
Case Prep: Thoracic Discectomy (Transpedicular / Costotransversectomy / Lateral Extracavitary / Thoracoscopic)
Case / Approach Snapshot
- Anatomy at risk: level localization, cord/cauda equina, exiting and traversing roots, dura, vertebral artery or segmental vessels, esophagus/trachea/pleura/viscera by approach, and fusion/instrumentation landmarks.
- Operative steps: position and pad carefully, confirm level, expose the planned corridor, decompress neural elements, reconstruct or instrument when indicated, verify alignment/hardware, and close with attention to hematoma and wound risk; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: wrong level, durotomy, neurologic change, vertebral artery/visceral/pleural injury, graft or hardware problem, epidural hematoma, dysphagia/airway issue, and infection prevention/escalation.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with a [central/paracentral, soft/calcified] [T_-T_] thoracic disc herniation causing [myelopathy / thoracic radiculopathy / band-like pain] planned for [transpedicular / costotransversectomy / lateral extracavitary / mini-open lateral / thoracoscopic] discectomy.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Transthoracic approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Full Endoscopic Transforaminal Thoracic Discectomy Operative Technique — Barber SM. Journal of visualized experiments : JoVE 2024. PubMed
- Transforaminal endoscopic thoracic discectomy: surgical technique — Telfeian AE. Journal of spine surgery (Hong Kong) 2023. PubMed
- Mini-open lateral retropleural thoracic discectomy approach — Uribe JS. Neurosurgical focus: Video 2022. PubMed
- Anterior Versus Posterior Thoracic Discectomy: A Systematic Review — Hurley ET. Spine 2017. PubMed
- Uniportal, Transforaminal Endoscopic Thoracic Discectomy: Review and Technical Note — Lee SH. Neurospine 2023. PubMed
- Percutaneous endoscopic thoracic discectomy — Regan JJ. Neurosurgery clinics of North America 1996. PubMed
- Surgical efficacy of minimally invasive thoracic discectomy — Elhadi AM. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia 2015. PubMed
- Retropleural Thoracic Approach — Wewel JT. Neurosurgery clinics of North America 2020. PubMed
- Thoracic discectomy and plating — Hsieh PC. Neurosurgical focus 2011. PubMed
- Endoscopic Versus Traditional Thoracic Discectomy: A Multicenter Retrospective Case Series and Meta-Analysis — Sofoluke N. Neurosurgery 2025. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
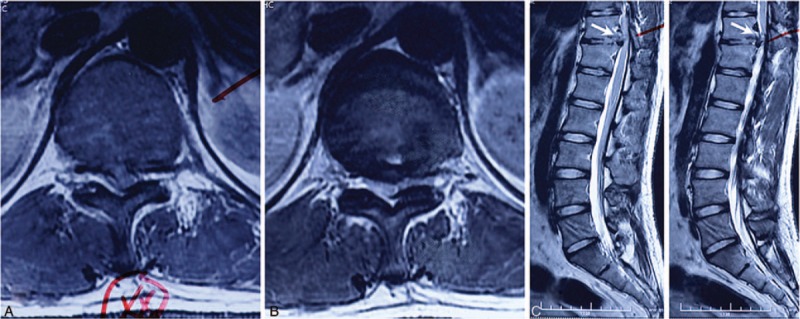 Figure 1. Preoperation magnetic resonance imaging revealed disc herniation on T11-12. Horizontal view (A and B) displayed secondary thoracic stenosis induced by herniated disc fragment; sagittal… Source: Percutaneous endoscopic thoracic discectomy via posterolateral approach — Medicine 2019; CC BY.
Figure 1. Preoperation magnetic resonance imaging revealed disc herniation on T11-12. Horizontal view (A and B) displayed secondary thoracic stenosis induced by herniated disc fragment; sagittal… Source: Percutaneous endoscopic thoracic discectomy via posterolateral approach — Medicine 2019; CC BY.
