
Case Prep: Pituitary Adenoma — Endoscopic Endonasal Transsphenoidal Approach
Case / Approach Snapshot
- Anatomy at risk: tumor compartment, arterial supply, venous drainage/sinuses, cranial nerves, white-matter tracts, pituitary/CSF pathways when relevant, and functional cortex.
- Operative steps: review imaging and goals, choose exposure, obtain brain relaxation, devascularize when possible, debulk internally, dissect capsule from critical structures, verify extent/safety, and reconstruct watertight closure; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: venous or arterial injury, swelling, seizure, cranial nerve or endocrine change, CSF leak, residual tumor left for safety, staged surgery, radiation, or adjuvant therapy.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [size] cm [functioning/non-functioning] pituitary [micro/macro]adenoma presenting with [visual loss/headaches/endocrinopathy/apoplexy] planned for endoscopic endonasal transsphenoidal resection.
Figures, Imaging & Video
🎥 Operative videos & resources
- Atlas / approach: Endoscopic endonasal approach chapter — nasal phase, sphenoidotomy, sellar opening, tumor removal, and reconstruction
- Video searches: endoscopic transsphenoidal pituitary adenoma on YouTube · pituitary adenoma endonasal resection operative video
- Imaging/endocrine review: Radiopaedia — pituitary adenoma · PubMed Central — endoscopic transsphenoidal pituitary adenoma
CNS Video Library
🧭 Operative approach: Endoscopic endonasal approach — detailed corridor setup, step-by-step technique & figures
Copyrighted operative figures/videos are linked, not copied. Embedded figures below are public-domain or CC-BY; see media-sources.md and CREDITS.md.
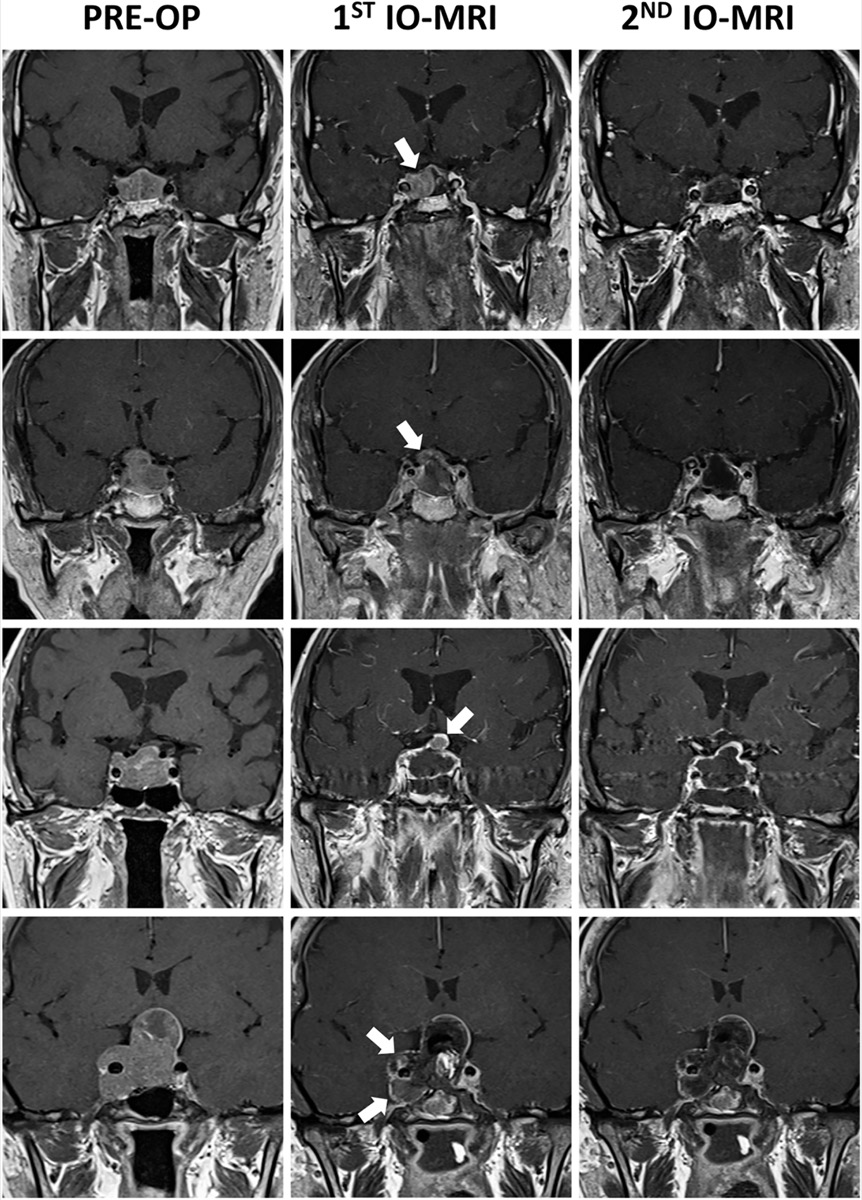
Macroadenoma with cavernous-sinus / suprasellar extension; intraoperative MRI detecting residual tumor (arrows). Source: Celtikci et al., Front Oncol 2021;11:733838, Fig 1. CC BY 4.0.
