
Case Prep: Cervical Disc Arthroplasty (Cervical Disc Replacement)
Case / Approach Snapshot
- Anatomy at risk: level localization, cord/cauda equina, exiting and traversing roots, dura, vertebral artery or segmental vessels, esophagus/trachea/pleura/viscera by approach, and fusion/instrumentation landmarks.
- Operative steps: position and pad carefully, confirm level, expose the planned corridor, decompress neural elements, reconstruct or instrument when indicated, verify alignment/hardware, and close with attention to hematoma and wound risk; use the detailed operative sequence and approach notes below as the step-by-step source.
- Rescue plans: wrong level, durotomy, neurologic change, vertebral artery/visceral/pleural injury, graft or hardware problem, epidural hematoma, dysphagia/airway issue, and infection prevention/escalation.
- Figures: review Figures, Imaging & Video and the Curated Image Set; embedded local figures should remain open-access, public-domain, or otherwise reusable with attribution.
- Papers: review High-Yield Literature for seminal sources, modern reviews, and outcome data specific to this page.
One-Liner
[Age]yo [M/F] with [single/two]-level cervical [radiculopathy/myelopathy] at [C_-C_] due to soft disc herniation planned for cervical total disc arthroplasty (motion-preserving).
Figures, Imaging & Video
🎥 Operative video — search operative video on YouTube ▸ · The Neurosurgical Atlas ▸
🧭 Operative approach: Anterior cervical (Smith-Robinson) approach — detailed corridor setup, step-by-step technique & figures
Neurosurgical Atlas · AO Spine / Surgery Reference · Radiopaedia · PubMed Central — operative figures © linked; see media-sources.md
High-Yield Literature
- Cervical disc arthroplasty: tips and tricks — Makhni MC. International orthopaedics 2019. PubMed
- Cervical disc arthroplasty — Zindrick M. The Journal of the American Academy of Orthopaedic Surgeons 2010. PubMed
- Osteolysis after cervical disc arthroplasty — Joaquim AF. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society 2020. PubMed
- Revision Strategies for Cervical Disc Arthroplasty — Roth SG. Clinical spine surgery 2023. PubMed
- The Role of Cervical Disc Arthroplasty in Elite Athletes — Brecount H. Current reviews in musculoskeletal medicine 2023. PubMed
- Cervical disc arthroplasty: What we know in 2020 and a literature review — Shin JJ. Journal of orthopaedic surgery (Hong Kong) 2021. PubMed
- Biomechanics of Cervical Disc Arthroplasty Devices — Patwardhan AG. Neurosurgery clinics of North America 2021. PubMed
- Multilevel cervical disc arthroplasty: a review of optimal surgical management and future directions — Tu TH. Journal of neurosurgery. Spine 2023. PubMed
- Four-Level Cervical Disc Arthroplasty — Chang HK. International journal of spine surgery 2024. PubMed
- Cervical disc arthroplasty: general introduction — Acosta FL Jr. Neurosurgery clinics of North America 2005. PubMed
Curated Image Set
Open-access figures are embedded from PubMed Central articles and kept unique to this guide.
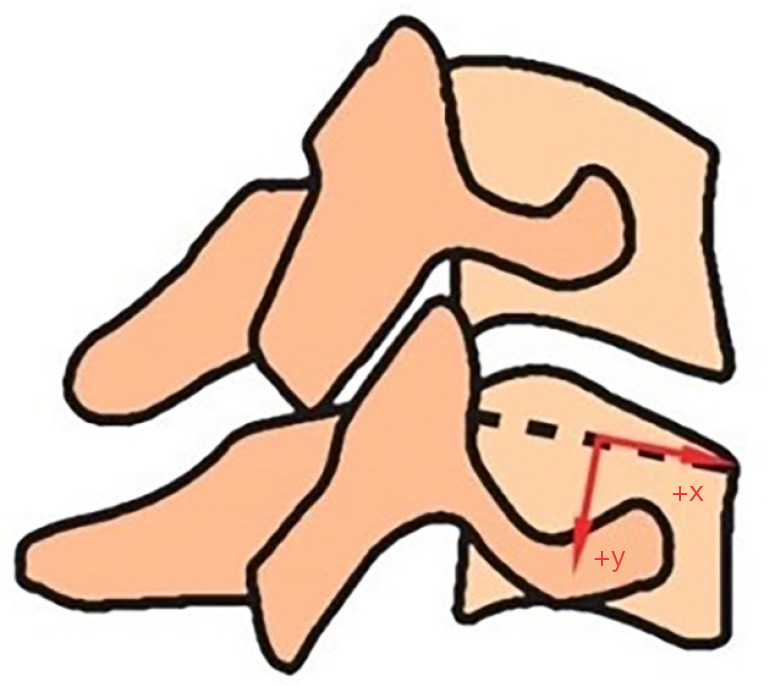 Figure 1. Centre of rotation. Source: Assessing in vivo flexion-extension quality of motion after cervical disc arthroplasty: a pilot study — Journal of Spine Surgery 2023; CC BY-NC-ND.