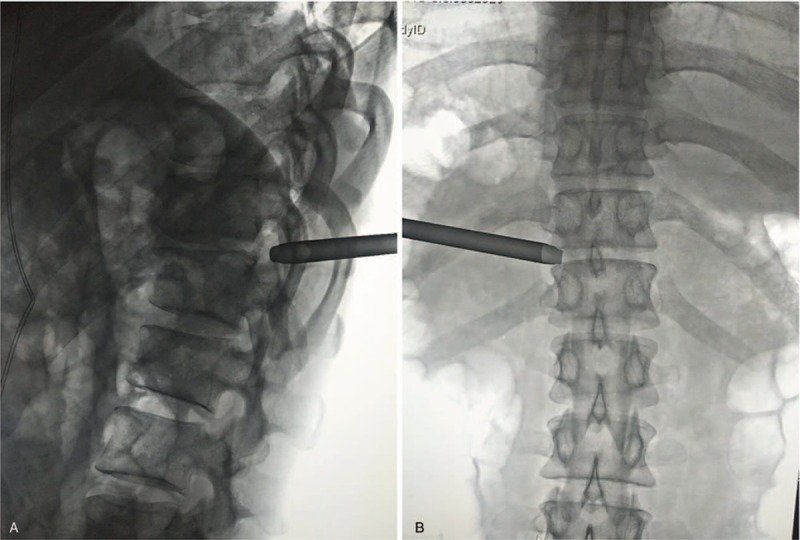 Figure 2. Intraoperation C-arm fluoroscopy displayed the location of the reamer cannula. The LT view showed that the distal end of the reamer cannula was anchored upon the cortex of superior… Source: Percutaneous endoscopic thoracic discectomy via posterolateral approach — Medicine 2019; CC BY.
Figure 2. Intraoperation C-arm fluoroscopy displayed the location of the reamer cannula. The LT view showed that the distal end of the reamer cannula was anchored upon the cortex of superior… Source: Percutaneous endoscopic thoracic discectomy via posterolateral approach — Medicine 2019; CC BY.
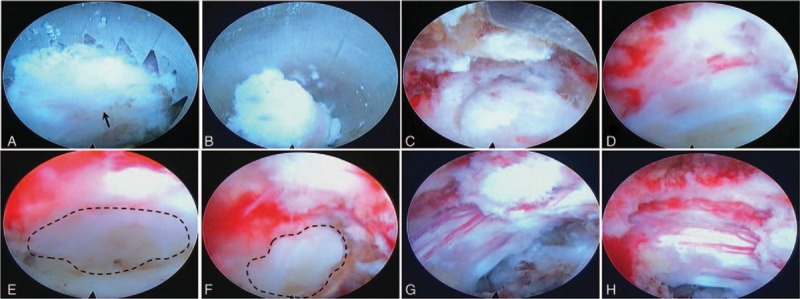 Figure 3. Intraoperation endoscopic views. After identifying the facet joint (A, arrow), the reamer was operated manually to remove the corresponding part of superior articular process (B). When… Source: Percutaneous endoscopic thoracic discectomy via posterolateral approach — Medicine 2019; CC BY.
Figure 3. Intraoperation endoscopic views. After identifying the facet joint (A, arrow), the reamer was operated manually to remove the corresponding part of superior articular process (B). When… Source: Percutaneous endoscopic thoracic discectomy via posterolateral approach — Medicine 2019; CC BY.
