
Case Prep: Arteriovenous Malformation (AVM) Resection
Case / Approach Snapshot
- Anatomy at risk: parent vessels, perforators, branch ostia, collateral circulation, venous drainage, cranial nerves, cisterns, and eloquent territories threatened by temporary occlusion or retraction.
- Operative steps: plan proximal and distal control, expose the corridor, obtain cerebrospinal fluid/brain relaxation, identify parent vessels before the lesion, treat the lesion/device target, and confirm flow and hemostasis before closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: intraoperative rupture, thromboembolism, branch or perforator compromise, vasospasm, inadequate proximal control, bypass or reconstructive options, anticoagulation/reversal, and postoperative surveillance.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [left/right] [location] AVM (Spetzler-Martin grade [I-V]) presenting with [hemorrhage / seizures / headache / incidental] planned for craniotomy for microsurgical resection [± preoperative embolization].
Figures, Imaging & Video
🎥 Operative videos & resources
- Atlas / technique: The Neurosurgical Atlas — search brain AVM resection and review circumferential dissection, feeder control, and draining-vein preservation
- Video searches: brain AVM resection on YouTube · Spetzler-Martin AVM surgery
- Angio anatomy: neuroangio.org — feeders, nidus, early draining veins, associated aneurysms, and embolization strategy
🧭 Operative approach: Pterional craniotomy — detailed corridor setup, step-by-step technique & figures
Copyrighted operative figures/videos are linked, not copied. Embedded figures below are public-domain or CC-BY; see media-sources.md and CREDITS.md.
High-Yield Literature
- Hepatic arteriovenous malformation — Shionoya K. Clinical case reports 2023. PubMed
- Brain arteriovenous malformation with transdural blood supply: Current status — Piao J. Experimental and therapeutic medicine 2019. PubMed
- Uterine arteriovenous malformation - diagnosis and management — Szpera-Goździewicz A. Ginekologia polska 2018. PubMed
- Capillary Malformation-Arteriovenous Malformation Syndrome — Alluhaibi R. Cureus 2021. PubMed
- Advanced brain arteriovenous malformation embolization techniques — Saatci I. Journal of neurointerventional surgery 2025. PubMed
- Intermixed arteriovenous malformation and hemangioblastoma: case report and literature review — Healy V. CNS oncology 2020. PubMed
- Transvenous arteriovenous malformation embolization — Brahimaj BC. Journal of neurointerventional surgery 2020. PubMed
- Thrombosed Arteriovenous Malformation of Umbilical Cord — Damiani GR. Journal of obstetrics and gynaecology of India 2023. PubMed
- A giant pelvic arteriovenous malformation — Izumi T. IJU case reports 2024. PubMed
- Arteriovenous Malformation of the Cervical Cord Region — Tanitame K. Internal medicine (Tokyo, Japan) 2020. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
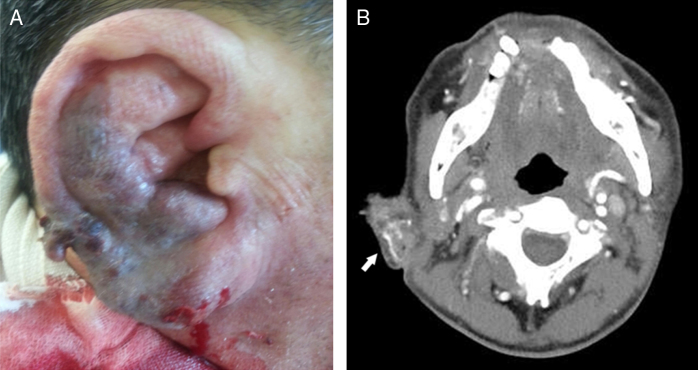 Figure 1. Gross findings and temporal bone computed tomographic angiography findings on the ear of a 60 year-old man, as recorded in the emergency room: (A) the patient presented with a swollen… Source: Arteriovenous malformation of the external ear: a clinical assessment with a scoping review of the literature☆ — Brazilian Journal of Otorhinolaryngology 2017; CC BY.
Figure 1. Gross findings and temporal bone computed tomographic angiography findings on the ear of a 60 year-old man, as recorded in the emergency room: (A) the patient presented with a swollen… Source: Arteriovenous malformation of the external ear: a clinical assessment with a scoping review of the literature☆ — Brazilian Journal of Otorhinolaryngology 2017; CC BY.