Figure 1. Centre of rotation. Source: Assessing in vivo flexion-extension quality of motion after cervical disc arthroplasty: a pilot study — Journal of Spine Surgery 2023; CC BY-NC-ND.
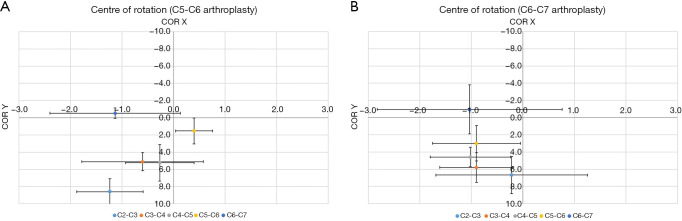 Figure 2. Centre of rotation in (A) C5-C6 and (B) C6-C7 arthroplasty group. (0,0) denotes the centre of superior endplate of caudal vertebra. COR, centre of rotation. Source: Assessing in vivo flexion-extension quality of motion after cervical disc arthroplasty: a pilot study — Journal of Spine Surgery 2023; CC BY-NC-ND.
Figure 2. Centre of rotation in (A) C5-C6 and (B) C6-C7 arthroplasty group. (0,0) denotes the centre of superior endplate of caudal vertebra. COR, centre of rotation. Source: Assessing in vivo flexion-extension quality of motion after cervical disc arthroplasty: a pilot study — Journal of Spine Surgery 2023; CC BY-NC-ND.
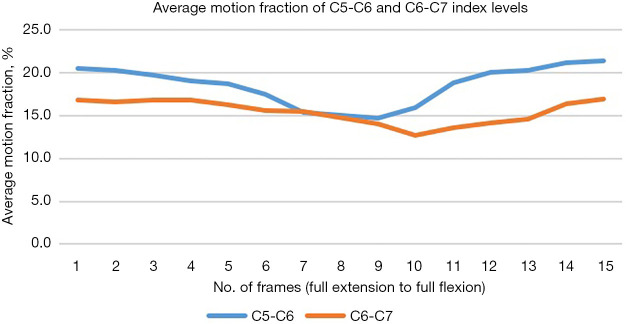 Figure 3. Average motion fraction throughout the arc of flexion-extension. Source: Assessing in vivo flexion-extension quality of motion after cervical disc arthroplasty: a pilot study — Journal of Spine Surgery 2023; CC BY-NC-ND.
Figure 3. Average motion fraction throughout the arc of flexion-extension. Source: Assessing in vivo flexion-extension quality of motion after cervical disc arthroplasty: a pilot study — Journal of Spine Surgery 2023; CC BY-NC-ND.
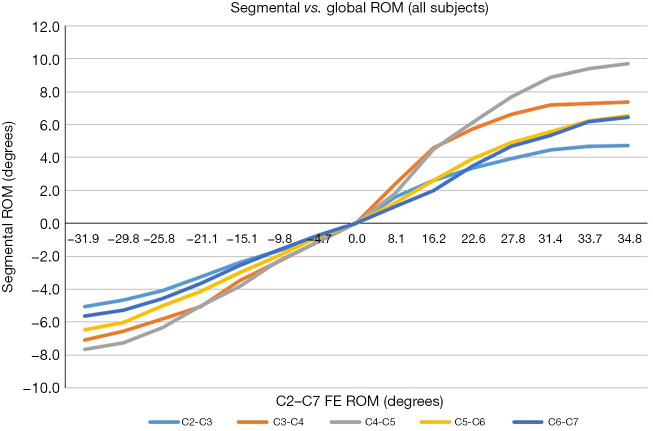 Figure 4. Segmental motion versus global range of motion. FE, flexion-extension; ROM, range of motion. Source: Assessing in vivo flexion-extension quality of motion after cervical disc arthroplasty: a pilot study — Journal of Spine Surgery 2023; CC BY-NC-ND.