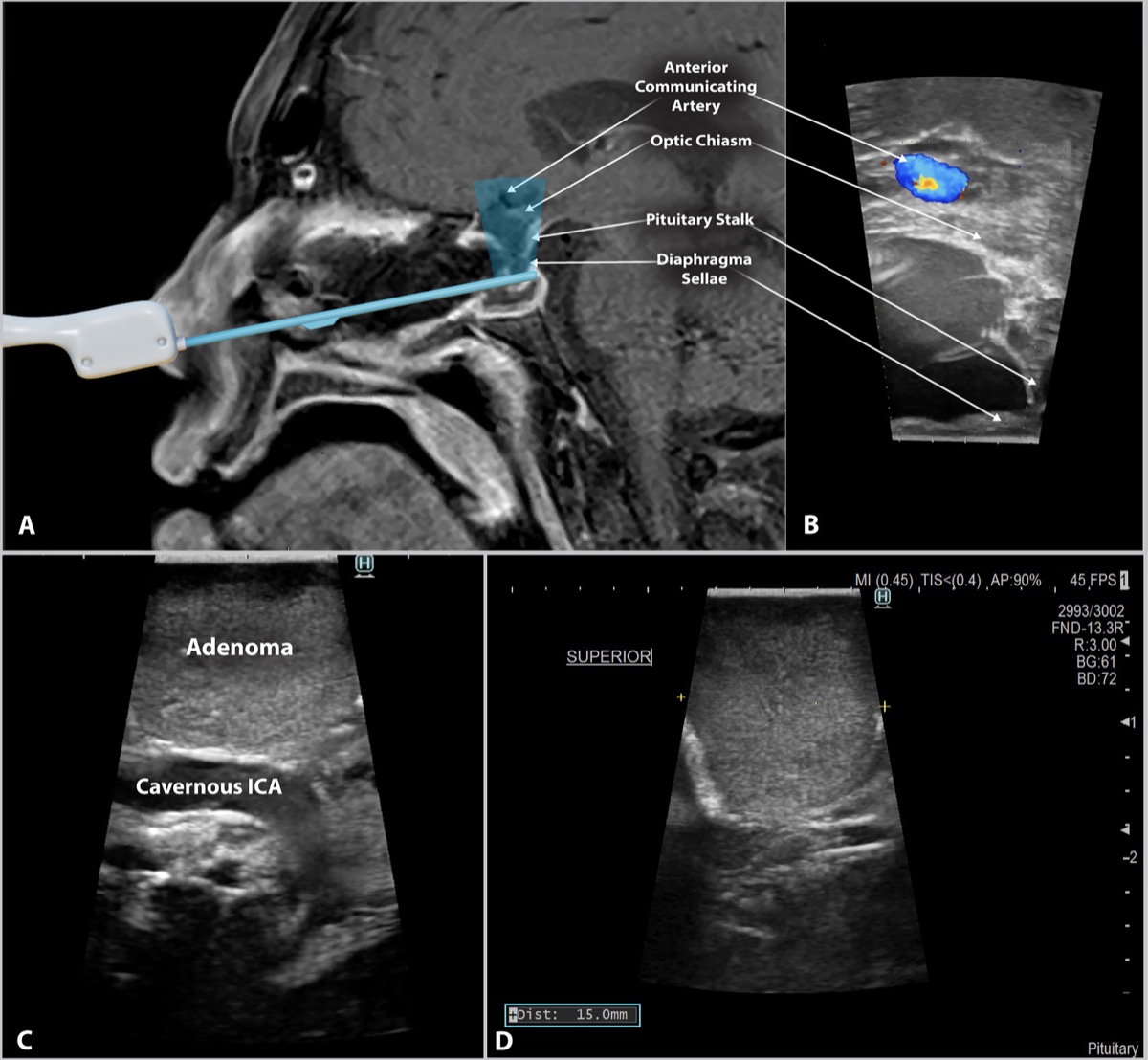
Intraoperative ultrasound during endonasal resection localizing the cavernous ICA and tumor margin. Source: Baker et al., Front Oncol 2022;12:1043697, Fig 1. CC BY 4.0.
High-Yield Literature
- Comparison of endoscopic and endoscope-assisted microscopic transsphenoidal surgery for pituitary adenoma resection: a prospective randomized study — Eördögh M. Frontiers in endocrinology 2025. PubMed
- Giant Pituitary Adenoma - Special Considerations — Tang OY. Otolaryngologic clinics of North America 2022. PubMed
- Endoscopic endonasal surgery for pituitary adenomas — Cappabianca P. World neurosurgery 2014. PubMed
- Surgical Anatomy Applied to the Resection of Craniopharyngiomas: Anatomic Compartments and Surgical Classifications — Almeida JP. World neurosurgery 2020. PubMed
- Endoscopic endonasal transsphenoidal approach: outcome analysis of 100 consecutive procedures — Cappabianca P. Minimally invasive neurosurgery : MIN 2002. PubMed
- Endoscopic endonasal transsphenoidal removal of recurrent and regrowing pituitary adenomas: experience on a 59-patient series — Cavallo LM. World neurosurgery 2013. PubMed
- Surgical complications associated with the endoscopic endonasal transsphenoidal approach for pituitary adenomas — Cappabianca P. Journal of neurosurgery 2002. PubMed
- Endoscopic endonasal pituitary surgery: surgical and outcome analysis of 50 cases — Charalampaki P. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia 2007. PubMed
- Surgical Nuances of Endoscopic Endonasal Resection of Craniopharyngiomas: 2-Dimensional Operative Video — Almeida JP. Operative neurosurgery (Hagerstown, Md.) 2020. PubMed
- Endoscopic anatomy of sphenoid sinus for pituitary surgery — Unlu A. Clinical anatomy (New York, N.Y.) 2008. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
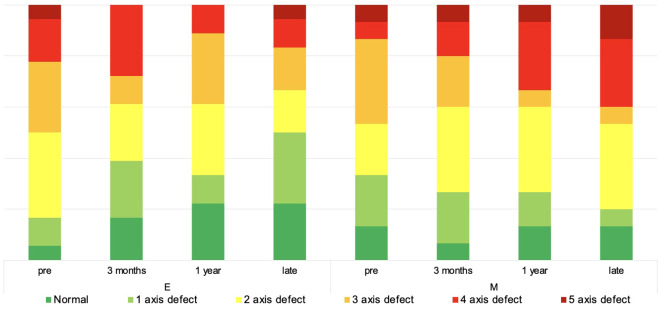 Figure 1. Anterior pituitary lobe function over time. The diagram depicts the non-continuous development of anterior pituitary lobe function over time. Source: Comparison of endoscopic and endoscope-assisted microscopic transsphenoidal surgery for pituitary adenoma resection: a prospective randomized study — Frontiers in Endocrinology 2025; CC BY.