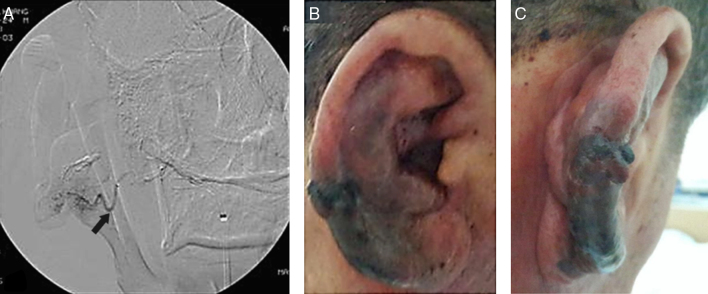 Figure 2. Preoperative therapeutic embolization using transfemoral cerebral angiography and gross ear findings 3 days after embolization: (A) transfemoral cerebral angiography revealed large… Source: Arteriovenous malformation of the external ear: a clinical assessment with a scoping review of the literature☆ — Brazilian Journal of Otorhinolaryngology 2017; CC BY.
Figure 2. Preoperative therapeutic embolization using transfemoral cerebral angiography and gross ear findings 3 days after embolization: (A) transfemoral cerebral angiography revealed large… Source: Arteriovenous malformation of the external ear: a clinical assessment with a scoping review of the literature☆ — Brazilian Journal of Otorhinolaryngology 2017; CC BY.
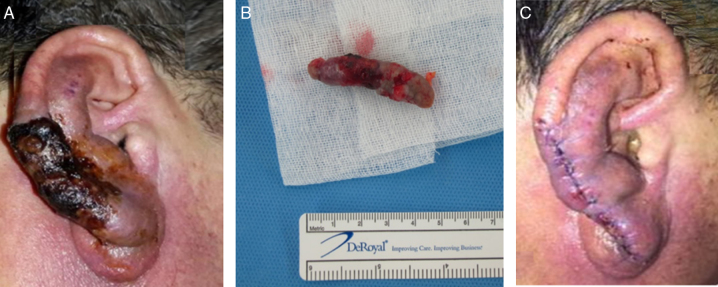 Figure 3. Gross ear findings at 2 weeks after embolization and total excision of the arteriovenous malformation. (A) Two weeks after transarterial embolization, the boundary of the necrotic skin… Source: Arteriovenous malformation of the external ear: a clinical assessment with a scoping review of the literature☆ — Brazilian Journal of Otorhinolaryngology 2017; CC BY.
Figure 3. Gross ear findings at 2 weeks after embolization and total excision of the arteriovenous malformation. (A) Two weeks after transarterial embolization, the boundary of the necrotic skin… Source: Arteriovenous malformation of the external ear: a clinical assessment with a scoping review of the literature☆ — Brazilian Journal of Otorhinolaryngology 2017; CC BY.
 Fig. 1. Findings of upper gastrointestinal endoscopy. Upper gastrointestinal endoscopy revealed a large ulcer at the duodenal bulb. Source: Efficacy of Arterial Embolization prior to Pancreaticoduodenectomy for Pancreatic Arteriovenous Malformation: A Case Report — Surgical Case Reports 2025; CC BY.
Fig. 1. Findings of upper gastrointestinal endoscopy. Upper gastrointestinal endoscopy revealed a large ulcer at the duodenal bulb. Source: Efficacy of Arterial Embolization prior to Pancreaticoduodenectomy for Pancreatic Arteriovenous Malformation: A Case Report — Surgical Case Reports 2025; CC BY.
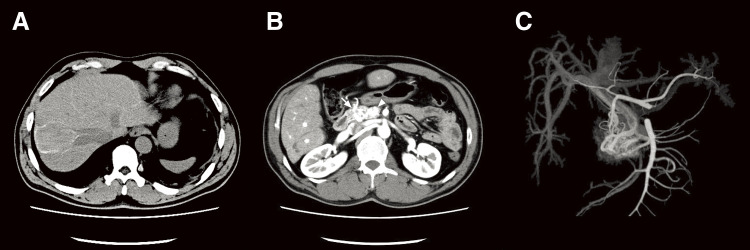 Fig. 2. Findings of computed tomography (CT). (A) Non-enhanced CT showed the presence of intrahepatic reticulated calcification, indicating the presence of Schistosomiasis japonica. (B)… Source: Efficacy of Arterial Embolization prior to Pancreaticoduodenectomy for Pancreatic Arteriovenous Malformation: A Case Report — Surgical Case Reports 2025; CC BY.