Figure 4. Segmental motion versus global range of motion. FE, flexion-extension; ROM, range of motion. Source: Assessing in vivo flexion-extension quality of motion after cervical disc arthroplasty: a pilot study — Journal of Spine Surgery 2023; CC BY-NC-ND.
 Fig. 1. Anteroposterior (A) and lateral (B) preoperative radiographs demonstrating spondylosis and anterior osteophyte formation at C5–C6. Source: Traumatic Migration of the Bryan Cervical Disc Arthroplasty — Global Spine Journal 2015; open access.
Fig. 1. Anteroposterior (A) and lateral (B) preoperative radiographs demonstrating spondylosis and anterior osteophyte formation at C5–C6. Source: Traumatic Migration of the Bryan Cervical Disc Arthroplasty — Global Spine Journal 2015; open access.
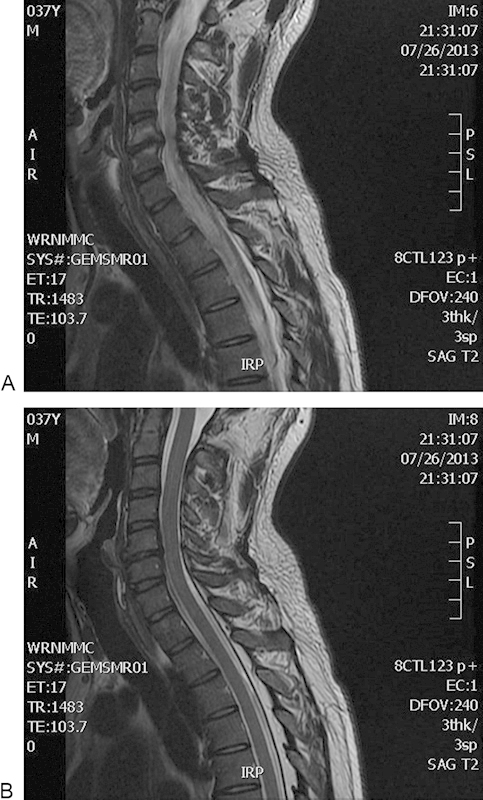 Fig. 2. Sequential sagittal magnetic resonance image slices (A, B) demonstrating disk–osteophyte complex resulting in moderate central canal narrowing with moderate left and mild right neural… Source: Traumatic Migration of the Bryan Cervical Disc Arthroplasty — Global Spine Journal 2015; open access.
Fig. 2. Sequential sagittal magnetic resonance image slices (A, B) demonstrating disk–osteophyte complex resulting in moderate central canal narrowing with moderate left and mild right neural… Source: Traumatic Migration of the Bryan Cervical Disc Arthroplasty — Global Spine Journal 2015; open access.
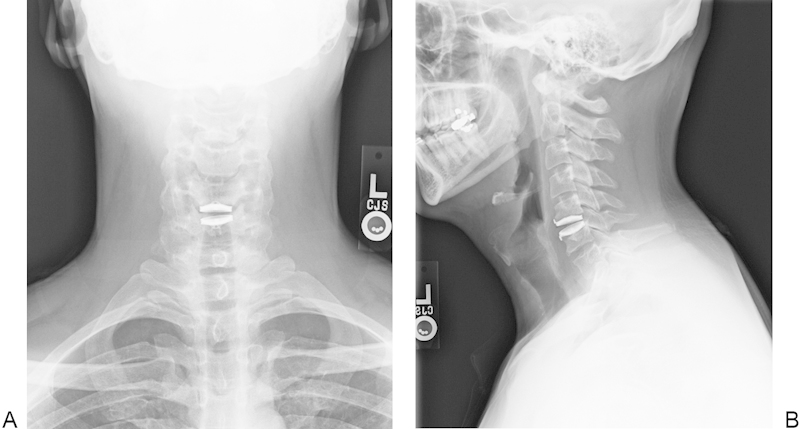 Fig. 3. Anteroposterior (A) and lateral (B) immediate postoperative radiographs demonstrating well-positioned and appropriately sized single-level Bryan Cervical Disc arthroplasty device at C5-C6. Source: Traumatic Migration of the Bryan Cervical Disc Arthroplasty — Global Spine Journal 2015; open access.