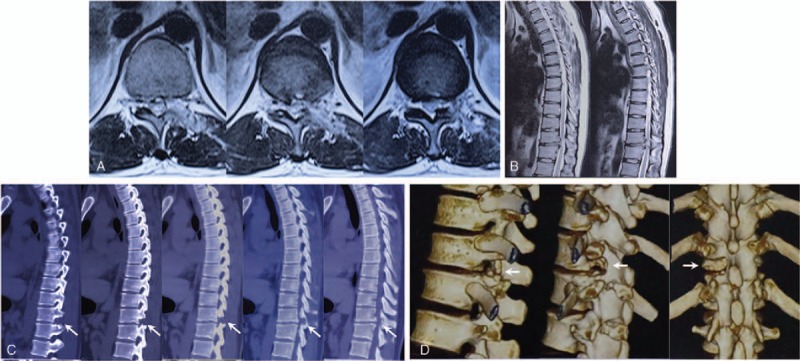 Figure 4. Post-operation imaging revealed satisfying decompression on T11–12. Magnetic resonance imaging demonstrated restored spinal canal and postoperative change of the disc and laminar (A and… Source: Percutaneous endoscopic thoracic discectomy via posterolateral approach — Medicine 2019; CC BY.
Figure 4. Post-operation imaging revealed satisfying decompression on T11–12. Magnetic resonance imaging demonstrated restored spinal canal and postoperative change of the disc and laminar (A and… Source: Percutaneous endoscopic thoracic discectomy via posterolateral approach — Medicine 2019; CC BY.
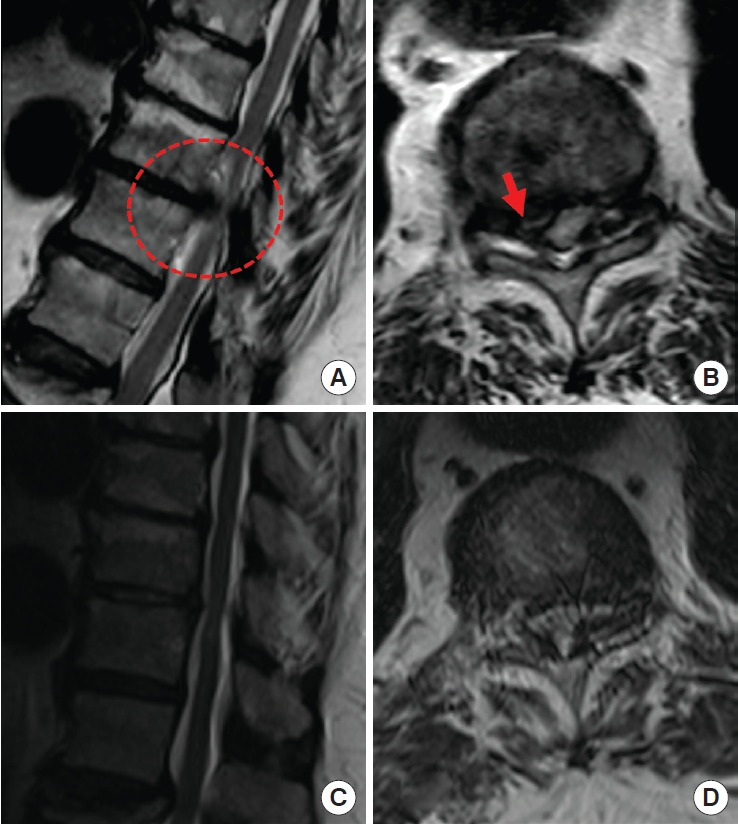 Fig. 1.. A 72-year-old female with thoracic myelopathy. (A, B) Preoperative magnetic resonance imaging show right paracentral disc extrusion with spinal cord compression (the circle and arrow)… Source: Uniportal, Transforaminal Endoscopic Thoracic Discectomy: Review and Technical Note — Neurospine 2023; CC BY-NC.
Fig. 1.. A 72-year-old female with thoracic myelopathy. (A, B) Preoperative magnetic resonance imaging show right paracentral disc extrusion with spinal cord compression (the circle and arrow)… Source: Uniportal, Transforaminal Endoscopic Thoracic Discectomy: Review and Technical Note — Neurospine 2023; CC BY-NC.