Figure 1. Anterior pituitary lobe function over time. The diagram depicts the non-continuous development of anterior pituitary lobe function over time. Source: Comparison of endoscopic and endoscope-assisted microscopic transsphenoidal surgery for pituitary adenoma resection: a prospective randomized study — Frontiers in Endocrinology 2025; CC BY.
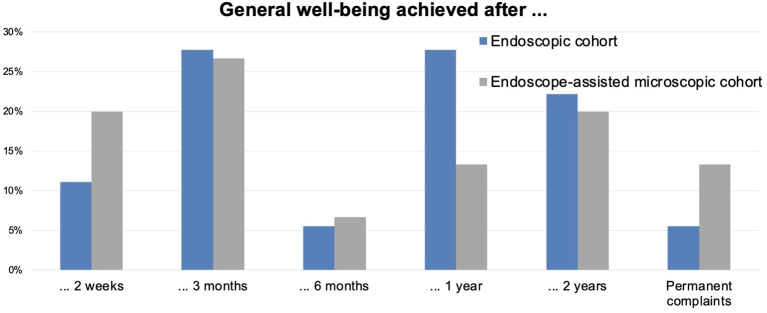 Figure 2. Achievement of overall well-being over time. The diagram depicts the non-continuous time point when symptom-free well-being was achieved. The values are in %. Source: Comparison of endoscopic and endoscope-assisted microscopic transsphenoidal surgery for pituitary adenoma resection: a prospective randomized study — Frontiers in Endocrinology 2025; CC BY.
Figure 2. Achievement of overall well-being over time. The diagram depicts the non-continuous time point when symptom-free well-being was achieved. The values are in %. Source: Comparison of endoscopic and endoscope-assisted microscopic transsphenoidal surgery for pituitary adenoma resection: a prospective randomized study — Frontiers in Endocrinology 2025; CC BY.
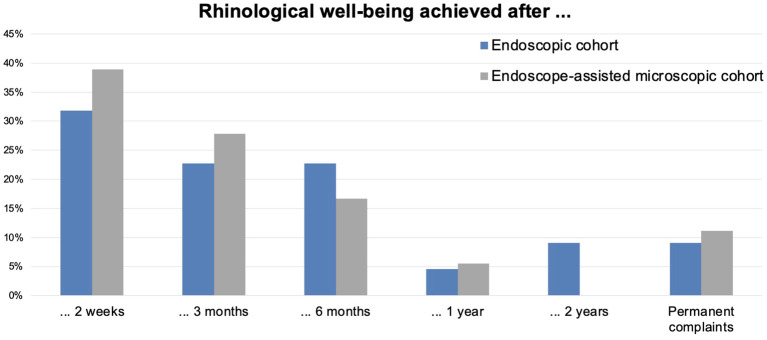 Figure 3. Achievement of rhinological well-being over time. The diagram depicts the non-continuous time point when symptom-free well-being was achieved. The values are in %. Source: Comparison of endoscopic and endoscope-assisted microscopic transsphenoidal surgery for pituitary adenoma resection: a prospective randomized study — Frontiers in Endocrinology 2025; CC BY.
Figure 3. Achievement of rhinological well-being over time. The diagram depicts the non-continuous time point when symptom-free well-being was achieved. The values are in %. Source: Comparison of endoscopic and endoscope-assisted microscopic transsphenoidal surgery for pituitary adenoma resection: a prospective randomized study — Frontiers in Endocrinology 2025; CC BY.
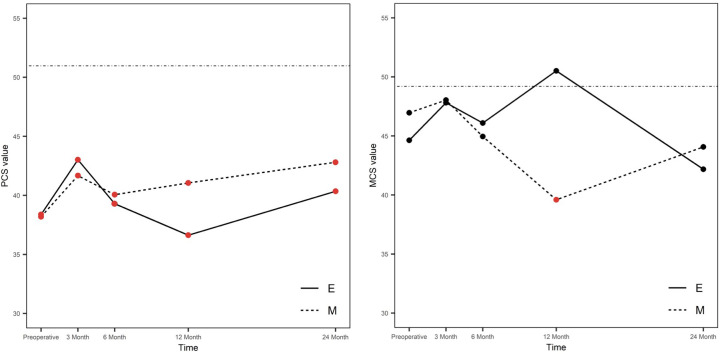 Figure 4. Mental and physical scores of SF-36 over time. E, endoscopic group; M, microsurgical group; MCS, mental component summary score; PCS, physical component summary score; continuous line,… Source: Comparison of endoscopic and endoscope-assisted microscopic transsphenoidal surgery for pituitary adenoma resection: a prospective randomized study — Frontiers in Endocrinology 2025; CC BY.
Figure 4. Mental and physical scores of SF-36 over time. E, endoscopic group; M, microsurgical group; MCS, mental component summary score; PCS, physical component summary score; continuous line,… Source: Comparison of endoscopic and endoscope-assisted microscopic transsphenoidal surgery for pituitary adenoma resection: a prospective randomized study — Frontiers in Endocrinology 2025; CC BY.
