
Case Prep: Anterior Communicating Artery (AComA) Aneurysm Clipping
Case / Approach Snapshot
- Anatomy at risk: parent vessels, perforators, branch ostia, collateral circulation, venous drainage, cranial nerves, cisterns, and eloquent territories threatened by temporary occlusion or retraction.
- Operative steps: plan proximal and distal control, expose the corridor, obtain cerebrospinal fluid/brain relaxation, identify parent vessels before the lesion, treat the lesion/device target, and confirm flow and hemostasis before closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: intraoperative rupture, thromboembolism, branch or perforator compromise, vasospasm, inadequate proximal control, bypass or reconstructive options, anticoagulation/reversal, and postoperative surveillance.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [ruptured/unruptured] anterior communicating artery aneurysm presenting with [SAH/incidental finding] planned for [right/left] pterional craniotomy for microsurgical clipping.
Figures, Imaging & Video
🎥 Operative videos & resources
- Atlas / approach: Pterional craniotomy chapter · Supraorbital eyebrow AComA case
- Video searches: AComA aneurysm clipping on YouTube · AComA aneurysm surgery on Neurosurgical Atlas
- Angio anatomy: neuroangio.org — ACA / AComA complex, perforators, cross-filling, projection patterns
🧭 Operative approach: Pterional craniotomy — detailed corridor setup, step-by-step technique & figures
Copyrighted operative figures/videos are linked, not copied. Embedded figures below are public-domain or CC-BY; see media-sources.md and CREDITS.md.
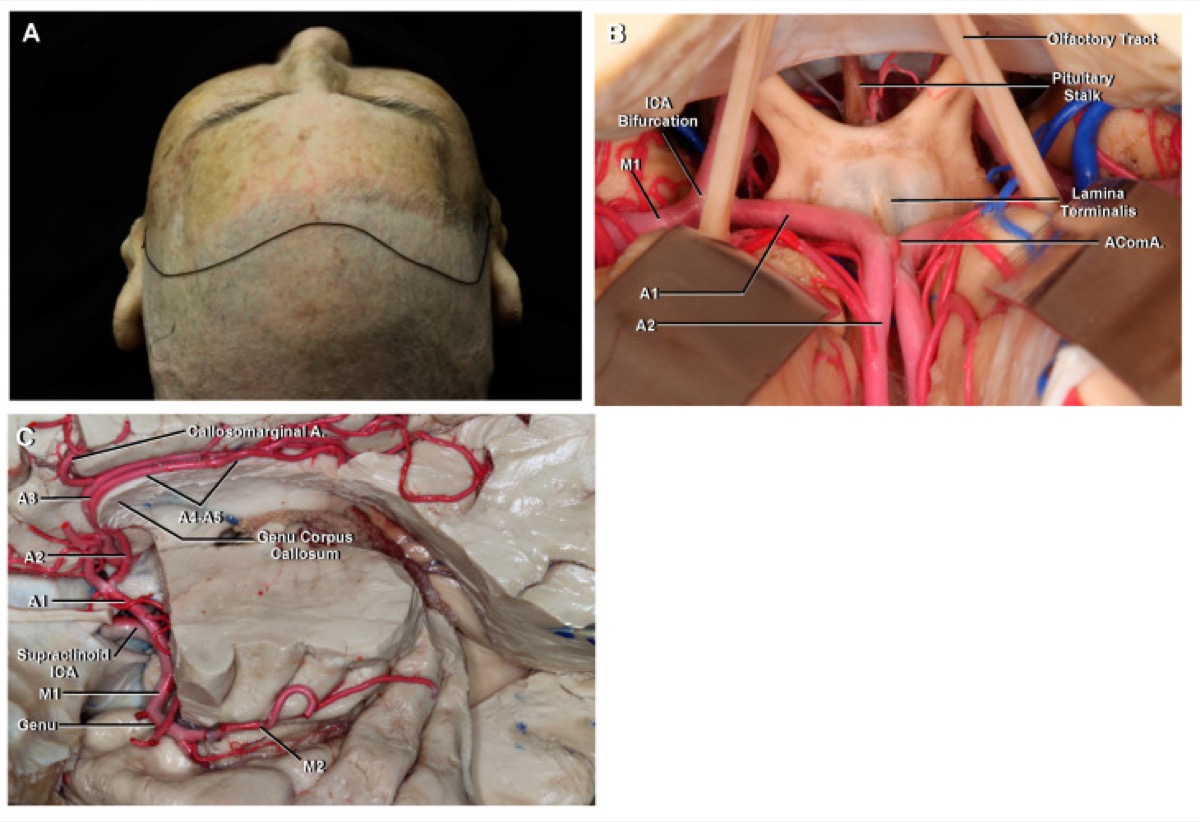
Poblete T et al., Microsurgical Anatomy of the Anterior Circulation, Brain Sci 2021;11(4):519 — CC BY 4.0.