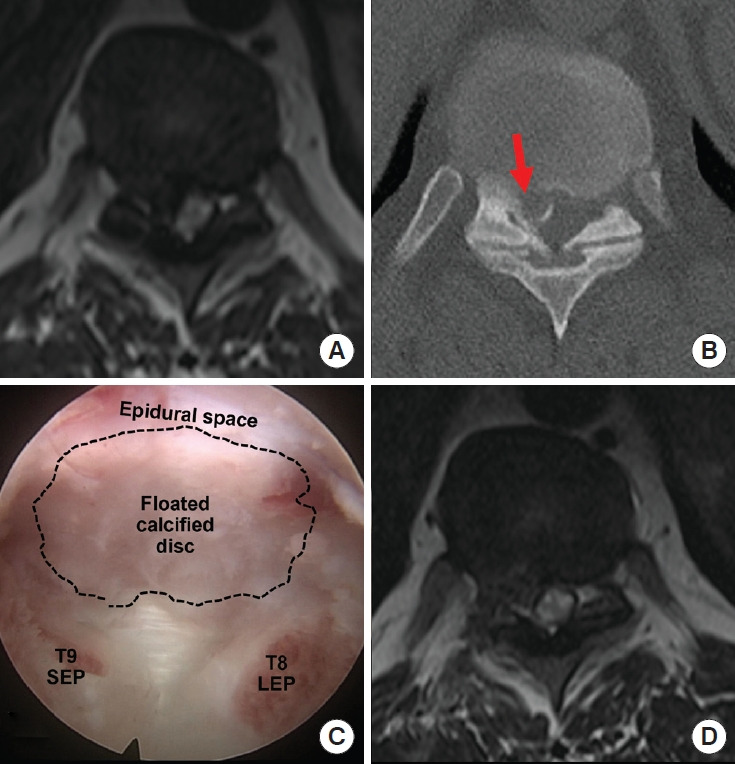 Fig. 2.. A 36-year-old female with thoracic myelopathy. The preoperative magnetic resonance imaging (MRI) (A) and computed tomography (B) show severe spinal cord compression and intramedullary… Source: Uniportal, Transforaminal Endoscopic Thoracic Discectomy: Review and Technical Note — Neurospine 2023; CC BY-NC.
Fig. 2.. A 36-year-old female with thoracic myelopathy. The preoperative magnetic resonance imaging (MRI) (A) and computed tomography (B) show severe spinal cord compression and intramedullary… Source: Uniportal, Transforaminal Endoscopic Thoracic Discectomy: Review and Technical Note — Neurospine 2023; CC BY-NC.
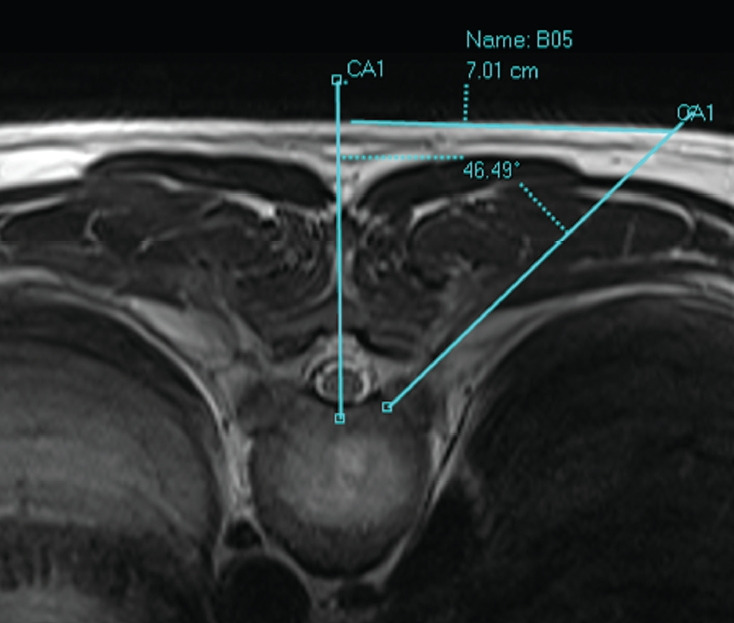 Fig. 3.. Axial magnetic resonance image demonstrates the location of portal (the entry of a discography needle) and access angle. The entry is located at around 5–8 cm from the midline, and the… Source: Uniportal, Transforaminal Endoscopic Thoracic Discectomy: Review and Technical Note — Neurospine 2023; CC BY-NC.