Fig. 2. Findings of computed tomography (CT). (A) Non-enhanced CT showed the presence of intrahepatic reticulated calcification, indicating the presence of Schistosomiasis japonica. (B)… Source: Efficacy of Arterial Embolization prior to Pancreaticoduodenectomy for Pancreatic Arteriovenous Malformation: A Case Report — Surgical Case Reports 2025; CC BY.
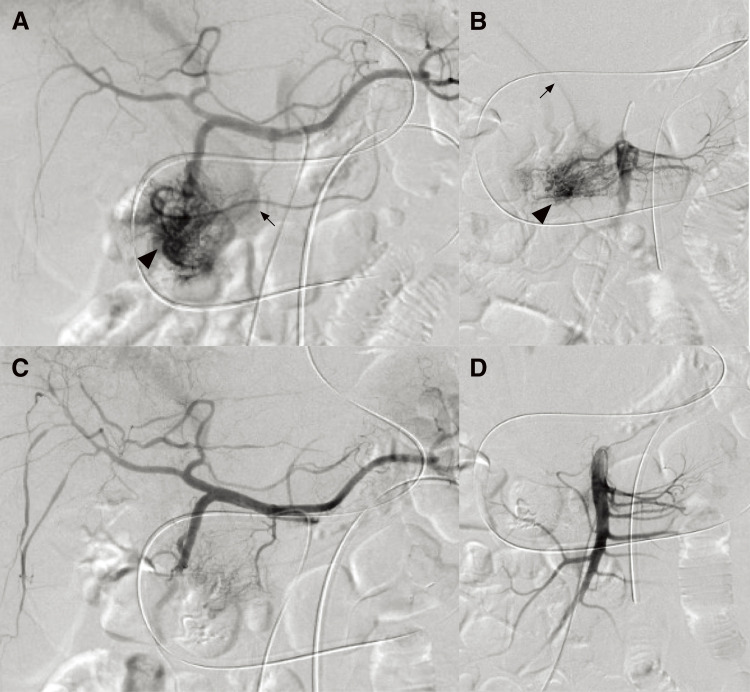 Fig. 3. Findings of angiography. (A) Angiography of the celiac axis showed a markedly proliferative vascular network at the pancreatic head (arrowhead) via the gastroduodenal artery and early… Source: Efficacy of Arterial Embolization prior to Pancreaticoduodenectomy for Pancreatic Arteriovenous Malformation: A Case Report — Surgical Case Reports 2025; CC BY.
Fig. 3. Findings of angiography. (A) Angiography of the celiac axis showed a markedly proliferative vascular network at the pancreatic head (arrowhead) via the gastroduodenal artery and early… Source: Efficacy of Arterial Embolization prior to Pancreaticoduodenectomy for Pancreatic Arteriovenous Malformation: A Case Report — Surgical Case Reports 2025; CC BY.
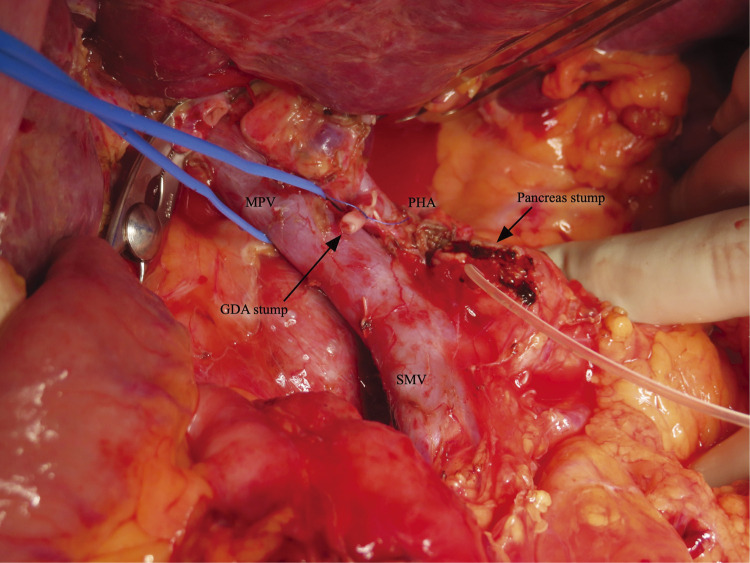 Fig. 4. Intraoperative findings. The intraoperative findings did not demonstrate the impact of arterial embolization on the pancreatic parenchyma.GDA, gastroduodenal artery; MPV, main portal… Source: Efficacy of Arterial Embolization prior to Pancreaticoduodenectomy for Pancreatic Arteriovenous Malformation: A Case Report — Surgical Case Reports 2025; CC BY.