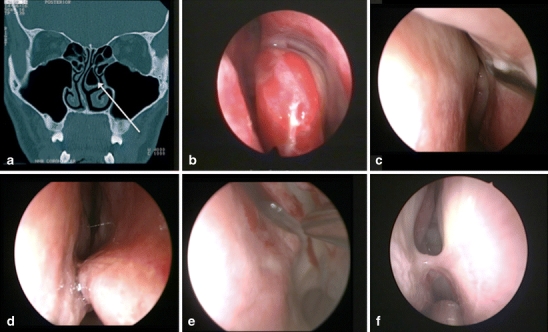 Fig. 1. Examples of endonasal anatomical variations that required surgical correction. a Coronal CT-scan with a left bullous middle turbinate, b left endonasal bullous middle turbinate, c left… Source: Variations of endonasal anatomy: relevance for the endoscopic endonasal transsphenoidal approach — Acta Neurochirurgica 2010; CC BY-NC.
Fig. 1. Examples of endonasal anatomical variations that required surgical correction. a Coronal CT-scan with a left bullous middle turbinate, b left endonasal bullous middle turbinate, c left… Source: Variations of endonasal anatomy: relevance for the endoscopic endonasal transsphenoidal approach — Acta Neurochirurgica 2010; CC BY-NC.
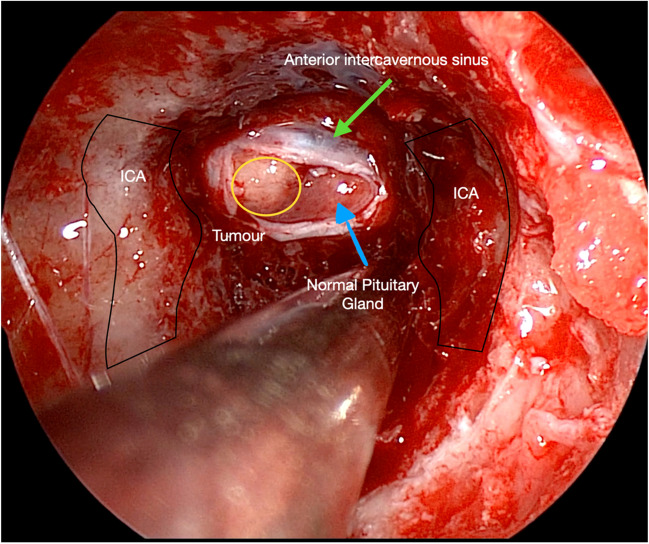 Fig. 1. An endoscopic view showing essential intra-sphenoidal anatomy. Internal Carotid arteries (ICA), a right-sided pituitary microadenoma (yellow) Source: HOW I DO IT: Cushing’s disease—selective adenomectomy via an endoscopic transsphenoidal approach — Acta Neurochirurgica 2024; CC BY.
Fig. 1. An endoscopic view showing essential intra-sphenoidal anatomy. Internal Carotid arteries (ICA), a right-sided pituitary microadenoma (yellow) Source: HOW I DO IT: Cushing’s disease—selective adenomectomy via an endoscopic transsphenoidal approach — Acta Neurochirurgica 2024; CC BY.
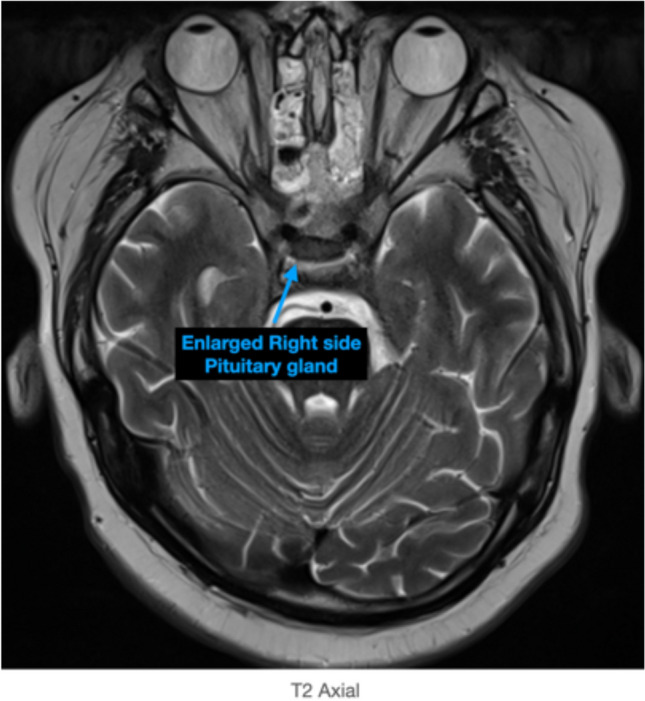 Fig. 2. Axial MRI T2 demonstrates a right-sided pituitary gland enlargement correlating to the pituitary microadenoma Source: HOW I DO IT: Cushing’s disease—selective adenomectomy via an endoscopic transsphenoidal approach — Acta Neurochirurgica 2024; CC BY.
Fig. 2. Axial MRI T2 demonstrates a right-sided pituitary gland enlargement correlating to the pituitary microadenoma Source: HOW I DO IT: Cushing’s disease—selective adenomectomy via an endoscopic transsphenoidal approach — Acta Neurochirurgica 2024; CC BY.