Fig. 3.. Axial magnetic resonance image demonstrates the location of portal (the entry of a discography needle) and access angle. The entry is located at around 5–8 cm from the midline, and the… Source: Uniportal, Transforaminal Endoscopic Thoracic Discectomy: Review and Technical Note — Neurospine 2023; CC BY-NC.
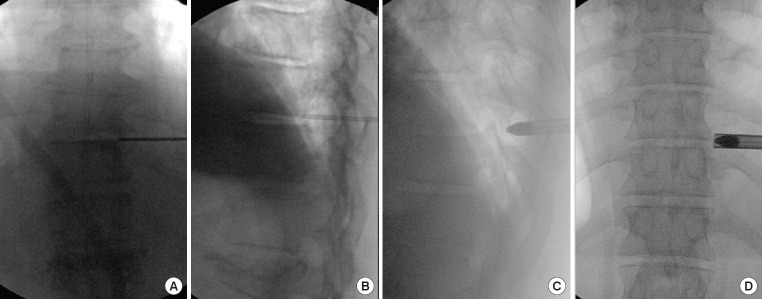 Fig. 4.. The initial discography needle and guide wide should touch the posterolateral corner of the intervertebral disc (A, B) on fluoroscopic images. (C, D) The obturator and working cannula is… Source: Uniportal, Transforaminal Endoscopic Thoracic Discectomy: Review and Technical Note — Neurospine 2023; CC BY-NC.
Fig. 4.. The initial discography needle and guide wide should touch the posterolateral corner of the intervertebral disc (A, B) on fluoroscopic images. (C, D) The obturator and working cannula is… Source: Uniportal, Transforaminal Endoscopic Thoracic Discectomy: Review and Technical Note — Neurospine 2023; CC BY-NC.
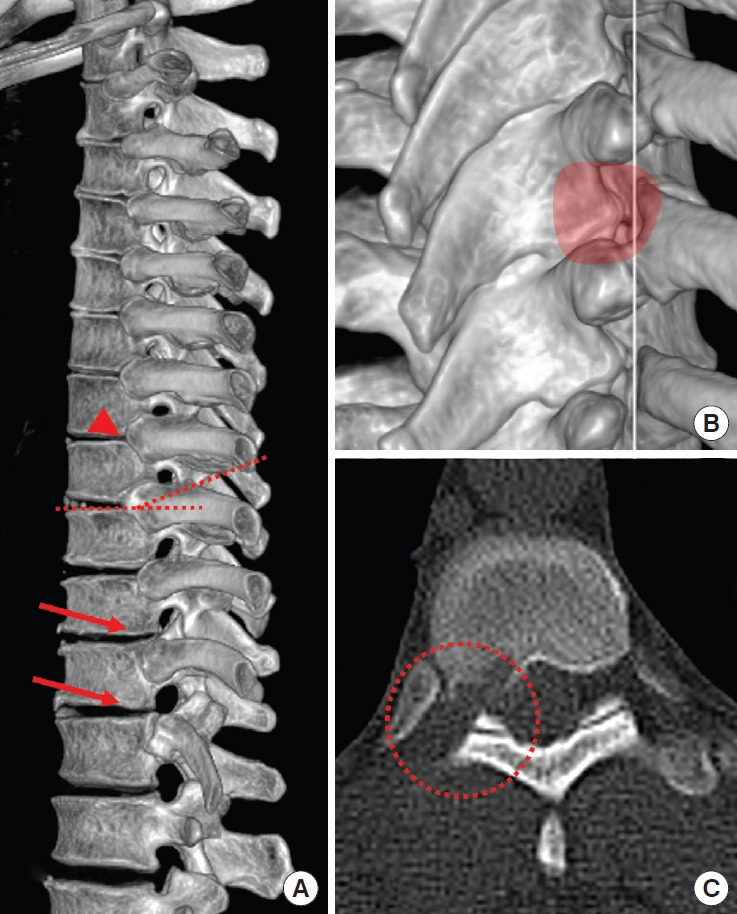 Fig. 5.. Computed tomography (CT) images demonstrate anatomical characteristics of the thoracic spine. (A) T10/11, T11/12 disc space is not covered by the corresponding rib heads (red arrows),… Source: Uniportal, Transforaminal Endoscopic Thoracic Discectomy: Review and Technical Note — Neurospine 2023; CC BY-NC.
