
Case Prep: Sacroiliac (SI) Joint Fusion
Case / Approach Snapshot
- Anatomy at risk: level localization, cord/cauda equina, exiting and traversing roots, dura, vertebral artery or segmental vessels, esophagus/trachea/pleura/viscera by approach, and fusion/instrumentation landmarks.
- Operative steps: position and pad carefully, confirm level, expose the planned corridor, decompress neural elements, reconstruct or instrument when indicated, verify alignment/hardware, and close with attention to hematoma and wound risk; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: wrong level, durotomy, neurologic change, vertebral artery/visceral/pleural injury, graft or hardware problem, epidural hematoma, dysphagia/airway issue, and infection prevention/escalation.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with sacroiliac joint dysfunction (SI joint pain) refractory to conservative management planned for minimally invasive [lateral transiliac] SI joint fusion.
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Sacroiliac Joint Interventions — Yang AJ. Physical medicine and rehabilitation clinics of North America 2022. PubMed
- Sacroiliac Joint Anatomy — Roberts SL. Physical medicine and rehabilitation clinics of North America 2021. PubMed
- Sacroiliac joint dysfunction: anatomy, pathophysiology, differential diagnosis, and treatment approaches — Waldman LE. Skeletal radiology 2025. PubMed
- Sacroiliac Joint Interventions — Soto Quijano DA. Physical medicine and rehabilitation clinics of North America 2018. PubMed