High-Yield Literature
- Anterior Communicating Artery Aneurysm Clipping: Experience at a Tertiary Care Center with Respect to Intraoperative Rupture — Singh RC. Asian journal of neurosurgery 2020. PubMed
- Utility of evoked potentials during anterior cerebral artery and anterior communicating artery aneurysm clipping — Rabai F. Clinical neurophysiology practice 2022. PubMed
- Contralateral Vasospasm in an Uncomplicated Elective Anterior Communicating Artery Aneurysm Clipping — Knight JA 2nd. World neurosurgery 2020. PubMed
- Clinical use of 3D printed models for anterior communicating artery aneurysm clipping: a prospective cohort study — Feng C. Frontiers in surgery 2025. PubMed
- Paradoxical giftedness and memory decline after anterior communicating artery aneurysm clipping: A high-resolution MRI case report — Mugikura S. Journal of clinical imaging science 2025. PubMed
- Posterior ischemic optic neuropathy with acute monocular vision loss following clipping of anterior communicating artery aneurysm. A case report and review of literature — Sharma AK. Surgical neurology international 2021. PubMed
- Different Sides of Craniotomy for Anteriorly Superiorly Projecting Anterior Communicating Artery Aneurysm Clipping: Outcome and Long-Term Cognitive Function: A Single-Center Retrospective Study — Chen J. World neurosurgery 2025. PubMed
- Letter to the Editor Regarding “Contralateral Vasospasm in an Uncomplicated Elective Anterior Communicating Artery Aneurysm Clipping” — Marrone S. World neurosurgery 2024. PubMed
- Infrared thermography brain mapping surveillance in vascular neurosurgery for anterior communicating artery aneurysm clipping — de Font-Réaulx Rojas E. Surgical neurology international 2018. PubMed
- Anterior communicating artery aneurysm clipping using standard small fronto-pterional approach, clipping with 3 Lazic clips — Reinert M. Neurosurgical focus 2015. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
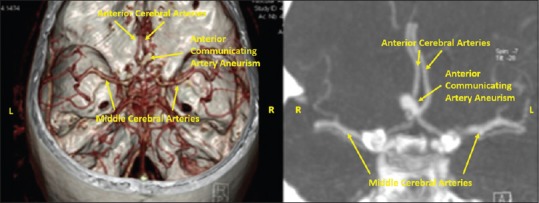 Figure 1. Unruptured incidental anterior communicating artery aneurysm of 8 × 5 mm Source: Infrared thermography brain mapping surveillance in vascular neurosurgery for anterior communicating artery aneurysm clipping — Surgical Neurology International 2018; CC BY-NC-SA.
Figure 1. Unruptured incidental anterior communicating artery aneurysm of 8 × 5 mm Source: Infrared thermography brain mapping surveillance in vascular neurosurgery for anterior communicating artery aneurysm clipping — Surgical Neurology International 2018; CC BY-NC-SA.
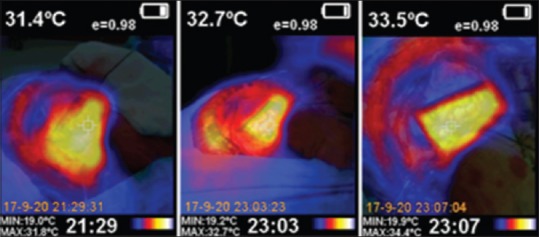 Figure 2. Image of the basal cortical metabolism measured by infrared thermography mapping (left). The temperature of the frontal lobe cortex is 31.4°C. Image of the second infrared thermography… Source: Infrared thermography brain mapping surveillance in vascular neurosurgery for anterior communicating artery aneurysm clipping — Surgical Neurology International 2018; CC BY-NC-SA.