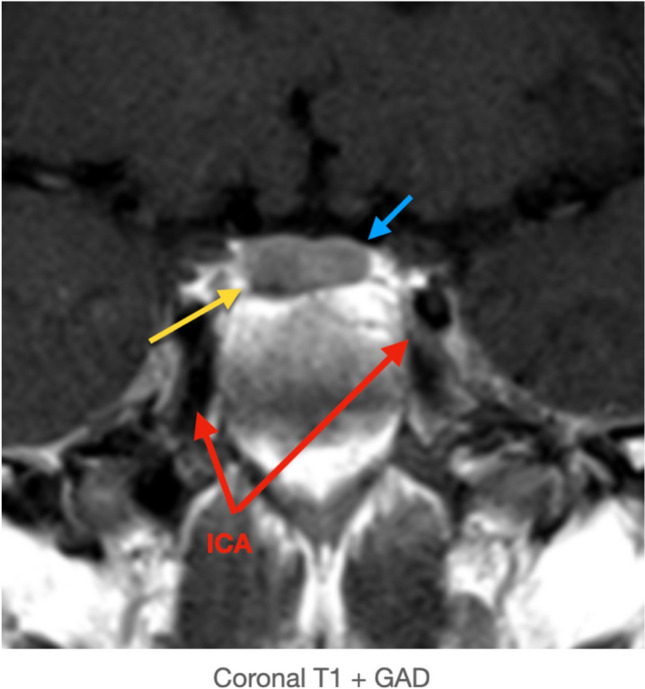 Fig. 3. Coronal T1 + GAD demonstrating the disproportionately enlarged right pituitary gland - microadenoma (yellow arrow), normal pituitary gland (blue arrow), and the internal carotid arteries… Source: HOW I DO IT: Cushing’s disease—selective adenomectomy via an endoscopic transsphenoidal approach — Acta Neurochirurgica 2024; CC BY.
Fig. 3. Coronal T1 + GAD demonstrating the disproportionately enlarged right pituitary gland - microadenoma (yellow arrow), normal pituitary gland (blue arrow), and the internal carotid arteries… Source: HOW I DO IT: Cushing’s disease—selective adenomectomy via an endoscopic transsphenoidal approach — Acta Neurochirurgica 2024; CC BY.
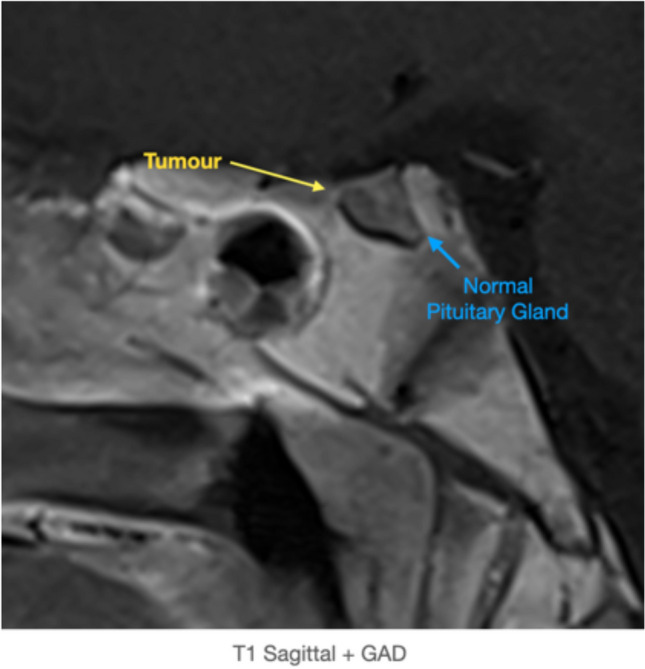 Fig. 4. T1 Sagittal + GAD demonstrating the pituitary microadenoma (yellow arrow) and normal pituitary gland (blue arrow). The conchal sphenoidal sinus can be appreciated Source: HOW I DO IT: Cushing’s disease—selective adenomectomy via an endoscopic transsphenoidal approach — Acta Neurochirurgica 2024; CC BY.
Fig. 4. T1 Sagittal + GAD demonstrating the pituitary microadenoma (yellow arrow) and normal pituitary gland (blue arrow). The conchal sphenoidal sinus can be appreciated Source: HOW I DO IT: Cushing’s disease—selective adenomectomy via an endoscopic transsphenoidal approach — Acta Neurochirurgica 2024; CC BY.
History of Present Illness
- Chief complaint: Visual field deficit / headaches / endocrinopathy / pituitary apoplexy
- Duration of symptoms:
- Visual changes (bitemporal hemianopsia, decreased acuity):
- Headache pattern:
- Endocrine symptoms:
- Acromegaly: enlarged hands/feet, coarsened features, sweating, joint pain
- Cushing disease: weight gain, striae, moon facies, easy bruising, proximal weakness
- Prolactinoma: amenorrhea/galactorrhea (F), decreased libido/gynecomastia (M)
- TSH-secreting: hyperthyroidism symptoms
- Hypopituitarism: fatigue, cold intolerance, decreased libido, adrenal insufficiency
- Apoplexy symptoms: sudden headache, visual loss, altered mental status, CN palsies
Past Medical History
- Prior transsphenoidal surgery
- Prior radiation (conventional, SRS)
- Diabetes mellitus (acromegaly)
- Hypertension (Cushing)
- Osteoporosis (Cushing, hypopituitarism)
- Adrenal insufficiency (on replacement)
- Hypothyroidism (on replacement)
- Obstructive sleep apnea (acromegaly)
- Cardiac disease (acromegaly)
- MEN1 syndrome
- Allergies:
- Medications (including hormone replacements):
Imaging Review
MRI Sella (Thin-cut, T1, T1+Gad, T2, Coronal and Sagittal)
- Tumor size: __ x __ x ___ mm (micro < 10mm, macro >= 10mm, giant >= 40mm)
- Enhancement pattern: Homogeneous / heterogeneous / cystic / hemorrhagic
- Sellar expansion: Floor eroded / intact
- Suprasellar extension:
- Chiasm compressed / elevated / displaced: [anterior / posterior / lateral]
- Distance from tumor to chiasm
- Chiasm position: prefixed / normal / postfixed
- Cavernous sinus invasion:
- Knosp grade: 0 / 1 / 2 / 3A / 3B / 4
- ICA encasement percentage
- Medial wall displacement vs invasion
- Infrasellar extension: Into sphenoid sinus / clivus
- Lateral extension: Into temporal fossa
- Stalk position: Midline / displaced
- Normal pituitary gland: Identified / compressed (location: superior / lateral)
- Signal characteristics:
- Hemorrhage (apoplexy): T1 bright
- Cystic components: T2 bright
- Consistency: firm (T2 dark) vs soft (T2 bright)
CT Sella / Sinuses
- Sphenoid sinus pneumatization: conchal / presellar / sellar (sellar = favorable)
- Septations within sphenoid sinus (may be off-midline, insert on carotid prominences)
- Sellar floor thickness
- Carotid canal bony coverage
- Nasal anatomy: septal deviation, turbinate hypertrophy
CTA (if large or vascular tumor)
- ICA course and relationship to tumor
- Cavernous ICA prominence
Navigation
- Thin-cut MRI sella loaded
- Thin-cut CT sinuses fused (for bony anatomy)
- ICA trajectories noted
- Sphenoid sinus septation mapped
Labs — Endocrine Workup
- Prolactin (rule out prolactinoma — medical management first if prolactin > 200)
- IGF-1 (screen for GH excess)
- GH (random and OGTT suppression if IGF-1 elevated)
- AM cortisol + ACTH (Cushing disease or adrenal insufficiency)
- 24-hour urine free cortisol (if Cushing suspected)
- Low-dose dexamethasone suppression test (if Cushing suspected)
- TSH, free T4 (TSH-secreting adenoma or central hypothyroidism)
- LH, FSH, estradiol/testosterone (hypogonadism)
- Alpha subunit (gonadotroph adenoma)
- BMP (Na — risk of DI/SIADH; glucose — acromegaly)
- CBC, coagulation
- Type and screen