- The sacroiliac joint: an overview of its anatomy, function and potential clinical implications — Vleeming A. Journal of anatomy 2012. PubMed
- Sacroiliac Joint: Mimics and Pitfalls — Lowry MKJ. Seminars in musculoskeletal radiology 2025. PubMed
- Sacroiliac joint pain — Dreyfuss P. The Journal of the American Academy of Orthopaedic Surgeons 2004. PubMed
- The Sacroiliac Joint — Polly DW Jr. Neurosurgery clinics of North America 2017. PubMed
- Sacroiliac Joint Diagnostic Block and Radiofrequency Ablation Techniques — Loh E. Physical medicine and rehabilitation clinics of North America 2021. PubMed
- The Sacroiliac Joint: A Current State-of-the-Art Review — Polly DW Jr. JBJS reviews 2024. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
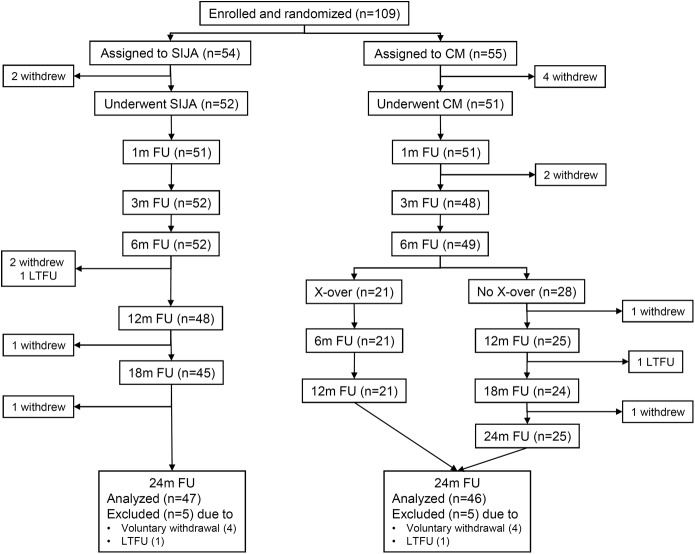 Fig. 1. Patient flow. SIJA = sacroiliac joint arthrodesis, CM = conservative management, FU = follow-up, m = month, X-over = crossover, and LTFU = lost to FU. Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
Fig. 1. Patient flow. SIJA = sacroiliac joint arthrodesis, CM = conservative management, FU = follow-up, m = month, X-over = crossover, and LTFU = lost to FU. Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
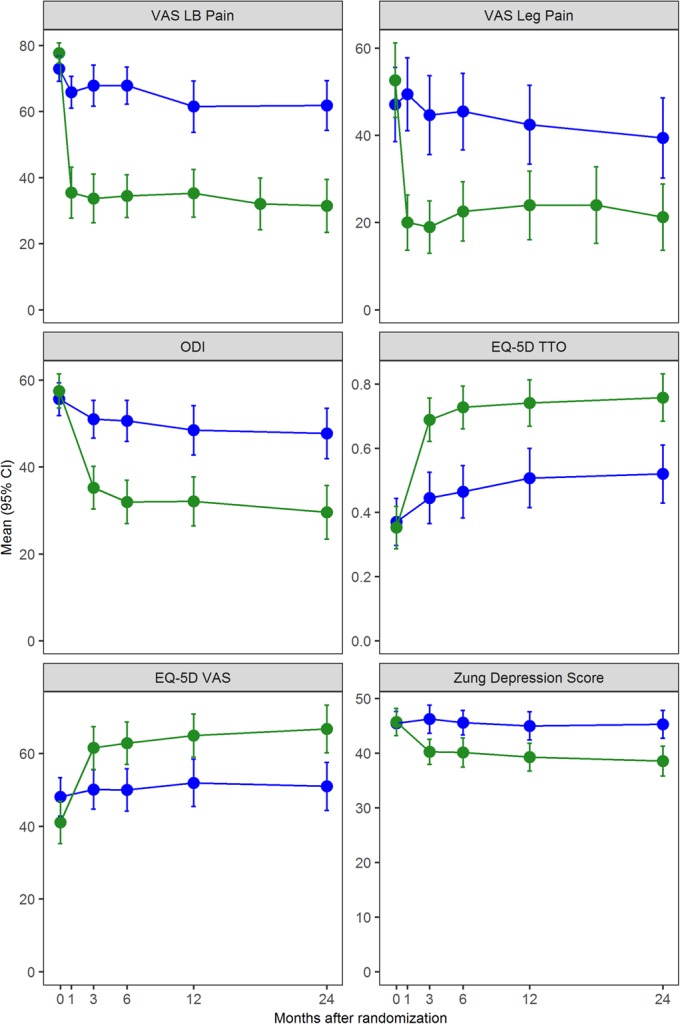 Fig. 2. Change in VAS low back (LB) pain, VAS leg pain, ODI, EQ-5D time trade-off (TTO), EQ-5D VAS, and Zung Depression Scale scores. Blue indicates the conservative management group, and green… Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