Figure 2. Image of the basal cortical metabolism measured by infrared thermography mapping (left). The temperature of the frontal lobe cortex is 31.4°C. Image of the second infrared thermography… Source: Infrared thermography brain mapping surveillance in vascular neurosurgery for anterior communicating artery aneurysm clipping — Surgical Neurology International 2018; CC BY-NC-SA.
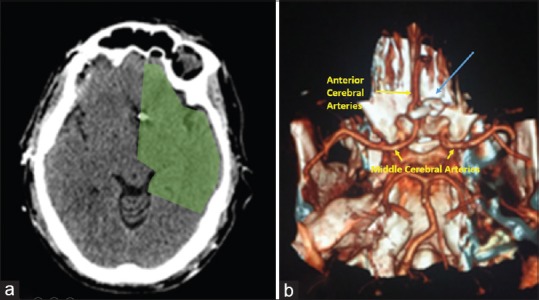 Figure 3. Postoperative computed tomography and angio-CT. No evidence of ischemia in the A1 or anterior communicating artery territory. Adequate clip placement in the neck of the aneurysm with… Source: Infrared thermography brain mapping surveillance in vascular neurosurgery for anterior communicating artery aneurysm clipping — Surgical Neurology International 2018; CC BY-NC-SA.
Figure 3. Postoperative computed tomography and angio-CT. No evidence of ischemia in the A1 or anterior communicating artery territory. Adequate clip placement in the neck of the aneurysm with… Source: Infrared thermography brain mapping surveillance in vascular neurosurgery for anterior communicating artery aneurysm clipping — Surgical Neurology International 2018; CC BY-NC-SA.
 Figure 4. Source: Infrared thermography brain mapping surveillance in vascular neurosurgery for anterior communicating artery aneurysm clipping — Surg Neurol Int. 2018 Sep 20;9:188. doi: 10.4103/sni.sni_58_18; CC BY-NC-SA.
Figure 4. Source: Infrared thermography brain mapping surveillance in vascular neurosurgery for anterior communicating artery aneurysm clipping — Surg Neurol Int. 2018 Sep 20;9:188. doi: 10.4103/sni.sni_58_18; CC BY-NC-SA.
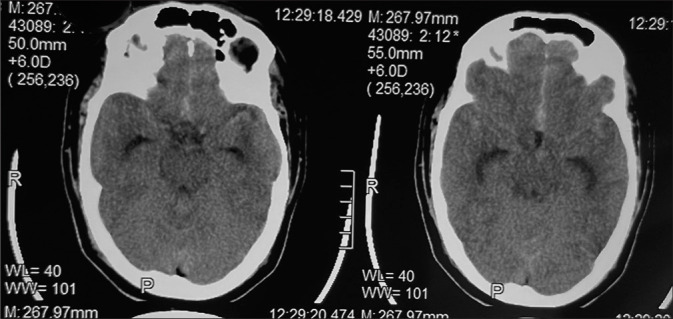 Figure 1:. NCCT brain showing SAH in the interhemispheric fissure and bilateral sylvian fissure. Source: Posterior ischemic optic neuropathy with acute monocular vision loss following clipping of anterior communicating artery aneurysm. A case report and review of literature — Surgical Neurology International 2021; CC BY-NC-SA.
Figure 1:. NCCT brain showing SAH in the interhemispheric fissure and bilateral sylvian fissure. Source: Posterior ischemic optic neuropathy with acute monocular vision loss following clipping of anterior communicating artery aneurysm. A case report and review of literature — Surgical Neurology International 2021; CC BY-NC-SA.