Pre-op Endocrine Considerations
- Prolactinoma (PRL > 200): Trial of cabergoline first; surgery if refractory, intolerant, or CSF leak
- Cushing disease: Stress-dose steroids NOT given pre-op (need post-op cortisol nadir for remission); may need post-op replacement
- Acromegaly: Somatostatin analog pre-treatment may soften tumor
- Adrenal insufficiency: Stress-dose hydrocortisone 100 mg IV at induction
Neurological Examination
Visual
- Visual acuity: Each eye (Snellen)
- Visual fields: Formal perimetry (Humphrey/Goldmann) — look for bitemporal hemianopsia
- Fundoscopy: Optic disc pallor (chronic compression)
- Color vision: Ishihara plates (sensitive early indicator)
- Pupillary exam: RAPD
Cranial Nerves
- CN III, IV, VI: EOM — especially if cavernous sinus invasion
- CN V1, V2: Facial sensation (cavernous sinus)
Endocrine Exam
- Acromegalic features (hands, feet, jaw, tongue)
- Cushingoid features (moon facies, striae, buffalo hump, bruising)
- Thyroid exam
- Galactorrhea
Surgical Planning
Case Logistics, OR Needs & Orders
- OR setup: navigation, endoscope/microscope as approach requires, ENT co-surgeon for endonasal cases, Doppler, lumbar drain only when indicated, reconstruction materials, and visual/endocrine baseline available.
- Special needs: steroid strategy individualized (Cushing workup may require avoiding preop steroids), DI/sodium protocol, AM cortisol/endocrine labs, visual-check plan, arterial line for large/vascular cases, and CSF-leak/nasal precautions.
- Immediate postop orders: neuro and visual checks, strict I/O with sodium/urine specific gravity schedule when pituitary stalk risk exists, cortisol/endocrine replacement plan, nasal precautions, MRI/CT timing, steroid taper, and DVT prophylaxis timing.
Diagnosis & Indication
- Working diagnosis: [Functioning/Non-functioning] pituitary [micro/macro]adenoma
- Surgical indication:
- Non-functioning: visual field deficit, progressive growth, mass effect
- GH-secreting: biochemical cure (acromegaly)
- ACTH-secreting: biochemical cure (Cushing disease)
- Prolactinoma: medication intolerance/failure, CSF leak from medical therapy, apoplexy
- TSH-secreting: biochemical cure
- Goals: Gross total resection with decompression of optic apparatus and endocrine remission (if functioning)
Position
- Patient position: Supine
- Head position: Slight extension (10-15 degrees) to align nasal corridor with sphenoid sinus. Head in [Mayfield skull clamp / horseshoe headrest]
- Navigation: Electromagnetic or optical navigation registered
- Patient rotation: Turn bed 180 degrees from anesthesia (or side approach depending on OR setup)
- ENT co-surgeon: For nasal approach and closure (nasoseptal flap)
Approach: Endoscopic Endonasal Transsphenoidal
- Nasal phase:
- Topical decongestion (oxymetazoline or cocaine pledgets)
- Identify middle turbinate bilaterally
- Out-fracture or partially resect middle turbinate (right side typically)
- Posterior septectomy — create a common corridor
- Identify sphenoid ostia bilaterally (landmark: superior turbinate)
- Wide sphenoidotomy — connect both ostia
- Harvest nasoseptal flap (Hadad-Bassagasteguy flap) early — based on posterior septal artery (branch of sphenopalatine artery)
- Sphenoid phase:
- Remove sphenoid septations (note relationship to carotid prominences)
- Identify key landmarks:
- Sellar floor (center)
- Carotid prominences (lateral)
- Opticocarotid recess (superolateral)
- Clival recess (inferior)
- Planum sphenoidale (superior)
- Open sellar floor with drill/Kerrison rongeurs
- Lateral limits: medial wall of cavernous sinus / carotid prominences
- Superior limit: tuberculum sellae (for suprasellar extension)
- Sellar phase:
- Open dura in cruciate fashion (identify normal vs tumor dura color)
- Use ring curettes, suction, and angled endoscopes to remove tumor
- Technique: systematic removal — inferior, lateral, then superior
- Identify normal gland (usually compressed superolaterally or posteriorly) — preserve
- Suprasellar component: wait for descent after inferior debulking; may need angled endoscope (30/45 degrees)
- If Knosp 3-4: medial cavernous sinus wall may need to be opened — risk to ICA
- Confirm extent of resection with angled endoscopes and navigation
- Closure:
- Hemostasis with Surgicel, Gelfoam
- Intrasellar: Gelfoam or fat graft (abdominal)
- CSF leak repair (if intraoperative CSF leak):
- Inlay graft (collagen matrix or fascia lata) + overlay graft
- Nasoseptal flap coverage
- Fibrin glue
- +/- Lumbar drain
- No CSF leak: Gelfoam packing, may not need nasoseptal flap
- Nasal packing (Merocel or NasoPore, remove POD 3-5)
