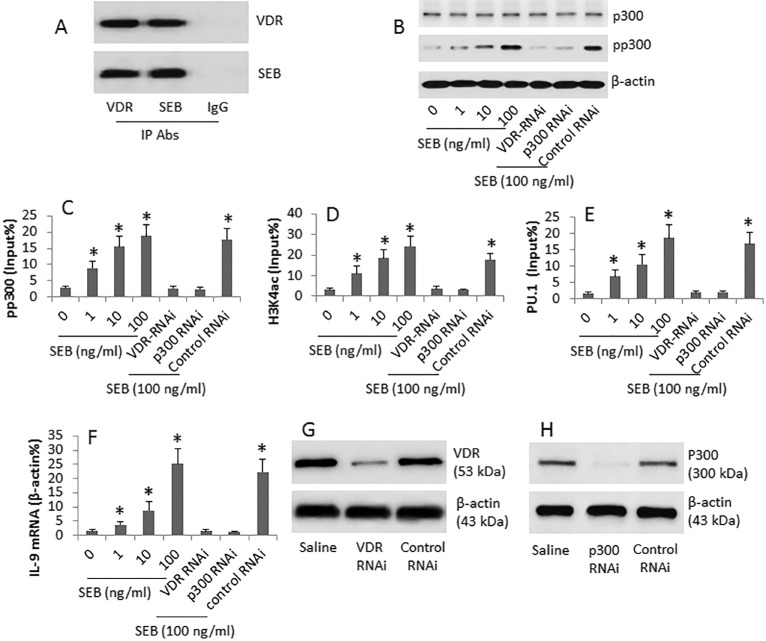 Figure 3. SEB regulates IL-9 gene expression in CD4+ T cellsCD4+ CD25− T cells were cultured SEB (at gradient doses as denoted) for 6 days. Cytosolic and nuclear extracts were prepared from the… Source: Induction of specific T helper-9 cells to inhibit glioma cell growth — Oncotarget 2017; CC BY.
Figure 3. SEB regulates IL-9 gene expression in CD4+ T cellsCD4+ CD25− T cells were cultured SEB (at gradient doses as denoted) for 6 days. Cytosolic and nuclear extracts were prepared from the… Source: Induction of specific T helper-9 cells to inhibit glioma cell growth — Oncotarget 2017; CC BY.
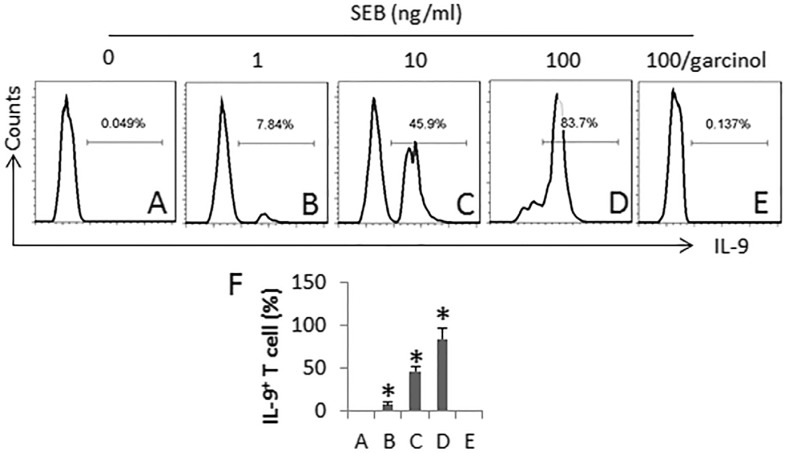 Figure 4. SEB induces Th9 cellsCD4+ CD25− T cells and DCs (T cell:DC = 5:1) were cultured in the presence of SEB (100 ng/ml) and IL-2 (10 ng/ml; used as a T cell activator) for 6 days. The medium… Source: Induction of specific T helper-9 cells to inhibit glioma cell growth — Oncotarget 2017; CC BY.