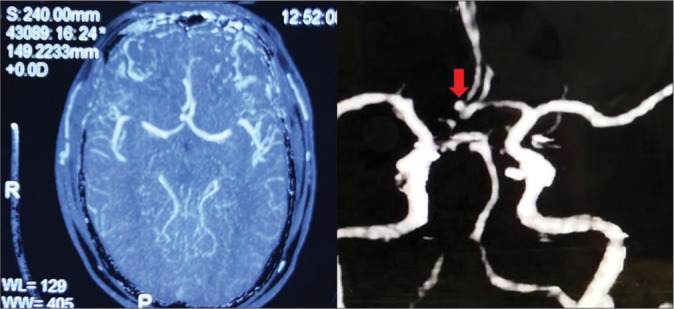 Figure 2:. Preoperative CT angiography was showing an anterior communicating artery aneurysm. Source: Posterior ischemic optic neuropathy with acute monocular vision loss following clipping of anterior communicating artery aneurysm. A case report and review of literature — Surgical Neurology International 2021; CC BY-NC-SA.
Figure 2:. Preoperative CT angiography was showing an anterior communicating artery aneurysm. Source: Posterior ischemic optic neuropathy with acute monocular vision loss following clipping of anterior communicating artery aneurysm. A case report and review of literature — Surgical Neurology International 2021; CC BY-NC-SA.
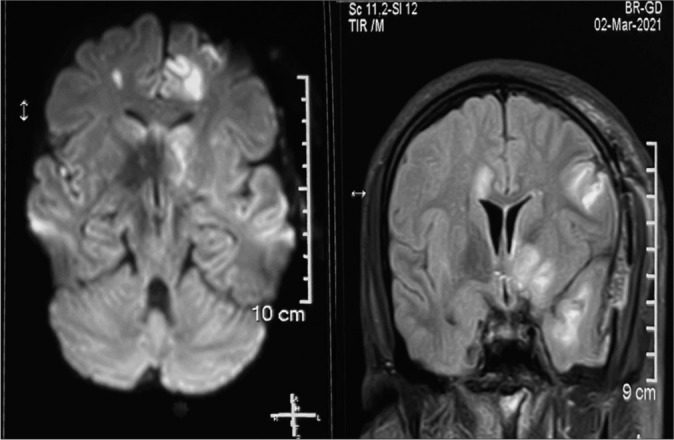 Figure 3:. MRI brain showing multiple focal infarcts. Source: Posterior ischemic optic neuropathy with acute monocular vision loss following clipping of anterior communicating artery aneurysm. A case report and review of literature — Surgical Neurology International 2021; CC BY-NC-SA.
Figure 3:. MRI brain showing multiple focal infarcts. Source: Posterior ischemic optic neuropathy with acute monocular vision loss following clipping of anterior communicating artery aneurysm. A case report and review of literature — Surgical Neurology International 2021; CC BY-NC-SA.
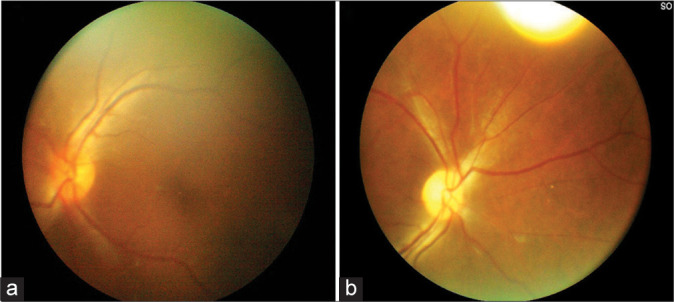 Figure 4:. (a) Fundus on postoperative day 3: Normal vessels, disc margins (b) well-defined disc with attenuation of blood vessels fundus picture on 15th postoperative day. Source: Posterior ischemic optic neuropathy with acute monocular vision loss following clipping of anterior communicating artery aneurysm. A case report and review of literature — Surgical Neurology International 2021; CC BY-NC-SA.
Figure 4:. (a) Fundus on postoperative day 3: Normal vessels, disc margins (b) well-defined disc with attenuation of blood vessels fundus picture on 15th postoperative day. Source: Posterior ischemic optic neuropathy with acute monocular vision loss following clipping of anterior communicating artery aneurysm. A case report and review of literature — Surgical Neurology International 2021; CC BY-NC-SA.