Fig. 2. Change in VAS low back (LB) pain, VAS leg pain, ODI, EQ-5D time trade-off (TTO), EQ-5D VAS, and Zung Depression Scale scores. Blue indicates the conservative management group, and green… Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
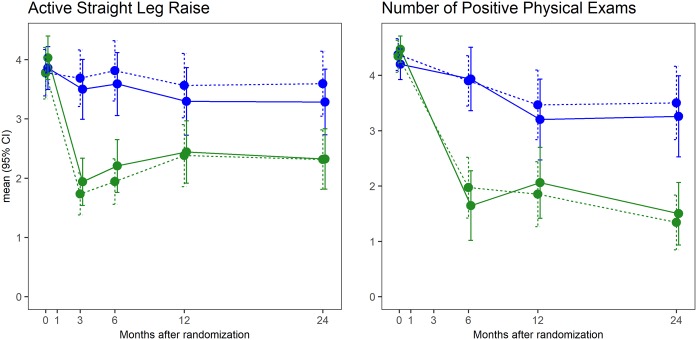 Fig. 3. Change in functional test (active straight leg raise test) by treatment and time (left) and the number of positive physical examination signs (right). Blue indicates the conservative… Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
Fig. 3. Change in functional test (active straight leg raise test) by treatment and time (left) and the number of positive physical examination signs (right). Blue indicates the conservative… Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
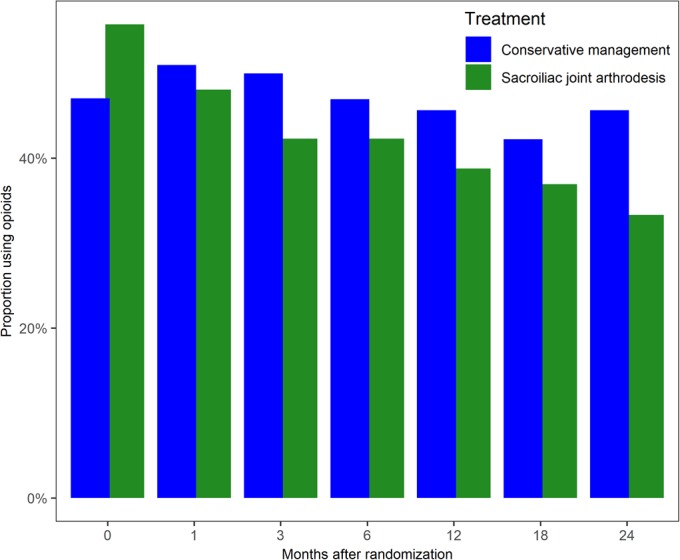 Fig. 4. Proportion of subjects reporting opioid use in the past 2 weeks by treatment and study visit. Blue indicates the conservative management (CM) group, and green indicates the sacroiliac… Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
Fig. 4. Proportion of subjects reporting opioid use in the past 2 weeks by treatment and study visit. Blue indicates the conservative management (CM) group, and green indicates the sacroiliac… Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
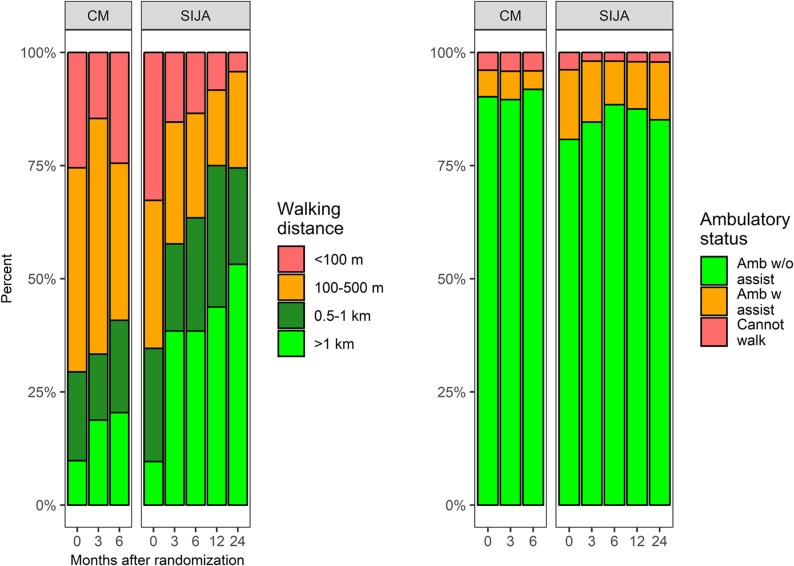 Fig. 5-A. Change in walking distance and ambulatory status. Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
Fig. 5-A. Change in walking distance and ambulatory status. Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
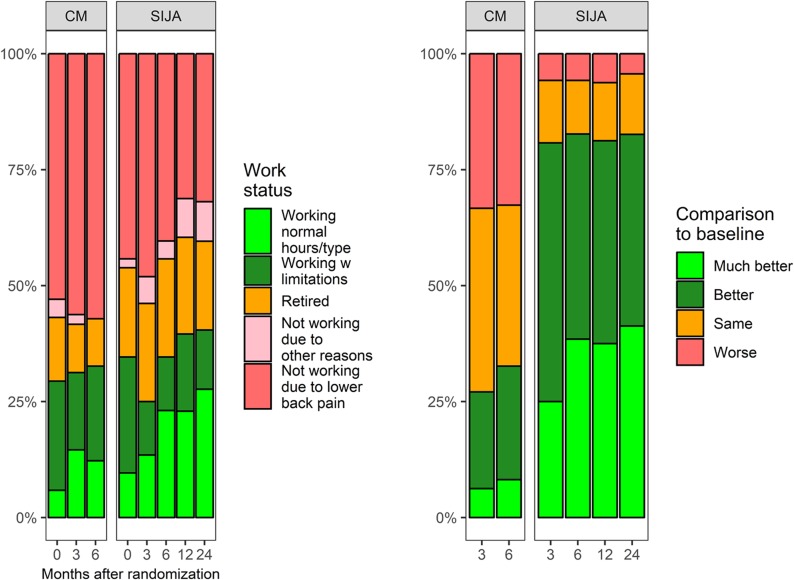 Fig. 5-B. Change in work status and comparison with baseline. Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