Figure 4. SEB induces Th9 cellsCD4+ CD25− T cells and DCs (T cell:DC = 5:1) were cultured in the presence of SEB (100 ng/ml) and IL-2 (10 ng/ml; used as a T cell activator) for 6 days. The medium… Source: Induction of specific T helper-9 cells to inhibit glioma cell growth — Oncotarget 2017; CC BY.
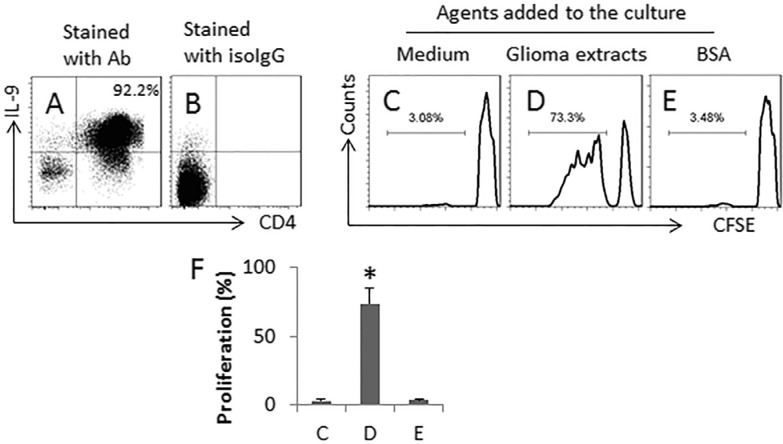 Figure 5. SEB and glioma cell extracts induce glioma-specific Th9 cellsTh9 cells were generated from naïve CD4+ CD25− T cells with the presence of glioma extracts (5 μg/ml) and DCs in the presence… Source: Induction of specific T helper-9 cells to inhibit glioma cell growth — Oncotarget 2017; CC BY.
Figure 5. SEB and glioma cell extracts induce glioma-specific Th9 cellsTh9 cells were generated from naïve CD4+ CD25− T cells with the presence of glioma extracts (5 μg/ml) and DCs in the presence… Source: Induction of specific T helper-9 cells to inhibit glioma cell growth — Oncotarget 2017; CC BY.
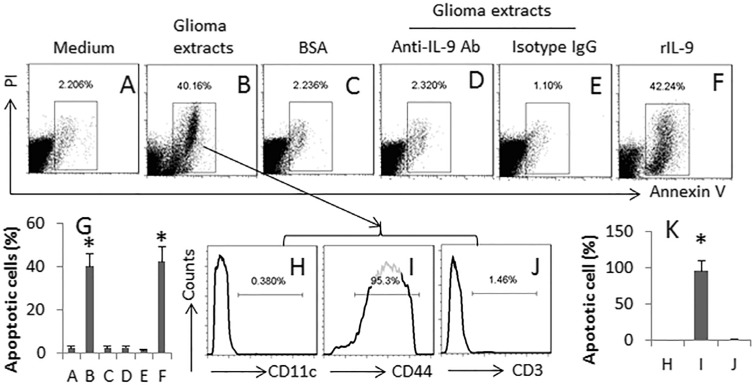 Figure 6. Glioma-specific Th9 cells induce glioma cell apoptosisTh9 cells were generated in the same procedures of Figure 4D. The cells (contain both Th9 cells and DCs; or #, naïve CD4+ T cells)… Source: Induction of specific T helper-9 cells to inhibit glioma cell growth — Oncotarget 2017; CC BY.
Figure 6. Glioma-specific Th9 cells induce glioma cell apoptosisTh9 cells were generated in the same procedures of Figure 4D. The cells (contain both Th9 cells and DCs; or #, naïve CD4+ T cells)… Source: Induction of specific T helper-9 cells to inhibit glioma cell growth — Oncotarget 2017; CC BY.