 Figure 9. Source: Posterior ischemic optic neuropathy with acute monocular vision loss following clipping of anterior communicating artery aneurysm. A case report and review of literature — Surg Neurol Int. 2021 Sep 20;12:471. doi: 10.25259/SNI_551_2021; CC BY-NC-SA.
Figure 9. Source: Posterior ischemic optic neuropathy with acute monocular vision loss following clipping of anterior communicating artery aneurysm. A case report and review of literature — Surg Neurol Int. 2021 Sep 20;12:471. doi: 10.25259/SNI_551_2021; CC BY-NC-SA.
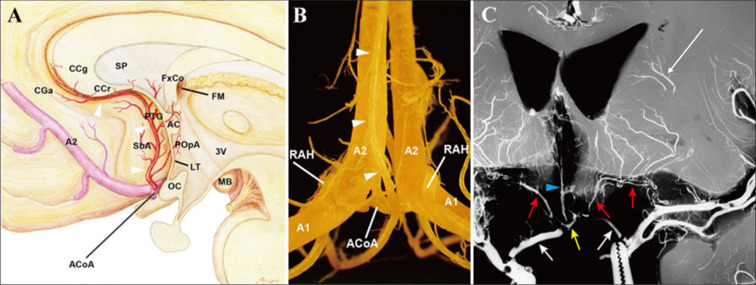 Figure 1:. Anatomy of the subcallosal and recurrent arteries of Heubner. (A) A schematic illustration, viewed sagittally, demonstrates the course and territory of the subcallosal artery…. Source: Paradoxical giftedness and memory decline after anterior communicating artery aneurysm clipping: A high-resolution MRI case report — Journal of Clinical Imaging Science 2025; CC BY-NC-SA.
Figure 1:. Anatomy of the subcallosal and recurrent arteries of Heubner. (A) A schematic illustration, viewed sagittally, demonstrates the course and territory of the subcallosal artery…. Source: Paradoxical giftedness and memory decline after anterior communicating artery aneurysm clipping: A high-resolution MRI case report — Journal of Clinical Imaging Science 2025; CC BY-NC-SA.
History of Present Illness
- Chief complaint: Thunderclap headache / loss of consciousness / incidental
- Hunt-Hess grade (if SAH): I-V
- Fisher grade (if SAH): 1-4
- Aneurysm size: ___ mm
- Dome projection: superior / anterior / posterior / inferior
- Prior SAH episodes:
Past Medical History
- Hypertension
- Smoking
- Family history of aneurysms
- Anticoagulation
- Allergies:
- Medications:
Imaging Review
CTA / DSA
- Aneurysm location: AComA
- Dome projection: (critical for surgical planning)
- Superior: most common; projects toward interhemispheric fissure
- Anterior: projects toward planum sphenoidale
- Posterior: projects toward hypothalamus/lamina terminalis (highest risk at surgery)
- Inferior: toward chiasm
- Size and neck width:
- A1 dominance: Left dominant / Right dominant / Codominant
- Approach side: Typically from the side of the dominant A1 (better angle to see AComA complex)
- If codominant: approach from right (non-dominant hemisphere) unless other factors
- A1 segments: Length, course, perforators
- A2 segments: Origin, course, relationship to dome
- AComA anatomy: Length, caliber, perforators (hypothalamic perforators from superior/posterior surface)
- Recurrent artery of Heubner: Origin from A1-A2 junction or proximal A2; courses back along A1
- Frontopolar and orbitofrontal arteries:
- Gyrus rectus: Size and relationship to aneurysm
- Cross-filling: Competency of AComA (compression studies)
CT Head
- SAH pattern (interhemispheric blood suggests AComA)
- Frontal lobe hematoma (common with AComA rupture)
- Hydrocephalus (common with AComA SAH)
Navigation
- CTA loaded
- A1-AComA-A2 complex mapped
Labs
- CBC, BMP, Coags
- Type and crossmatch (2 units)
- Na (hyponatremia common with AComA SAH — cerebral salt wasting)
Neurological Examination
- GCS:
- Abulia / personality changes (frontal lobe, bilateral ACA territory):
- Memory (anterior communicating perforators supply memory circuits):
- Lower extremity weakness (ACA territory):
- Language (if left-sided approach):
- Visual fields (chiasm proximity):
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: microscope, clip tray with temporary/permanent clips, ICG/Doppler, vascular instruments, blood available, DSA/CTA images displayed, and bypass/parent-vessel rescue plan for complex aneurysms.