Fig. 3. Anteroposterior (A) and lateral (B) immediate postoperative radiographs demonstrating well-positioned and appropriately sized single-level Bryan Cervical Disc arthroplasty device at C5-C6. Source: Traumatic Migration of the Bryan Cervical Disc Arthroplasty — Global Spine Journal 2015; open access.
 Fig. 4. Lateral (A), flexion (B), and extension (C) radiographs at 6 weeks postoperatively demonstrating no change in the location or placement of the device, without evidence of migration or… Source: Traumatic Migration of the Bryan Cervical Disc Arthroplasty — Global Spine Journal 2015; open access.
Fig. 4. Lateral (A), flexion (B), and extension (C) radiographs at 6 weeks postoperatively demonstrating no change in the location or placement of the device, without evidence of migration or… Source: Traumatic Migration of the Bryan Cervical Disc Arthroplasty — Global Spine Journal 2015; open access.
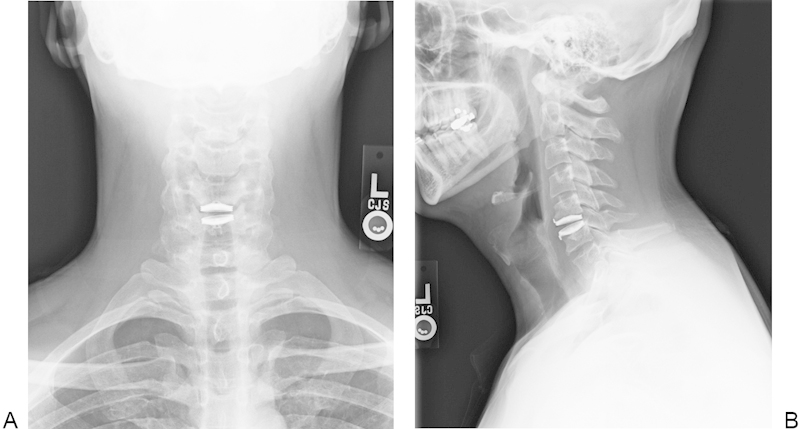 Fig. 5. Anteroposterior (A) and lateral (B) radiographs at 3 months postoperation demonstrating no change in position of the implant. Source: Traumatic Migration of the Bryan Cervical Disc Arthroplasty — Global Spine Journal 2015; open access.
Fig. 5. Anteroposterior (A) and lateral (B) radiographs at 3 months postoperation demonstrating no change in position of the implant. Source: Traumatic Migration of the Bryan Cervical Disc Arthroplasty — Global Spine Journal 2015; open access.
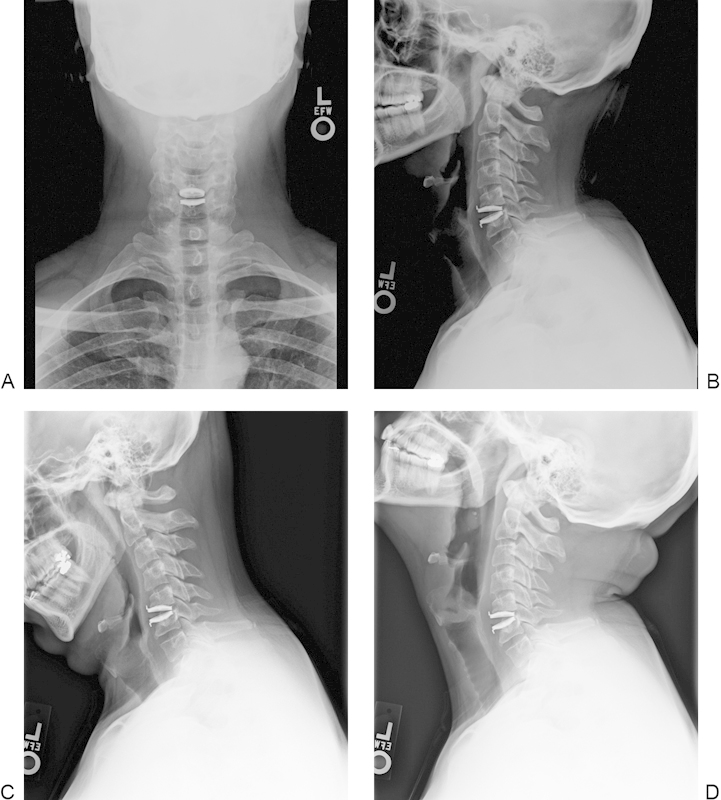 Fig. 6. Anteroposterior (A), lateral (B), flexion (C), and extension (D) radiographs at 6 months postoperatively showing migration of the Bryan Cervical Disc device ∼2 mm anteriorly, without… Source: Traumatic Migration of the Bryan Cervical Disc Arthroplasty — Global Spine Journal 2015; open access.