Critical Anatomy & Structures at Risk
- Internal carotid arteries — bilateral, lateral to sella in cavernous sinus; carotid prominences in sphenoid sinus
- Optic chiasm — superior to tumor; decompression is the goal
- Optic nerves — in optic canals, superolateral
- Normal pituitary gland — compressed by tumor; must identify and preserve
- Pituitary stalk — connects hypothalamus to gland; injury causes DI
- Cavernous sinus contents — CN III, IV, V1, V2, VI
- Sphenopalatine artery / posterior septal artery — blood supply to nasoseptal flap; preserve pedicle
- Diaphragma sellae — may descend into sella intraoperatively (marks complete suprasellar decompression)
- Arachnoid membrane — intact arachnoid = no CSF leak; if violated, must repair
Equipment & Instrumentation
- 0-degree and 30-degree rigid endoscopes (4mm)
- Endoscope holder/arm
- High-definition camera and monitor
- Navigation system (electromagnetic preferred for endonasal)
- High-speed drill (diamond burr for sellar floor)
- Kerrison rongeurs (various angles)
- Ring curettes (various sizes and angles)
- Micro-Doppler (to confirm ICA location)
- Endonasal instrument set (suction, dissectors, scissors)
- Hemostatic agents (Surgicel, Gelfoam, Floseal, fibrin glue)
- Closure materials: collagen matrix (DuraGen/DuraMatrix), fascia lata, abdominal fat
- Nasoseptal flap instruments
- Nasal packing (Merocel / NasoPore)
- Specimen containers
Monitoring
- Standard ASA monitors
- Visual evoked potentials (VEPs) — if significant chiasmal compression (not universally used)
- No IONM typically required for standard transsphenoidal
Anesthesia Considerations
- Arterial line (not always needed for straightforward cases)
- Two large-bore IVs
- Foley catheter (for DI monitoring — strict I&Os)
- No Foley suction (risk of mucosal injury to urethra from DI-related polyuria)
- Throat pack (prevents blood swallowing)
- Dexamethasone 10 mg IV (if not Cushing disease)
- Cushing disease: Do NOT give steroids pre-op (need post-op cortisol nadir)
- Adrenal insufficiency: Stress-dose hydrocortisone 100 mg IV at induction
- Cefazolin 2g IV
- Topical vasoconstrictors for nasal mucosa (oxymetazoline)
- Avoid excessive fluid administration (if concern for DI)
Potential Complications & Contingencies
- CSF leak — most common complication; nasoseptal flap closure, possible lumbar drain
- Diabetes insipidus (DI) — from stalk/posterior pituitary injury; monitor UOP, Na q4-6h; treat with DDAVP if UOP > 300 mL/hr with rising Na
- SIADH — delayed (typically days 5-10); monitor Na closely after discharge
- Hypopituitarism — new anterior pituitary deficits; check AM cortisol POD1
- ICA injury — catastrophic; pack and emergent angiography/endovascular treatment
- Visual worsening — from hematoma in sella or aggressive packing; emergent CT/MRI and return to OR
- Meningitis — monitor for fever, stiff neck; CSF leak is a risk factor
- Epistaxis — usually from sphenopalatine artery branch; may need repacking or embolization
- Incomplete resection — if cavernous sinus invasion (Knosp 3-4); plan for adjuvant SRS
Operative Note Template
Preoperative Diagnosis: [Non-functioning / GH-secreting / ACTH-secreting / prolactin-secreting] pituitary macroadenoma with [chiasmal compression / cavernous sinus invasion (Knosp ___)]
Postoperative Diagnosis: Same (pending final pathology and immunohistochemistry)
Procedure: Endoscopic endonasal transsphenoidal resection of pituitary adenoma
Surgeon: Co-surgeon (ENT): Assistant: Anesthesia: General endotracheal anesthesia
EBL: Fluids: Specimens: Pituitary adenoma (sent for permanent pathology, immunohistochemistry, Ki-67) Drains: [None / Lumbar drain] Complications: None Implants: None
Indications: The patient is a [age]yo [M/F] with a [size] cm [type] pituitary macroadenoma. Preoperative MRI demonstrated [findings including suprasellar extension, chiasmal compression, cavernous sinus involvement]. The patient presented with [visual field deficit / endocrinopathy / mass effect]. Formal visual field testing showed [findings]. Endocrine workup demonstrated [findings]. After discussion of risks, benefits, and alternatives, the patient elected to proceed with endoscopic endonasal transsphenoidal resection.
Description of Procedure: [Standard opening — anesthesia, positioning]
The patient was positioned supine with the head slightly extended in a [Mayfield clamp / horseshoe headrest]. [Electromagnetic navigation was registered and accuracy confirmed.] [A lumbar drain was placed.] The nose was prepared with oxymetazoline-soaked pledgets bilaterally. A time-out was performed.