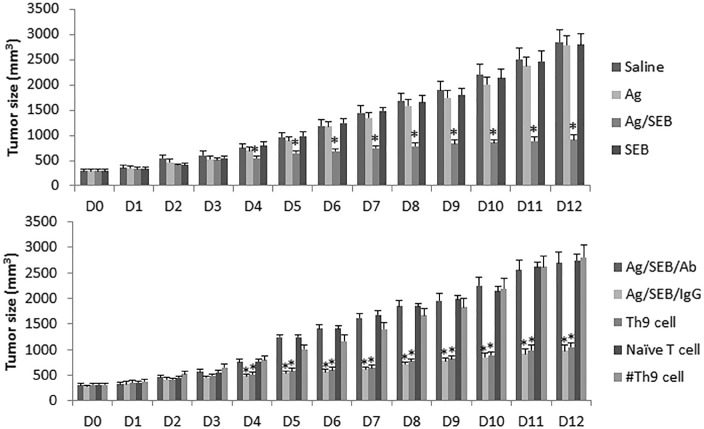 Figure 7. Administration with SEB enforces the effect of immunotherapy of Ag on experimental gliomaThe bars indicate the tumor size (mean ± SD) recorded from glioma-bearing mice. The treatment is… Source: Induction of specific T helper-9 cells to inhibit glioma cell growth — Oncotarget 2017; CC BY.
Figure 7. Administration with SEB enforces the effect of immunotherapy of Ag on experimental gliomaThe bars indicate the tumor size (mean ± SD) recorded from glioma-bearing mice. The treatment is… Source: Induction of specific T helper-9 cells to inhibit glioma cell growth — Oncotarget 2017; CC BY.
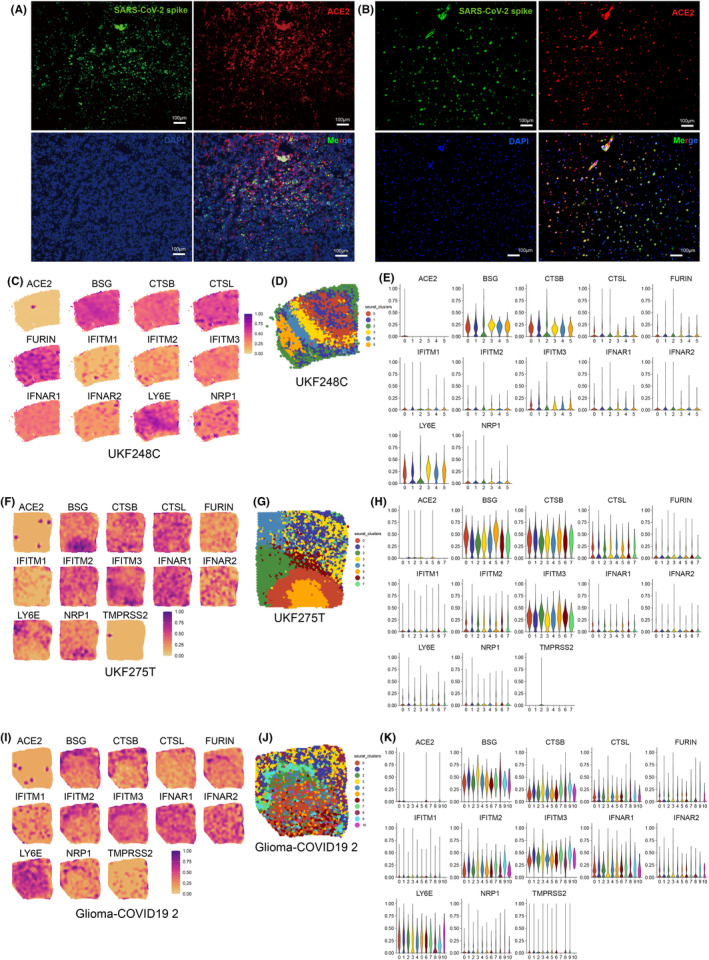 FIGURE 1. Glioma tissues are susceptible to SARS‐CoV‐2. (A) Immunofluorescent staining detecting the presence of the SARS‐CoV‐2 spike protein and ACE2 in glioblastoma tissue obtained from a… Source: Evidences of neurological injury caused by COVID‐19 from glioma tissues and glioma organoids — CNS Neuroscience & Therapeutics 2024; CC BY.