Fig. 6. Anteroposterior (A), lateral (B), flexion (C), and extension (D) radiographs at 6 months postoperatively showing migration of the Bryan Cervical Disc device ∼2 mm anteriorly, without… Source: Traumatic Migration of the Bryan Cervical Disc Arthroplasty — Global Spine Journal 2015; open access.
History of Present Illness
- Chief complaint: Radiculopathy / myelopathy from soft disc herniation/spondylosis
- Failed conservative management
- Ideal candidate: younger patient, single/two-level soft disc disease, preserved motion, minimal facet arthropathy, no significant instability or kyphosis — motion preservation aims to reduce adjacent segment degeneration vs fusion
Past Medical History
- Contraindications: significant facet arthrosis, ankylosis, instability, severe osteoporosis, infection, significant kyphotic deformity, OPLL, prior fusion adjacent
- Metal allergy (implant materials)
- Standard PMH, smoking, etc.
Imaging Review
X-ray (AP, lateral, flexion/extension)
- Preserved motion at target level (arthroplasty requires mobile segment), alignment/lordosis, facet integrity, no instability
MRI
- Soft disc vs hard spondylosis, cord/root compression, facet arthropathy (excludes arthroplasty if severe)
CT
- Bony anatomy, ossification, endplate morphology, exclude OPLL
Labs
- CBC, BMP, Coags, Type and screen
Neurological Examination
- Full cervical myotomal/dermatomal exam, myelopathy signs, baseline swallowing/voice
Surgical Planning
Case Logistics, OR Needs & Orders
- OR table/bed: standard supine radiolucent OR table, often reversed for C-arm access; tape shoulders caudally for lower-cervical lateral fluoroscopy.
- OR setup: radiolucent/Jackson table, fluoroscopy or O-arm/navigation, microscope/loupes for decompression, implant trays/graft ready for fusion, neuromonitoring for myelopathy/cord-risk cases, and postop brace plan confirmed.
- Special needs: arterial line/Foley/type-screen for long fusion/corpectomy, no long paralytic when MEPs are used, MAP/normotension for myelopathy or cord-risk cases, antibiotic redosing, and anticoagulation/DVT plan.
- Immediate postop orders: neuro checks by myotome/sensory level, airway/dysphagia watch for anterior cervical cases, CT/X-rays per construct, drain care, brace/activity orders, DVT prophylaxis timing, bowel regimen, and PT/OT mobilization.