Nasal phase: The endoscope was introduced into the [right] nasal cavity. The middle turbinate was identified and out-fractured laterally. A nasoseptal flap was harvested on the [right] side, based on the posterior septal artery, and stored in the nasopharynx. A posterior septectomy was performed to create a binostril corridor. The bilateral sphenoid ostia were identified at the level of the superior turbinates. A wide sphenoidotomy was performed, removing the rostrum of the sphenoid and connecting both ostia.
Sphenoid phase: The sphenoid sinus was entered and the septations were removed. The key landmarks were identified: sellar floor centrally, bilateral carotid prominences laterally, opticocarotid recesses superolaterally, and the clivus inferiorly. [Navigation confirmed anatomy.] The sellar floor was opened with a [high-speed drill / Kerrison rongeurs] and the opening was enlarged laterally to the medial edges of the cavernous sinuses and superiorly to the tuberculum sellae.
Sellar phase: The sellar dura was coagulated and opened in a cruciate fashion. [The tumor was immediately encountered and was noted to be soft/firm, gray/white/hemorrhagic.] Tumor removal was performed systematically using ring curettes, suction, and angled endoscopes. The inferior and lateral components were removed first, followed by the superior component. [With 30-degree endoscope visualization, the suprasellar component was observed to descend into the sella and was progressively removed.] The normal pituitary gland was identified [superiorly/posteriorly/laterally] and carefully preserved. [The diaphragma sellae was observed to descend into the sella, indicating complete suprasellar decompression.]
[For Knosp 3-4: The medial wall of the cavernous sinus was opened and tumor within the cavernous sinus was debulked. The ICA was identified with micro-Doppler and direct visualization, and all manipulation was kept medial to the artery.]
Intraoperative assessment: [An intraoperative CSF leak was / was not identified. Navigation confirmed extent of resection.]
Closure: Hemostasis was achieved with [Surgicel/Floseal]. The sella was packed with [Gelfoam / abdominal fat graft]. [An inlay collagen matrix graft was placed, followed by the nasoseptal flap to cover the entire bony defect. Fibrin glue was applied. / No CSF leak was noted, and the sella was packed with Gelfoam.] [Nasal packing was placed bilaterally.] A throat pack was removed. [The lumbar drain was clamped.]
Postoperative: The patient was awakened from anesthesia, extubated, and found to be neurologically intact. The patient was transferred to the neurosurgical ICU for monitoring.
Postoperative Plan
- ICU monitoring x 24 hours (or step-down)
- Neuro checks q1h x 12h, then q2h
- Strict I&Os: Urine output q1h (DI monitoring)
- Serum Na q6h x 48 hours, then BID until discharge
- DI protocol: If UOP > 300 mL/hr x 2 consecutive hours with rising Na > 145 → DDAVP 1 mcg IV; hold if Na < 135
- AM cortisol POD1 (6 AM): If < 2 → adrenal insufficiency, start hydrocortisone; if 2-10 → borderline, may need replacement; if > 10 → reassuring
- MRI sella within 24-48 hours (extent of resection)
- Visual fields: Formal perimetry at 4-6 weeks
- Cushing disease: Serial cortisol q6h (looking for nadir < 2-5 for remission); do NOT give steroids until cortisol confirmed low or patient symptomatic
- Acromegaly: IGF-1 and GH at 6-12 weeks post-op
- Activity: No nose blowing, no straining, no heavy lifting x 6 weeks
- Nasal care: Saline irrigations starting after packing removal (POD 3-5)
- Sinus precautions: No bending, no valsalva
- CSF leak precautions: If repair performed, HOB 30 degrees, stool softeners
- DVT prophylaxis: SCDs, heparin SQ POD1
- Discharge: POD 2-3 typically (if no DI, no CSF leak, Na stable)
- Follow-up: ENT debridement 1-2 weeks; Neurosurgery clinic 2-4 weeks; Endocrine 4-6 weeks
- Long-term: Annual MRI sella; endocrine labs; visual fields as needed
- Delayed hyponatremia warning: Educate patient to check Na at day 7-10 or return for symptoms (nausea, headache, confusion)
Chief-Level Case Review
Use these as the senior-level mental model for Pituitary Adenoma — Endoscopic Endonasal Transsphenoidal Approach:
- Decision point: Decide the real endpoint before opening: cure, cytoreduction, diagnosis, decompression, separation from critical structures, or safe maximal resection.
- Technical lever: Map what must be left behind: perforators, cranial nerves, venous sinuses, eloquent cortex/tracts, hypothalamus/pituitary axis, and adherent capsule planes.
- Bailout: Sequence matters: devascularize early when safe, create CSF/working space, debulk before traction, and preserve the arachnoid plane unless oncologic goals justify violating it.
- Postop watch: The postop plan should match the risk structure: endocrine/vision/swallow/CN checks, steroid taper, seizure plan, MRI timing, CSF-leak watch, and adjuvant-treatment handoff.
Common Pimp Questions
Use these to pressure-test preparation for Pituitary Adenoma — Endoscopic Endonasal Transsphenoidal Approach:
- What is the surgical goal: gross-total, maximal safe, decompression, diagnosis, or cytoreduction?
- What eloquent cortex, tract, cranial nerve, vessel, or sinus defines the stopping point?
- What adjunct changes the case: navigation, mapping, 5-ALA, ultrasound, endoscope, ICG, or neuromonitoring?
- What is the edema, steroid, seizure, DVT, and postop imaging plan?
- What complication would you check for first in PACU based on this lesion location?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Extent-of-resection goal and functional stopping points: [attending-specific]
- Mapping/monitoring, 5-ALA, ultrasound, ICG, endoscope, or tractography preferences: [attending-specific]
- Steroid, antiepileptic, mannitol/hypertonic saline, and antibiotic plan: [attending-specific]
- Postop MRI timing, ICU/floor threshold, and adjuvant-referral workflow: [attending-specific]