Fig. 4. Intraoperative findings. The intraoperative findings did not demonstrate the impact of arterial embolization on the pancreatic parenchyma.GDA, gastroduodenal artery; MPV, main portal… Source: Efficacy of Arterial Embolization prior to Pancreaticoduodenectomy for Pancreatic Arteriovenous Malformation: A Case Report — Surgical Case Reports 2025; CC BY.
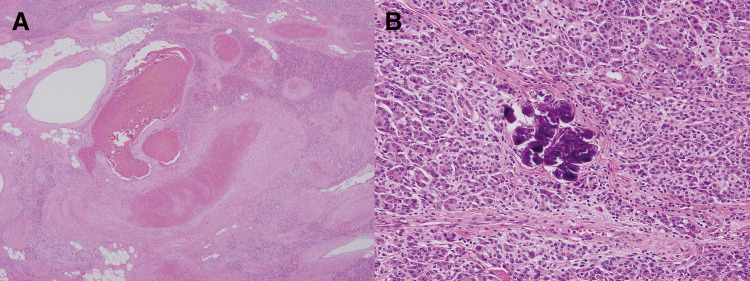 Fig. 5. Pathological findings of resected specimens (hematoxylin and eosin staining). (A) Dilated vessels of unequal size were found in the pancreatic parenchyma, consistent with the finding of… Source: Efficacy of Arterial Embolization prior to Pancreaticoduodenectomy for Pancreatic Arteriovenous Malformation: A Case Report — Surgical Case Reports 2025; CC BY.
Fig. 5. Pathological findings of resected specimens (hematoxylin and eosin staining). (A) Dilated vessels of unequal size were found in the pancreatic parenchyma, consistent with the finding of… Source: Efficacy of Arterial Embolization prior to Pancreaticoduodenectomy for Pancreatic Arteriovenous Malformation: A Case Report — Surgical Case Reports 2025; CC BY.
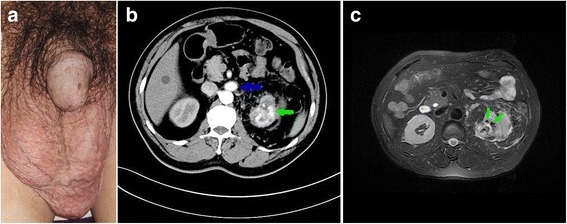 Fig. 1. a Physical examination showed grade 3 left varicocele. b Computed tomography showed early enhanced dilated renal vein (blue arrow) and irregular lesion in the upper pole of left kidney,… Source: Varicocele due to renal arteriovenous malformation mimicking a renal tumor: a case report — Journal of Medical Case Reports 2018; CC BY.
Fig. 1. a Physical examination showed grade 3 left varicocele. b Computed tomography showed early enhanced dilated renal vein (blue arrow) and irregular lesion in the upper pole of left kidney,… Source: Varicocele due to renal arteriovenous malformation mimicking a renal tumor: a case report — Journal of Medical Case Reports 2018; CC BY.