FIGURE 1. Glioma tissues are susceptible to SARS‐CoV‐2. (A) Immunofluorescent staining detecting the presence of the SARS‐CoV‐2 spike protein and ACE2 in glioblastoma tissue obtained from a… Source: Evidences of neurological injury caused by COVID‐19 from glioma tissues and glioma organoids — CNS Neuroscience & Therapeutics 2024; CC BY.
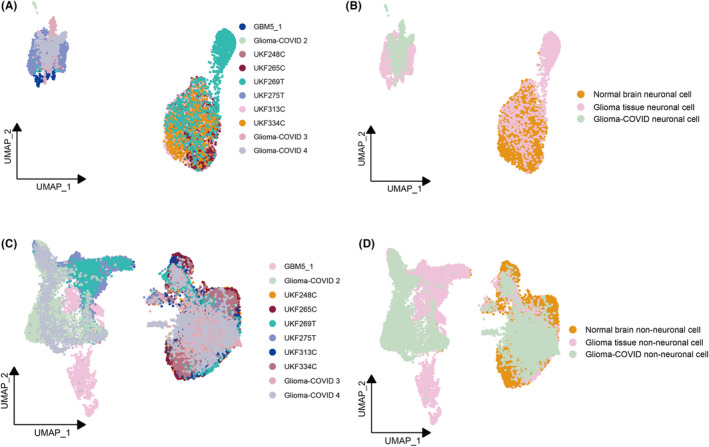 FIGURE 3. The global comparison of the differences of the neuronal cells or non‐neuronal cells in normal brain tissues, glioma tissues, and glioma‐COVID tissues. (A, B) UMAP representation of the… Source: Evidences of neurological injury caused by COVID‐19 from glioma tissues and glioma organoids — CNS Neuroscience & Therapeutics 2024; CC BY.
FIGURE 3. The global comparison of the differences of the neuronal cells or non‐neuronal cells in normal brain tissues, glioma tissues, and glioma‐COVID tissues. (A, B) UMAP representation of the… Source: Evidences of neurological injury caused by COVID‐19 from glioma tissues and glioma organoids — CNS Neuroscience & Therapeutics 2024; CC BY.
History of Present Illness
- Chief complaint: Seizures / progressive neurological deficit / headaches / cognitive changes / incidental
- Duration:
- Seizure type and frequency:
- Current AEDs and control:
- Functional status (KPS):
- Handedness (determines language dominance):
- Any prior biopsy or treatment:
Past Medical History
- Prior brain tumor / prior resection
- Prior radiation
- Prior chemotherapy (temozolomide)
- Seizure medications
- Steroid use (current dexamethasone dose)
- Li-Fraumeni, NF1, NF2, tuberous sclerosis (predisposition syndromes)
- Allergies:
- Medications:
Imaging Review
MRI Brain (T1, T1+Gad, T2, FLAIR, DWI, ADC, SWI, perfusion)
- Location: [Lobe] — relationship to eloquent cortex
- Size: __ x __ x ___ cm
- Enhancement: (Grade IV: ring-enhancing with central necrosis; Grade II/III: non-enhancing or patchy)
- FLAIR extent: Infiltrative margin (FLAIR abnormality > enhancement = infiltrative glioma)
- Necrosis / hemorrhage: SWI for blood products
- Edema / mass effect:
- Midline shift:
- Multifocal / crossing midline (butterfly glioma):
- Perfusion: Elevated rCBV correlates with higher grade
- Spectroscopy (MRS): Elevated choline, decreased NAA
- Differential:
- Grade IV (GBM): Ring enhancement, necrosis, restricted diffusion rim
- Grade III (Anaplastic astrocytoma/oligodendroglioma): Patchy enhancement
- Grade II (Low-grade glioma): Non-enhancing, T2/FLAIR bright, cortex-based
fMRI (Functional MRI)
- Motor mapping: Hand, foot, tongue activation relative to tumor
- Language mapping: Broca and Wernicke activation (if dominant hemisphere)
- Distance from tumor to activation: < 1 cm = high risk
DTI Tractography
- Corticospinal tract: Displaced / infiltrated / disrupted
- Arcuate fasciculus: (Language — dominant hemisphere)
- Inferior frontal-occipital fasciculus (IFOF): (Semantic processing)
- Superior longitudinal fasciculus (SLF):
- Optic radiations:
- Relationship to tumor: Displaced (resectable) vs infiltrated (partially resectable) vs disrupted (not recoverable)
Navigation
- Thin-cut MRI with gadolinium loaded
- FLAIR sequence loaded (for non-enhancing tumor margin)
- DTI tractography overlaid
- fMRI data integrated
Labs
- CBC
- BMP
- Coagulation
- Type and screen
- Dexamethasone level (if on steroids)
Neurological Examination
Mental Status
- KPS score:
- Language: Fluency, comprehension, repetition, naming, reading, writing
- Neglect (non-dominant parietal):
- Memory:
- Executive function:
Motor
- Full motor exam including fine motor:
- Drift:
Sensory
- Including cortical sensory modalities:
Visual Fields
- Formal perimetry if occipital/temporal/parietal tumor:
Baseline Documentation
- CRITICAL: Document every deficit carefully — this is the baseline against which postoperative function will be measured
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: Mayfield, navigation with latest MRI/DTI/functional data, microscope/exoscope, ultrasound/5-ALA/fluorescence when used, CUSA, cortical/subcortical mapping tools for eloquent lesions, and specimens/pathology workflow ready.
- Special needs: arterial line for large/eloquent/vascular tumors, dexamethasone plan, seizure prophylaxis for cortical lesions or seizure history, mannitol/hypertonic availability, language/motor mapping plan, and blood available for meningioma/skull-base cases.
- Immediate postop orders: neuro checks with deficit-specific exam, MRI brain with contrast within 24-48h when resection assessment matters, CT for hemorrhage concern, dex taper, antiepileptic duration, DVT timing, pathology/molecular follow-up, and rehab consults as needed.
Diagnosis & Indication
- Working diagnosis: [Suspected WHO Grade ___] glioma
- Surgical indication: Maximal safe resection improves overall survival (even for Grade IV GBM); tissue diagnosis needed for molecular profiling (IDH, 1p/19q, MGMT, TERT, ATRX)
- Goals: Maximal safe resection — remove as much enhancing (GBM) or FLAIR-abnormal (low-grade) tumor as safely possible while preserving neurological function
- EOR targets: For GBM: > 95% enhancing tumor; For LGG: maximum FLAIR resection
Awake vs Asleep Decision
- Awake craniotomy indications:
- Tumor in/near dominant hemisphere language areas
- Tumor in/near motor cortex (supplementary motor area, primary motor)
- Insular glioma
- Any tumor where subcortical mapping will define resection margins
- Asleep with monitoring:
- Non-dominant hemisphere, non-eloquent location
- MEP/SSEP monitoring sufficient
- Patient unable to cooperate with awake surgery
Position
- Patient position: Based on tumor location:
- Frontal: Supine, head rotated contralateral 20-40 degrees
- Temporal: Supine, head rotated contralateral 60-90 degrees
- Parietal: Supine or lateral, vertex turned toward floor
- Occipital: Prone, lateral, or Concorde
- Insular: Supine, head rotated 60-80 degrees contralateral (sylvian fissure approach)
- Head position: Tumor at highest point for gravity retraction
- Skull clamp: Mayfield 3-pin
- Awake craniotomy: Comfortable semi-reclined, face visible to neuropsych team
Incision
- Centered over tumor using navigation-guided marking
- For awake: Include enough exposure for cortical and subcortical mapping
- Type: Curvilinear, extending 2-3 cm beyond tumor margins
Approach
- Direct convexity craniotomy over the tumor
- For insular tumors: Pterional or extended sylvian approach — split sylvian fissure widely
- Craniotomy size: Generous — must see normal brain margin around tumor, and expose cortical mapping sites
Key Surgical Steps
- Craniotomy — navigation-confirmed over tumor with surrounding normal cortex exposed
- Dural opening — curvilinear, reflect toward tumor
- Cortical mapping (if awake):
- Map motor cortex (direct cortical stimulation, 1-4 mA bipolar probe)
- Map language sites (counting, naming, reading — watch for speech arrest, paraphasias)
- Mark positive sites with sterile tags
- Identify tumor on cortical surface — color change, consistency, navigation confirmation
- Corticotomy — enter through non-eloquent cortex, through a sulcus when possible (transsulcal approach)