Fig. 5-B. Change in work status and comparison with baseline. Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
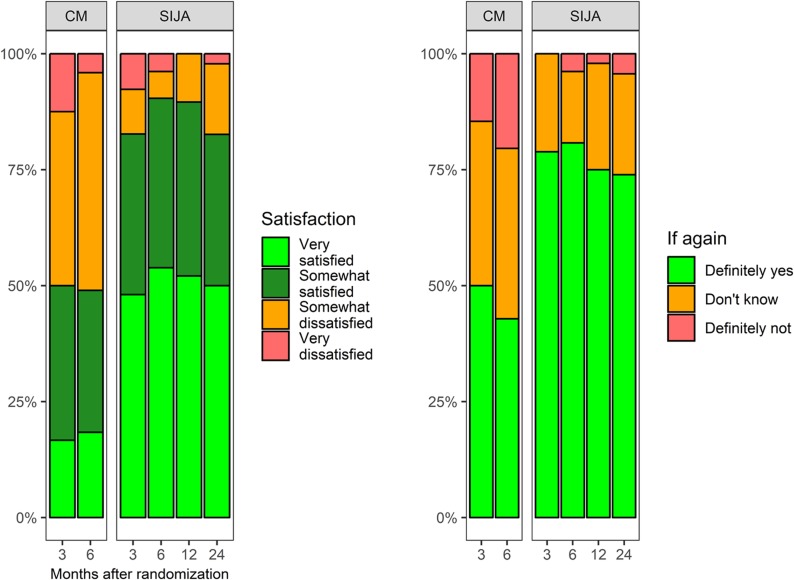 Fig. 5-C. Change in satisfaction and desirability of having a surgical procedure again by treatment and follow-up visit. Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
Fig. 5-C. Change in satisfaction and desirability of having a surgical procedure again by treatment and follow-up visit. Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
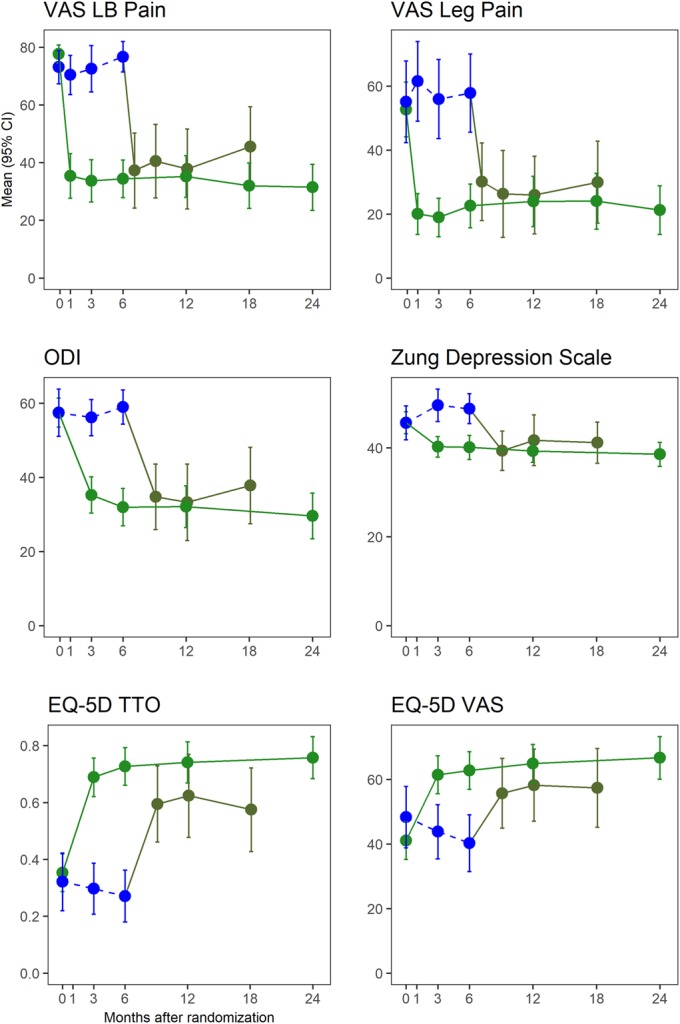 Fig. 6. Change in VAS low back (LB) pain, VAS leg pain, ODI, Zung Depression Scale, EQ-5D time trade-off (TTO), and EQ-5D VAS scores including subjects who crossed over from conservative… Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
Fig. 6. Change in VAS low back (LB) pain, VAS leg pain, ODI, Zung Depression Scale, EQ-5D time trade-off (TTO), and EQ-5D VAS scores including subjects who crossed over from conservative… Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
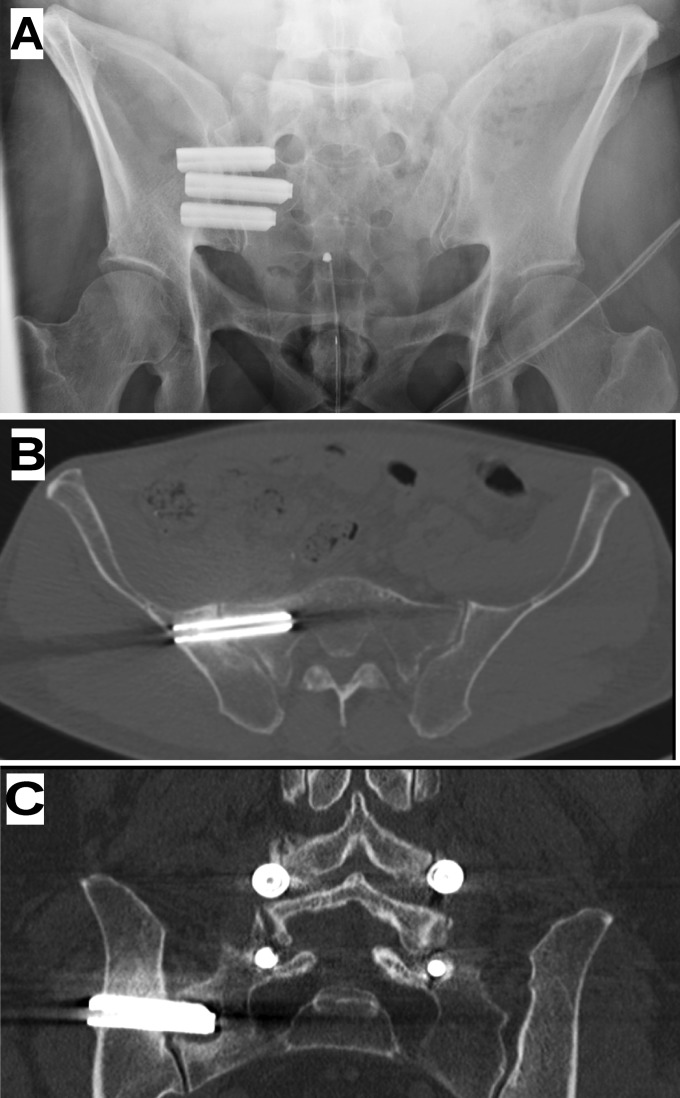 Fig. 7. Imaging of typical configuration of implants. Fig. 7-A Inlet-view pelvic radiograph. Fig. 7-B A 12-month CT image from a different subject showing no radiolucencies around the first… Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
Fig. 7. Imaging of typical configuration of implants. Fig. 7-A Inlet-view pelvic radiograph. Fig. 7-B A 12-month CT image from a different subject showing no radiolucencies around the first… Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