- Special needs: arterial line, BP target before and after occlusion, nimodipine/EVD/SAH pathway if ruptured, seizure prophylaxis by lesion/location, dexamethasone only when edema risk warrants, and neuromonitoring for deep/eloquent corridors.
- Immediate postop orders: ICU neuro checks, SBP parameters, CTA/DSA or CT timing, EVD/vasospasm surveillance for SAH, antiepileptic plan, DVT timing, and focused motor/language/cranial-nerve exams.
Approach Selection
- Side of approach: Typically from the side of the DOMINANT A1
- Dominant A1 = more direct view of AComA complex
- Follow the dominant A1 to the AComA
- Non-dominant A1: may be hypoplastic, harder to follow
- Alternative: Right pterional (if non-dominant hemisphere, codominant A1s)
- Interhemispheric approach: Rarely — for superiorly projecting aneurysms with bilateral A1 access
Position
- Patient position: Supine
- Head position: Rotated 20-30 degrees contralateral (LESS rotation than MCA — need to see across midline). Extended to drop the frontal lobe from the anterior skull base. Vertex tilted down.
- Skull clamp: Mayfield
- Single pin: Contralateral frontal
- Double pins: Ipsilateral retroauricular
- Table: Reverse Trendelenburg
Incision
- Type: Curvilinear pterional incision (same as MCA)
- Key: May need slightly more medial/frontal exposure than MCA
Approach: Pterional Craniotomy (with Anterior Interhemispheric Corridor)
- Craniotomy: Standard pterional — flush sphenoid wing, low frontal exposure
- Key difference from MCA: Need medial frontal exposure along the skull base to the planum sphenoidale
- Gyrus rectus resection: Often needed (1-1.5 cm subpial resection) to visualize the AComA complex deep in the interhemispheric fissure
Microsurgical Steps
- Pterional craniotomy — flush sphenoid wing
- Dural opening — curvilinear based on sphenoid ridge
- Sylvian fissure split — proximal split to identify the ipsilateral ICA and A1 origin
- CSF drainage — open carotid and chiasmatic cisterns; drain CSF from lamina terminalis cistern
- Identify ipsilateral A1 at ICA bifurcation
- Follow A1 medially toward the AComA
- Identify ipsilateral optic nerve — A1 runs over the optic nerve/chiasm
- Identify recurrent artery of Heubner — courses back from A1-A2 junction along A1
- Gyrus rectus resection — subpial resection of 1-1.5 cm to expose AComA complex
- Identify AComA, contralateral A1, and both A2 segments
- Identify hypothalamic perforators — arise from POSTERIOR/SUPERIOR surface of AComA; MUST preserve
- Proximal control — temporary clip on ipsilateral A1 (and contralateral A1 if cross-filling)
- Dissect aneurysm neck — direction depends on dome projection:
- Superior projection: dome in interhemispheric fissure; dissect neck from below
- Anterior projection: dome against planum; visible early (careful not to rupture during approach)
- Posterior projection: dome toward hypothalamus; HIGHEST RISK — dissect dome LAST, work around neck
- Inferior projection: dome toward chiasm; early identification needed
- Clip application:
- Clip parallel to AComA axis
- Preserve A1, A2, AComA, Heubner, and perforators
- Fenestrated clip may be needed if A2 incorporated
- Confirmation: Micro-Doppler, ICG — all parent vessels and perforators patent
Critical Anatomy & Structures at Risk
- Hypothalamic perforators — from posterior/superior AComA surface → supply hypothalamus and memory circuits. Injury → memory deficit, DI, hypothalamic dysfunction
- Recurrent artery of Heubner — supplies head of caudate and anterior limb of internal capsule. Injury → contralateral face/arm weakness and dysarthria
- Contralateral A1 and A2 — must be preserved for bilateral ACA territory perfusion
- Optic chiasm/nerves — lie beneath the A1 segments
- Frontopolar and orbitofrontal arteries — early A2 branches
- Lamina terminalis — thin membrane forming anterior wall of third ventricle
- Gyrus rectus — partial resection acceptable; bilateral resection → abulia
Equipment
- Operating microscope