Fig. 5.. Computed tomography (CT) images demonstrate anatomical characteristics of the thoracic spine. (A) T10/11, T11/12 disc space is not covered by the corresponding rib heads (red arrows),… Source: Uniportal, Transforaminal Endoscopic Thoracic Discectomy: Review and Technical Note — Neurospine 2023; CC BY-NC.
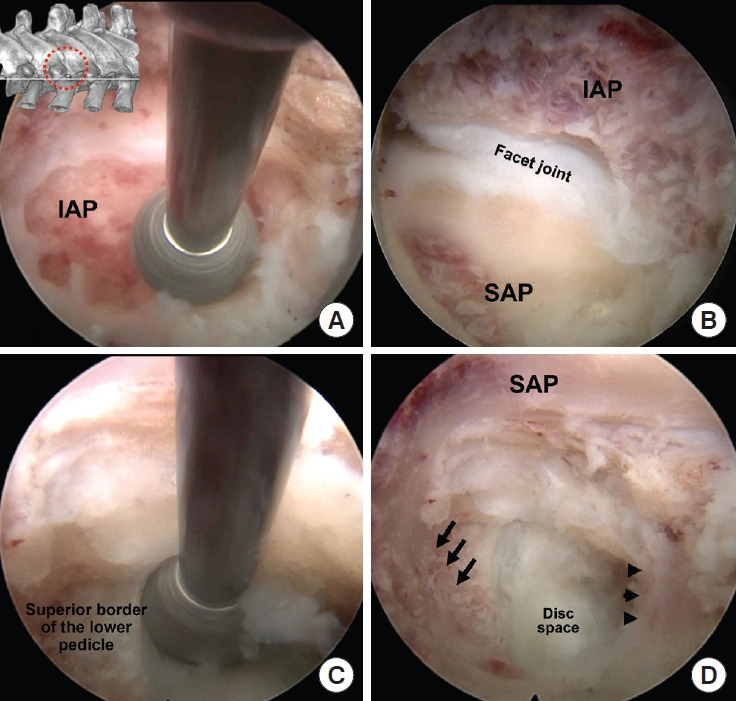 Fig. 6.. Intraoperative pictures of sequential steps showing exposure of a right side T9/10 intervertebral foramen and intervertebral disc space. (A) After soft tissue removal, lateral aspect of… Source: Uniportal, Transforaminal Endoscopic Thoracic Discectomy: Review and Technical Note — Neurospine 2023; CC BY-NC.
Fig. 6.. Intraoperative pictures of sequential steps showing exposure of a right side T9/10 intervertebral foramen and intervertebral disc space. (A) After soft tissue removal, lateral aspect of… Source: Uniportal, Transforaminal Endoscopic Thoracic Discectomy: Review and Technical Note — Neurospine 2023; CC BY-NC.