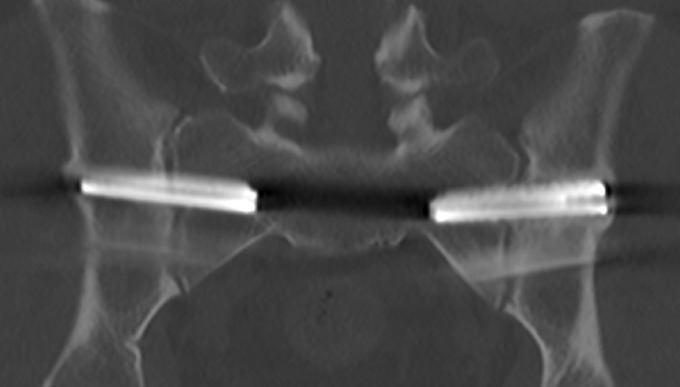 Fig. 8. A 12-month CT image depicting bilateral implants with bone apposition along the entire length of the superior and inferior sides of both implants. Also, there is bone overgrowth at the… Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
Fig. 8. A 12-month CT image depicting bilateral implants with bone apposition along the entire length of the superior and inferior sides of both implants. Also, there is bone overgrowth at the… Source: Randomized Trial of Sacroiliac Joint Arthrodesis Compared with Conservative Management for Chronic Low Back Pain Attributed to the Sacroiliac Joint — The Journal of Bone and Joint Surgery. American Volume 2019; CC BY-NC-ND.
History of Present Illness
- Chief complaint: Unilateral low back/buttock pain below L5, often radiating to posterior thigh/groin, worse with sitting-to-standing, stairs, single-leg loading
- Fortin finger sign (points to PSIS), pain over the SI joint
- Failed conservative management (PT, NSAIDs, SI joint injections)
- Etiology: degenerative, post-lumbar fusion (adjacent SI stress), post-partum, trauma
Past Medical History
- Prior lumbar fusion (accelerates SI degeneration), inflammatory arthropathy (sacroiliitis — different management), prior pelvic trauma
- Standard PMH
Imaging Review
Diagnostic Workup (key — confirm the SI joint is the pain source)
- Image-guided SI joint anesthetic injection(s) providing significant temporary relief (>50-75%) — strongly supports diagnosis and surgical candidacy