Position & Approach
- Same as ACDF: supine, neutral neck (avoid excessive extension — preserves natural alignment for the prosthesis), horseshoe/Mayfield, shoulders taped down
- Anterior Smith-Robinson approach (typically left-sided)
Key Surgical Steps
- Fluoroscopic level confirmation, transverse incision, platysma, develop interval (carotid sheath lateral, trachea/esophagus medial)
- Longus colli elevation, midline marking is critical (prosthesis must be centered for proper articulation)
- Complete discectomy and decompression (PLL removal, foraminotomy) — same thoroughness as ACDF
- Preserve endplates (do not over-resect — prosthesis relies on endplate integrity; keep parallel, preserve bone)
- Maintain uncovertebral joints/lateral anatomy for device centering
- Trial and size prosthesis (height, footprint) under fluoroscopy
- Center the device precisely in coronal and sagittal planes (off-center → heterotopic ossification, wear, malfunction)
- Implant the arthroplasty device, confirm position/motion with fluoroscopy
- Closure (no plate; no bone graft needed)
Critical Anatomy & Structures at Risk
- Recurrent laryngeal nerve, esophagus, carotid sheath (same as ACDF)
- Endplates — preserve for device function
- Spinal cord/roots (decompression)
- Vertebral arteries (lateral limit)
Equipment
- Cervical arthroplasty device + trials (level-specific instrumentation)
- Fluoroscopy, microscope/loupes, Caspar pins (careful — avoid endplate damage), Kerrison/curettes, drill
Monitoring
- SSEPs, MEPs (myelopathy), EMG
Anesthesia
- Same as ACDF
Potential Complications
- Heterotopic ossification (can negate motion preservation)
- Device migration/subsidence/malposition
- Dysphagia, RLN palsy, esophageal injury (approach)
- Persistent/recurrent neural compression, facet pain
- Adjacent segment disease (theoretically reduced vs fusion)
Operative Note Template
Preoperative Diagnosis: Cervical [radiculopathy/myelopathy] at [C_-C_] from soft disc herniation
Postoperative Diagnosis: Same
Procedure: Cervical total disc arthroplasty at [C_-C_]
Surgeon / Assistant: Anesthesia: General endotracheal EBL / Fluids: Adjuncts: Fluoroscopy, microscope/loupes Implants: Cervical disc arthroplasty device [type/size] Monitoring: [SSEP/MEP if myelopathic] — stable Complications: None
Indications: [Age]yo [M/F] with single-level [C_-C_] [radiculopathy/myelopathy] from a soft disc with preserved motion and minimal facet arthrosis — an ideal arthroplasty candidate. Risks/benefits/alternatives (incl. ACDF) discussed.
Description of Procedure: After consent and time-out, general anesthesia was induced and the patient positioned supine with the neck neutral (avoiding excess extension). A left anterior Smith-Robinson approach exposed the [C_-C_] disc; the level was confirmed fluoroscopically and the longus colli elevated symmetrically with careful midline marking. A complete discectomy and decompression (including PLL/foraminotomy) was performed while preserving the bony endplates parallel and intact.
The disc space was trialed and the arthroplasty device sized and centered precisely in the coronal and sagittal planes under fluoroscopy, then implanted; position and segmental motion were confirmed. No plate or graft was required.
Hemostasis was obtained and the wound closed in layers. The patient was awakened neurologically [at baseline] and transferred to recovery.
Postoperative Plan
- Floor, neuro checks, airway/neck swelling monitoring (as ACDF)
- NO rigid collar (motion preservation; soft collar only briefly for comfort)
- NSAIDs often given to reduce heterotopic ossification (opposite of fusion philosophy)
- Early ROM, X-rays POD1
- Activity, follow-up; flexion/extension films to confirm motion at follow-up
Chief-Level Case Review
Use these as the senior-level mental model for Cervical Disc Arthroplasty (Cervical Disc Replacement):
- Decision point: Localize twice and instrument once: numbering, transitional anatomy, prior hardware, rib count, navigation dataset, and fluoroscopic level confirmation are mandatory.
- Technical lever: Positioning is treatment: table choice, abdomen-free prone setup, alignment goals, shoulders/hips, eyes/plexus pressure, neuromonitoring baselines, and fluoroscopic access all change the case.
- Bailout: Protect neural elements by sequence: decompression before correction when needed, MAP support for cord risk, no long paralytic with MEPs, and immediate response to signal change.
- Postop watch: Finish with construct logic: decompression adequacy, screw purchase, alignment, fusion bed/graft, drain plan, brace/activity orders, postop CT/X-rays, and DVT timing.
Common Pimp Questions
Use these to pressure-test preparation for Cervical Disc Arthroplasty (Cervical Disc Replacement):
- What neurologic level and root are responsible for the presenting deficit?
- What is the decompression target and how will you know it is adequately decompressed?
- What instability, deformity, bone-quality, or fusion variable changes the construct?
- What vascular, visceral, dural, or neural structure is the main structure at risk?
- What postop brace, drain, mobilization, MAP, antibiotic, and DVT plan should be ordered?
Attending Preference Variables
Items that commonly vary by surgeon or institution:
- Positioning frame, arms, traction, and localization workflow: [attending-specific]
- Navigation/robot/fluoro use, screw system, graft/biologic choice, and drain threshold: [attending-specific]
- Neuromonitoring modality and MAP goal for myelopathy, deformity, or cord-risk cases: [attending-specific]
- Brace, Foley, antibiotics, mobilization, and DVT prophylaxis timing: [attending-specific]