History of Present Illness
- Chief complaint: Myelopathy (gait, lower extremity weakness/numbness, bowel/bladder), band-like thoracic/radicular pain, sensory level
- Thoracic disc herniations are uncommon; calcified/central ones are dangerous (cord compression, narrow canal, tenuous blood supply)
- Failed conservative management; progressive myelopathy = surgical
- Calcified vs soft, central vs lateral (determines approach)
Past Medical History
- Pulmonary status (anterior/thoracoscopic approaches), prior thoracic surgery
- Standard PMH
Imaging Review
MRI Thoracic
- Disc level, central vs paracentral vs lateral, cord compression/signal change, canal compromise
CT / CT myelogram
- Calcification (calcified discs are adherent to dura — higher risk, may have intradural extension/dural defect), bony anatomy, rib/pedicle landmarks
- Level localization is notoriously difficult in the thoracic spine — count from C2 and sacrum, mark with reference (rib, fiducial), confirm intraop
X-ray (localization)
Labs
- CBC, BMP, Coags, type and crossmatch
Neurological Examination
- Lower extremity motor/sensory (sensory level), reflexes (hyperreflexia/Babinski — myelopathy), gait, sphincter, abdominal reflexes
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: radiolucent table configured for lateral or anterior thoracic exposure, with C-arm access and chest/vascular exposure needs coordinated before positioning.
- OR setup: radiolucent/Jackson table, fluoroscopy or O-arm/navigation, microscope/loupes for decompression, implant trays/graft ready for fusion, neuromonitoring for myelopathy/cord-risk cases, and postop brace plan confirmed.
- Special needs: arterial line/Foley/type-screen for long fusion/corpectomy, no long paralytic when MEPs are used, MAP/normotension for myelopathy or cord-risk cases, antibiotic redosing, and anticoagulation/DVT plan.
- Immediate postop orders: neuro checks by myotome/sensory level, airway/dysphagia watch for anterior cervical cases, CT/X-rays per construct, drain care, brace/activity orders, DVT prophylaxis timing, bowel regimen, and PT/OT mobilization.
Approach Selection (NEVER a standard posterior laminectomy for central disc — cord retraction is catastrophic)
- Transpedicular: posterolateral, for lateral/paracentral soft discs; remove pedicle for access
- Costotransversectomy: posterolateral, more ventral access (remove transverse process + rib head)
- Lateral extracavitary: wide posterolateral, good ventral access without thoracotomy
- Anterior transthoracic / thoracoscopic: best for central calcified discs (direct ventral access, no cord manipulation) — needs thoracic access/lung deflation
- Principle: access the disc from the side/front, decompress the cord WITHOUT retracting it
Position
- OR table/bed: radiolucent table configured for lateral or anterior thoracic exposure, with C-arm access and chest/vascular exposure needs coordinated before positioning.
- Posterolateral approaches: prone; Anterior/thoracoscopic: lateral decubitus (lung deflation, double-lumen tube)
- Mayfield/foam, IONM baseline
Key Surgical Steps (Transpedicular/Costotransversectomy example)
- Meticulous level localization (fluoroscopy, count from both ends, confirm rib/pedicle); wrong-level thoracic surgery is a notorious error
- Posterolateral exposure; remove facet/pedicle (± transverse process and rib head for costotransversectomy)
- Reach the disc space ventrolateral to the thecal sac
- Create a cavity in the vertebral body/disc space, then push the disc fragment AWAY from the cord into the cavity (down-and-away — never toward the cord)
- For calcified/transdural disc: work carefully; if dura is breached/adherent, may leave a calcified shell adherent to dura or repair the dural defect (CSF leak risk)
- Confirm cord decompression (thecal sac re-expands)
- ± Instrumented fusion (if significant bone/facet/pedicle removed or instability)
- Closure (chest tube if transthoracic/thoracoscopic)
Critical Anatomy & Structures at Risk
- Spinal cord — do NOT retract (thoracic cord watershed blood supply, low tolerance); work ventral, push fragment away
- Artery of Adamkiewicz / segmental arteries (T8-L1, usually left) — cord infarction
- Dura (calcified disc adherence — CSF leak, intradural fragment)