- Physical exam provocative tests (≥3 positive: thigh thrust, FABER, distraction, compression, Gaenslen)
CT / X-ray
- SI joint degeneration, anatomy for implant trajectory, exclude other pathology, sacral dysmorphism
MRI lumbar
- Exclude lumbar source (rule out concurrent stenosis/radiculopathy mimicking)
Labs
- CBC, BMP, Coags, type and screen
Neurological Examination
- Lower extremity exam (typically normal — distinguishes from radiculopathy), SI provocative tests, gait
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- OR setup: radiolucent/Jackson table, fluoroscopy or O-arm/navigation, microscope/loupes for decompression, implant trays/graft ready for fusion, neuromonitoring for myelopathy/cord-risk cases, and postop brace plan confirmed.
- Special needs: arterial line/Foley/type-screen for long fusion/corpectomy, no long paralytic when MEPs are used, MAP/normotension for myelopathy or cord-risk cases, antibiotic redosing, and anticoagulation/DVT plan.
- Immediate postop orders: neuro checks by myotome/sensory level, airway/dysphagia watch for anterior cervical cases, CT/X-rays per construct, drain care, brace/activity orders, DVT prophylaxis timing, bowel regimen, and PT/OT mobilization.
Diagnosis & Indication
- Indication: SI joint pain confirmed by exam + diagnostic injection relief, refractory to ≥6 months conservative care
- Goals: fuse/stabilize the SI joint with implants placed across the joint
Position
- OR table/bed: Jackson/Allen/open-frame radiolucent table, or ProAxis/hinged table when sagittal alignment adjustment is useful; keep abdomen free for venous decompression.