- Navigation (CTA)
- Micro-Doppler
- ICG videoangiography
- Aneurysm clips (including fenestrated for A2 preservation)
- Temporary clips (for ipsilateral A1, contralateral A1 if needed)
- High-speed drill
- Microsurgical instruments
Monitoring
- SSEPs
- MEPs (bilateral — ACA supplies leg motor cortex)
- EEG
Anesthesia Considerations
- Same as MCA aneurysm protocol
- Special attention to Na monitoring (cerebral salt wasting more common with AComA)
- Burst suppression available for temporary clipping
Potential Complications & Contingencies
- Hypothalamic perforator injury → memory deficit (particularly with posterior-projecting dome)
- Heubner artery injury → contralateral face/arm weakness, dysarthria
- Bilateral ACA infarction → abulia, akinetic mutism, bilateral leg weakness
- Intraoperative rupture → proximal A1 temporary clip; may need contralateral A1 clip
- Vasospasm (ruptured cases)
- DI / hypothalamic dysfunction (from perforator injury)
Operative Note Template
Preoperative Diagnosis: [Ruptured/Unruptured] anterior communicating artery aneurysm
Postoperative Diagnosis: Same
Procedure: [Right/Left] pterional craniotomy for microsurgical clipping of AComA aneurysm
[Follow MCA aneurysm template with specific modifications:]
- Describe dominant A1 identification and follow to AComA
- Describe gyrus rectus resection extent
- Describe AComA complex anatomy (A1s, A2s, AComA, perforators, Heubner)
- Describe dome projection and dissection strategy
- Describe clip placement relative to AComA axis
- Describe ICG/Doppler confirmation of all vessels including contralateral A1/A2
Postoperative Plan
- Same as MCA aneurysm post-op plan
- Na monitoring q4-6h (cerebral salt wasting is more common with AComA)
- Memory assessment — formal neuropsych testing if concern for perforator injury
- DI monitoring — strict I&Os, UOP hourly (hypothalamic perforators at risk)
- If ruptured: EVD management if placed; hydrocephalus monitoring
- Behavioral assessment: abulia, personality changes (frontal lobe injury)
Chief-Level Case Review
Use these as the senior-level mental model for Anterior Communicating Artery (AComA) Aneurysm Clipping:
- Decision point: The operation is won or lost on control: identify inflow, outflow, perforators, collateral options, and the fastest route to temporary control before exposing the lesion itself.
- Technical lever: Do not accept a cosmetic result over physiology: ICG/Doppler/DSA, branch patency, perforator preservation, and parent-vessel caliber matter more than how the clip or resection bed looks.
- Bailout: Have a rupture or ischemia script ready: lower pressure, suction strategy, temporary occlusion time, heparin/reversal plan, bypass/reconstruction threshold, and postop BP targets.
- Postop watch: Postop danger is delayed: vasospasm, thromboembolism, hyperperfusion, hemorrhage, edema, hydrocephalus, and seizure plans need explicit orders.
Common Pimp Questions
Use these to pressure-test preparation for Anterior Communicating Artery (AComA) Aneurysm Clipping:
- What is the proximal-control plan before the lesion is manipulated?
- Which branch, perforator, or venous structure is most likely to be injured in this exposure?
- What are the intraoperative rupture steps, including temporary clip, suction, BP, and backup clip strategy?
- What confirms treatment success: ICG, Doppler, puncture/deflation, DSA, or postoperative CTA?
- What postoperative BP, vasospasm, antiplatelet, or anticoagulation issue changes the orders tonight?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Preferred approach side, sylvian split style, and cisternal-opening sequence: [attending-specific]
- Temporary clip threshold, burst-suppression preference, and BP during occlusion: [attending-specific]
- Clip manufacturer/shape sequence and whether Doppler, ICG, puncture, or intraop DSA is routine: [attending-specific]
- Antiplatelet/anticoagulation reversal and restart timing: [attending-specific]