History of Present Illness
- Chief complaint: Intracranial hemorrhage / seizures / progressive deficit / headache / incidental
- Prior hemorrhage (annual rupture risk ~2-4%, higher if prior bleed, deep location, deep venous drainage, associated aneurysm):
- Seizure history:
- Prior embolization / radiosurgery:
Imaging Review
MRI/MRA
- Nidus location, size, eloquence of adjacent brain
- Flow voids, prior hemorrhage (hemosiderin)
DSA (gold standard)
- Spetzler-Martin grade:
- Size: < 3 cm (1), 3-6 cm (2), > 6 cm (3)
- Eloquence: non-eloquent (0), eloquent (1)
- Venous drainage: superficial only (0), any deep (1)
- Total = 1-5
- Supplementary Lawton-Young grade (age, bleeding, compactness) — refines risk
- Feeding arteries (which territories)
- Nidus compactness (compact vs diffuse)
- Venous drainage (superficial/deep, number of draining veins)
- Associated aneurysms (flow-related — may bleed)
- Flow characteristics (high vs low flow)
Navigation / Functional
- DSA/MRA/CTA fused to navigation
- fMRI / DTI if eloquent location
Labs
- CBC, BMP, Coags, Type and crossmatch (4 units — AVMs bleed)
Neurological Examination
- Complete exam focused on AVM location/eloquence; document baseline deficits
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: microscope, neuronavigation, ICG/Doppler, temporary clips/vascular instruments, blood available, embolization images loaded, and hybrid/DSA access if intraoperative angiography is planned.
- Special needs: arterial line, Foley, seizure prophylaxis for cortical lesions, BP floor/ceiling agreed with anesthesia, staged embolization plan, and readiness for swelling/normal-perfusion-pressure breakthrough.
- Immediate postop orders: ICU neuro checks, strict SBP target, CT/CTA or formal angiography per surgeon, seizure prophylaxis, dexamethasone if edema risk, DVT timing, and low threshold for imaging with headache/deficit.
Diagnosis & Indication
- Working diagnosis: [Location] AVM, SM grade [__]
- Indication: Ruptured AVM, low-grade (SM I-II) AVMs, refractory seizures; SM III individualized; SM IV-V usually NOT resected (high risk) unless ruptured/progressive
- Goals: Complete nidus resection (partial resection does NOT reduce hemorrhage risk and may increase it)
- Multimodal: Preoperative embolization (reduce flow, target deep feeders), radiosurgery (small/deep), or surgery
Preoperative Embolization
- Staged embolization days before surgery to reduce nidus flow and target surgically inaccessible deep feeders
- Reduces intraoperative blood loss
Position
- Based on AVM location — lesion at highest point; Mayfield
- Large craniotomy (wider than the nidus — need to see all feeders and draining veins)
Microsurgical Principles (Spetzler/Lawton)
- Wide craniotomy — expose nidus plus margin
- Identify the draining vein(s) — PRESERVE until the end (premature venous occlusion → nidus engorgement and rupture)
- Circumferential dissection around the nidus
- Feeding artery control first — coagulate/clip arterial feeders progressively, working around the nidus
- Stay on the nidus — dissect in the gliotic plane immediately around the nidus (avoid entering nidus → bleeding; avoid straying into normal brain → deficit)
- Deep feeders last — these are thin-walled, fragile, hard to coagulate (“AVM feeders from hell”); may need clips, careful bipolar, hemostatic agents
- Take the draining vein LAST — only after all arterial supply controlled; vein should become dark/less pulsatile when arterial feeders are eliminated
- Deliver nidus
- Meticulous hemostasis — inspect resection bed; “normal perfusion pressure breakthrough” risk
- ICG / intraoperative angiography — confirm no residual nidus
Critical Anatomy & Structures at Risk
- Draining vein(s) — preserve until arterial supply controlled
- Deep perforating feeders — fragile, dangerous bleeding source
- Eloquent cortex / white matter tracts — depending on location
- En passage vessels — arteries that supply both nidus and normal brain (preserve the normal branch)
Equipment
- Microscope, navigation, ICG, intraoperative angiography capability
- AVM micro-clips (mini/micro aneurysm clips for feeders)
- Bipolar (multiple), hemostatic agents (Surgicel, Floseal)
- CUSA, cottonoids
- Cell saver
Monitoring
- SSEPs, MEPs (if eloquent), EEG
Anesthesia
- Arterial line, central line, 2 large-bore IVs
- 4 units crossmatched, massive transfusion protocol available
- Controlled hypotension during resection (reduce bleeding)
- Post-resection: avoid hypertension (NPPB risk)
Potential Complications
- Hemorrhage — major risk; preserve draining vein until end
- Normal perfusion pressure breakthrough (NPPB) — post-resection hyperemia/edema/hemorrhage in surrounding brain; strict BP control
- Residual nidus — intraoperative angiography to confirm complete resection
- Neurological deficit — eloquent location, perforator injury
- Seizures
Operative Note Template
Preoperative Diagnosis: [Left/Right] [location] arteriovenous malformation, Spetzler-Martin grade [__] [ruptured/unruptured]
Postoperative Diagnosis: Same
Procedure: [Left/Right] [location] craniotomy for microsurgical resection of AVM [following preoperative embolization]
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids / Blood products: [4 units crossmatched, cell saver] Adjuncts: Neuronavigation, ICG videoangiography, intraoperative/postoperative DSA Monitoring: SSEP / MEP [/ mapping if eloquent] — stable Complications: None
Indications: [Age]yo [M/F] with a [ruptured/symptomatic] [location] AVM (SM grade [__]). After [staged preoperative embolization and] discussion of risks/benefits/alternatives (including radiosurgery and observation), microsurgical resection was undertaken.