- Subcortical resection:
- Use CUSA and bipolar for tumor removal
- Stay in the tumor — identify tumor-brain interface by color, consistency, and navigation
- 5-ALA fluorescence: Tumor glows pink/red under blue-violet light (for high-grade gliomas)
- Ultrasound to confirm tumor boundaries and depth
- Subcortical mapping (if awake):
- Stimulate white matter tracts during resection
- Motor response = near corticospinal tract (STOP)
- Speech error = near arcuate fasciculus or IFOF (STOP)
- Mapping defines the functional boundary of resection
- Progressive circumferential resection — work around the tumor, deepening progressively
- Assess extent of resection:
- Navigation (note brain shift limitation)
- Intraoperative ultrasound
- 5-ALA fluorescence (any residual fluorescence?)
- Intraoperative MRI (if available) — gold standard for EOR assessment
- Final hemostasis — bipolar, Surgicel, Gelfoam
- Send specimens: Multiple samples from different tumor regions; mark enhancing rim vs core vs margin
Critical Anatomy & Structures at Risk
- Corticospinal tract — mapped by MEPs and subcortical stimulation; DTI shows displacement
- Language networks — Broca area, Wernicke area, arcuate fasciculus, IFOF, SLF
- Supplementary motor area (SMA) — medial frontal; resection causes transient contralateral akinesia that typically recovers
- Pericallosal arteries — medial tumors; branches supply motor cortex
- Middle cerebral artery branches — lateral/insular tumors
- Lenticulostriate arteries — deep/insular tumors; supply internal capsule
- Optic radiations — temporal/parietal/occipital tumors (Meyer’s loop in temporal lobe)
- Basal ganglia / internal capsule — deep margin of many tumors
Equipment & Instrumentation
- Operating microscope
- Stereotactic navigation (MRI + fMRI + DTI overlays)
- CUSA (Cavitron Ultrasonic Aspirator) — primary debulking tool
- Intraoperative ultrasound
- 5-ALA (Gleolan) — patient takes 20 mg/kg PO 2-4 hours pre-op (for Grade III/IV); blue-violet light filter on microscope
- Bipolar (multiple tip sizes)
- Microsurgical instruments
- Cortical/subcortical stimulator (bipolar probe, 60 Hz, 1-4 mA)
- Mapping tags (sterile numbered markers)
- Hemostatic agents
- Specimen containers (labeled by tumor region)
- [Intraoperative MRI if available]
Monitoring
- Asleep:
- SSEPs (median + tibial)
- MEPs (transcranial)
- Phase reversal (to localize central sulcus)
- ECoG (if seizure concern)
- Awake:
- Direct cortical stimulation (Penfield technique or high-frequency stimulation)
- Subcortical stimulation (during resection)
- Continuous speech/motor testing by neuropsych/speech pathology team
- ECoG (to detect afterdischarges from stimulation)
Anesthesia Considerations
- Asleep:
- Arterial line
- Foley
- Mannitol available
- Dexamethasone 10 mg (typically already on steroids)
- Levetiracetam 1000 mg IV
- Cefazolin 2g
- No paralytic (if MEP monitoring)
- 5-ALA: Cover patient from direct light exposure; photosensitivity precautions x 24h post-op
- Awake (asleep-awake-asleep or monitored anesthesia care):
- Propofol/remifentanil infusion for asleep phases
- Scalp block (regional anesthesia of supraorbital, auriculotemporal, greater/lesser occipital nerves)
- Dexmedetomidine during awake phase (light sedation without respiratory depression)
- Anti-emetics (ondansetron — vomiting during awake surgery is dangerous)
- Seizure protocol: cold saline irrigation if stimulation-induced seizure; low-dose propofol bolus if needed
- Comfortable positioning is critical — padded, semi-reclined, face visible