- Pleura/lung (anterior/lateral), thoracic duct, great vessels (anterior)
- Nerve roots (sacrificable in thoracic for access if needed)
Equipment
- Microscope, high-speed drill, navigation/fluoroscopy
- Down-pushing curettes/instruments, Kerrison, fusion instrumentation
- Thoracoscopic set / thoracic access (anterior), chest tube, dural repair materials
Monitoring
- SSEPs, MEPs (essential — cord at high risk), EMG
Anesthesia
- Double-lumen tube/lung isolation (anterior/thoracoscopic), MAP support, arterial line, no paralytic (IONM), crossmatched blood
Potential Complications
- Spinal cord injury/infarction (retraction, vascular) — paraplegia
- Wrong-level surgery (localization)
- CSF leak (calcified transdural disc), pleural injury/effusion/pneumothorax
- Instability (if extensive bone removal), pulmonary complications, incomplete decompression
Operative Note Template
Preoperative Diagnosis: [T_-T_] thoracic disc herniation ([central/calcified]) with [myelopathy/radiculopathy]
Postoperative Diagnosis: Same
Procedure: [Transpedicular / costotransversectomy / lateral extracavitary / transthoracic / thoracoscopic] thoracic discectomy at [T_-T_] [with instrumented fusion]
Surgeon / Assistant: Anesthesia: General endotracheal [double-lumen tube for anterior/thoracoscopic] EBL / Fluids / Blood products: [crossmatched] Adjuncts: Fluoroscopy/navigation, microscope, high-speed drill; SSEP/MEP; MAP support Implants: [Fusion hardware if used]; [chest tube if transthoracic] Complications: None
Indications: [Age]yo [M/F] with a [central/calcified] thoracic disc at [T_-T_] causing [myelopathy/band pain], where ventral decompression without cord retraction is required. Risks (cord injury, wrong-level, CSF leak, pleural injury) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and neuromonitoring established. Meticulous fluoroscopic level localization was performed (counting from both ends). The patient was positioned [prone for posterolateral / lateral decubitus with lung deflation for anterior]. A [transpedicular/costotransversectomy/transthoracic] corridor was developed to reach the disc ventrolateral to the cord.
A cavity was created in the disc/body and the disc fragment was pushed away from the cord into the cavity (down-and-away — no cord retraction); [the calcified/transdural component was carefully addressed, with dural repair as needed]. Cord decompression was confirmed (thecal sac re-expanded). [Instrumented fusion was performed for the bone removed.] Neuromonitoring remained stable.
[A chest tube was placed for the transthoracic approach.] Closure was performed in layers. The patient was transferred with serial neuro exams [and CXR/chest-tube management].
Postoperative Plan
- ICU/step-down, neuro checks q1h (lower extremity, sensory level, sphincter), MAP support
- Chest X-ray / chest tube management (anterior/thoracoscopic — pneumothorax/effusion)
- CSF leak precautions (if dural breach), MRI/CT postop
- DVT prophylaxis (mechanical), pulmonary toilet, pain control
- Follow-up imaging; rehab
Chief-Level Case Review
Use these as the senior-level mental model for Thoracic Discectomy (Transpedicular / Costotransversectomy / Lateral Extracavitary / Thoracoscopic):
- Decision point: Localize twice and instrument once: numbering, transitional anatomy, prior hardware, rib count, navigation dataset, and fluoroscopic level confirmation are mandatory.
- Technical lever: Positioning is treatment: table choice, abdomen-free prone setup, alignment goals, shoulders/hips, eyes/plexus pressure, neuromonitoring baselines, and fluoroscopic access all change the case.
- Bailout: Protect neural elements by sequence: decompression before correction when needed, MAP support for cord risk, no long paralytic with MEPs, and immediate response to signal change.
- Postop watch: Finish with construct logic: decompression adequacy, screw purchase, alignment, fusion bed/graft, drain plan, brace/activity orders, postop CT/X-rays, and DVT timing.
Common Pimp Questions
Use these to pressure-test preparation for Thoracic Discectomy (Transpedicular / Costotransversectomy / Lateral Extracavitary / Thoracoscopic):
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]