Description of Procedure: After consent and time-out, general anesthesia was induced with arterial/central access, crossmatched blood and cell saver available, and neuromonitoring established. The head was fixed in Mayfield and positioned with the lesion uppermost. A wide [location] craniotomy was performed — larger than the nidus to expose all feeders and draining veins — and the dura opened.
Under the microscope, the nidus and its major draining vein(s) were identified; the draining vein was preserved and protected throughout. Circumferential dissection was carried out in the gliotic plane immediately around the nidus, progressively coagulating and dividing arterial feeders while staying on the nidus and sparing en-passage vessels. The deep, thin-walled feeders were controlled with micro-clips and careful bipolar. Only after all arterial supply was eliminated — confirmed by the draining vein becoming dark and less pulsatile — was the draining vein coagulated and divided last, and the nidus delivered en bloc.
The resection bed was inspected and meticulous hemostasis obtained under controlled normotension. Intraoperative angiography (ICG ± catheter DSA) confirmed no residual nidus or early venous filling. The dura was closed, the bone flap replaced, and the scalp closed in layers. Strict blood-pressure control was maintained to prevent normal-perfusion-pressure breakthrough. The patient was transferred to the NSICU in stable condition.
Postoperative Plan
- NSICU, neuro checks q1h
- Strict BP control (e.g., SBP < 120-140) to prevent NPPB hemorrhage x 24-48h
- Postop DSA within 24-48h (confirm complete resection — residual nidus needs re-resection)
- Seizure prophylaxis
- CT head, monitor for hemorrhage/edema
- Follow-up DSA, clinic
Chief-Level Case Review
Use these as the senior-level mental model for Arteriovenous Malformation (AVM) Resection:
- Decision point: The operation is won or lost on control: identify inflow, outflow, perforators, collateral options, and the fastest route to temporary control before exposing the lesion itself.
- Technical lever: Do not accept a cosmetic result over physiology: ICG/Doppler/DSA, branch patency, perforator preservation, and parent-vessel caliber matter more than how the clip or resection bed looks.
- Bailout: Have a rupture or ischemia script ready: lower pressure, suction strategy, temporary occlusion time, heparin/reversal plan, bypass/reconstruction threshold, and postop BP targets.
- Postop watch: Postop danger is delayed: vasospasm, thromboembolism, hyperperfusion, hemorrhage, edema, hydrocephalus, and seizure plans need explicit orders.
Common Pimp Questions
Use these to pressure-test preparation for Arteriovenous Malformation (AVM) Resection:
- What is the proximal-control plan before the lesion is manipulated?
- Which branch, perforator, or venous structure is most likely to be injured in this exposure?
- What are the intraoperative rupture steps, including temporary clip, suction, BP, and backup clip strategy?
- What confirms treatment success: ICG, Doppler, puncture/deflation, DSA, or postoperative CTA?
- What postoperative BP, vasospasm, antiplatelet, or anticoagulation issue changes the orders tonight?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Preferred approach side, sylvian split style, and cisternal-opening sequence: [attending-specific]
- Temporary clip threshold, burst-suppression preference, and BP during occlusion: [attending-specific]
- Clip manufacturer/shape sequence and whether Doppler, ICG, puncture, or intraop DSA is routine: [attending-specific]
- Antiplatelet/anticoagulation reversal and restart timing: [attending-specific]