- Foley (patient will be awake for extended period)
Potential Complications & Contingencies
- New neurological deficit — if monitoring changes, stop resection at that boundary; SMA syndrome is typically transient
- Intraoperative seizure (awake) — cold saline irrigation on cortex, propofol 20-50 mg IV; consider converting to asleep
- Hemorrhage — meticulous bipolar hemostasis; consider that GBM neovasculature is fragile
- Brain swelling — mannitol, hyperventilation, ensure venous drainage, additional CSF drainage
- Incomplete resection — document planned residual if near eloquent structures; adjuvant therapy
- 5-ALA false positive — reactive gliosis and radiation changes can fluoresce; correlate with navigation
Operative Note Template
Preoperative Diagnosis: [Left/Right] [location] glioma (suspected WHO Grade ___)
Postoperative Diagnosis: Same (pending final pathology and molecular profiling)
Procedure: [Left/Right] [location] craniotomy for [awake/asleep] maximal safe resection of glioma [with cortical/subcortical mapping] [with 5-ALA fluorescence guidance] [with intraoperative MRI]
[Include details specific to glioma surgery: 5-ALA findings, mapping results, functional boundaries identified, extent of resection assessment method, specimen labeling]
Postoperative Plan
- ICU x 24 hours
- Neuro checks q1h x 24h — compare to preoperative baseline
- HOB 30 degrees
- MRI brain with gadolinium within 24-48 hours (MUST be within 48h before postoperative enhancement confounds interpretation)
- CT head immediately post-op (if any concern for hemorrhage)
- Dexamethasone taper (maintain therapeutic dose until edema stabilizes, then taper over 1-2 weeks)
- Continue AEDs (levetiracetam)
- DVT prophylaxis: SCDs, heparin SQ POD1
- 5-ALA precautions: Avoid direct sunlight/bright light x 24 hours (photosensitivity)
- Pain management: Acetaminophen-based
- Pathology and molecular markers:
- WHO grade
- IDH1/2 mutation status
- 1p/19q codeletion (oligodendroglioma)
- MGMT promoter methylation
- TERT promoter mutation
- ATRX loss
- Ki-67 proliferative index
- CDKN2A/B homozygous deletion (Grade 4 astrocytoma)
- Tumor board discussion with neuro-oncology, radiation oncology
- Adjuvant therapy:
- GBM: Concurrent temozolomide + radiation (Stupp protocol) → adjuvant TMZ
- Grade III: Radiation +/- chemotherapy depending on molecular profile
- Grade II (IDH-mutant): Consider observation if GTR; RT + chemotherapy if subtotal or progressive
- Follow-up: Clinic 2 weeks; serial MRI q3-4 months
Chief-Level Case Review
Use these as the senior-level mental model for Glioma Resection (Supratentorial):
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Glioma Resection (Supratentorial):
- What is the surgical goal: gross-total, maximal safe, decompression, diagnosis, or cytoreduction?
- What eloquent cortex, tract, cranial nerve, vessel, or sinus defines the stopping point?
- What adjunct changes the case: navigation, mapping, 5-ALA, ultrasound, endoscope, ICG, or neuromonitoring?
- What is the edema, steroid, seizure, DVT, and postop imaging plan?
- What complication would you check for first in PACU based on this lesion location?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Extent-of-resection goal and functional stopping points: [attending-specific]
- Mapping/monitoring, 5-ALA, ultrasound, ICG, endoscope, or tractography preferences: [attending-specific]
- Steroid, antiepileptic, mannitol/hypertonic saline, and antibiotic plan: [attending-specific]
- Postop MRI timing, ICU/floor threshold, and adjuvant-referral workflow: [attending-specific]