- Lateral or prone (per system), fluoroscopy (inlet/outlet/lateral pelvis), padded
Key Surgical Steps (MIS Lateral Transiliac)
- Fluoroscopic localization (true lateral, inlet, outlet pelvic views)
- Small lateral buttock incision over the ilium
- Guide pin across the ilium, through the SI joint, into the sacrum under fluoroscopy — stay within bone, avoid the sacral foramina/canal and the sciatic notch; confirm trajectory on all views
- Sequential drilling/broaching across the joint
- Place implants (triangular titanium rods / screws / threaded implants) across the SI joint (typically 2-3) for stabilization/fusion
- Confirm implant position on inlet/outlet/lateral fluoroscopy (within sacral bone, not in foramina/canal)
- Closure
Critical Anatomy & Structures at Risk
- Sacral nerve roots (S1, S2) in the foramina — implant too anterior/medial breaches foramen
- L5 nerve root (anterior to sacral ala)
- Sacral canal / cauda (too medial), sciatic notch / superior gluteal vessels (too inferior/posterior)
- SI joint, iliac vessels (anterior breach)
Equipment
- SI fusion implant system (triangular implants/screws + instruments), fluoroscopy (essential) ± navigation/robotics
- Neuromonitoring (selected)
Monitoring
- Triggered EMG (selected — confirm implants not breaching foramina)
Anesthesia
- General; fluoroscopy; standard
Potential Complications
- Sacral nerve root injury (foraminal breach), L5 injury
- Implant malposition, vascular injury (notch/anterior breach)
- Nonunion/persistent pain (patient selection critical), implant loosening
- Wound issues, nerve irritation
Operative Note Template
Preoperative Diagnosis: [Right/Left] sacroiliac joint dysfunction (confirmed by diagnostic injection), refractory to conservative care
Postoperative Diagnosis: Same
Procedure: Minimally invasive [right/left] sacroiliac joint fusion with [N] [triangular titanium] implants
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Fluoroscopy (inlet/outlet/lateral) [± navigation]; [triggered EMG] Implants: [N] SI fusion implants [triangular titanium] Complications: None
Indications: [Age]yo [M/F] with SI joint pain confirmed by exam and >[50–75]% relief from image-guided SI injection, refractory to ≥6 months of conservative care. Risks (sacral nerve injury, malposition) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and the patient positioned [lateral/prone] with fluoroscopy. True lateral, inlet, and outlet pelvic views were obtained. A small lateral buttock incision was made over the ilium, and a guide pin advanced across the ilium, through the SI joint, into the sacrum — staying within bone and avoiding the sacral foramina, canal, and sciatic notch, confirmed on all views.
The trajectory was drilled/broached and [N] implants placed across the joint for stabilization/fusion. Final inlet/outlet/lateral fluoroscopy confirmed the implants were within sacral bone and clear of the foramina/canal. [Triggered EMG confirmed no foraminal breach.]
Closure was performed. The patient was discharged [same day] with protected weight-bearing on the operative side.
Postoperative Plan
- Outpatient/short stay, neuro checks (sacral roots)
- Protected weight-bearing per surgeon (often partial on operative side x weeks)
- X-ray/CT postop (implant position), pain assessment
- Activity progression, PT; follow-up for fusion
- Counsel: outcomes depend on correct patient selection (confirmed SI source)
Chief-Level Case Review
Use these as the senior-level mental model for Sacroiliac (SI) Joint Fusion:
- Decision point: Localize twice and instrument once: numbering, transitional anatomy, prior hardware, rib count, navigation dataset, and fluoroscopic level confirmation are mandatory.
- Technical lever: Positioning is treatment: table choice, abdomen-free prone setup, alignment goals, shoulders/hips, eyes/plexus pressure, neuromonitoring baselines, and fluoroscopic access all change the case.
- Bailout: Protect neural elements by sequence: decompression before correction when needed, MAP support for cord risk, no long paralytic with MEPs, and immediate response to signal change.
- Postop watch: Finish with construct logic: decompression adequacy, screw purchase, alignment, fusion bed/graft, drain plan, brace/activity orders, postop CT/X-rays, and DVT timing.
Common Pimp Questions
Use these to pressure-test preparation for Sacroiliac (SI) Joint Fusion:
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]